Introduction
Over 100 different types of liver disease have been
identified in total, including malignant liver cancer, which arises
from tumors that originate in the liver, or originate in another
organ and migrate to the liver. The pathological features of
malignant liver cancer are rapid progression and high mortality
rates, which has been the third leading cause of cancer-associated
mortality worldwide (1); therefore,
it is crucial to identify benign and malignant liver lesions. With
the invention and application of high-field superconducting
magnetic resonance imaging (MRI), in particular the clinical
application of 3.0T MRI, diffusion weighted imaging (DWI) has
significance in differentiating benign and malignant liver lesions
(2). DWI has been observed in a
variety of well-vascularized tissues, including the brain, liver,
pancreas, kidney, muscle, and placenta (3–5). The basic
principle of DWI is to add the symmetric diffusion-sensitive
gradient pulse (b) into conventional spin echo (SE) T2-weighted
scanning sequence. Based on the principles of osmotic water
diffusion, water molecules are activated and migrate towards the
direction of the applied gradient field (6). The greater the b-value, the more severe
the phase dispersion of water molecules, and the more apparent the
signal reduction. If lesions are present in organs, the dispersion
degree of water molecules in normal tissue and lesions will vary,
therefore the degree of signal reduction will be different, thus
facilitating the detection of lesions (7). The b-value scheme also affects the DWI
parameters and the separation between their values in cancer and
normal tissue when the number of b-values is small. In the
diagnosis of liver lesions, DWI imaging may be used as an adjunct
technique to contrast-enhanced MRI, which provides high
sensitivity. The applications of DWI technology based on this
theory are currently more widely reported in liver disease research
(8–11), but its value in diagnosing focal liver
lesions varied among previous studies (12–16). The
purpose of the present study was to employ DW MRI at 3.0T and to
apply different b-values to scan liver lesions, with the aim of
observing DWI features and apparent diffusion coefficient (ADC)
changes of lesions with different characteristics; investigating
the differential diagnostic value of DWI towards benign and
malignant liver lesions.
Materials and methods
Clinical data
A total of 91 patients with liver space-occupying
lesions (145 lesions), were inspected by MRI (Signa 3T HDx; GE
Healthcare, Chicago, IL, USA) at Zhongnan Hospital of Wuhan
University (Wuhan, China) from November 2015 and May 2016. Lesions
were collected from all patients, including 60 males and 31
females, between 26–82 years of age, with an average age of 53
years old. Patients were divided into two groups, according to the
presence of benign or malignant lesions. The malignant lesion group
(M) consisted of 36 patients (26 males and 10 females), including
22 cases (18 males and 4 females) of liver cancer, and 14 cases (8
males and 6 females) of liver metastatic tumor; the benign lesion
group (B) consisted of 55 patients (34 males and 21 females),
including 36 cases (21 males and 9 females) of liver hemangioma, 11
cases (6 males and 5 females) of liver cyst, 5 cases (4 males and 1
female) of focal nodular hyperplasia, and 3 cases (3 males) of
liver abscess. The present study was conducted in accordance with
the declaration of Helsinki. Ethical approval was gained from the
Ethics Committee of Wuhan University (Wuhan, China), and written
informed consent was obtained from all study participants.
Scanning method and scan
sequences
In order to avoid susceptibility artifacts caused by
waste products in organs, each patient was asked to restrict water
and dietary intake for 12 h prior to scanning, and fast on the
morning of inspection. Each patient was placed in the supine
position in the feet-first-to-head scanning order, and the scanning
range covered the entire liver (inferior xiphoid to superior
kidney). Transverse-view T1 weighted imaging (T1WI) and T2 weighted
imaging (T2WI) routine scanning accompanied by routine fat
suppression was performed on all patients. T1WI scanning used the
fast spoiled gradient-echo sequence, repetition time (TR),
4,000–4,500 msec; echo time (TE), 2.4–3.8 msec; and field of view
(FOV) at 32×37-2×37 mm. T2WI scanning used the fast spin echo-XL
sequence, TR, 6,400–6,800 msec; TE, 90.0–92.0 msec; and FOV at
30×30-40×30 mm. infrared-spin-echo echo-planar imaging (SE-EPI) was
used for DWI, with b-values at 500, 1,000, and 1,500
sec/mm2, respectively. For three-time scanning (without
breath holding); thickness 6 mm, layer spacing 2 mm. The layer
varied from 16–20 levels with the b-value changes, and the scanning
time was ~230 sec.
