Introduction
Gastric cancer is one of the leading causes of
cancer related death worldwide (1).
Advanced gastric cancer exhibits poor prognosis, and even optimal
combination modalities of surgery, chemotherapy, and radiotherapy
cannot attain satisfactory survival outcomes.
S-1 is a fluoropyrimidine containing compound
consisting of a combination of tegafur, gimeracil, and oteracil
potassium. A randomized phase III trial of adjuvant chemotherapy
with S-1 (ACTS-GC) demonstrated that surgery with S-1 adjuvant
chemotherapy surpassed surgery alone in stage II⁄III gastric cancer
(2,3).
Thereafter, curative gastrectomy and adjuvant chemotherapy using
S-1 have become a standard treatment for stage II/III gastric
cancer in Japan. However, in the subgroup analysis of ACTS-GC, the
5-year overall survival (OS) rate of patients with stage III
disease was 50.2%, leaving room for improvement.
Molecular targeted therapy is an alternative
therapeutic tool for advanced cancer, and the receptor tyrosine
kinase (RTK) family is one such promising candidate target. The
fibroblast growth factor (FGF) family which includes important
regulatory factors of cell growth and differentiation, has been
found to be involved in embryonic development, angiogenesis, and
tumorigenesis (4,5). The FGF receptor (FGFR) family, one type
of RTK family, is a transmembrane tyrosine kinase receptor involved
in signaling via interaction with the FGF family. To date, four
different members of the FGFR family, FGFR1, FGFR2, FGFR3 and
FGFR4, have been cloned and characterized (6–8). FGFR2
gene amplification was initially found in a gastric cancer cell
line originating from diffuse type gastric cancer (9). FGFR2 has been demonstrated to be a poor
prognostic biomarker (10,11) and antibodies (12–14) or
small molecule inhibitors (15–18)
targeting FGFR2 can suppress gastric cancer progression in
vivo and in vitro.
The human epidermal growth factor receptor
(EGFR/HER) family is involved in complex and tightly controlled
signaling pathways that regulate various cellular functions, such
as cell proliferation, organ development, and organ repair. Among
four members of the HER family (EGFR, HER2, HER3 and HER4), HER3 is
indicated to play an important role in HER signaling and drug
resistance (19). With dimerization
with EGFR or HER2, HER3 signals through phosphatidylinositol
3-kinase pathway (20,21).
We have previously analyzed various RTK expressions
and reported that HER3 and EGFR were significant and marginally
significant independent prognostic factors, respectively, in
patients with stage II/III gastric cancer who underwent curative
gastrectomy followed by adjuvant chemotherapy with S-1 (22). However, we have not included this
critical RTK of FGFR2 in the study. We hypothesized that FGFR2
alone or that in combination with HER3 and EGFR plays an important
role on survival outcomes of these patients. Therefore, we analyzed
correlation between HER3 or EGFR expression and FGFR2 expression
using the identical patients of the previous study, and evaluated
the prognostic impact of FGFR2 expression in patients with stage
II/III gastric cancer treated by curative gastrectomy followed by
adjuvant chemotherapy with S-1.
Materials and methods
Patients
From January 2000 to December 2010, 172 patients
with stage II/III advanced gastric cancer underwent curative
surgery followed by adjuvant S-1 chemotherapy at Kitasato
University Hospital. Of the 172 patients, informed consent to use
specimens was obtained from 167 patients, for whom the median
follow up term was 75 months (inter quartile range, 61–90 months).
These patients were identical to the patients whom we had analyzed
previously (22).
This study was conducted in accordance with the
Declaration of Helsinki and was approved by the Research Ethics
Committee of the Kitasato University School of Medicine
(Sagamihara, Japan).
Surgery
Gastrectomy with D1 lymph node dissection was
performed for clinical stage IA gastric cancer (n=25). Gastrectomy
with D2 lymph node dissection was otherwise performed (n=142). The
extent of lymph node dissection was determined according to the
Japanese Classification of Gastric Carcinoma (second English
edition) (23).
Postoperative chemotherapy of S-1
The dose of S-1 was based on body-surface area:
<1.25 m2 (80 mg daily); ≥1.25 m2 but
<1.50 m2 (100 mg daily); ≥1.50 m2 (120 mg
daily). The adjuvant S-1 was administered for 4 weeks followed by 2
weeks rest. This 6-week cycle was repeated principally during the
first year after surgery.
Immunohistochemistry (IHC)
analysis
Tumor specimens used in this study were derived from
routine formalin-fixed, paraffin embedded tissue samples obtained
from resected gastric cancer specimens. Sections (3-µm thick) were
cut from the paraffin blocks and mounted on silanized slides. For
IHC analysis of FGFR2, tumor tissue sections were deparaffinized in
xylene and dehydrated with graded ethanol. After washing with
distilled water, antigen unmasking was performed with a pressure
cooker using citrate buffer. Endogenous peroxidase activity was
blocked by incubation in 3% H2O2/methanol for
15 min, and nonspecific antibody binding was blocked by incubation
with 1% diluted normal horse serum for 30 min. Sections were then
incubated at room temperature for 60 min with the following
antibodies: Mouse FGFR2 monoclonal antibody (M01, clone 1G3)
(dilution of 1:800; Abnova, Heidelberg, Germany,). Immune complexes
were detected with a Vectastain Elite ABC kit (Vector Laboratories,
Inc., Burlingame, CA, USA) according to the manufacturer's
instructions. These immune complexes were detected using the
3,3′-diaminobenzidine tetrahydrochloride substrate with/without
nickel ammonium sulfate (DAB; Vector Laboratories, Inc.) as a
chromogen for 5 min. Sections were counterstained with
hematoxylin.
IHC staining of HER3 and EGFR was performed as
previously reported (22).
