Introduction
Breast cancer remains the leading cause of cancer
mortality in females in developing and developed regions (1,2).
Recurrence and poor survival rates are still reported for certain
patients diagnosed with stage I breast cancer (3–5). In
addition to surgical resection, there are specific treatments
administered to patients with breast cancer, including sentinel
lymph node biopsy followed by surgery, radiation therapy,
chemotherapy, hormone therapy and targeted therapy. Personalized
therapies are administered depending on the type and stage of the
cancer and the expression status of estrogen receptor (ER),
progesterone receptor (PgR) and human epidermal growth factor
receptor 2 (HER2). Although personalized therapy based on the
intrinsic subtype of breast cancer has progressed, further
understanding of the molecular biology of the genes involved in
breast cancer development is required.
Cell adhesion molecule (CADM) genes include 4
subfamilies, which are CADM1, CADM2, CADM3 and CADM4. These genes
encode an immunoglobulin superfamily molecule that is involved in
the maintenance of cell-cell adhesion in a variety of human
epithelial cells and therefore protects against malignant
conversion (6,7). It has been established that CADM1 is
located on chromosome 11q23.2 and functions as a tumor suppressor
gene in non-small cell lung cancer (8). CADM1 expression is preferentially lost
in invasive lung adenocarcinoma lesions compared with those that
are non-invasive (9). Previous
studies have identified that the expression of CADM1 is frequently
inactivated in numerous types of cancer, including breast cancer
(10–14). The loss of CADM1 and protein 4.1B
expression leads to the development and progression of breast
cancer, particularly in invasion and metastasis, using primary
breast cancer specimens and breast cancer cell lines (15). Low or aberrant expression of CADM1 in
tumors is significantly associated with lymphovascular invasion and
advanced tumor stages, demonstrating the potential for CADM1
expression to be used as a prognostic biomarker that may aid
effective personalized therapy.
CADM4 is located on chromosome 19q13.31 and
investigation into its role in tumor development is ongoing.
Previous studies have demonstrated that CADM4 may function as a
tumor suppressor in renal clear cell carcinoma and that it is
inactivated in breast and colon cancer (16,17).
Although several previous studies have demonstrated the tumor
suppressive roles of CADM1 and CADM4, further studies are required
to evaluate the expression levels in clinical samples.
The present study reports the association of CADM1
and CADM4 expression levels with clinicopathological factors,
including survival rate in patients with breast cancer, evaluated
using immunohistochemistry (IHC) staining.
Materials and methods
Patients and tissue samples
Primary invasive breast cancer samples were obtained
from patients that underwent surgical resection without systemic
drug therapy prior to surgery at the Department of Organ Regulatory
Surgery at Fukushima Medical University Hospital (Fukushima,
Japan). This cohort consisted of 208 patients who were recruited at
the time of surgery between January 2002 and December 2005.
Detailed backgrounds for each tissue donor were
collected, including age, sex, clinical stage and hormone status
(Table I). Tumor histopathology was
classified according to the Union for International Cancer Control
(UICC) tumor-node-metastasis classification (the 7th
classification) (18,19). Written informed consent was obtained
from all participants. This study was approved by the Institutional
Review Board of Fukushima Medical University (Fukushima,
Japan).
 | Table I.Clinicopathological characteristics of
patients with primary breast cancer. |
Table I.
