Introduction
According to GLOBOCAN 2018 estimations, gastric
cancer (GC) constitutes the sixth most common malignancy worldwide
(1). Despite the decline in stomach
cancer-associated mortality, its burden remains significant, being
the third leading cause of cancer mortality globally. Chemotherapy
serves a prominent role in the treatment of advanced- and
early-stage cancer. It is therefore paramount to identify
prognostic factors to assess patient responses to chemotherapy in
GC.
BRCA1 DNA repair associated (BRCA1) mutations
comprise risk factors for the development of breast and ovarian
cancer; moreover, carriers of BRCA1 germline mutations
exhibit a four- to seven-fold increased risk of developing GC
compared with the general population (2,3). In
addition, genetic alterations in the BRCA1 region have been
identified in early-onset GC and non-specific sporadic GC (4,5);
notably, BRCA1 polymorphism in sporadic GC has been reported
to be associated with the response to chemotherapy (6).
The underlying mechanism of BRCA1/2
loss-of-function mutations in tumorigenesis has been linked to
accelerated mutation acquisition in cells, caused by DNA
double-strand breaks (DSBs) and impaired homologous recombination.
Breast cancer type 1 susceptibility protein (BRCA1) and BRCA2
expression loss results in increased susceptibility to
chemotherapeutic agents in patients with breast, ovarian and lung
cancer (7–9). In vitro, BRCA1- and
BRCA2-deficient cells display a hypersensitivity to drugs that
induce DNA DSBs, including platinum-based agents (10,11). The
association of germline BRCA1/2 mutations with sensitivity to
platinum-based agents is relatively well established in epithelial
ovarian cancer (12). BRCA1/2 loss
of expression may therefore be useful for predicting the efficacy
of platinum-based chemotherapy in patients with GC. However, it
remains controversial whether BRCA1 protein expression loss is
beneficial to the survival of patients with GC (13–15).
Data associated with the impact of BRCA2 expression in GC is even
more limited.
The present study aimed to investigate the role of
BRCA1 and BRCA2 gene expression in predicting the
efficacy of chemotherapy in patients with GC. BRCA1 and BRCA2
protein and mRNA expression in formalin-fixed, paraffin-embedded
(FFPE) samples was evaluated using immunohistochemistry (IHC) and
in-situ hybridization (ISH) on tissue microarrays (TMAs),
along with reverse transcription-quantitative polymerase chain
reaction (RT-qPCR) analysis of the impact of BRCA1/2 expression
loss on overall survival (OS) and disease free survival (DFS).
Patients and methods
Patients
A total of 683 patients with available FFPE tumor
specimens were identified, according to the confirmation of a GC
diagnosis from Seoul National University College of Medicine
(Seoul, South Korea) between January 2010 and December 2011. Among
these patients, 365 with stage IIA-IIIC disease who underwent
curative resection and available specimens for BRCA1 and BRCA2 IHC
analysis were included. The inclusion criteria were as follows: i)
Patients with gastric carcinoma tumor >0.5 cm; ii) patients who
have primary gastric cancer tissue; and iii) patients with stage II
and III GC. The exclusion criteria were as follows: i) Patients
with gastric carcinoma tumor <0.5 cm; ii) patients with
metastatic tumor tissue only; iii) patients with stage I or IV GC;
and iv) patients who underwent palliative surgery. Adjuvant
chemotherapy was administered at the discretion of the physician.
Clinical data were retrieved from patient medical records, and
pathological stage was reassigned according to the American Joint
Committee on Cancer staging system, 7th edition (16). The median follow-up period was 71.8
months. All FFPE tissue samples were obtained from the archive of
the Department of Pathology, Seoul National University Hospital
(Seoul, South Korea).
The present study was approved by the Institutional
Review Board (IRB)/Independent Ethics Committee of Seoul National
University Hospital (H-1706-105-860). At the time of resection,
consent to perform surgery was obtained from the patients, but
consent for the research use of residual tissue was not obtained.
The requirement for written consent was waived by the IRB due to
the retrospective nature of the present study and the use of
anonymous clinical data.