Scoring system of IHC staining
To assess IHC staining, all slides were observed
under a microscope. Investigators were blinded to the prognostic
analysis data. We adopted almost the same scoring system for FGFR2
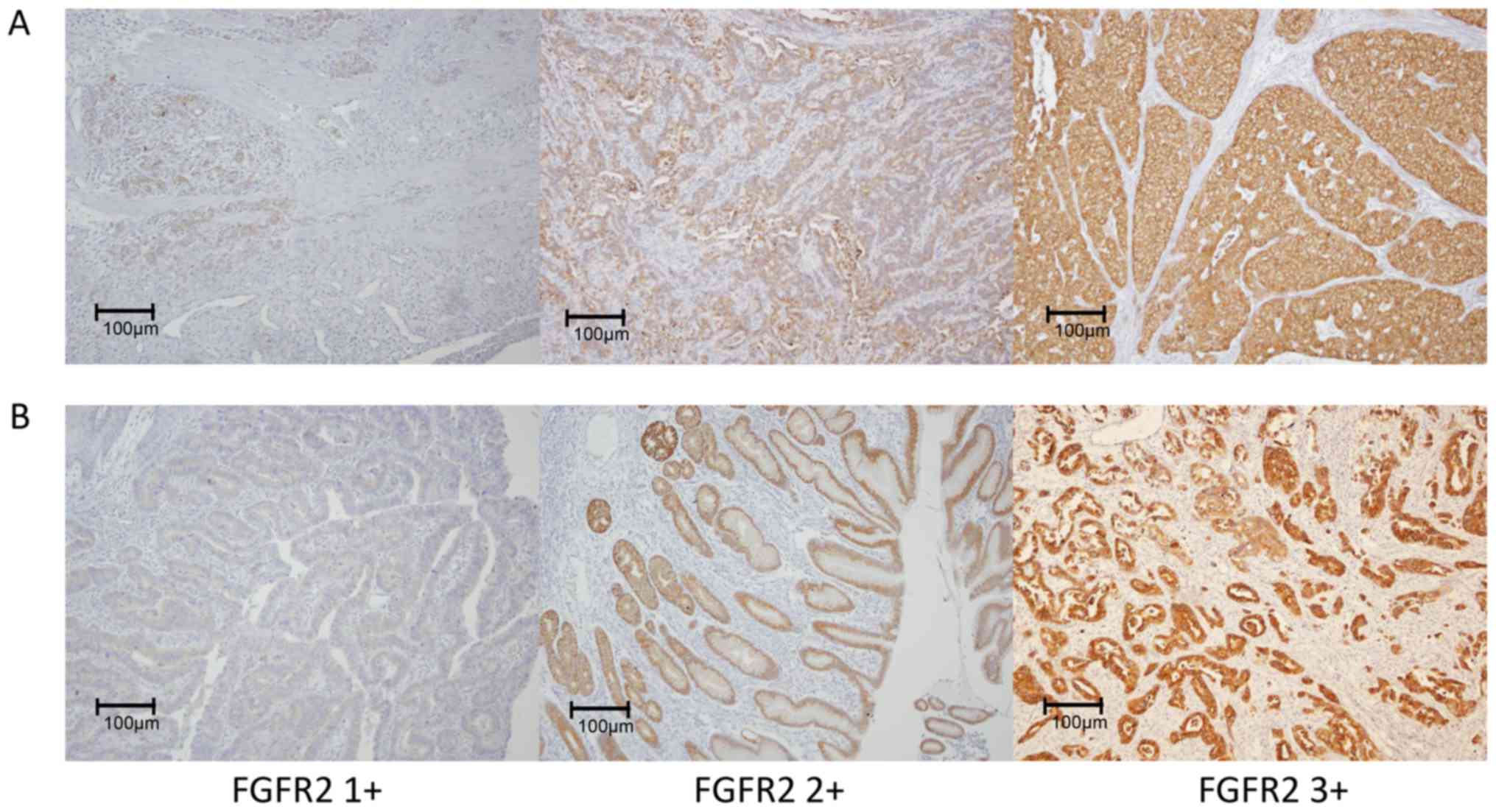
as was reported by Nagatsuma et al (24). We defined the scores for FGFR2 as
follows: 0, staining reactivity in <50 % of cancer cells; 1+,
cytoplasm and/or nuclear reactivity with faint staining in more
than 50% of the cancer cells; 2+, cytoplasm and/or nuclear
reactivity with weak or moderate staining in more than 50% of the
cancer cells; 3+, cytoplasm and/or nuclear reactivity with strong
staining in more than 50% of the cancer cells.
The scoring system for IHC staining of HER3 and EGFR
was described before (22).
Statistical analysis
Relapse-free survivals (RFS) were measured from the
dates of surgery to the dates of relapse of gastric cancers or
dates of last follow-up. Patients who died from causes other than
gastric cancer were regarded as censored at the time of death.
Patients who were alive at the times of their last visits were also
regarded as censored. Student's t-test was used to analyze
continuous variables, and Chi square test or Fisher's exact test
was used to analyze categorical variables. Survival curves were
estimated using the Kaplan-Meier method, and the statistical
significance of differences between survival curves was assessed
using the log-rank test. Survival analyses were conducted using a
Cox proportional hazards model. All calculations were performed
using the JMP® 11.2 (SAS Institute Inc., Cary, NC, USA),
and P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics and stage
distributions
The characteristics of patients included in this
study are listed in Table I. More
than half of the patients had pT4a tumors. The FGFR2 IHC results
were obtained in all 167 specimens as follows: FGFR2 grade 1+, 32
(19%); FGFR2 grade 2+, 80 (48%); FGFR2 grade 3+, 55 (33%).
Representative examples of immunostaining for FGFR2 in diffuse type
cancer (Fig. 1A) and intestinal type
cancer (Fig. 1B).
 | Table I.Characteristics of the patients. |
Table I.
Characteristics of the patients.
