Introduction
Esophageal carcinosarcoma (ECS) is a rare type of
esophageal cancer that was designated as such by Virchow et
al (1) due to the presence of
carcinomatous and sarcomatous components. The components consist of
spindles or polymorphous tumor cells with a mesenchymal character.
This tumor often presents with polypoid growth with a stalk, and is
characterized by the presence of esophageal squamous cell carcinoma
(ESCC) in situ surrounding the stalk (2). It has been suggested that the sarcoma
component is derived from SCC (3–5).
Epithelial-mesenchymal transition (EMT) has been
reported as an important means of tumor invasion and metastasis in
numerous types of canonical cancer (6,7). Zinc
finger E-box-binding homeobox 1 (ZEB1) is associated with EMT
transcription factors (8). Members of
the microRNA (miR)-200 family have been reported to serve an
important role in dysregulating the epithelial phenotype by
targeting ZEB factors, thereby preventing E-cadherin downregulation
and resulting in EMT (9). In human
cancer, ZEB1 expression has been indicated to be increased when
miR-200 expression is decreased due to promoter DNA methylation
(10,11). The EMT activator ZEB1, in particular,
has also been indicated to confer stemness and resistance to
anticancer treatment (9). ZEB1 was
specifically recognized in the sarcoma component compared with the
carcinoma component in spindle cell carcinoma of the esophagus,
among which a number of ECS cases were included (8). To the best of our knowledge, information
regarding ZEB1 expression in ECS is limited.
In the present study, the aim was to clarify the
molecular features associated with prognosis by comparing the
clinicopathological factors and prognosis of ECS and ESCC in
pT1.
Materials and methods
Patients and data collection
Esophagectomy was performed in 325 patients with
esophageal tumors at Kitasato University Hospital (Sagamihara,
Japan) between January 2004 and December 2014, and 5 male and 1
female patient (1.8%), with a mean age of 68 years (range, 60–77
years), were diagnosed with ECS. The present study was conducted in
accordance with the Declaration of Helsinki and approved by the
Research Ethics Committee of Kitasato University School of Medicine
(Sagamihara, Japan). Written consent was obtained from all
patients. All tissue samples were collected at the Kitasato
University Hospital. The clinical and pathological features were
analyzed and tumor stage was classified according to the 6th
edition of the Union for International Cancer Control
Tumor-Node-Metastasis (UICC-TNM 6th edition) staging system of
esophageal cancer (12). The median
follow-up time was 29 months (range, 16–33 months).
Immunohistochemical staining
Serial tissues sections (4-µm thick) were fixed in
10% formalin at room temperature for 16–24 h and embedded in
paraffin. The slices were incubated with 3%
H2O2 at room temperature for 5 min to
deactivate endogenous peroxidase and subsequently washed with PBS.
Rabbit anti-human ZEB1 polyclonal antibody (dilution 1:100; cat.
no. HPA027524; Atlas Antibodies AB, Stockholm, Sweden), rabbit
Snail 1 polyclonal antibody (dilution, 1:500; cat. no. GTX125918;
Gene Tex, Los Angeles, USA) and rabbit Twist-related protein 1
(Twist 1) polyclonal antibody (dilution, 1:500; cat. no. ab50581;
Abcam, Cambridge, UK) were added, and the slices were incubated at
4°C overnight. Immune complexes were amplified using a Vectastain
Universal Elite ABC kit (dilution, 1:50; cat. no. PK-6200; Vector
Laboratories, Inc., Burlingame, CA, USA), at room temperature for
10 min, according to the manufacturer's protocols. These complexes
were subsequently detected by incubation at room temperature with
the chromogen 3,3′-diaminobenzidine (3%) for 1 min. The invasive
front of the carcinoma components and the sarcomatous areas were
compared. Using a light microscope (Olympus AX80; Olympus
Corporation, Tokyo, Japan) (×20 magnification), positive staining
was defined as nuclear immunoreactivity in neoplastic cells.