IHC analysis of BRCA1 and BRCA2
expression
BRCA1 and BRCA2 nuclear expression was analyzed
using IHC with anti-BRCA1 (cat. no. 07-434; EMD Millipore,
Billerica, MA, USA) and anti-BRCA2 (cat. no. MAB2476; R&D
Systems, Inc., Minneapolis, MN, USA) antibodies (13). For IHC, 4-µm tissue sections for TMA
were stained using the standard streptavidin-biotin complex method.
Sectioning was performed after the specimens were de-paraffinized
and rinsed in PBS. The sections were subsequently rehydrated, and
antigen retrieval was performed by immersing the slides in 10 mM
citrate buffer (pH 6.0, 0.01 M citric acid, 0.01 M sodium citrate)
and heating for 10 min in the microwave. The sections were
incubated for 30 min with non-immune serum, followed by incubation
with primary mouse anti-BRCA1 (dilution, 1:150) and anti-BRCA2
(dilution, 1:500) antibodies for 2 h. Biotinylated secondary
antibody (cat. no. BP-1400; ready to use; Vector Laboratories,
Inc., Burlingame, CA, USA) was added (300 µl/slide) for 30 min at
room temperature, followed by streptavidin (dilution, 1:500), with
diaminobenzene (DAB) as the chromogen. All sections were
counterstained with hematoxylin (Sigma-Aldrich: Merck KGaA,
Darmstadt, Germany) for 10 sec. Normal gastric mucosa samples were
used as positive controls and samples not stained with primary
antibody represented the negative controls (Fig. 1).
A modified histochemical score (H-score) was
utilized to estimate BRCA1 and BRCA2 expression levels. This score
included assessment of the intensity and percentage of positive
cell staining. For intensity, a score index of 0, 1, 2, and 3 that
corresponded to negative, weak, moderate and strong staining,
respectively, was utilized. The percentage of positive cells was
scored as 0 to 100. The final score was the product of intensity
and positive cell percentage (range, 0-300). Positive expression of
BRCA1 and BRCA2 was defined by positive staining in ≥10% of the
cancer cells. Positive expression of BRCA1 and BRCA2 was further
classified as low and high expression according to the median
H-score cut-off of expression. Median H-score was 60 for BRCA1 and
70 for BRCA2.
RNA ISH
In situ detection of BRCA1 and
BRCA2 mRNA transcription using the RNAscope kit (Advanced
Cell Diagnostics, Hayward, CA, USA) was performed according to the
manufacturer's protocol. Housekeeping gene Peptidylpropyl
isomerase B (PPIB) was used as an internal-control mRNA;
if the PPIB score was 0, the sample was regarded as not
available for gene expression. A horseradish peroxidase-based
signal amplification system was used for hybridization to the
target probes, followed by color development with
3,3′-diaminobenzidine. The slides were counter-stained with
hematoxylin for 10 sec at room temperature. Positive staining was
determined by brown punctate dots in the nucleus and/or cytoplasm.
BRCA1 and BRCA2 expression was scored using the
instructions in the RNAscope FFPE assay kit: Score 0, no staining;
score 1, staining that was difficult to identify under a 40X
objective lens in >10% of tumor cells; score 2, staining that
was difficult to identify under a 20X objective lens, but easy
under a 40X objective lens in >10% of tumor cells; score 3,
staining that was difficult to identify under a 10X objective lens,
but easy under a 20X objective lens in >10% of tumor cells; and
score 4, easy to identify under a 10X objective lens in >10% of
tumor cells.
RT-qPCR
A total of 110 GC specimens were obtained for mRNA
extraction. Of these specimens, RNA from 72 was successfully
amplified. Tumor tissue from a representative paraffin block was
cut into 10-µm sections, and micro-dissection was utilized to
minimize the influence on the surrounding normal tissues. The
proportion of tumor cells was ~80%. Total RNA was extracted from
the FFPE tumor tissue using the RNeasy FFPE kit (Qiagen GmbH,
Hilden, Germany) according to the manufacturer's protocol. Total
RNA (1 mg) was reverse transcribed using the GoScript reverse
transcription system (Promega Corporation, Madison, WI, USA)
according to the manufacturer's protocol.