Image processing
The DWI images were automatically processed by
ADW4.4 workstation (GE Healthcare), and ADC values were measured
from the solid part of the layer with the greatest diameter. Cystic
lesions were measured, avoiding cystic fluid, and focusing on the
circular region of interest (ROI), ranging between 100–540
mm2. Particular care was taken to avoid too small or too
large ROI, as too small ROI may involve local liquefaction
necrosis, and too large ROI may include normal tissue. The
measurement was performed three times at different sites, from
which the average was calculated.
Statistical analysis
SPSS 13.0 software (SPSS, Inc., Chicago, IL, USA)
was used for statistical analysis, and the results were expressed
as the mean ± standard deviation. The average ADC values of benign
and malignant space-occupying liver lesions, and the average ADC
values of benign and malignant space-occupying liver lesions with
normal liver (the ratio of lesion to normal liver, RLN), under the
three b-values were compared. The comparison used single-factor
analysis of variance, and the Least-Significant Difference test was
used for post hoc intergroup analysis to compare differences
between groups. The significance level α was 0.05, and P<0.05
was considered to indicate a statistically significant
difference.
Results
Analysis of patient lesions
Amongst the 91 patients, a total of 145 lesions were
identified, including 83 located in the right lobe, 52 located in
the left lobe and 10 located in the caudate lobe. The minimum
lesion diameter was ~8 mm and round in shape; the largest lesion
diameter was ~46 mm with a slightly irregular shape. A total of 39
patients presented with multiple lesions, and the remaining
patients only presented with a single lesion.
MRI performance
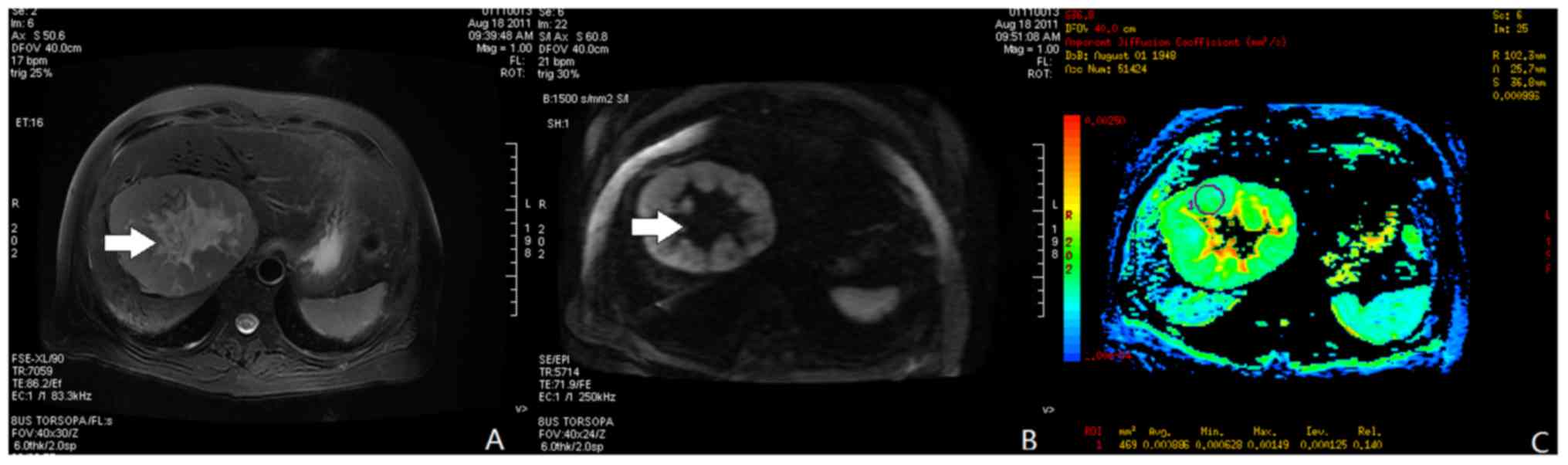
The solid region of primary liver cancer exhibited a
slight low- or iso-intensity signal in T1WI whereas the necrotic
area exhibited a low signal. In T2WI, 11 cases were associated with
partial slight high-intensity signals; 9 with iso-intensity signals
and 2 with a circular shadow of low-intensity signals (Fig. 1). The majority of tumors exhibited