| Category | n=167 |
|---|
| Age (years) |
|
| Median
(range) | 65 (35–83) |
| Sex, n (%) |
|
| Male | 117 (70) |
| Tumor stage (TNM
7th), n (%) |
|
| T2 | 28
(17) |
| T3 | 34
(20) |
| T4a | 103 (62) |
| T4b | 2
(1) |
| Nodal stage (TNM
7th), n (%) |
|
| N0 | 24
(14) |
| N1 | 43
(26) |
| N2 | 38
(23) |
| N3 | 62
(37) |
| TNM 7th stage, n
(%) |
|
| IIA | 13 (8) |
| IIB | 36
(22) |
| IIIA | 43
(26) |
| IIIB | 37
(22) |
| IIIC | 38
(23) |
| Histological type, n
(%) |
|
|
Diffuse | 58
(35) |
|
Intestinal | 109 (65) |
| FGFR2 IHC status, n
(%) |
|
| 0 | 0 |
| 1+ | 32
(19) |
| 2+ | 80
(48) |
| 3+ | 55
(33) |
| HER3 IHC status, n
(%) |
|
| 0 | 69
(41) |
| 1+ | 68
(41) |
| 2+ | 30
(18) |
| 3+ | 0 |
| EGFR IHC status, n
(%) |
|
| 0 | 0 |
| 1+ | 62
(37) |
| 2+ | 57
(34) |
| 3+ | 48
(29) |
Relations of FGFR2 expression to
clinicopathological features and correlation between FGFR2
expression and HER3 or EGFR expression
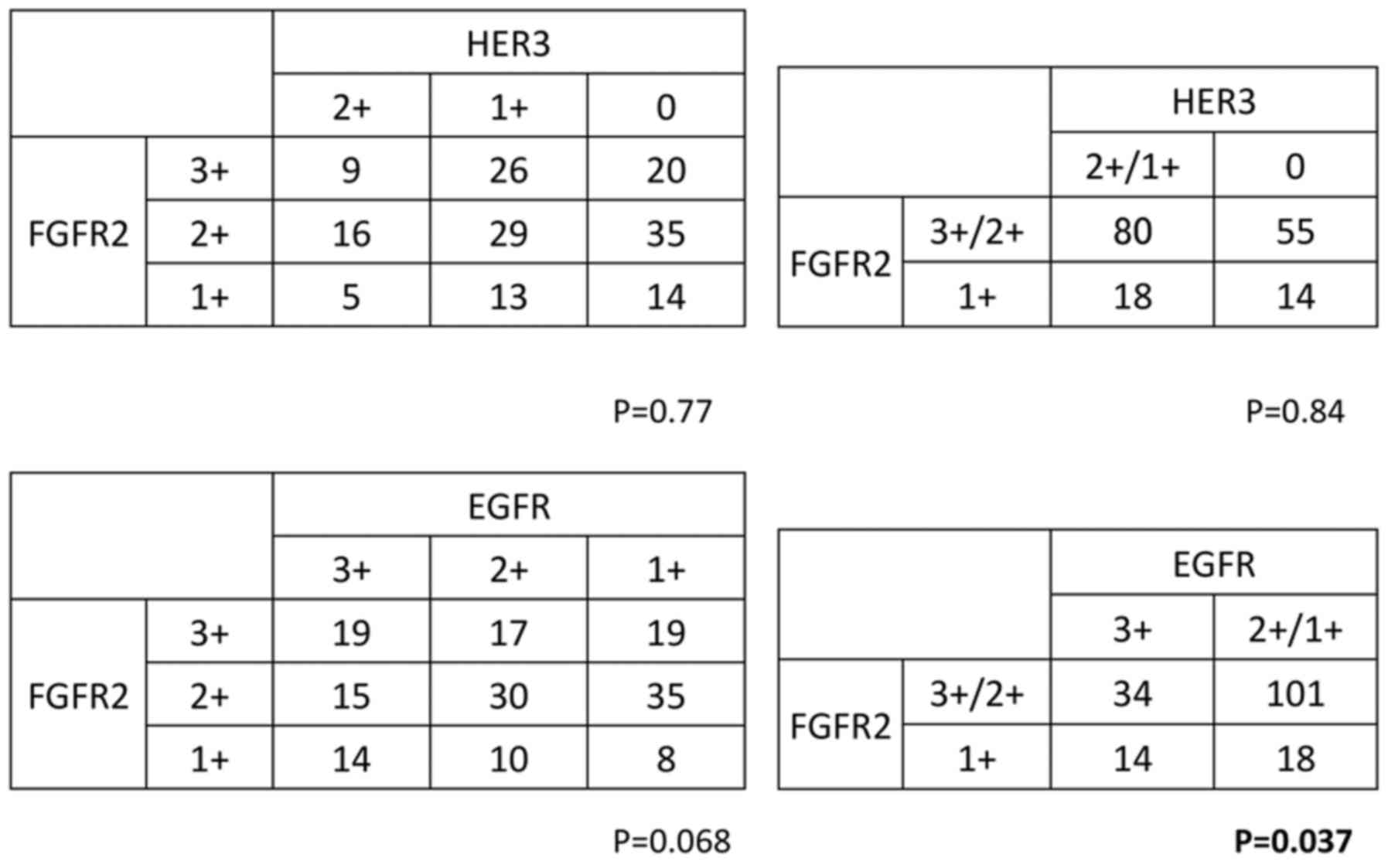
We divided the study samples into two groups [low
FGFR2 expression group: FGFR2 IHC grade 1+, 2+ (n=112); high FGFR2
expression group: FGFR2 IHC grade 3+ (n=55)]. The relations of IHC
staining levels to clinicopathological features were then examined.
FGFR2 IHC staining level was significantly related to patients' age
(P=0.043) and tended to be related to lymph node metastasis
(P=0.099) (Table II). There was no
correlation between FGFR2 expression and HER3 expression, whereas
the FGFR2 expression level was correlated with the EGFR expression
level (P=0.037; Fig. 2).
| Table II.Relations of FGFR2 IHC staining
levels to clinicopathological features. |
Table II.
Relations of FGFR2 IHC staining
levels to clinicopathological features.