Clinicopathological characteristics of
patients with primary breast cancer.
| Characteristics | n (%) |
|---|
| Age (years) |
|
| Average
(range) | 55.3 (31–88) |
|
<50 | 82 (39) |
| ≥50 | 126 (61) |
| Sex |
|
| Male | 0 (0) |
|
Female | 208 (100) |
| Metastatic lymph
nodes |
|
| 0 | 128 (62) |
| 1–3 | 56 (27) |
| ≥4 | 24 (11) |
| Lymphovascular
invasion |
|
| − | 84 (40) |
| + | 124 (60) |
| Hormone status |
|
| +/+ and
+/− | 157 (75) |
| −/− | 51 (25) |
| Human epidermal
growth factor receptor 2 |
|
| + | 16 (8) |
| − | 192 (92) |
| Triple
negative | 33 (16) |
| pT stage |
|
| 1 | 116 (56) |
| 2 | 83 (40) |
| 3 | 3 (1) |
| 4 | 6 (3) |
| Pathological
stage |
|
| I | 82 (39) |
| II | 120 (58) |
| III | 6 (3) |
| Local recurrence |
|
| − | 202 (97) |
| + | 6 (3) |
| Remote
recurrence |
|
| − | 192 (92) |
| + | 16 (8) |
IHC analysis
The aforementioned breast cancer tissue samples were
fixed in 10% formalin, embedded in paraffin, cut into 4 µm sections
and stained with hematoxylin and eosin (H&E) and other primary
antibodies. Rabbit polyclonal antibodies against CADM1 (1:500,
C-18, generated by the Division of Molecular Pathology, Institute
of Medical Science, The University of Tokyo) and CADM4 (1:500,
Bc-2, generated by the Division of Molecular Pathology, Institute
of Medical Science, The University of Tokyo) were used as described
previously (20). Antibodies used for
IHC staining were as follows: Anti-ER (1:500, cat. no., MA5-13191;
Dako; Agilent Technologies GmbH, Waldbronn, Germany), anti-PgR
(1:500, cat. no., MA5-12581; Dako; Agilent Technologies GmbH). For
HER2 status, the Histofine® Simple Stain HER2 mono assay
kit was used (cat. no. 427041; Nichirei Biosciences, Inc., Tokyo,
Japan). Analyses of ER, PgR and HER2 were performed by IHC staining
according to the manufacturer's protocol. Sections were
deparaffinized in xylene and hydrated using a graded series of
ethanol at room temperature. Subsequently the sections were washed
3 times in PBS and endogenous peroxidase was blocked with 0.3% in
methanol for 30 min at room temperature. Antigens were retrieved by
autoclaving the sections on slides in 0.01 M pH 6.0 citrate buffer
for 10 min at 121°C. Subsequent to washing in PBS, the sections
were incubated in primary antibody overnight at 4°C. A further wash
in PBS was followed by treatment with the secondary antibody
[K1491, Dako EnVision kit/horseradish peroxidase (HRP)] for 30 min
at room temperature and diaminobenzidine (K1491, Dako EnVision
kit/HRP) was used for staining detection (both from Dako: Agilent
Technologies GmbH). Finally, the sections were counterstained with
hematoxylin. Expression of these proteins was evaluated using
optical microscopy (BX43; Olympus Corporation, Tokyo, Japan) at
×400 magnification.