Hematoxylin at 0.1% concentration was used to stain at room
temperature for 5 min, then 0.025% eosin was used to stain at room
temperature for 3 min. As a control tissue of ZEB1 in the present
study, according to the study by Kikuchi et al (13), mammary gland tissues were also
stained. Triple-negative breast cancer tissues demonstrating the
strongest staining were used as a positive control, whereas normal
breast tissues that did exhibit staining were used as a negative
control (13). The positive and
negative controls were primary tumors and the corresponding
non-cancerous tissues from 3 patients with triple-negative invasive
breast cancer who all underwent a partial resection of the breast
in September 1999 at Kitasato University Hospital. Based on
previous studies (14–17), gastric adenocarcinoma tissues with
confirmed staining were used as a positive control for Twist 1 and
Snail 1, while a non-cancerous mucosa sample was used as the
negative control. The positive and negative controls were primary
tumors and the corresponding non-cancerous tissues from 3 patients
with macroscopic type 0–IIc early gastric cancer who underwent
laparoscopic gastrectomy in October and November, 2016, and
November 2005, respectively, at Kitasato University Hospital.
Statistical analysis
All statistical analyses were performed using
JMP® 11.0 software (SAS Institute Inc., Cary, NC, USA).
Frequency tables were analyzed using the χ2 test, while
the significance of categorical variables was evaluated with the
likelihood ratio. Disease-specific survival was measured from the
date of diagnosis to the time of patient mortality due to a
specific disease, or censored at the date of the last follow-up
evaluation. For evaluation of relapse-free survival, recurrence was
defined as development of local recurrence, distant metastasis or
patient mortality from ECS (whichever occurred first). Survival
functions were estimated by life tables and the Kaplan-Meier
method, and compared by log-rank test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics
The characteristics of the patients with ECS are
indicated in Table I. The mean age
was 68 years. With the exception of 1 unknown case, all patients
had a history of smoking and drinking. The main symptoms reported
were difficulty in swallowing, coughing and chest pain in 3, 2 and
1 case, respectively. All cases had an American Society of
Anesthesiologists-Physical Status of ≤2 (18). All patients underwent computed
tomography, and 5 patients underwent upper gastrointestinal
contrast studies. Regarding clinical T stage (cT), cT1, cT2, cT3
and cT4 were indicated in 1, 1, 3 and 1 case, respectively
(Fig. 1). The longitudinal length of
the tumor was 2.5–10.5 cm (mean, 6.5 cm). Pathological T stage (pT)
was eventually diagnosed as pT1 in all cases. According to Japanese
Classification of Esophageal Cancer 11th Edition (2), the final pathological morphological type
was pedunculated type, sessile (broad based) type, and pedunculated
and slightly elevated type in 4, 1, and 1 cases, respectively. All
patients underwent radical surgery with complete tumor
resection.
 | Table I.Characteristic of patients with
esophageal carcinoma. |
Table I.
Characteristic of patients with
esophageal carcinoma.
| Variables | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 |
|---|
| Sex | Male | Female | Male | Male | Male | Male |
| Age, years | 61 | 60 | 73 | 77 | 68 | 71 |
| Smoking status | Former | Unknown | Current | Current | Current | Former |
| Chief
complaint | Chest pain | Dysphagia | Cough | Cough | Dysphagia | Dysphagia |
| Location | Mt | Mt | Lt | Ut | Mt | Mt |
| Clinical T