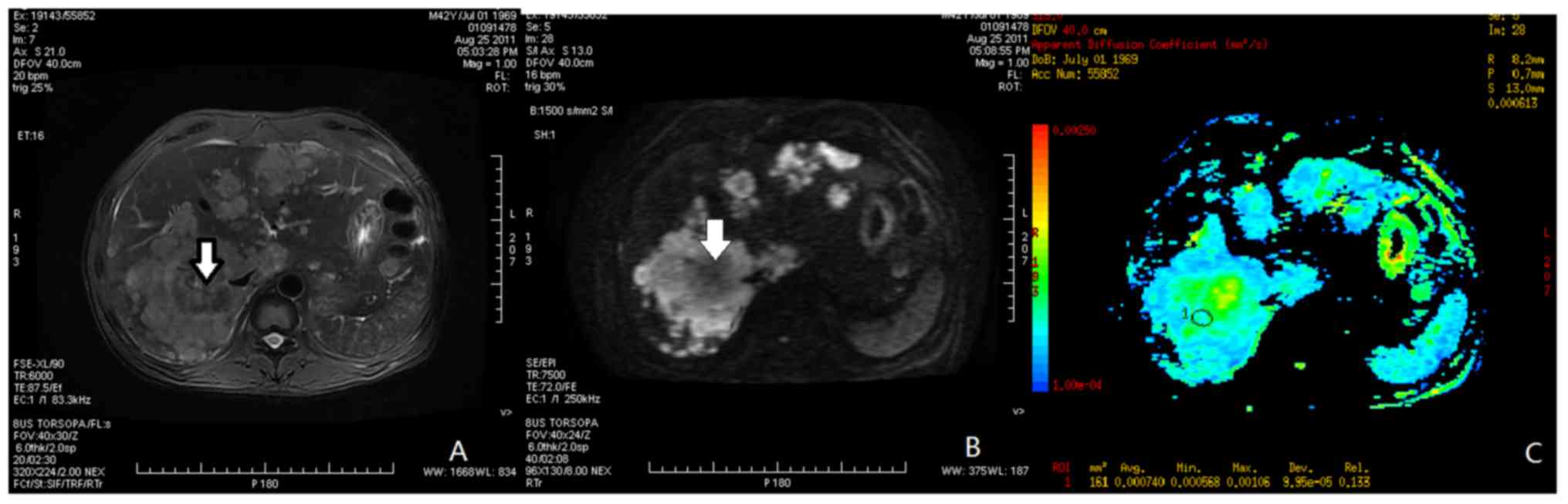
slight high-intensity signals in DWI. The majority of liver
metastatic tumors demonstrated multiple oval low-intensity signals
in T1WI, and high-intensity signals in T2WI. Partial high- and
low-intensity signals may appear in DWI. The enhanced scanning
revealed peripheral enhancement. Liver cysts revealed low intensity
signals in T1WI, and significantly high-intensity signals in T2WI
(Fig. 2). Hepatic hemangiomas
demonstrated low-intensity signals in T1WI, which were higher than
in liver cysts, and ‘light-bulb signs’ high-intensity signals in
T2WI (Fig. 3). In DWI,
higher-than-liver-parenchyma signals were observed. Focal nodular
hyperplasia demonstrated higher-than-liver-parenchyma signals in
T1WI, and iso-intensity signals in T2WI, together with partial
high-intensity signals (Fig. 4). In
DWI, it revealed slight high-intensity signals. The 22 cases of
primary hepatocellular exhibited iso-or hypo-signals with
hypo-signals in cystic necrotic areas on T1W1, demonstrated
hyper-signals (11 cases), iso-signals (9 cases), a circular shadow
of low-intensity signals (2 cases), circular hypo-signals on T2W1
and demonstrated slightly hyper-signals (20 cases), iso-signals (2
cases) or iso-signals on DWI. The 14 cases of liver metastases
exhibited multiple circular hypo-signals (12 cases) or slightly
circular hyper-signals (2 cases) on T1WI, multiple circular
hyper-signals on T2WI and hyper-signals (11 cases) and iso-or
hypo-signals on DWI; which all showed annular enhancement in the
enhanced scan. The hepatic cysts demonstrated hypo-signals on T1W1,
hyper-signals on T2W1, hypo-signals (11 cases) and slightly
hyper-signals (1 case) on DWI. Hepatic hemangioma presented
hypo-signals on T1W1, which was higher than cyst, and presented
hyper-signal on T2W1, called ‘Bulb sign’; higher than liver
parenchyma of signals on DWI. Hepatic focal nodular hyperplasia (5
cases) presented higher signals than liver parenchyma on T1W1,
iso-signals (4 cases) and hyper-signals (1 case) on T2W1, slightly
hyper-signals on DWI (Figs.
1–4).
Measurements of ADC values
Statistical analyses of ADC values between liver