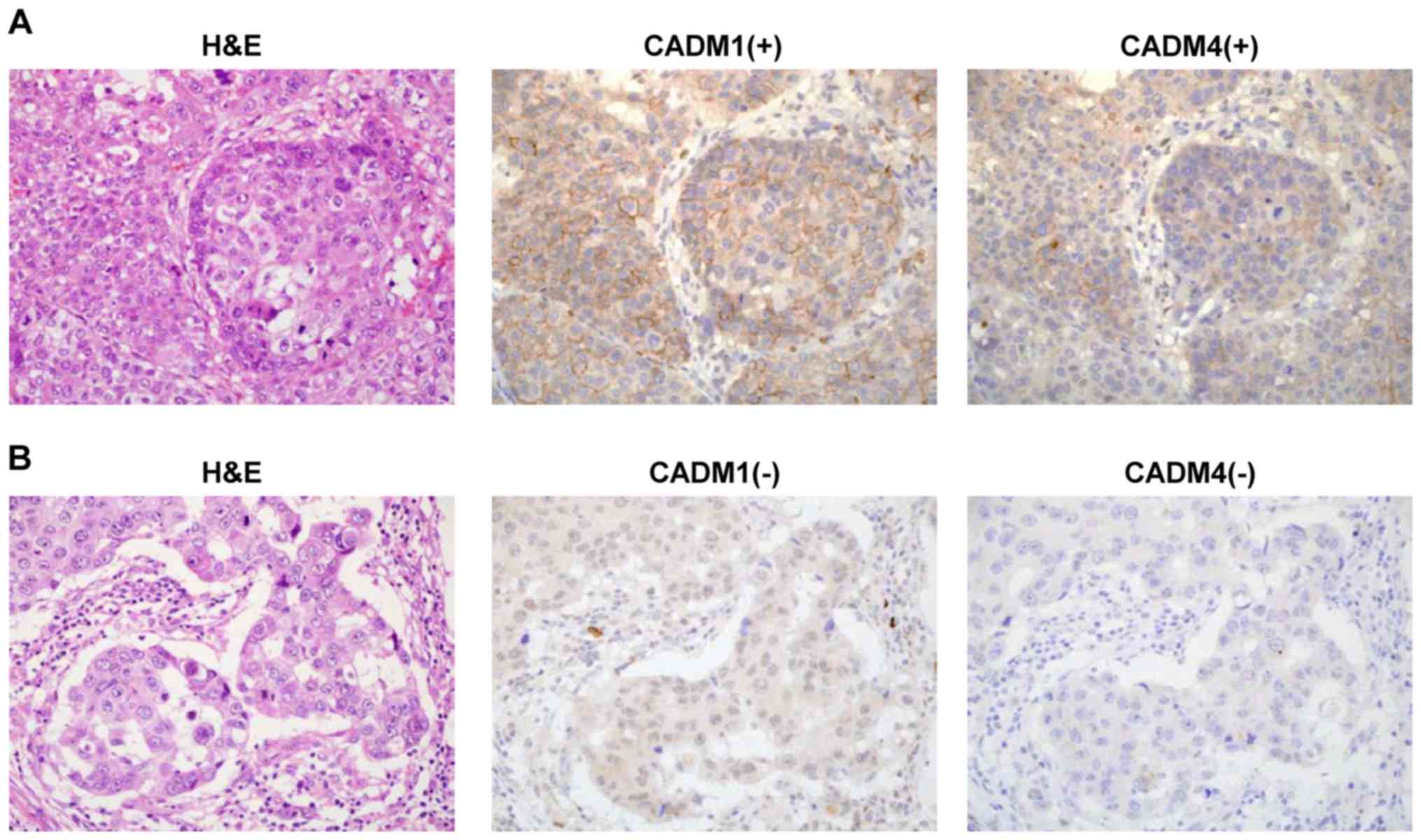
Assessment of IHC stain
The stain signals of CADM1 and CADM4 protein levels
were detected in the membranes in normal mammary epithelial cells.
Cytoplasmic immunoreactivity without membrane staining was defined
as aberrant expression. Membranous staining of CADM1 or CADM4 was
evaluated by calculating the percentage of cancer cells with
membrane expression in the entire area of invasive and non-invasive
lesions. The tumors or lesions were then scored as previously
described (15). Tumors were defined
with scores of 1 (11–30% cells with membrane expression), 2
(31–60%) or 3 (61–100%) as positive staining for CADM1 or CADM4
expression and tumors with a score of 0 (0–10%) as negative
staining. ER, PgR and HER2 expression levels were evaluated
semi-quantitatively with scores representing the ratio of the
number of positive staining cells compared with negative cells, as
previously described (21).
Assessment of the staining was performed blindly by two independent
investigators, including an experienced pathologist (Dr Akiteru
Goto from Akita University, who is the pathologist and Dr Motonobu
Saito from Fukushima Medical University). Discordance was resolved
by discussion.