factor | cT4 | cT3 | cT3 | cT3 | cT2 | cT1 |
| Albumin level,
g/dl | 4.1 | 4 | 3.3 | 3.3 | 3.4 | 3.4 |
| Neutrophil to
lymphocyte ratio | 3 | 2.9 | 1.7 | 2.4 | 6.9 | 6.6 |
| ASA-PS | Class 1 | Class 1 | Class 2 | Class 1 | Class 1 | Class 2 |
| Tumor length,
cm | 2.5 | 10.5 | 4.5 | 6.5 | 8.5 | 6.6 |
| Macroscopic
type | 0–Ip | 0–Ip | 0–Ip | 0–Isp | 0–Ip+IIa | 0–Ip |
| Lymphatic
invasion | Unknown | 2 | 0 | 0 | 1 | 0 |
| Venous
invasion | Unknown | 2 | 0 | 0 | 1 | 0 |
| pT factor | pT1 | pT1 | pT1 | pT1 | pT1 | pT1 |
| pN factor | pN0 | pN1 | pN0 | pN0 | pN1 | pN0 |
| Immunohistochemical
findings | Unknown | Vimentin(+) | Vimentin(+) | G-CSF(+) | Vimentin(+) | Vimentin(+) |
| Initial
treatment | NF + RT +
Resection | Resection + NF +
RT | Resection | Resection | Resection | Resection |
| Tumor
recurrence | No | Yes | No | Yes | Yes | No |
| Treatment following
recurrence | None | 5-FU + cisplatin,
irinotecan + cisplatin | None | 5-FU + | BSC cisplatin | None |
| Prognosis | Alive | Succumbed to
tumor | Succumbed to
AMI | Succumbed to
tumor | Succumbed to
tumor | Alive |
Patient 1 received preoperative chemoradiotherapy
(CRT), where radiotherapy was applied at 40 Gy due to suspected
tracheal invasion (cT4). The CRT therapy included radiotherapy
concurrent with nedaplatin + 5-fluorouracil (FU) chemotherapy due
to renal dysfunction. Nedaplatin + 5-FU chemotherapy consisted of
two courses of chemotherapy with 5-fluorouracil (800
mg/m2 on days 1–5) and nedaplatin (90 mg/m2
on day 1) every 4 weeks. Postoperative adjuvant CRT was performed
in patient 2 due to vigorous vascular invasion and lymph node
metastasis in the pathological results, and chemotherapy
[nedaplatin (50 mg/m2 on day 1) + 5-FU (400
mg/m2 on days 1–5)] was additionally used due to renal
dysfunction. The pathological depth of invasion was pT1 in all
cases, and there was a large discrepancy between clinically
diagnosed depth of tumor invasion prior to surgery and depth of
tumor invasion following surgery. Lymph node metastasis was
indicated in 2 cases. Postoperative complications included
hoarseness due to recurrent laryngeal nerve paralysis in 3 cases,
and anastomotic leakage [Clavien-Dindo classification (19) grade IIIa], which caused a
gastrointestinal tract to lung fistula, in 1 case. Postoperative
recurrence was observed in 3 cases despite the superficial depth of
invasion in all cases. The 3 patients with recurrence succumbed at
20, 28, and 32 months due to the progression of recurrence in the
lymph nodes, liver and lungs/bones, respectively. Patient 2, in
particular, presented with multiple lung metastases and fifth rib
metastasis at 16 months post-surgery, despite preoperative adjuvant
CRT. Despite administration of 8 courses of cisplatin (15
mg/m2 on day 1) + 5-FU (750 mg/m2 on days
1–5) and 1 course of cisplatin (90 mg/m2 on day 1) +
irinotecan (75 mg/m2 on day 1), the patient succumbed at
32 months post-surgery. Patient 4 presented with ECS with pT1
(UICC-TNM 6th edition) lymph node metastasis 0, lymphatic invasion
0, venous invasion 0 and granulocyte colony-stimulation
factor-positive tumor cells in the immunohistochemical analysis.
This patient experienced recurrence of lymph node metastasis at 6
months post-surgery, and despite administration of 8 courses of
cisplatin (60 mg/m2 on day 1) + 5-FU (800
mg/m2 on days 1–5), the patient additionally developed
brain metastasis and succumbed at 20 months post-surgery. Patient 5
presented with liver metastasis at 23 months post-surgery and
additionally developed pleural dissemination, lung metastasis and
para-aortic lymph node metastasis at 26 months post-surgery. The
patient succumbed 2 months later.