|
Variable/category | FGFR2 1+/2+
(n=112) | FGFR2 3+
(n=55) | P-value |
|---|
| Age |
|
| 0.043 |
|
<65 | 53 | 17 |
|
|
≥65 | 59 | 38 |
|
| Sex |
|
| 1.000 |
|
Male | 78 | 39 |
|
|
Female | 34 | 16 |
|
| Serosal
invasion |
|
| 0.734 |
|
Absent | 43 | 19 |
|
|
Present | 69 | 36 |
|
| Lymph node
metastasis |
|
| 0.099 |
|
Absent | 20 | 4 |
|
|
Present | 92 | 51 |
|
| Cancer stage, n
(%) |
|
| 0.283 |
|
IIA/IIB | 36 | 13 |
|
|
IIIA/IIIB/IIIC | 76 | 42 |
|
| Histologic type, n
(%) |
|
| 0.604 |
|
Diffuse | 37 | 21 |
|
|
Intestinal | 75 | 34 |
|
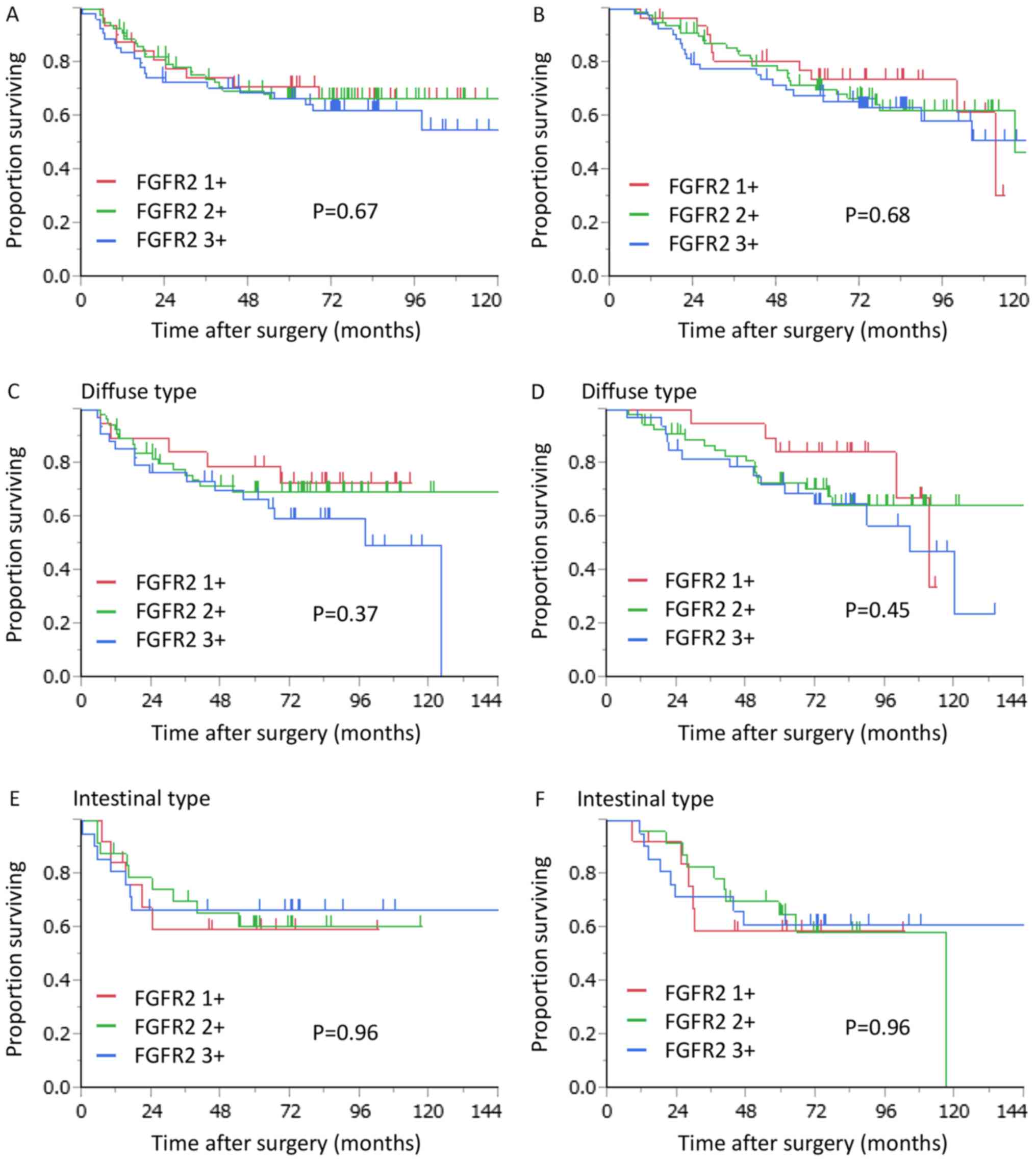
Effects of clinicopathological factors
and FGFR2 expression on RFS and OS
Five-year RFS and OS were 67.7 and 70.1%,
respectively. Elderly patients aged 65 or more had significantly
worse RFS and OS than young patients aged less than 65 [hazard
ratio (HR) 1.75, 95% confidence interval (CI) 1.02–3.10, P=0.042
and HR 2.20 95% CI 1.28–3.94, P=0.005], while female patients had
significantly better OS than male patients (HR 0.47, 95% CI
0.24–0.85, P=0.012). Patients with TNM stage III had significantly
worse RFS than those with TNM stage II (HR 2.68, 95% CI 1.38–5.87,
P=0.003). On the other hand, there was no relation of FGFR2
expression status to RFS or OS in the study group (Table III, Fig.
3). However, when we restricted patients to those with diffuse
type cancer, patients with high FGFR2 expression had slightly worse
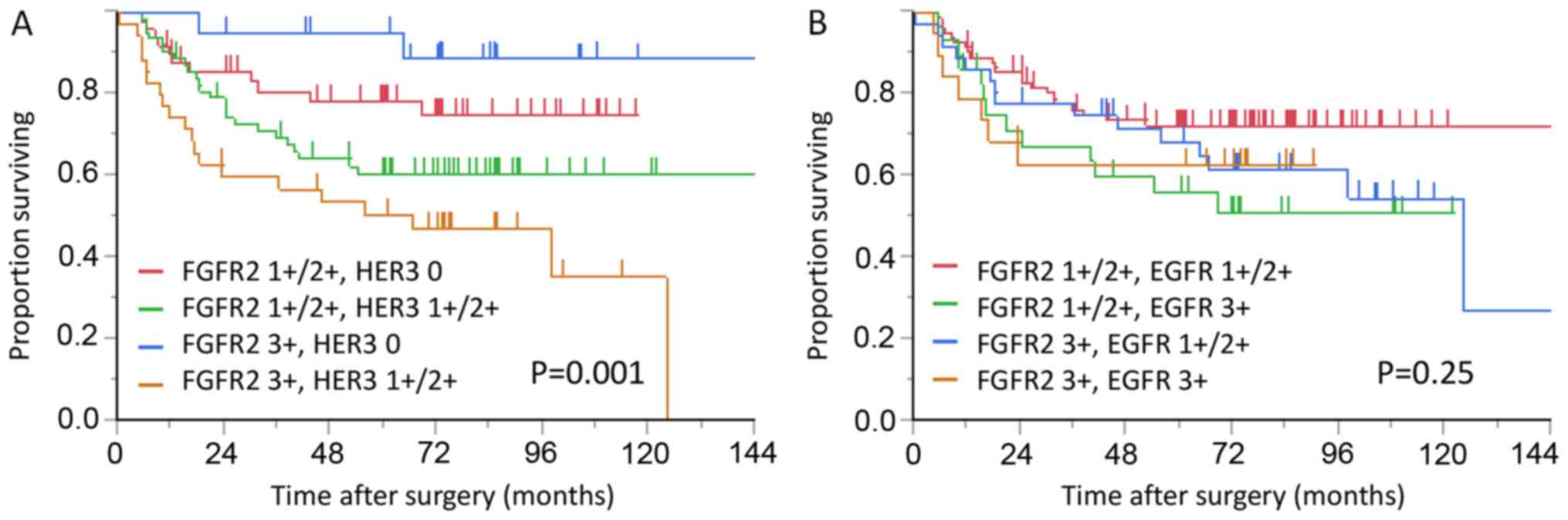
RFS than those with low FGFR2 expression (P=0.37; Fig. 3C). Moreover, when we combined FGFR2
and HER3 expression, prognostic impact of HER3 was augmented by
FGFR2 expression with 5-year survival rate of 95 and 51% in
patients with FGFR2/HER3 3+/0 and FGFR2/HER3 3+/1+ or 2+,
respectively (P<0.001; Fig. 4A).