cancer compared with liver metastatic tumors within the three
b-value groups (500, 1,000 and 1,500 sec/mm2)
demonstrated statistical significance differences (P<0.05;
Table I). However, in the low b-value
group (b=500 sec/mm2), the ADC values were significantly
different between malignant lesions, including liver cancer and
liver cysts (P<0.05). ADC values between liver cancer and other
malignant lesions, including liver hemangioma, focal nodular
hyperplasia (FNH), and hepatic abscesses, revealed no significant
differences (P>0.05; Table II),
In the middle b-value group (b=1,000 sec/mm2), ADC
values were significantly different between liver cancer and liver
cysts and between liver hemangioma and liver abscesses (P<0.05;
Table II). Furthermore, ADC values
between liver metastatic tumors and liver cysts, liver hemangioma,
or liver abscesses were also statistically significant (P<0.05;
Table II). In the high b-value group
(b=1,500 sec/mm2), the ADC values were significantly
different between liver cancer and liver cysts or liver hemangioma
(P<0.05), and those between liver metastatic tumor and liver
cysts or hepatic hemangioma were also statistically significant
(P<0.05). Due to a lack of non-representative samples,
statistical analysis of the differences between liver abscesses and
FNH was not performed.
 | Table I.Comparison of mean ADC values between
benign and malignant lesions with different b-values in diffusion
weighted imaging. |
Table I.
Comparison of mean ADC values between
benign and malignant lesions with different b-values in diffusion
weighted imaging.
|
| ADC of malignant
lesions (×10−3 mm2/sec) | ADC of benign lesions
(×10−3 mm2/sec) |
|
|---|
|
|
|
|
|
|---|
| b
(sec/mm2) | Primary liver
cancer | Liver metastatic
tumor | Hepatic
hemangioma | Liver cyst | P-value |
|---|
| 500 | 2.36±0.41 | 2.46±0.57 | 2.59±0.63 | 2.92±0.74 | <0.05 |
| 1,000 | 1.99±0.62 | 2.17±0.42 | 2.23±0.41 | 2.51±0.61 | <0.05 |
| 1,500 | 1.79±0.67 | 1.89±0.78 | 2.05±0.55 | 2.48±0.41 | <0.01 |
| Table II.ADC values of benign and malignant
lesions in diffusion weighted imaging with different b-values. |
Table II.