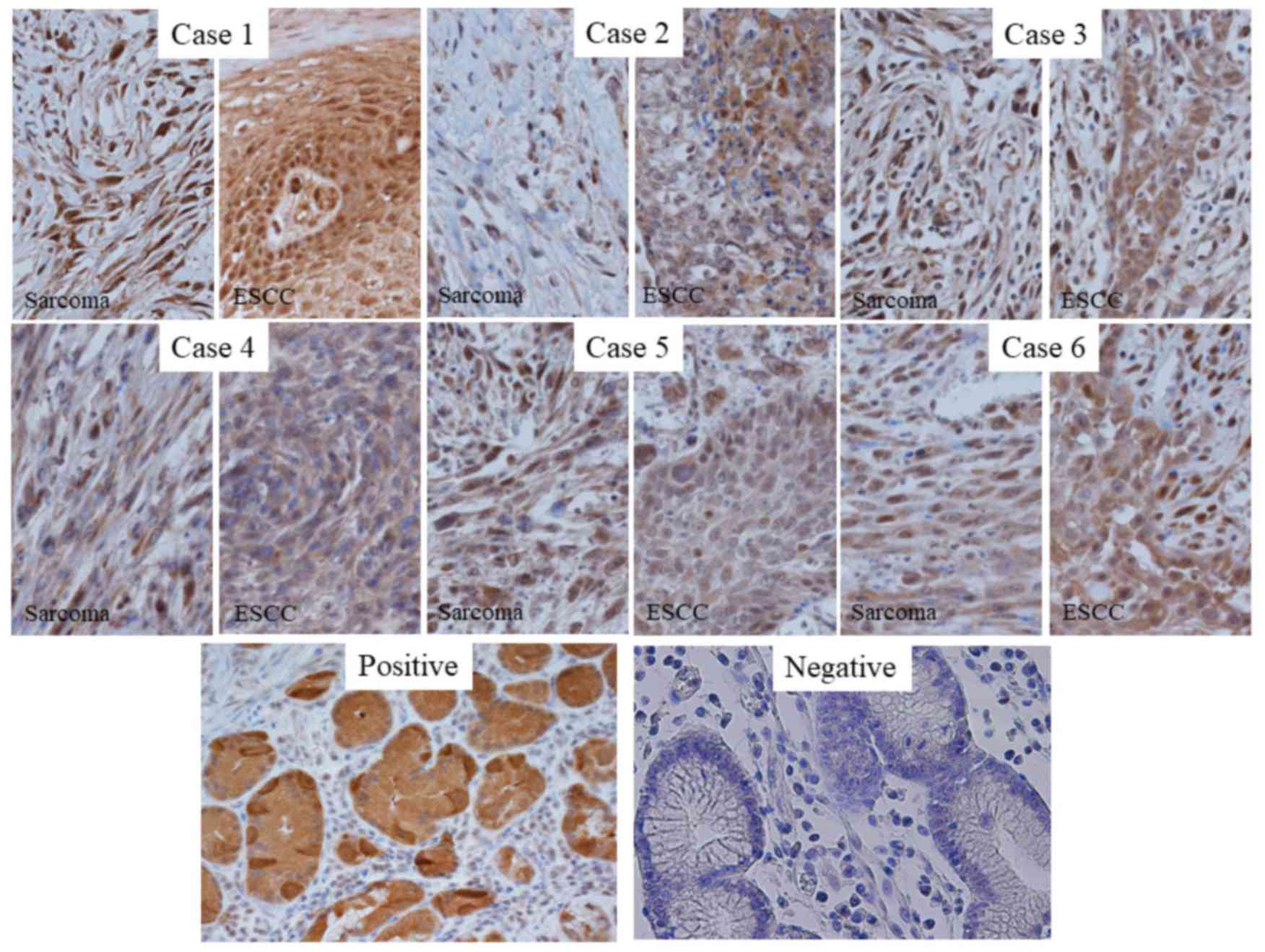
Pathological features
Histopathological findings indicated carcinomatous
cells and sarcomatous cells (Fig. 2).
The sarcomatous component exhibited spindle-shaped heterotypic
cells with varying sizes of enlarged nuclei. ESCC components,
scattered in an island shape, were indicated in the lesion. The two
components were separate in certain places and intermingled in
others. All cases exhibited ZEB1 expression in neoplastic cells
distributed uniformly in the sarcomatous component (Fig. 3). Neoplastic cells in the carcinoma
components were negative for ZEB1. In 2 cases, metastatic lymph
nodes were negative for ZEB1 (Fig.
4). The expression of Twist 1 and Snail 1, which are
EMT-associated factors similar to ZEB1, was confirmed. As a result,
Snail 1 was weakly expressed in the sarcoma component and the ESCC
component (Fig. 5). Twist 1 was
strongly expressed in the sarcoma and the ESCC component (Fig. 6). There was no indication that Twist 1
and Snail 1 were expressed specifically in the sarcoma
component.
Treatment and clinical outcome
Prognostic analysis of 115 cases of pT1 ESCC with
the same depth of tumor invasion as ECS (Table II) indicated a 5-year
disease-specific survival rate of 40.0% in ECS and 90.6% in ESCC.
ECS had a significantly worse prognosis compared with ESCC in pT1
cases (P=0.0016; Fig. 7A). The 5-year
relapse-free survival rate was 22.2% in ECS and 77.1% in ESCC, and
ECS had a significantly worse prognosis, compared with ESCC
(P=0.0267; Fig. 7B).
| Table II.Univariate analysis of esophageal
carcinosarcoma and esophageal squamous cell carcinoma with the same
depth of tumor invasion. |
Table II.