Statistical significant differences were also found between the
FGFR2/HER3 3+/0 group and the FGFR2/HER3 1+ or 2+/1+ or 2+ group
and between the FGFR2/HER3 1+ or 2+/0 group and the FGFR2/HER3
3+/1+ or 2+ group with P values of 0.021 and 0.004, respectively.
When we combined FGFR2 and EGFR expression, no correlation was
found in RFS (Fig. 4B).
| Table III.Cox proportional hazards analysis of
clinicopathological factors for OS and RFS. |
Table III.
Cox proportional hazards analysis of
clinicopathological factors for OS and RFS.
|
|
|
| RFS | OS |
|---|
|
|
|
|
|
|
|---|
| Variable | Category | No. of
patients | 5-year survival
(%) | HR (95% CI) | P-value | 5-year survival
(%) | HR (95% CI) | P-value |
|---|
| Age | <65 | 70 | 76.6 | 1.0 | 0.042 | 83.1 | 1.0 | 0.005 |
|
| ≥65 | 97 | 60.8 | 1.75
(1.02–3.10) |
| 60.9 | 2.20
(1.28–3.94) |
|
| Sex | Male | 117 | 62.5 | 1.0 | 0.084 | 62.9 | 1.0 | 0.012 |
|
| Female | 50 | 79.5 | 0.59
(0.31–1.07) |
| 85.8 | 0.47
(0.24–0.85) |
|
| TNM stage | IIA/IIB | 49 | 84.5 | 1.0 | 0.003 | 78.3 | 1.0 | 0.088 |
|
| IIIA/IIIB/IIIC | 118 | 60.8 | 2.68
(1.38–5.87) |
| 66.7 | 1.67
(0.93–3.22) |
|
| Histologic
type | Differentiated | 58 | 70.4 | 1.0 | 0.410 | 61.9 | 1.0 | 0.096 |
|
|
Undifferentiated | 109 | 62.4 | 0.80
(0.47–1.38) |
| 74.6 | 0.64
(0.38–1.09) |
|
| FGFR2 IHC
status | 1+, 2+ | 112 | 68.1 | 1.0 | 0.377 | 71.2 | 1.0 | 0.411 |
|
| 3+ | 55 | 66.6 | 1.27
(0.74–2.16) |
| 67.8 | 1.25
(0.73–2.09) |
|
We further analyzed RFS using the combined
expressions of the three biomarkers (Fig.
5). Patients with FGFR2 3+, HER3 1+/2+, and EGFR 3+ belonged to
one of the worst survival groups with 5 year relapse-free and OS
rates of 53 and 59%, respectively. However, no significant
difference was found between the FGFR2 3+, HER3 1+/2+, EGFR 3+
group, the FGFR2 1+, 2+, HER3 1+/2+, EGFR 3+ group, and the FGFR2
3+, HER3 1+/2+, EGFR 1+, 2+ group (P=0.82).
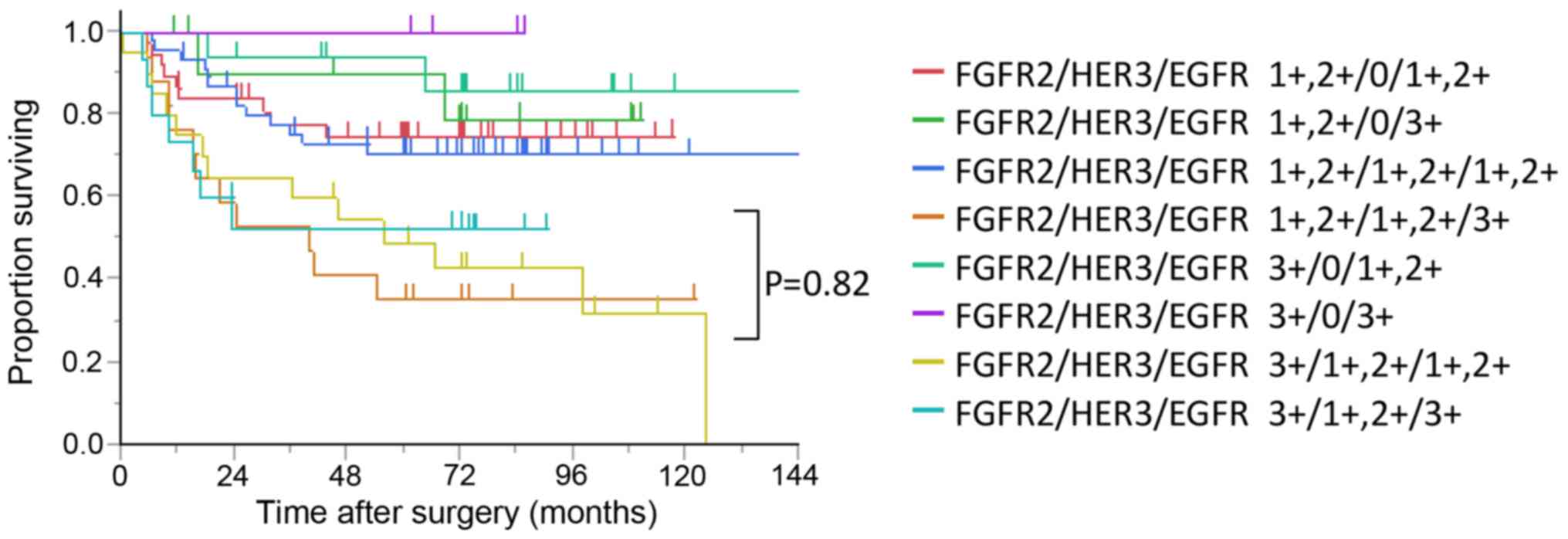 | Figure 5.Kaplan-Meier curves for relapse-free
survival in patients with stage II/III gastric cancer stratified by
combination of FGFR2, HER3, and EGFR expressions. Although patients
with FGFR2 3+, HER3 1+/2+, and EGFR 3+ belongs to one of the worst
survival groups, no significant difference is found between the
FGFR2 3+, HER3 1+/2+, and EGFR 3+ group, FGFR2 1+/2+, HER3 1+/2+,
and EGFR 3+ group, and FGFR2 3+, HER3 1+/2+, and EGFR 1+/2+ group
(P=0.82). FGFR, fibroblast growth factor receptor; HER, human