Statistical analysis
Statistical analysis was performed using JMP v10
software (SAS Institute, Inc., Cary, NC, USA). The Fisher's exact
test and χ2 test was used to examine the association
between CADM1/4 expression levels and clinicopathological
parameters. The Kaplan-Meier method using GraphPad Prism v6.0
(GraphPad Software, Inc., La Jolla, CA, USA) and log rank test were
used to plot overall survival and cancer specific curves. P<0.05
was considered to indicate a statistically significant
difference.
Results
Patient characteristics and CADM1 and
CADM4 expression levels in breast cancer
CADM1 and CADM4 expression levels were evaluated
using IHC staining in 208 patients with breast cancer (Fig. 1A and B). The characteristics of these
patients are presented in Table I.
This cohort included 33 (16%) patients with triple negative breast
cancer and primarily consisted of stage I and II disease. CADM1
expression was positive in 48 patients (23.1% with scores of 1, 2
or 3) and negative in 160 patients (76.9% with a score of 0). CADM4
expression was positive in 42 patients (20.2%, with scores of 1, 2
or 3) and negative in 166 patients (79.8% with a score of 0;
Table II).
| Table II.CADM1 and CADM4 expression status in
the current cohort. |
Table II.
CADM1 and CADM4 expression status in
the current cohort.
| IHC results | CADM1 | CADM4 |
|---|
| Negative |
|
|
| 0 | 160 | 166 |
| Positive |
|
|
| 1 | 34 | 29 |
| 2 and
3 | 14 | 13 |
Associations between CADM1 and CADM4
expression levels and clinicopathological factors in breast
cancer
CADM1 and CADM4 expression levels were not
associated with age, number of metastatic lymph nodes,
lymphovascular invasion, local recurrence or remote recurrence
(Table III). However, the lack of
expression of CADM4 was significantly reduced in patients who were
ER and PgR negative compared with those who were ER and/or PgR
positive (hormone status; P=0.004). Notably, the lack of expression
of CADM4 was significantly reduced in the triple negative breast
cancer cases compared with other all cases (P=0.008). In addition,
there was a no statistically significant association between CADM1
and CADM4 expression and depth of invasion (pT stage; P=0.041 and