ADC values of benign and malignant
lesions in diffusion weighted imaging with different b-values.
|
| ADC values of
malignant lesions | ADC values of benign
lesions |
|
|---|
|
|
|
|
|
|---|
| b | Primary liver
cancer | Liver metastatic
tumor | Hepatic
hemangioma | Liver cyst | FNH | Liver abscess | P-value |
|---|
| 500 | 1.45±0.46 | 1.47±0.33 | 1.56±0.45 | 1.86±0.64 | 2.48±0.66 | 1.52±0.24 |
>0.05 |
| 1,000 | 1.44±0.45 | 1.61±0.49 | 1.77±0.36 | 1.97±0.58 | 2.18±0.52 | 1.75±0.36 | P<0.05 |
| 1,500 | 1.48±0.46 | 1.54±0.39 | 1.82±0.61 | 1.88±0.52 | 1.96±0.56 | 1.77±0.61 | P<0.05 |
Within all three b-value groups, including the low
b-value group (b=500 sec/mm2), the middle b-value group
(b=1,000 sec/mm2) and the high b-value group (b=1,500
sec/mm2) the ADC values were significantly different
between liver cancer compared with benign lesions in all groups at
(P<0.05, P<0.05 and P<0.01), respectively (Table I). The comparison of ADC values of
liver space-occupying lesions with normal liver tissue under
different b-values is presented in Table
II.
The statistical analysis revealed that among the
three b-value groups, in the low b-value group (b=500
sec/mm2), the ADC value differences between malignant
and benign lesions were statistically significant (P<0.05); in
the middle b-value group (b=1,000 sec/mm2), the ADC
value differences between malignant and benign lesions were
statistically significant (P<0.05); in the high b-value group
(b=1,500 sec/mm2), the ADC value differences between
malignant and benign lesions were statistically significant
(P<0.05).
Discussion
The aim of the present study was to investigate the
MRI analysis of malignant and benign liver lesions and normal liver
parenchyma. In previous years, with the rapid development and
improvement of MRI technologies, and particularly the wide
application of SE-EPI detection technology, it is possible to
suppress or reduce artifacts caused by physiological motions.
Therefore, DWI is able to be effectively used for the diagnosis of
liver space-occupying lesions. DWI is a noninvasive method to study
the micro-motions of water molecules (17), and may provide further diagnostic
information than conventional T1WI and T2WI. This further allows
for research on specific aspects of the human body at the
micro-level and reflects the spatial organization of human tissue,
in addition to the functional status of water molecule exchange
among different organs under physiological and pathological
conditions. The current application of DWI has been confirmed in
the central nervous system (18,19), and
the application of DW1 to investigate other parts of the human
body. The primary purpose of the present study was to evaluate the
application values of DWI and ADC in diagnosing primary liver
cancer and liver metastatic tumors.
Different b-values have important impacts on DWI and
ADC values, and the selection of a b-value may determine the size
of ADC value (20). In the present
study, three different b-values (500, 1,000, and 1,500
sec/mm2) were used for the measurement. Analysis of the
results revealed that the lower the b-value, the greater the ADC
value, and the lower the diffusion weighted signals. In addition,
the higher the b-value, the smaller the ADC value, and the higher
the diffusion weighted signals, at which point the ADC value is
more accurate and closer to the actual D value. However, a higher
b-value requires an increased TE value during scanning, and thus
the signal attenuation is more apparent, and at times it may prove
difficult to view the images (21).
As for the selection of the b-value in DWI towards liver lesions,
multiple scholars have obtained different results. A previous study
has demonstrated that the b-values within 500–750
sec/mm2 were more appropriate (22). Vandecaveye et al (23) considered a b-value of 500
sec/mm2 to be more appropriate. Another previous study
reported that when the b-value reached 1,000 sec/mm2 or
above, the liver signal attenuation was particularly apparent
(24). The results from the present
study demonstrated that when the b-value was set at 1,000
sec/mm2, the liver signals demonstrated no significant
attenuation. However, when the b-value was set at 1,500
sec/mm2, liver signals in specific cases demonstrated
notable attenuation. Notably, in the middle b-value group, in the
present study, the differences between liver cysts, liver
hemangiomas, liver abscesses, and liver malignant lesions were
significant. However, the results in the low- and high b-value
groups, with ADC values measured under b=1,000 sec/mm2
may be more conducive towards the characteristic differentiation of
liver space-occupying lesions, consistent with the results of
Bruegel et al (25). It is
hypothesized that the reasons for the above discrepancies may be
caused by different field intensities and settings in different
studies, yet the specific reasons and the rational range of the
b-value still warrants further study.