epidermal growth factor receptor; EGFR, EGFR, epidermal growth
factor receptor. |
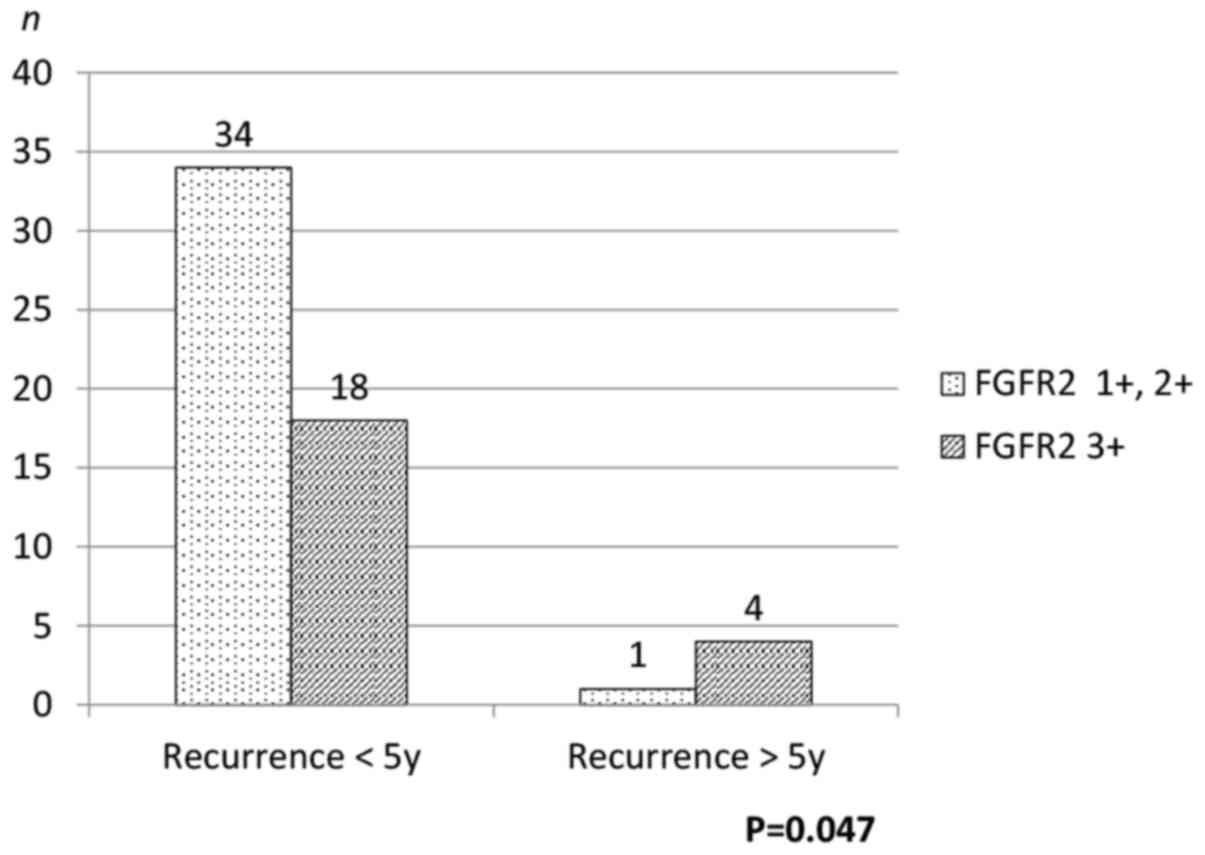
Timing of recurrence
Of the 165 patients, 57 recurred. Proportion or
patients with recurrence was similar between the high FGFR2
expression group and the low FGFR2 expression group [40% (22/55)
vs. 31% (35/112), P=0.27]. Of the 57 recurred patients, 5 recurred
more than 5 years after surgery (Table
IV). Proportion of patients who recurred more than 5 years
after surgery was significantly larger in the high FGFR2 expression
group than in the low FGFR2 expression group [18% (4/22) vs. 2.9%
(1/35), P=0.047] (Fig. 6). All the 5
patients had tumors of diffuse type and serosal invasion (pT4a).
Reciprocal relation was found between FGFR2 expression and EGFR
expression. That is, 4 had tumors with FGFR2 grade 3+ and EGFR
grade 1+, while the other had tumors with FGFR2 grade 1+ and EGFR
grade 3+. One female patient with high FGFR2 expression recurred
more than 10 years after surgery. She was 55 years old at the time
of surgery and underwent total gastrectomy with D2 lymph node
dissection. She had a tumor with serosal invasion (pT4a) but no
lymph node metastasis at the time of surgery. At the 10th year
check-up, CT scan revealed that she had para-aortic lymph node
metastasis.
| Table IV.Patients who had recurrence >5
years after surgery. |
Table IV.
Patients who had recurrence >5
years after surgery.
| Age | Sex | Histology | pT | pN | pStage | FGFR2 IHC | HER3 IHC | EGFR IHC | Interval between
surgery and recurrence (months) |
|---|
| 38 | F | Diffuse | 4a | 0 | IIB | 3+ | 2+ | 1+ | 67 |
| 55 | F | Diffuse | 4a | 0 | IIB | 3+ | 1+ | 1+ | 124 |
| 66 | F | Diffuse | 4a | 1 | IIIA | 3+ | 0 | 1+ | 64 |
| 63 | M | Diffuse | 4a | 3 | IIIC | 1+ | 0 | 3+ | 68 |
| 66 | M | Diffuse | 4a | 3 | IIIC | 3+ | 1+ | 1+ | 98 |
Discussion
The present study retrospectively evaluated the
influence of FGFR2 expression on the survival outcomes of patients
with stage II/III gastric cancer who underwent curative gastrectomy
followed by adjuvant chemotherapy using S1. The FGFR2 expression
was not significantly associated with RFS or OS. When we restricted
patients to those with diffuse type cancer, FGFR2 expression levels
tended to be negatively correlated with RFS. Moreover, proportion
of patients who recurred more than 5 years after surgery was
significantly larger in the high FGFR2 expression group than in the
low FGFR2 expression group.