P=0.039, respectively) and pathological stage (P=0.038 and P=0.029,
respectively).
| Table III.Clinicopathological characteristics of
patients with primary breast cancer and expression of CADM1 and
CADM4. |
Table III.
Clinicopathological characteristics of
patients with primary breast cancer and expression of CADM1 and
CADM4.
|
| CADM1, n (%) | CADM4, n (%) |
|---|
|
|
|
|
|---|
| Characteristics | + (n=48) | − (n=160) | P-value | + (n=42) | − (n=166) | P-value |
|---|
| Age (years) |
|
| 0.738 |
|
| 0.857 |
|
<50 | 20 (42) | 62 (39) |
| 14 (33) | 60 (36) |
|
| ≥50 | 28 (58) | 98 (61) |
| 28 (67) | 106 (64) |
|
| Metastatic lymph
nodes |
|
| 0.137 |
|
| 0.083 |
| 0 | 34 (71) | 94 (59) |
| 30 (71) | 99 (60) |
|
|
1–3 | 12 (25) | 44 (28) |
| 11 (26) | 44 (27) |
|
| ≥4 | 2 (4) | 22 (13) |
| 1 (3) | 23 (13) |
|
| Lymphovascular
invasion |
|
| 0.617 |
|
| 0.863 |
| − | 21 (44) | 63 (39) |
| 17 (40) | 70 (42) |
|
| + | 27 (56) | 97 (61) |
| 25 (60) | 96 (58) |
|
| Hormone status |
|
| 0.570 |
|
| 0.004 |
| +/+ or
+/− | 38 (79) | 119 (74) |
| 24 (57) | 133 (80) |
|
|
−/− | 10 (21) | 41 (26) |
| 18 (43) | 33 (20) |
|
| Her2 |
|
| 0.126 |
|
| 1 |
|
Positive | 1 (2) | 15 (9) |
| 3 (7) | 13 (8) |
|
|
Negative | 47 (98) | 145 (91) |
| 39 (93) | 153 (92) |
|
| Triple
negative |
|
| 0.367 |
|
| 0.008 |
|
Yes | 10 (21) | 23 (14) |
| 13 (31) | 20 (12) |
|
| No | 38 (79) | 137 (86) |
| 29 (69) | 146 (88) |
|
| pT stage |
|
| 0.041 |
|
| 0.039 |
| 1 | 35 (73) | 81 (50) |
| 31 (74) | 83 (50) |
|
| 2 | 13 (27) | 70 (44) |
| 10 (24) | 75 (45) |
|
| 3 | 0 | 3 (2) |
| 0 | 3 (2) |
|
| 4 | 0 | 6 (4) |
| 1 (2) | 5 (3) |
|
| Pathological
stage |
|
| 0.038 |
|
| 0.029 |
| I | 26 (54) | 56 (35) |
| 24 (57) | 58 (35) |
|
| II | 22 (46) | 98 (61) |
| 17 (41) | 103 (62) |
|
|
III | 0 | 6 (4) |
| 1 (2) | 5 (3) |
|
| Local
recurrence |
|
| 1 |
|
| 1 |
| − | 47 (98) | 155 (97) |
| 41 (98) | 161 (97) |
|
| + | 1 (2) | 5 (3) |
| 1 (2) | 5 (3) |
|
| Remote
recurrence |
|
| 0.372 |
|
| 0.314 |
| − | 46 (96) | 146 (91) |
| 37 (88) | 156 (94) |
|
| + | 2 (4) | 14 (9) |
| 5 (12) | 10 (6) |
|
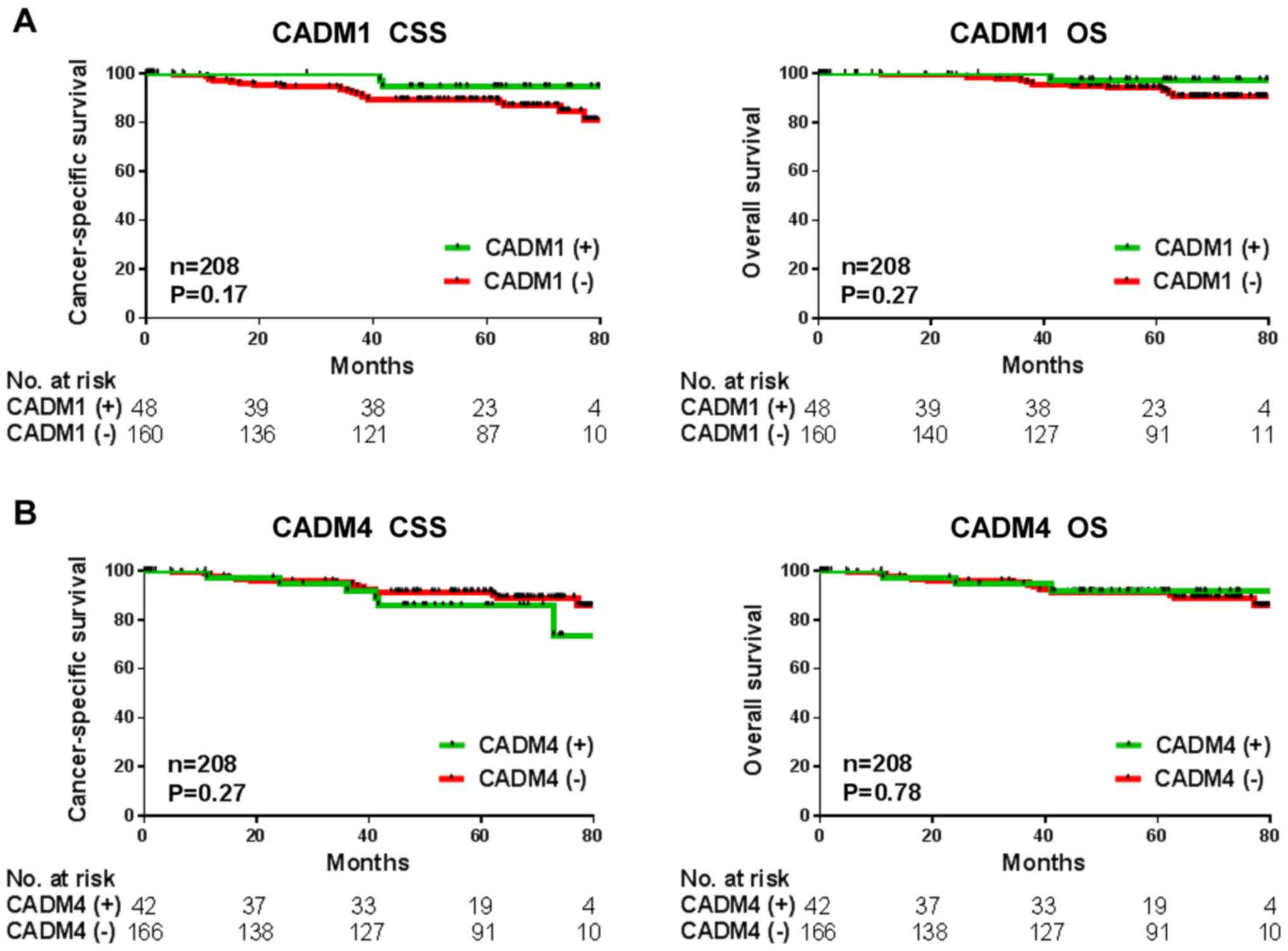
Associations between CADM1 and CADM4
expression levels and prognosis in breast cancer
To investigate whether CADM1 and CADM4 may be a