It was observed throughout the present study that,
due to the characteristic differences between benign and malignant
liver lesions, the ADC values also differed, with significantly
higher ADC values detected for benign lesions compared with
malignant lesions. Thus, its mechanisms may be associated with the
pathological phenotype and biochemical component changes which
occur in these lesions (26).
Statistical analysis revealed that the different ADC values
observed between benign liver lesions including liver cysts, liver
hemangiomas, and liver abscesses (in the middle b-value group;
excluding FNH), and malignant lesions including liver cancer, were
statistically significant. As DWI uses the diffusion of water
molecules inside lesions to diagnose diseases, and due to the
tissue component differences in various diseases, the free water
content may also be different. The majority of lesions of primary
liver cancer and liver metastatic tumors are solid lesions (partial
lesions appear as central necrosis, and the ROI points selected in
the present study all avoided the cystic necrosis area), lesions
may have less free water, making diffusion slow, resulting in a
decreased ADC value. Hepatic hemangioma is mainly composed of blood
sinusoids and fibrous interval, and because blood sinusoids are
full of blood, the physiological movement of water molecules is
relatively free and water is able to diffuse rapidly. Therefore,
the ADC values obtained are significantly increased compared with
those obtained in hepatocellular carcinoma (27). Thus, DWI has a significant value in
determining benign and malignant liver space-occupying lesions
(28,29), and may further be used to clarify,
differentiate, and diagnose malignant and benign liver lesions. In
addition, it also provides a noninvasive and reliable clinical
adjuvant diagnosis method.
The comparison of ADC values between benign and
malignant liver lesions with normal liver parenchyma is named ratio
of lesion to normal liver (RLN). Due to patients' individual
differences, disease status, size and location of ROI, and
different operators, patients may exhibit a wide variation in ADC
values even if the b-value is the same. The use of RLN may reduce
the individual differences between patients' characteristics,
including height and weight, but no data demonstrating that RLN is
able to distinguish liver malignant tumors and benign lesions has
been identified in previous years. In the present study, RLN
<1.6 was set as the threshold, and the results indicated that
the sensitivity, specificity, and accuracy calculated under high
b-values were higher than those calculated under low b-values. When
compared with the settings using ADC <1.65×10−3
mm2/sec as the threshold, the specificities obtained
under high b-values were higher than the latter, but the
sensitivities and accuracies were decreased. Therefore, the
combination of the two may contribute to improving the
identification ability of ADC values towards benign and malignant
liver lesions. The results of the present study demonstrated that
the differences in RLN between malignant and benign liver lesions
were statistically significant, demonstrating more value in
differentially diagnosing the features of liver space-occupying
lesions than when simply using the ADC values.
Although MRI is expensive and not the preferred
method of diagnosis at present, it has a number of advantages as an
effective means for identifying suspicious liver space-occupying
lesions. MRI is a noninvasive method adopting high soft tissue
resolution, multi-dimensional imaging, and large scanning field,
which also identifies adjacent organ invasion and large-range lymph
node metastasis. The development of MRI, together with advances in
technology in the computer field, the constant improvement of
processing skills, the gradual maturation of coil theories, and the
innovations of imaging sequence and post-processing methods has
demonstrated considerable progress. Such progress is connected with
the research directions of actual clinical needs, and the potential
for MRI to be promoted in clinics, thus benefiting more patients
with cancer.
To conclude, it was observed that liver
space-occupying lesions demonstrate different DWI features and ADC
ranges, and DWI accurately determines the nature of lesions, thus
exhibiting significance towards the identification of liver benign
and malignant space-occupying lesions.
Acknowledgements
The present study was funded by the National Natural
Science Foundation of China (grant nos. 81171315, 81227902).
References
|
1
|
Shibata T and Aburatani H: Exploration of
liver cancer genomes. Nat Rev Gastroenterol Hepatol. 11:340–349.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parikh T, Drew SJ, Lee VS, Wong S, Hecht
EM, Babb JS and Taouli B: Focal liver lesion detection and
characterization with diffusion-weighted MR imaging: Comparison
with standard breath-hold T2-weighted imaging. Radiolgy.