The FGFR2 expression level was not significantly
associated with RFS or OS. Nagatsuma et al (24) reported that high expression of FGFR 2
correlated with tumor progression and survival in patients with
gastric cancer. However, they did not refer to adjuvant
chemotherapies and stage distribution. On the other hand, patients
in this current study had pathological stage II or III and received
adjuvant chemotherapy using S1. Adjuvant S1 chemotherapy might have
some power to negate the difference of survival outcomes between
different FGFR2 expression levels.
When we restricted patients to those with diffuse
type gastric cancer, survival outcome was not significantly but
slightly correlated with FGFR2 expression. High FGFR2 expression
tended to be slightly worse survival outcomes. Inokuchi et
al reported that high FGFR2 expression significantly correlated
with tumor progression and survival only in diffuse type gastric
cancer (25). If our study patients
had not been treated with S1 adjuvant chemotherapy, the negative
effect of FGFR2 expression might have significance on survival
outcomes.
We previously reported that HER3 expression was a
significant independent prognostic factor in patients with stage
II/III gastric cancer who receive curative resection and adjuvant
chemotherapy with S-1. In our current study, the analyzed patients
of which are identical to those of previous one, FGFR2
overexpression augmented prognostic impact of HER3 expression. EGFR
family members are reported to be downstream targets of the
amplified and highly activated FGFR2 kinase (26). That may explain the augmentation by
FGFR2 expression. On the other hand, among the patients without
expression of HER3, patients with high FGFR2 expression had higher
survival than those with low FGFR2 expression. However, the
difference between these patients is not statistically significant
in the log-rank test (P=0.19). FGFR2 overexpression would not be as
strongly associated with RFS as HER3 would be. That may be the
reason why high FGFR2 expression did not have significantly lower
RFS than low FGFR2 expression in patients without expression of
HER3.
An interesting finding of our study was that
patients who had recurrence more than 5 years after surgery had a
significantly higher probability of having tumors with high FGFR2
expression. Recurrent sites of long-term failure mostly were
peritoneum among diffuse type tumors. The patient with gastric
cancer was assumed to be cured at 5 years after surgery unless any
signs of recurrence were found. Then, the follow-up was usually
terminated. However, we more recently have experienced late
recurrence since the introduction of adjuvant chemotherapy using
S1. Indeed, 18% of the recurrent patients with high FGFR2
expression recurred more than 5 years after surgery. This would
affect the follow-up strategy for gastrectomized patients who
underwent S1 adjuvant chemotherapy. A few studies have focused on
the timing of recurrence and clinicopathological factors (27–29).
Preoperative serum carcinoembryonic antigen level, tumor size, LN
metastasis and venous invasion have been reported to be independent
predictors of the timing of recurrence. However, no biomarker has
been reported to be able to predict the timing of recurrence after
surgery. To the best of our knowledge, this finding for the first
time indicated that FGFR2 could predict long-term failure of
postoperative adjuvant S1 chemotherapy in curative advanced gastric
cancer. For patients with long-term failure, FGFR2 IHC level should
be examined. If FGFR2 overexpression were confirmed, antibodies or
small molecule inhibitors targeting FGFR2 might suppress
progression of recurrent tumors.
One patient who recurred more than 5 years after
surgery had tumors with FGFR2 IHC status of 1+. Instead, this
patient had a tumor with EGFR IHC status of 3+. Moreover, EGFR
expression level was negatively correlated with FGFR2 expression.
This negative correlation might somewhat be associated with the
reciprocal relation of the expressions of FGFR2 and EGFR in these
patients. We cannot fully understand the underlying mechanism of
this phenomenon, but one plausible reason is that both the EGFR and
FGFR2-overexpressing cancer cells would have aggressive nature to
cause early failure of S1 adjuvant chemotherapy, while either EGFR
or FGFR2-overexpressing cancer cells would have relatively slow
growing nature and could evade chemotherapy with the capacity of
dormancy (30). That might be the
reason why the reciprocal expression between the EGFR and the FGFR2
was found in patients who recurred more than 5 years after
surgery.
It has been reported that Helicobacter pylori
profoundly activates the epidermal growth factor receptor (EGFR)
and its family members HER2 and HER3 (31). We only have checked Helicobacter
pylori infection in 37 (22%) patients since we did not check it
before 2009. In the analysis of these limited patients, no
correlations were found between the Helicobacter infection and
EGFR, HER3, or FGFR2 expression (data not shown).
Our study has some important limitations. First, the
analysis was based on retrospective data collected at a single
center, and the number of included patients was so small that we
sometimes could not demonstrate statistically significant
difference. Second, no rigid rule was applied in terms of dose
reduction and termination of S1 administration. Administered dose
of S1 differed between the studied patients. Third, not all the
patients were followed up for 10 years, so exact recurrence rate
may be different than the observed one.
In conclusion, there was no interaction between
FGFR2 expression and patient survival outcomes in patients with
stage II/III gastric cancer after the standard treatment in Japan.
On the other hand, proportion of patients who recurred more than 5
years after surgery was significantly larger in the high FGFR2
expression group than in the low FGFR2 expression group. Patients
with FGFR overexpression in stage II/III gastric cancer should be
carefully followed-up for more than 5 years after surgery.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sakuramoto S, Sasako M, Yamaguchi T,
Kinoshita T, Fujii M, Nashimoto A, Furukawa H, Nakajima T, Ohashi
Y, Imamura H, et al: Adjuvant chemotherapy for gastric cancer with
S-1, an oral fluoropyrimidine. N Engl J Med. 357:1810–1820. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sasako M, Sakuramoto S, Katai H, Kinoshita
T, Furukawa H, Yamaguchi T, Nashimoto A, Fujii M, Nakajima T and
Ohashi Y: Five-year outcomes of a randomized phase III trial
comparing adjuvant chemotherapy with S-1 versus surgery alone in
stage II or III gastric cancer. J Clin Oncol. 29:4387–4393. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Goetz R and Mohammadi M: Exploring
mechanisms of FGF signalling through the lens of structural
biology. Nat Rev Mol Cell Biol. 14:166–180. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dedes KJ, Wetterskog D, Ashworth A, Kaye
SB and Reis-Filho JS: Emerging therapeutic targets in endometrial
cancer. Nat Rev Clin Oncol. 8:261–271. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Eswarakumar VP, Lax I and Schlessinger J:
Cellular signaling by fibroblast growth factor receptors. Cytokine
Growth Factor Rev. 16:139–149. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Turner N and Grose R: Fibroblast growth
factor signalling: From development to cancer. Nat Rev Cancer.