Univariate analysis of esophageal
carcinosarcoma and esophageal squamous cell carcinoma with the same
depth of tumor invasion.
|
Characteristics | pT1 carcinosarcoma
(n=6) | pT1 squamous cell
carcinoma (n=115) | P-value |
|---|
| Sex |
|
| 0.85 |
|
Male | 5 | 99 |
|
|
Female | 1 | 16 |
|
| Age, years |
|
| 0.65 |
|
<65 | 2 | 49 |
|
|
>64 | 4 | 66 |
|
| Location of
tumor |
|
| 0.99 |
|
Cervical esophagus | 0 | 1 |
|
| Upper
thoracic esophagus | 1 | 20 |
|
| Middle
thoracic esophagus | 4 | 67 |
|
| Lower
thoracic esophagus | 1 | 24 |
|
|
Abdominal esophagus | 0 | 3 |
|
| pN factor |
|
| 0.96 |
|
pN1 | 2 | 42 |
|
|
pN0 | 4 | 73 |
|
| Procedure of
esophagectomy |
|
| 0.61 |
|
VATS | 1 | 80 |
|
|
Thoracotomy | 5 | 35 |
|
| Neoadjuvant
chemotherapy |
|
| 0.58 |
|
Presence | 1 | 38 |
|
|
Absence | 5 | 77 |
|
| Recurrence |
|
| 0.03 |
|
Presence | 3 | 18 |
|
|
Absence | 3 | 97 |
|
Discussion
In the present study, the clinicopathological
features of ECS were examined. The results indicated that there was
a large discrepancy between the cT factor and the pT factor in ECS.
Even in cases with a predicted depth of invasion of cT2 or beyond
with large polypoid tumors, the pT factor in all cases indicated
that the depth of tumor was superficial invasion only. Regarding
the fact that all cases were T1 cases, this was uncommon. According
to previous studies, half of reported cases were pT1 (20–22). Due
to the high level of patient awareness with regard to health in the
area in which the Kitasato University Hospital is situated, the
diagnosis of the disease at an early stage is more likely. However,
as a number of patients harbored large tumors occupying the lumen,
the present study reported an unexpectedly large discrepancy
between the pathological depth of tumor invasion and the clinically
predicted depth of invasion. It has been reported that >90% of
ECS lesions are pedunculated or semipedunculated (23). The polypoid lesions have a
predominantly sarcoma component, whereas the superficial ESCC
component is mainly present in the stem and base (2). Therefore, sarcomatous metaplasia
originally occurs in superficial carcinoma, and only the
sarcoma-like component increases rapidly toward the lumen (2).
It has been suggested that in carcinosarcoma, the
sarcoma component may derive from EMT (24,25). EMT
is involved in a number of developmental milestones, including
gastrulation, neural crest formation and heart morphogenesis, which
rely on the plastic transition between the epithelium and
mesenchyme (6). By contrast, during
the progression of epithelial tumors, cancer cells develop
increased motility and invasiveness (6). EMT has been established as an important
step in the metastatic cascade of epithelial tumors (7). There are numerous molecules that could
explain EMT, including ZEB1, Twist 1 and Snail; however, in
esophageal carcinosarcoma, ZEB1 has been suggested to serve a
critical role in the EMT process (7).
In the present study, it is noteworthy that high expression of ZEB1
was recognized only in the sarcoma component. For this reason,
immunohistochemical staining was confirmed in all 6 cases, and as
depicted in Fig. 3, the expression of
ZEB1 was confirmed to be increased in the ECS component, confirm
with the ESCC component. This result suggests that ZEB1
upregulation in ESCC cells may cause EMT and the transformation to
carcinosarcoma. In addition, another study reported that
phospholipid glutathione peroxidase (GPX4) inhibition, which
induces ferroptic cell death in therapy-resistant cancer cells
across diverse mesenchymal cell-state contexts, did not exhibit
consistent sensitization in Snail 1 and Twist 1, but ZEB1 was
correlated with mesenchymal state sensitivity to GPX4 inhibition
(26). ZEB1 is a transcriptional
factor that can induce EMT through critical mediators, including
transforming growth factor β1 (27,28) and
miR-200 (29–31), suggesting that the clinical data of
the present study may support the underlying molecular mechanism of
ZEB1 in EMT.