Template cDNA was amplified using the
TaqMan® gene expression assay (Applied Biosystems,
Foster City, CA, USA) and the 7500 PCR system (Applied Biosystems;
Thermo Fisher Scientific, Inc.). The 20-µl PCR mixture contained 2X
Premix ExTaq (Probe qPCR; Takara Bio, Inc., Otsu, Japan), 1 µl cDNA
and 1 µl each of the primers and probes [BRCA1
(Hs01556193_m1), BRCA2 (Hs00609073_m1), and ACTB
(Hs99999903_m1) (cat. no. 4331182)]. Amplification was performed in
a 96-well optical plate at 95°C for 30 sec, followed by 45 cycles
at 95°C for 5 sec and 60°C for 34 sec. The experiment was performed
in triplicate, and relative gene expression was calculated
according to the comparative Cq method (17). The final values were determined using
the following formula: mRNA expression level=2−ΔΔCq.
Statistical analysis
All statistical analyses were performed using SPSS
statistics 23 software (IBM Corp., Armonk, NY, USA). Differences in
clinicopathological parameters according to nuclear BRCA1 and BRCA2
expression were evaluated using the χ2 test and
linear-by-linear association. The minimum, maximum and mean values
of relative BRCA1 and BRCA2 mRNA expression were calculated as
2−ΔΔCq of each gene and plotted in Fig. 2. OS was defined from initial cancer
diagnosis to the time of death (from any cause). Patient survival
was analyzed using a Kaplan-Meier plot and the log-rank test. The
period of disease-free survival (DFS) was defined as the duration
between surgery and disease recurrence, any cause of death prior to
disease recurrence, or the most recent follow-up. Comparison of the
methods used to measure BRCA1 and BRCA2 expression levels was
performed using the χ2 test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics and clinical
outcomes
In the present study, a total of 367 patient samples
were analyzed and baseline characteristics are summarized in
Table I. The median age was 62±12.9
years. A total of 253 patients (68.9%) underwent subtotal
gastrectomy and 114 patients (31.1%) underwent total gastrectomy.
Neoadjuvant chemotherapy was administered to 9 patients. Of the 273
informative cases, 180 (49.0%) received postoperative chemotherapy.
The chemotherapy regimen were as follows: Etoposide and platinum
agent (n=3); fludarabine and mitoxantrone (n=1); 5-fluorouracil
(5-FU), leucovorin (folinic acid) and oxaliplatin (n=1); 5-FU and
cisplatin (n=67); FU (n=12); tegafur, gimeracil, and oteracil
potassium (S-1) (n=62); S-1 with cisplatin (n=6); capecitabine and
oxaliplatin (n=17); and capecitabine and cisplatin (n=28). Of the
192 informative cases, a platinum regimen was used in 135
patients.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Variable | n | % |
|---|
| Sex |
|
|
|
Male | 239 | 65.1 |
|
Female | 128 | 34.9 |
| Age, years |
|
|
|
≤45 | 45 | 12.3 |
| 45<
× ≤60 | 130 | 35.4 |
|
>60 | 192 | 52.3 |
| Adjuvant
chemotherapy |
|
|
| No | 93 | 25.3 |
|
Yes | 180 | 49.0 |
| Not
available | 94 | 25.6 |
| Histological grade
and type |
|
|
| Well
differentiated | 22 | 6.0 |
|
Moderately differentiated | 110 | 30.0 |
| Poorly
differentiated | 173 | 47.1 |
| Signet
ring cell carcinoma | 48 | 13.1 |
|
Mucinous adenocarcinoma | 13 | 3.5 |
|
Undifferentiated
carcinoma | 1 | 0.3 |
|
T-stagea |
|
|
| T1 | 19 | 5.2 |
| T2 | 49 | 13.4 |
| T3 | 183 | 49.9 |
| T4 | 116 | 31.6 |
|
N-stagea |
|
|
| N0 | 78 | 21.3 |
| N1 | 84 | 22.9 |
| N2 | 100 | 27.2 |
| N3 | 105 | 28.6 |
| TNM
stagea |
|
|
| II | 177 | 48.2 |
|
III | 190 | 51.8 |
| Lymphatic
invasion |
|
|
|
Absent | 121 | 33 |
|
Present | 246 | 67 |
| Venous
invasion |
|
|
|
Absent | 283 | 77.1 |
|
Present | 84 | 22.9 |
| Perineural
invasion |
|
|
|
Absent | 172 | 46.9 |
|
Present | 195 | 53.1 |
Adjuvant chemotherapy was used by 43.5% of patients
(n=77) with stage II disease and in 54.2% (n=103) with stage III
disease. In 22% of patients (n=39) with stage II disease and 50% of
patients (n=95) with stage III disease, a platinum-based treatment
was included in the adjuvant chemotherapy regimen. Histological
grades according to WHO classification of well differentiated,
moderately differentiated and poorly differentiated were
represented by 6.0, 30.0 and 47.1% of patients, respectively.