10:116–129. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brooks AN, Kilgour E and Smith PD:
Molecular pathways: Fibroblast growth factor signaling: A new
therapeutic opportunity in cancer. Clin Cancer Res. 18:1855–1862.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hattori Y, Odagiri H, Nakatani H, Miyagawa
K, Naito K, Sakamoto H, Katoh O, Yoshida T, Sugimura T and Terada
M: K-sam, an amplified gene in stomach cancer, is a member of the
heparin-binding growth factor receptor genes. Proc Natl Acad Sci
USA. 87:pp. 5983–5987. 1990; View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Matsumoto K, Arao T, Hamaguchi T, Shimada
Y, Kato K, Oda I, Taniguchi H, Koizumi F, Yanagihara K, Sasaki H,
et al: FGFR2 gene amplification and clinicopathological features in
gastric cancer. Br J Cancer. 106:727–732. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Su X, Zhan P, Gavine PR, Morgan S, Womack
C, Ni X, Shen D, Bang YJ, Im SA, Ho Kim W, et al: FGFR2
amplification has prognostic significance in gastric cancer:
Results from a large international multicentre study. Br J Cancer.
110:967–975. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhao WM, Wang L, Park H, Chhim S,
Tanphanich M, Yashiro M and Kim KJ: Monoclonal antibodies to
fibroblast growth factor receptor 2 effectively inhibit growth of
gastric tumor xenografts. Clin Cancer Res. 16:5750–5758. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bai A, Meetze K, Vo NY, Kollipara S, Mazsa
EK, Winston WM, Weiler S, Poling LL, Chen T, Ismail NS, et al:
GP369, an FGFR2-IIIb-specific antibody, exhibits potent antitumor
activity against human cancers driven by activated FGFR2 signaling.
Cancer Res. 70:7630–7639. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sommer A, Kopitz C, Schatz CA, Nising CF,
Mahlert C, Lerchen HG, Stelte-Ludwig B, Hammer S, Greven S,
Schuhmacher J, et al: Preclinical efficacy of the auristatin-based
antibody-drug conjugate BAY 1187982 for the treatment of
FGFR2-positive solid tumors. Cancer Res. 76:6331–6339. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chang J, Wang S, Zhang Z, Liu X, Wu Z,
Geng R, Ge X, Dai C, Liu R, Zhang Q, et al: Multiple receptor
tyrosine kinase activation attenuates therapeutic efficacy of the
fibroblast growth factor receptor 2 inhibitor AZD4547 in FGFR2
amplified gastric cancer. Oncotarget. 6:2009–2022. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pearson A, Smyth E, Babina IS,
Herrera-Abreu MT, Tarazona N, Peckitt C, Kilgour E, Smith NR, Geh
C, Rooney C, et al: High-level clonal FGFR amplification and
response to FGFR inhibition in a translational clinical trial.
Cancer Discov. 6:838–851. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kim ST, Jang HL, Lee SJ, Lee J, Choi YL,
Kim KM, Cho J, Park SH, Park YS, Lim HY, et al: Pazopanib, a novel
multitargeted kinase inhibitor, shows potent in vitro antitumor
activity in gastric cancer cell lines with FGFR2 amplification. Mol
Cancer Ther. 13:2527–2536. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Xie L, Su X, Zhang L, Yin X, Tang L, Zhang
X, Xu Y, Gao Z, Liu K, Zhou M, et al: FGFR2 gene amplification in
gastric cancer predicts sensitivity to the selective FGFR inhibitor
AZD4547. Clin Cancer Res. 19:2572–2583. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang N, Chang Y, Rios A and An Z:
HER3/ErbB3, an emerging cancer therapeutic target. Acta Biochim
Biophys Sin (Shanghai). 48:39–48. 2016.PubMed/NCBI
|
|
20
|
Sithanandam G and Anderson LM: The ERBB3
receptor in cancer and cancer gene therapy. Cancer Gene Ther.
15:413–448. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoshioka T, Nishikawa Y, Ito R, Kawamata
M, Doi Y, Yamamoto Y, Yoshida M, Omori Y, Kotanagi H, Masuko T and
Enomoto K: Significance of integrin αvβ5 and erbB3 in enhanced cell
migration and liver metastasis of colon carcinomas stimulated by
hepatocyte-derived heregulin. Cancer Sci. 101:2011–2018. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ema A, Yamashita K, Ushiku H, Kojo K,
Minatani N, Kikuchi M, Mieno H, Moriya H, Hosoda K, Katada N, et
al: Immunohistochemical analysis of RTKs expression identified HER3
as a prognostic indicator of gastric cancer. Cancer Sci.
105:1591–1600. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Japanese Gastric Cancer Association, .
Japanese classification of gastric carcinoma-2nd english edition.
Gastric Cancer. 1:10–24. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nagatsuma AK, Aizawa M, Kuwata T, Doi T,
Ohtsu A, Fujii H and Ochiai A: Expression profiles of HER2, EGFR,
MET and FGFR2 in a large cohort of patients with gastric
adenocarcinoma. Gastric Cancer. 18:227–238. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Inokuchi M, Murase H, Otsuki S, Kawano T
and Kojima K: Different clinical significance of FGFR1-4 expression
between diffuse-type and intestinal-type gastric cancer. World J
Surg Oncol. 15:22017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kunii K, Davis L, Gorenstein J, Hatch H,
Yashiro M, Di Bacco A, Elbi C and Lutterbach B: FGFR2-amplified
gastric cancer cell lines require FGFR2 and Erbb3 signaling for
growth and survival. Cancer Res. 68:2340–2348. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Adachi Y, Oshiro T, Mori M, Maehara Y and
Sugimachi K: Prediction of early and late recurrence after curative
resection for gastric carcinoma. Cancer. 77:2445–2448. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Eom BW, Yoon H, Ryu KW, Lee JH, Cho SJ,
Lee JY, Kim CG, Choi IJ, Lee JS, Kook MC, et al: Predictors of
timing and patterns of recurrence after curative resection for
gastric cancer. Dig Surg. 27:481–486. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Choi JY, Ha TK and Kwon SJ:
Clinicopathologic characteristics of gastric cancer patients
according to the timing of the recurrence after curative surgery. J
Gastric Cancer. 11:46–54. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Aguirre-Ghiso JA: Models, mechanisms and
clinical evidence for cancer dormancy. Nat Rev Cancer. 7:834–846.
2007. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tegtmeyer N, Neddermann M, Asche CI and
Backert S: Subversion of host kinases: A key network in cellular
signaling hijacked by Helicobacter pylori CagA. Mol Microbiol.
105:358–372. 2017. View Article : Google Scholar : PubMed/NCBI
|