Zhang et al (32) reported that spindle cell carcinoma
(SpCC) had a depth of pathological T1/2 (P<0.001) and a good
prognosis (P=0.044), compared with typical SCC, with increased
tumor depth, compare with SpCC. In the present study, the prognosis
of ECS was significantly worse compared with that of ESCC in terms
of disease-specific survival rate (P=0.0016). The prognostic
relevance between SpCC and ESCC differed between the study by Zhang
et al (32) and the present
study. However, in this previous study, the depth of tumor was
significantly shallower in SpCC cases compared with that in typical
SCC cases. It was considered that an identical depth of tumor may
cancel out the prognostic difference observed. In fact, when the
pathological factors of the patient background were stratified into
pT1/2 and the prognostic analysis was performed, it was reported
that there was no significant difference in the prognosis between
SpCC and typical SCC (32).
Therefore, the present study, to the best of our knowledge,
included novel findings comparing ECS cases and ESCC cases with
pT1.
It has been reported that the expression of ZEB1 in
the sarcoma component may be a cause of poor prognosis by
participating in treatment resistance, for example, against
chemotherapy, and causing distant metastasis (33). In addition, previous studies reported
that the inhibition of ZEB1 expression suppressed the tumorigenesis
of breast cancer cells (34), that
ZEB1 promoted metastasis and loss of cell polarity by repressing
the expression of lethal giant larvae homolog 2 in colorectal
cancer cells (35), and that ZEB1 was
associated with the resistance to chemotherapeutic agents,
including gemcitabine, 5-FU and cisplatin in pancreatic cancer
cells (36). Recurrent cases were
observed in the present study, despite administration of
postoperative adjuvant therapy with anticancer drugs. It has been
reported that recurrent tumors may be derived from sarcoma
(37) with strong expression of ZEB1
being expected. For the treatment of recurrent tumors with expected
anticancer drug resistance, no further promising results will be
obtained unless molecular targeted treatment is applied. In
addition, in a previous study in our laboratory (Department of
Surgery, Kitasato University School of Medicine), it was confirmed
that the suppression of ZEB1 expression in triple-negative breast
cancer resulted in a loss of resistance to phenylbutyrate in the
majority of cases (13).
Based on the aforementioned finding, the present
study aimed to indicate the molecular uniqueness of ESC by
confirming its specificity, as numerous molecules could be
associated with EMT, including ZEB1, Snail 1 and Twist 1. According
to the results of the comparative investigation, it was revealed
that ZEB1 is highly characteristic of sarcoma components of EMT in
ESC. However, a limitation of the present study is that it cannot
fully explain the association between ZEB1 and poor prognosis.
Despite that ZEB1 indicated an association with ESC, the present
study did not examine this association on a molecular level,
therefore further investigation is required.
In conclusion, a detailed clinicopathological
analysis of ECS was performed in the present study, and its unique
clinical and molecular features were identified. The features of
ECS indicated in the present study may be of great assistance in
further developing a novel therapeutic strategy for the
drug-resistant neoplasm.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
HH and KY conducted the conception and design,
acquisition of data, analysis of data and drafting the manuscript.
MWat performed the acquisition of data, and the drafting and
revising of the manuscript. MWas, AE, MK and HMo aided with
acquisition of data and assisted with revising the manuscript. YK
aided with the statistical analysis and analysis of data. KH and
HMi participated in the design and coordination of the study and
assisted with revising the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki and approved by the Research Ethics
Committee of Kitasato University School of Medicine (Sagamihara,
Japan). Written informed consent was obtained from each
patient.
Patient consent for publication
Written informed consent was obtained from each
patient for the publication of their data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Virchow RL: Die Krankhalften Geschwulste.
A Hirschwald, Berlin Volume. 2:pp181–182. 1865.
|
|
2
|
Japan Esophageal Society, . Japanese
classification of esophageal cancer, 11th edition: Part II and III.
Esophagus. 14:37–65. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kashiwabara K, Sano T, Oyama T, Najahima
T, Makita F, Hashimoto N, Iwanami K, Kawashima O, Matsumoto T and
Matsuzaki Y: A case of esophageal sarcomatoid carcinoma with
molecular evidence of a monoclonal origin. Pathol Res Pract.
197:41–46. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Handra-Luca A, Terris B, Couvelard A,
Molas G, Degott C and Flejou JF: Spindle cell squamous carcinoma of
the oesophagus: An analysis of 17 cases, with new
immunohistochemical evidence for a clonal origin. Histopathology.