Intestinal type (according to Lauren classification) was observed
in 40.3% of patients. Lymphatic, venous and perineural invasion
were identified in 67.0, 22.9 and 53.1% of patients, respectively.
Relapse occurred in 76 patients (20.7%) and mortality in 102
patients (29.2%) during the median follow-up period of 44.2 months.
The 5-year DFS rate was 70.0% and the 5-year OS rate was 66.0%.
A total of 360 of the 367 GC cases were informative
for BRCA1 and BRCA2 IHC. A lack of BRCA1 expression was observed in
61 patients (16.9%) and BRCA1-positive expression was observed in
299 patients (83.1%). No clinicopathological parameters were
significantly associated with BRCA1 expression status (Table II). A lack of BRCA2 expression was
observed in 63 patients (17.5%) and BRCA2-positive expression was
apparent in 296 patients (82.4%). A lack of BRCA2 expression was
associated with patient age <45 years (P=0.01), a histological
type of signet ring cell carcinoma (P<0.001) and a Lauren
classification of diffuse type (P<0.001).
| Table II.Association between BRCA
immunohistochemistry status and clinicopathological features in 360
informative gastric cancer cases. |
Table II.
Association between BRCA
immunohistochemistry status and clinicopathological features in 360
informative gastric cancer cases.
|
| BRCA1 IHC |
| BRCA2 IHC |
|
|
|
|---|
|
|
|
|
|
|
|
|
|---|
|
| Negative | Positive |
| Negative | Positive |
| Total |
|---|
|
|
|
|
|
|
|
|
|
|---|
| Variable | n | % | n | % | P-value | n | % | n | % | P-value | n | % |
|---|
| Total patients | 61 | 16.9 | 299 | 83.1 |
| 63 | 17.5 | 297 | 82.5 |
|
|
|
| Sex |
|
|
|
| 0.459 |
|
|
|
| 0.045 |
|
|
|
Male | 42 | 18.0 | 191 | 82.0 |
| 34 | 14.6 | 199 | 85.4 |
| 233 | 64.7 |
|
Female | 19 | 15.0 | 108 | 85.0 |
| 29 | 23.0 | 97 | 77.0 |
| 127 | 35.3 |
| Age, years |
|