potential prognostic biomarker in the cohort in the present study,
Kaplan-Meier analysis was performed. Date of tumor recurrence or
mortality were considered the end points for cancer-specific
survival and overall survival rates. The patients with decreased
CADM1 expression levels had poorer cancer-specific and overall
survival rates (P=0.17 and P=0.27, respectively), but this was not
significant in the current cohort (Fig.
2A). There was also no association observed between decreased
CADM4 levels and cancer-specific or overall survival rates (P=0.27
and P=0.78, respectively; Fig.
2B).
Discussion
In the present study, CADM1 and CADM4 expression
levels were evaluated in patients with breast cancer and compared
with clinicopathological factors. The decreased expression levels
of CADM1 and CADM4 were significantly associated with advanced
tumor progression (pT stage and pathological stage) in this breast
cancer cohort (Table III). It has
been reported that decreased expression of CADM1 correlates with
local invasion, lymph node metastasis, lymphovascular invasion
(15) and poor prognosis in breast
cancer (22). In addition, lower
expression of CADM4 also correlates with poor prognosis (17). These previous studies suggest that
CADM1 and CADM4 possess important tumor suppressive roles in breast
cancer and support the results of the current study.
Although inactivation of CADM1 via promoter
methylation has been observed in breast cancer (15), further investigation into the
molecular aspects is required. CADM1 has an important role in tumor
development through suppressing epithelial-mesenchymal transition
and oncogenic signaling (23). In
addition to the current study which demonstrates the loss of CADM1
and CADM4 are associated with breast cancer progression, a recent
study revealed that loss of CADM1 expression was detected in
patients with metastasis compared with those without, suggesting
that CADM1 may serve an important role in preventing the
progression of metastasis (22). As
CADM4 is involved in cell-to-cell adhesion, loss of CADM4 may also
be associated with metastasis through this function. However, the
role of CADM4 in cancer progression remains to be fully elucidated.