39:125–132. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Matsumoto T, Fujii H, Arakawa A, Yamasaki
S, Sonoue H, Hattori K, Kajiyama Y, Hirose S and Tsurumaru M: Loss
of heterozygosity analysis shows monoclonal evolution with frequent
genetic progression and divergence in esophageal carcinosarcoma.
Hum Pathol. 35:322–327. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Larue L and Bellacosa A:
Epithelial-mesenchymal transition in development and cancer: Role
of phosphatidylinositol 3′ kinase/AKT pathways. Oncogene.
24:7443–7454. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nieto MA: The ins and outs of the
epithelial to mesenchymal transition in health and disease. Annu
Rev Cell Dev Biol. 27:347–376. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nakazawa T, Nobusawa S, Ikota H, Kuwano H,
Takeyoshi I and Yokoo H: Wide expression of ZEB1 in sarcomatous
component of spidle cell carcinoma of esophagus. Pathol Int.
65:635–643. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Brabletz S and Brabletz T: The ZEB/miR-200
feedback loop a motor of cellular plasticity in development and
cancer? EMBO Rep. 11:670–677. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lim YY, Wright JA, Attema JL, Gregory PA,
Bert AG, Smith E, Thomas D, Lopez AF, Drew PA, Khew-Goodall Y and
Goodall GJ: Epigenetic modulation of the miR-200 family is
associated with transition to a breast cancer stem-cell-like state.
J Cell Sci. 126:2256–2266. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhou X, Wang Y, Shan B, Han J, Zhu H, Lv
Y, Fan X, Sang M, Liu XD and Liu W: The downregulation of
miR200c/141 promotes ZEB1/2 expression and gastric cancer
progression. Med Oncol. 32:4282015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sobin LH and Wittekind C: TNM
classification of malignant tumors. 6th. New York: Wiley-Liss;
2002
|
|
13
|
Kikuchi M, Yamashita K, Waraya M, Minatani
N, Ushiku H, Kojo K, Ema A, Kosaka Y, Katoh H, Sengoku N, et al:
Epigenetic regulation of ZEB1-RAB25/ESRP1 axis plays a critical
role in phenylbutyrate treatment-resistant breast cancer.
Oncotarget. 7:1741–1753. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhu DY, Guo QS, Li YL, Cui B, Guo J, Liu
JX and Li P: Twist1 correlates with poor differentiation and
progression in gastric adenocarcinoma via elevation of FGFR2
expression. World J Gastroenterol. 20:18306–18315. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sung CO, Lee KW, Han S and Kim SH: Twist1
is up-regulated in gastric cancer-associated fibroblasts with poor
clinical outcomes. Am J Pathol. 179:1827–1838. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dong H, Xie L, Tang C, Chen S, Liu Q,
Zhang Q, Zheng W, Zheng Z and Zhang H: Snail1 correlates with
patient outcomes in E-cadherin-preserved gastroesophageal junction
adenocarcinoma. Clin Transi Oncol. 16:783–791. 2014. View Article : Google Scholar
|
|
17
|
Yu J, Li J, Chen Y, Cao W, Lu Y, Yang J
and Xing E: Snail enhances glycolysis in the epithelial-mesenchymal
transition process by targeting FBP1 in gastric cancer. Cell
Physiol Biochem. 43:31–38. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Owens WD, Felts JA and Spitznagel EL Jr:
ASA physical status classifications: A study of consistency of
ratings. Anesthesiology. 49:239–243. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dindo D, Demartines N and Clavien PA:
Classification of surgical complications: A new proposal with
evaluation in a cohort of 6336 patients and results of a survey.
Ann Surg. 240:205–213. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kimura H, Konishi K, Kawamura T, Nojima N,
Satou T, Maeda K, Yabushita K, Kuroda Y, Tsuji M and Miwa A:
Esophageal sarcomas: Report of three cases. Dig Surg. 16:244–247.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ji F, Xu YM and Xu CF: Endoscopic
polypectomy: A promising therapeutic choice for esophageal
carcinosarcoma. World J Gastroenterol. 15:3448–3450. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang L, Lin Y, Long H, Liu H, Rao H, He Y,
Rong T and Liang Y: Esophageal carcinosarcoma: A unique entity with
better prognosis. Ann Surg Oncol. 20:997–1004. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Takemura M, Osugi H, Takeda N, Okuda E,
Ueno M and Kinoshita H: Three cases of resected so-called
carcinosarcoma of the esophagus and review of the japanese
literature. J Jpn Surg Assoc. 62:659–664. 2001.(In Japanese).