|
|
| 0.018 |
|
|
|
| 0.220 |
|
|
|
<45 | 4 | 9.3 | 39 | 90.7 |
| 11 | 25.6 | 32 | 74.4 |
| 43 | 11.9 |
|
45–60 | 15 | 11.7 | 113 | 88.3 |
| 24 | 18.8 | 104 | 81.3 |
| 128 | 35.6 |
|
>60 | 42 | 22.2 | 147 | 77.8 |
| 28 | 14.8 | 161 | 85.2 |
| 189 | 52.5 |
| Histological grade
and type |
|
|
|
| 0.174 |
|
|
|
| <0.001 |
|
|
| Well
differentiated | 3 | 13.6 | 19 | 86.4 |
| 2 | 9.1 | 20 | 90.9 |
| 22 | 6.1 |
|
Moderately differentiated | 25 | 23.4 | 82 | 76.6 |
| 9 | 8.4 | 98 | 91.6 |
| 107 | 29.7 |
| Poorly
differentiated | 29 | 16.9 | 143 | 83.1 |
| 27 | 15.7 | 145 | 84.3 |
| 172 | 47.8 |
| Signet
ring cell carcinoma | 3 | 6.5 | 43 | 93.5 |
| 21 | 46.7 | 24 | 53.3 |
| 46 | 12.8 |
|
Mucinous adenocarcinoma | 1 | 8.3 | 11 | 91.7 |
| 4 | 33.3 | 8 | 66.7 |
| 12 | 3.3 |
|
Undifferentiated
carcinoma | 0 | 0.0 | 1 | 100.0 |
| 0 | 0.0 | 1 | 100.0 |
| 1 | 0.3 |
| Lauren
classification |
|
|
|
| 0.065 |
|
|
|
| <0.001 |
|
|
|
Intestinal | 31 | 21.4 | 114 | 78.6 |
| 13 | 9.0 | 132 | 91.0 |
| 145 | 40.3 |
|
Diffuse | 30 | 14.0 | 185 | 86.0 |
| 50 | 23.4 | 164 | 76.6 |
| 215 | 59.7 |
| Location |
|
|
|
| 0.056 |
|
|
|
| 0.072 |
|
|
| Upper
third | 13 | 19.1 | 55 | 80.9 |
| 9 | 13.2 | 59 | 86.8 |
| 68 | 18.9 |
| Middle
third | 8 | 8.8 | 83 | 91.2 |
| 23 | 25.3 | 68 | 74.7 |
| 91 | 25.3 |
| Lower
third | 40 | 19.9 | 161 | 80.1 |
| 31 | 15.4 | 170 | 84.6 |
| 201 | 55.8 |
| T stage |
|
|
|
| 0.739 |
|
|
|
| 0.072 |
|
|
| T1 | 4 | 22.2 | 14 | 77.8 |
| 6 | 33.3 | 12 | 66.7 |
| 18 | 5.0 |
| T2 | 10 | 20.8 | 38 | 79.2 |
| 4 | 8.3 | 44 | 91.7 |
| 48 | 13.3 |
| T3 | 30 | 16.8 | 149 | 83.2 |
| 29 | 16.3 | 149 | 83.7 |
| 179 | 49.7 |
| T4 | 17 | 14.8 | 98 | 85.2 |
| 24 | 20.9 | 91 | 79.1 |
| 115 | 31.9 |
| N stage |
|
|
|
| 0.582 |
|
|
|
| 0.796 |
|
|
| N0 | 9 | 11.8 | 67 | 88.2 |
| 14 | 18.7 | 61 | 81.3 |
| 76 | 21.1 |