Whilst the association between hormone status and CADM1 and CADM4
expression levels remains unknown, the results of the present study
identify that the loss of expression of CADM1 and CADM4 are less
frequent in ER and PgR negative cases, particularly as the loss of
CADM4 expression was not significantly associated with triple
negative breast cancer cases in the present study. Therefore,
further studies are required to investigate these associations.
Biomarkers that are capable of identifying patients
at high risk of relapse following surgical resection may provide
physicians with tools to aid in the diagnosis of cancer recurrence
and administer optimal therapeutic strategies. Previous studies
have demonstrated that CADM1 and CADM4 may be an effective
prognostic biomarker in numerous types of malignant tumor,
including breast cancer (17,22). Loss of CADM1 was significantly
associated with poorer disease free survival and overall survival
rates in patients with breast cancer as well as in a limited number
of ER and PgR-positive patients (22). Furthermore, the loss of CADM4
expression was associated with poorer disease-free survival in
patients with stage I or II breast cancer.
In conclusion, the present study aimed to validate
the use of CADM1 and CADM4 as prognostic biomarkers, but neither
was validated using the current cohort (Fig. 2). Future studies are required to
further inform on this important field of research. The present
study has a number of limitations. Firstly, the patients primarily
had stage I or II breast cancer and this was a small sample size in
this cohort and therefore are not sufficient to enable an effective
analysis of patient prognosis. Secondly, the evaluation of CADM1
and CADM4 protein expression levels used IHC staining only. As
CADM1 expression was regulated by promoter methylation or gene
aberrations, further investigation of these alterations are
required.
References
|
1
|
Katanoda K, Hori M, Matsuda T, Shibata A,
Nishino Y, Hattori M, Soda M, Ioka A, Sobue T and Nishimoto H: An
updated report on the trends in cancer incidence and mortality in
Japan, 1958-2013. Jpn J Clin Oncol. 45:390–401. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chia SK, Speers CH, Bryce CJ, Hayes MM and
Olivotto IA: Ten-year outcomes in a population-based cohort of
node-negative, lymphatic, and vascular invasion-negative early
breast cancers without adjuvant systemic therapies. J Clin Oncol.
22:1630–1637. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cianfrocca M and Goldstein LJ: Prognostic
and predictive factors in early-stage breast cancer. Oncologist.
9:606–616. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hanrahan EO, Valero V, Gonzalez-Angulo AM
and Hortobagyi GN: Prognosis and management of patients with
node-negative invasive breast carcinoma that is 1 cm or smaller in
size (stage 1; T1a, bN0M0): A review of the literature. J Clin
Oncol. 24:2113–2122. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Murakami Y: Involvement of a cell adhesion
molecule, TSLC1/IGSF4, in human oncogenesis. Cancer Sci.
96:543–552. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Murakami Y: Functional cloning of a tumor
suppressor gene, TSLC1, in human non-small cell lung cancer.
Oncogene. 21:6936–6948. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kuramochi M, Fukuhara H, Nobukuni T, Kanbe
T, Maruyama T, Ghosh HP, Pletcher M, Isomura M, Onizuka M, Kitamura
T, et al: TSLC1 is a tumor-suppressor gene in human non-small-cell
lung cancer. Nat Genet. 27:427–430. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Goto A, Niki T, Chi-Pin L, Matsubara D,
Murakami Y, Funata N and Fukayama M: Loss of TSLC1 expression in
lung adenocarcinoma: Relationships with histological subtypes, sex
and prognostic significance. Cancer Sci. 96:480–486. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hui AB, Lo KW, Kwong J, Lam EC, Chan SY,
Chow LS, Chan AS, Teo PM and Huang DP: Epigenetic inactivation of
TSLC1 gene in nasopharyngeal carcinoma. Mol Carcinog. 38:170–178.