View Article : Google Scholar
|
|
24
|
Sung CO, Choi H, Lee KW and Kim SH:
Sarcomatoid carcinoma represents a complete phenotype with various
pathways of epithelial mesenchymal transition. J Clin Pathol.
66:601–606. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pang A, Carbini M, Moreira AL and Maki RG:
Carcinosarcomas and related cancers: Tumors caught in the act of
epithelial-mesenchymal transition. J Clin Oncol Dec. 36:210–216.
2018. View Article : Google Scholar
|
|
26
|
Viswanathan VS, Ryan MJ, Dhruv HD, Gill S,
Eichhoff OM, Seashore-Ludlow B, Kaffenberger SD, Eaton JK, Shimada
K, Aguirre AJ, et al: Dependency of a therapy-resistant state of
cancer cells on a lipid peroxidase pathway. Nature. 547:453–457.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Horiguchi K, Sakamoto K, Koinuma D, Semba
K, Inoue A, Inoue S, Fujii H, Yamaguchi A, Miyazawa K, Miyazono K
and Saitoh M: TGF-β drives epithelial-mesenchymal transition
through δEF1-mediated downregulation of ESRP. Oncogene.
31:3190–3201. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Joseph JV, Conroy S, Tomar T,
Eggens-Meijer E, Bhat K, Copray S, Walenkamp AM, Boddeke E,
Balasubramanyian V, Wagemakers M, et al: TGF-β is an inducer of
ZEB1-dependent mesenchymal transdifferentiation in glioblastoma
that is associated with tumor invasion. Cell Death Dis.
5:e14432014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Korpal M, Lee ES, Hu G and Kang Y: The
miR-200 family inhibits epithelial-mesenchymal transition and
cancer cell migration by direct targeting of E-cadherin
transcriptional repressors ZEB1 and ZEB2. J Biol Chem.
283:14910–14914. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gregory PA, Bert AG, Paterson EL, Barry
SC, Tsykin A, Farshid G, Vadas MA, Khew-Goodall Y and Goodall GJ:
The miR-200 family and miR-205 regulate epithelial to mesenchymal
transition by targeting ZEB1 and SIP1. Nat Cell Biol. 10:593–601.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Park SM, Gaur AB, Lengyel E and Peter ME:
The miR-200 family determines the epithelial phenotype of cancer
cells by targeting the E-cadherin repressors ZEB1 and ZEB2. Gene
Dev. 22:894–907. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhang B, Xiao Q, Yang D, Li X, Hu J, Wang
Y and Wang W: Spindle cell carcinoma of the esophagus: A
multicenter analysis in comparison with typical squamous cell
carcinoma. Medicine (Baltimore). 95:e47682016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Aigner K, Dampier B, Descovich L, Mikula
M, Sultan A, Schreiber M, Mikuliys W, Brabletz T, Strand D, Obrist
P, et al: The transcription factor ZEB1 (deltaEF1) promotes tumour
cell dedifferentiation by repressing master regulators of
epithelial polarity. Oncogene. 26:6979–6988. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Arima Y, Hayashi H, Sasaki M, Hosonaga M,
Goto T, Chiyoda T, Kuninaka S, Shibata T, Ohata H, Nakagama H, et
al: Induction of ZEB proteins by inactivation of RB protein is key
determinant of mesenchymal phenotype of breast cancer. J Biol Chem.
287:7896–7906. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Spaderna S, Schmalhofer O, Wahlbuhl M,
Dimmler A, Bauer K, Sultan A, Hlubek F, Jung A, Strand D, Eger A,
et al: The transcriptional repressor ZEB1 promotes metastasis and
loss of cell polarity in cancer. Cancer Res. 68:537–544. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Arumugam T, Ramachandran V, Fournier KF,
Wang H, Marquis L, Abbruzzese JL, Gallick GE, Logsdon CD, McConkey
DJ and Choi W: Epithelial to mesenchymal transition contributes to
drug resistance in pancreatic cancer. Cancer Res. 69:5820–5828.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sanada Y, Hihara J, Yoshida K and
Yamaguchi Y: Esophageal carcinosarcoma with intramural metastasis.
Dis Esophagus. 19:119–131. 2006. View Article : Google Scholar : PubMed/NCBI
|