246:812–822. 2008.
|
|
3
|
Ma J Evidence-based guideline: The role of
diffusion and perfusion MRI for the diagnosis of acute ischemic
stroke: explanation and viewpoint. Chin J Magn Resonan Imag.
1:324–329. 2010.
|
|
4
|
Huang BC, Zhan SH, Geng DY, et al:
Diffusion weighted imaging features after hepatic right portal vein
ligation in rats. Chin J Magn Reson Imaging. 1–59. 2010.
|
|
5
|
Naminoto T, Yamashita Y, Sumi S, Tang Y
and Takahashi M: Focal liver masses: Characterization with
diffusion-weighted echoplanar MR imaging. Radiology. 204:739–744.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Koh DM, Collins DJ and Orton MR:
Intravoxel incoherent motion in body diffusion-weighted MRI:
Reality and challenges. AJR Am J Roentgenol. 196:1351–1361. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lewis S, Dyvorne H, Cui Y and Taouli B:
Diffusion-weighted imaging of the liver: Techniques and
applications. Magn Reson Imaging Clin N Am. 22:373–395. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hu G, Chan Q, Quan X, Zhang X, Li Y, Zhong
X and Lin X: Intravoxel incoherent motion MRI evaluation for the
staging of liver fibrosis in a rat model. J Magn Reson Imaging.
42:331–339. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chung SR, Lee SS, Kim N, Yu ES, Kim E,
Kühn B and Kim IS: Intravoxel incoherent motion MRI for liver
fibrosis assessment: A pilot study. Acta Radiol. 56:1428–1436.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Joo I, Lee JM, Grimm R, Han JK and Choi
BI: Monitoring vascular disrupting therapy in a rabbit liver tumor
model: Relationship between tumor perfusion parameters at IVIM
diffusion-weighted MR imaging and those at dynamic
contrast-enhanced MR imaging. Radiology. 278:104–113. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Park YS, Lee CH, Kim JH, Kim IS, Kiefer B,
Seo TS, Kim KA and Park CM: Using intravoxel incoherent motion
(IVIM) MR imaging to predict lipiodol uptake in patients with
hepatocellular carcinoma following transcatheter arterial
chemoembolization: A preliminary result. Magn Reson Imaging.
32:638–646. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang M, Li X, Zou J, Chen X, Chen S and
Xiang W: Evaluation of hepatic tumors using intravoxel incoherent
motion diffusion-weighted MRI. Med Sci Monit. 22:702–709. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Doblas S, Wagner M, Leitao HS, Daire JL,
Sinkus R, Vilgrain V and Van Beers BE: Determination of malignancy
and characterization of hepatic tumor type with diffusion-weighted
magnetic resonance imaging: Comparison of apparent diffusion
coefficient and intravoxel incoherent motion-derived measurements.