2003. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Honda T, Tamura G, Waki T, Jin Z, Sato K,
Motoyama T, Kawata S, Kimura W, Nishizuka S and Murakami Y:
Hypermethylation of the TSLC1 gene promoter in primary gastric
cancers and gastric cancer cell lines. Jpn J Cancer Res.
93:857–860. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jansen M, Fukushima N, Rosty C, Walter K,
Altink R, Heek TV, Hruban R, Offerhaus JG and Goggins M: Aberrant
methylation of the 5′ CpG island of TSLC1 is common in pancreatic
ductal adenocarcinoma and is first manifest in high-grade PanlNs.
Cancer Biol Ther. 1:293–296. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fukuhara H, Kuramochi M, Fukami T,
Kasahara K, Furuhata M, Nobukuni T, Maruyama T, Isogai K, Sekiya T,
Shuin T, et al: Promoter methylation of TSLC1 and tumor suppression
by its gene product in human prostate cancer. Jpn J Cancer Res.
93:605–609. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Steenbergen RD, Kramer D, Braakhuis BJ,
Stern PL, Verheijen RH, Meijer CJ and Snijders PJ: TSLC1 gene
silencing in cervical cancer cell lines and cervical neoplasia. J
Natl Cancer Inst. 96:294–305. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Takahashi Y, Iwai M, Kawai T, Arakawa A,
Ito T, Sakurai-Yageta M, Ito A, Goto A, Saito M, Kasumi F and
Murakami Y: Aberrant expression of tumor suppressors CADM1 and 4.1B
in invasive lesions of primary breast cancer. Breast Cancer.
19:242–252. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jang SM, Han H, Jun YJ, Jang SH, Min KW,
Sim J, Ahn HI, Lee KH, Jang KS and Paik SS: Clinicopathological
significance of CADM4 expression, and its correlation with
expression of E-cadherin and Ki-67 in colorectal adenocarcinomas. J
Clin Pathol. 65:902–906. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jang SM, Sim J, Han H, Ahn HI, Kim H, Yi
K, Jun YJ, Rehman A, Chung MS, Jang K and Paik SS:
Clinicopathological significance of CADM4 expression in invasive
ductal carcinoma of the breast. J Clin Pathol. 66:681–686. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sobin LH and Compton CC: TNM seventh
edition: What's new, what's changed: communication from the
international union against cancer and the American joint committee
on cancer. Cancer. 116:5336–5339. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sobin LH, Gospodarowicz MK and Wittekind
Ch: International Union Against Cancer (UICC) TNM Classification of
Malignant Tumors. 7th. Wiley-Blackwell; Oxford, UK: 2009
|
|
20
|
Nagata M, Sakurai-Yageta M, Yamada D, Goto
A, Ito A, Fukuhara H, Kume H, Morikawa T, Fukayama M, Homma Y and
Murakami Y: Aberrations of a cell adhesion molecule CADM4 in renal
clear cell carcinoma. Int J Cancer. 130:1329–1337. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Saito M, Matsuzaki M, Sakuma T, Katagata
N, Watanabe F, Yamaguchi Y, Schetter AJ, Takenoshita S and Nomizu
T: Clinicopathological study of non-palpable familial breast cancer
detected by screening mammography and diagnosed as DCIS. Breast
Cancer. 21:140–145. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wikman H, Westphal L, Schmid F, Pollari S,
Kropidlowski J, Sielaff-Frimpong B, Glatzel M, Matschke J, Westphal
M, Iljin K, et al: Loss of CADM1 expression is associated with poor
prognosis and brain metastasis in breast cancer patients.
Oncotarget. 5:3076–3087. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Masuda M, Kikuchi S, Maruyama T,
Sakurai-Yageta M, Williams YN, Ghosh HP and Murakami Y: Tumor
suppressor in lung cancer (TSLC)1 suppresses epithelial cell
scattering and tubulogenesis. J Biol Chem. 280:42164–42171. 2005.
View Article : Google Scholar : PubMed/NCBI
|