Invest Radiol. 48:722–728. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Watanabe H, Kanematsu M, Goshima S, Kajita
K, Kawada H, Noda Y, Tatahashi Y, Kawai N, Kondo H and Moriyama N:
Characterizing focal hepatic lesions by free-breathing intravoxel
incoherent motion MRI at 3.0 T. Acta Radiol. 55:1166–1173. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Colagrande S, Regini F, Pasquinelli F,
Mazzoni LN, Mungai F, Filippone A and Grazioli L: Focal liver
lesion classification and characterization in noncirrhotic liver: a
prospective comparison of diffusion-weighted magnetic
resonance-related parameters. J Comput Assist Tomogr. 37:560–567.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhu L, Cheng Q, Luo W, Bao L and Guo G: A
comparative study of apparent diffusion coefficient and intravoxel
incoherent motion-derived parameters for the characterization of
common solid hepatic tumors. Acta Radiol. 56:1411–1418. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kandpal H, Sharma R, Madhusudhan KS and
Kapoor KS: Respiratory-triggered versus breath-hold
diffusion-weighted MRI of liver lesions: Comparison of image
quality and apparent diffusion coefficient values. AJR Am J
Roentgenol. 192:915–922. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jungmann PM, Baum T, Schaeffeler C,
Sauerschnig M, Brucker PU, Mann A, Ganter C, Bieri O, Rummeny EJ,
Woertler K and Bauer JS: 3.0T MR imaging of the ankle: Axial
traction for morphological cartilage evaluation, quantitative T2
mapping and cartilage diffusion imaging-A preliminary study. Eur J
Radiol. 84:1546–1554. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tang Y, Wang H, Wang Y, Li J, Jia R, Ma L
and Ye H: Quantitative comparison of MR diffusion-weighted imaging
for liver focal lesions between 3.0T and 1.5T: Regions of interest
of the minimum-spot ADC, the largest possible solid part and the
maximum diameter in lesions. J Magn Reson Imaging. 44:1320–1329.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gourtsoyianni S, Papanikolaou N,
Yarmenitis S, Maris T, Karantanas A and Gourtsoyiannis N:
Respiratory gated diffusion-weighted imaging of the liver: Value of
apparent diffusion coefficient measurements in the differentiation
between most commonly encountered benign and malignant focal liver
lesions. Eur Radiol. 18:486–492. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kakite S, Hadrien D, Besa C, Cooper N,
Facciuto M, Donnerhack C and Taouli B: Hepatocellular carcinoma:
Short-term reproducibility of apparent diffusion coefficient and
intravoxel incoherent motion parameters at 3.0T. J Magn Reson
Imaging. 41:149–156. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yoshikawa T, Kawamitsu H, Mitchell DG,
Ohno Y, Ku Y, Seo Y, Fujii M and Sugimura K: ADC measurement of
abdominal organs and lesions using parallel imaging technique. AJR
Am J Roentgenol. 187:1521–1530. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vandecaveye V, De Keyzer F, Verslype C, Op
de Beeck K, Komuta M, Topal B, Roebben I, Bielen D, Roskams T,
Nevens F and Dymarkowski S: Diffusion-weighted MRI provides
additional value to conventional dynamic contrast-enhanced MRI for
detection of hepatocellular carcinoma. Eur Radiol. 19:2456–2466.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Taouli B, Vilgrain V, Dumont E, Daire JL,
Fan B and Menu Y: Evaluation of liver diffusion isotropy and
characterization of focal hepatic lesions with two single-shot
echo-planar MR imaging sequences: Prospective study in 66 patients.
Radiology. 226:71–78. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bruegel M, Holzapfel K, Gaa J, Woertler K,
Waldt S, Kiefer B, Stemmer A, Ganter C and Rummeny EJ:
Characterization of focal liver lesions by ADC measurements using a
respiratory triggered diffusion-weighted single-shot echo-planar MR
imaging technique. Eur Radiol. 18:477–485. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ma C, Liu L, Li J, Wang L, Chen LG, Zhang
Y, Chen SY and Lu JP: Apparent diffusion coefficient (ADC)
measurements in pancreatic adenocarcinoma: A preliminary study of
the effect of region of interest on ADC values and interobserver
variability. J Magn Reson Imaging. 43:407–413. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bruegel M, Muenzel D, Waldt S, Specht K
and Rummeny EJ: Hepatic epithelioid hemangioendothelioma: Findings
at CT and MRI including preliminary observations at
diffusion-weighted echo-planar imaging. Abdom Imaging. 36:415–424.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ertas G, Onaygil C, Akin Y, Kaya H and
Aribal E: Quantitative differentiation of breast lesions at 3T
diffusion-weighted imaging (DWI) using the ratio of distributed
diffusion coefficient (DDC). J Magn Reson Imaging. 44:1633–1641.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Erturk SM, Ichikawa T, Sano K, Motosugi U,
Sou H and Araki T: Diffusion-weighted magnetic resonance imaging
for characterization of focal liver masses: Impact of parallel
imaging (SENSE) and b value. J Comput Assist Tomogr. 32:865–871.
2008. View Article : Google Scholar : PubMed/NCBI
|