| N1 | 14 | 17.1 | 68 | 82.9 |
| 15 | 18.3 | 67 | 81.7 |
| 82 | 22.8 |
| N2 | 19 | 19.4 | 79 | 80.6 |
| 14 | 14.3 | 84 | 85.7 |
| 98 | 27.2 |
| N3 | 19 | 18.3 | 85 | 81.7 |
| 20 | 19.2 | 84 | 80.8 |
| 104 | 28.9 |
| TNM stage |
|
|
|
| 0.810 |
|
|
|
| 0.580 |
|
|
| II | 30 | 17.4 | 142 | 82.6 |
| 32 | 18.7 | 139 | 81.3 |
| 172 | 47.8 |
|
III | 31 | 16.5 | 157 | 83.5 |
| 31 | 16.5 | 157 | 83.5 |
| 188 | 52.2 |
| Lymphatic
invasion |
|
|
|
| 0.725 |
|
|
|
| 0.280 |
|
|
|
Absent | 21 | 17.9 | 96 | 82.1 |
| 24 | 20.7 | 92 | 79.3 |
| 117 | 32.5 |
|
Present | 40 | 16.5 | 203 | 83.5 |
| 39 | 16.0 | 204 | 84.0 |
| 243 | 67.5 |
| Vascular
invasion |
|
|
|
| 0.358 |
|
|
|
| 0.120 |
|
|
|
Absent | 44 | 15.9 | 232 | 84.1 |
| 53 | 19.3 | 222 | 80.7 |
| 276 | 76.7 |
|
Present | 17 | 20.2 | 67 | 79.8 |
| 10 | 11.9 | 74 | 88.1 |
| 84 | 23.3 |
| Perineural
invasion |
|
|
|
| 0.066 |
|
|
|
| 0.673 |
|
|
|
Absent | 35 | 20.8 | 133 | 79.2 |
| 31 | 18.5 | 137 | 81.5 |
| 168 | 46.7 |
|
Present | 26 | 13.5 | 166 | 86.5 |
| 32 | 16.8 | 159 | 83.2 |
| 192 | 53.3 |
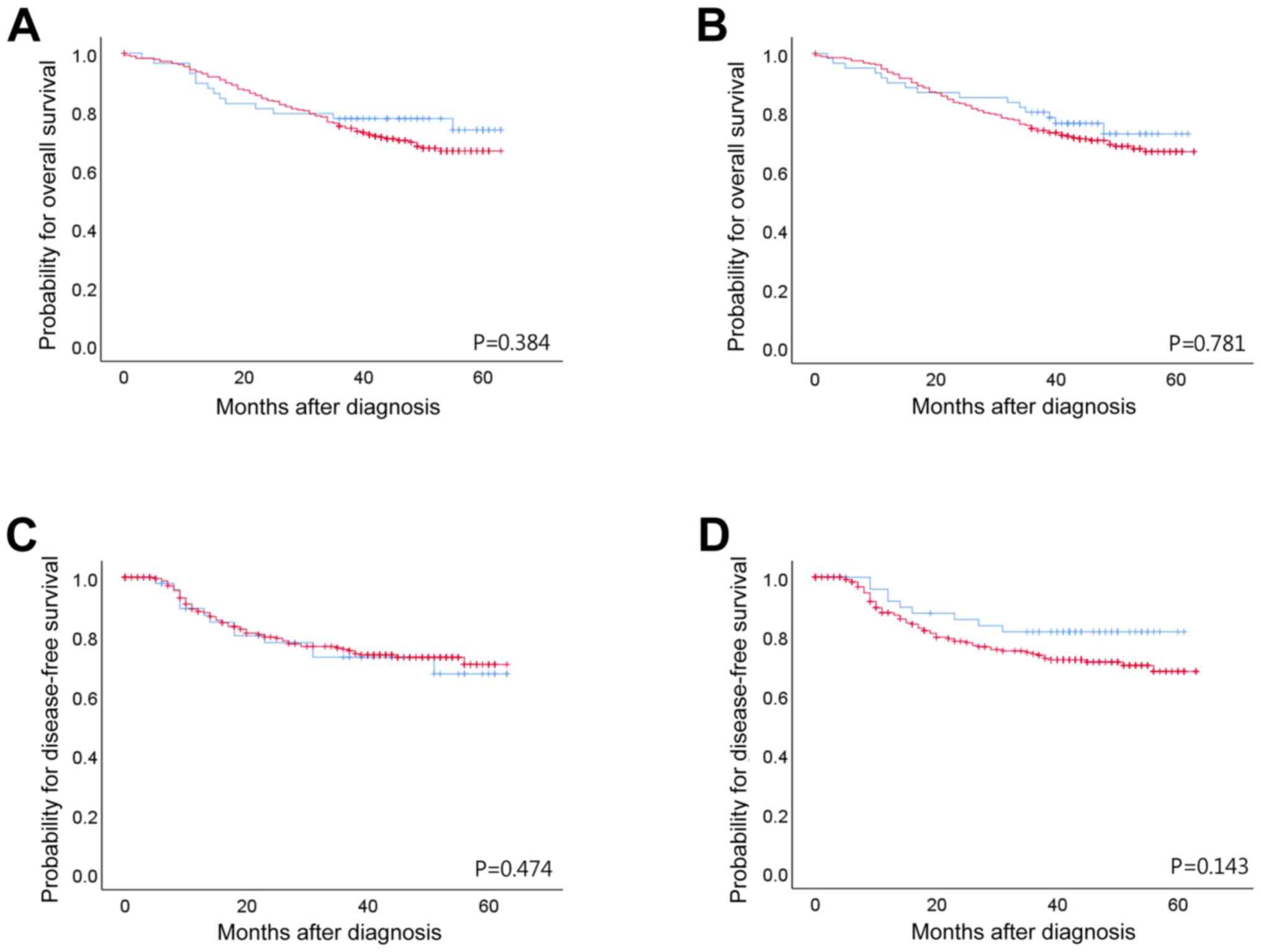
Prognosis according to BRCA1 and BRCA2
expression
Following Kaplan-Meier analysis, neither BRCA1 nor
BRCA2 (as evaluated by IHC) had any significant impact on the OS or
DFS of patients with stage II/III GC. Total patient and subgroup
analyses of DFS and OS did not highlight any significant
differences between patients who received adjuvant chemotherapy and
those who did not (Fig. 2). The
benefits of adjuvant chemotherapy and platinum regimens were not
statistically significant, although platinum-treated BRCA1-positive
patients with stage II disease exhibited a longer DFS time
(P=0.016; Table III). The
prognostic value of BRCA1 and BRCA2 expression did not remain
significant. Vascular invasion (P=0.028), perineural invasion
(P=0.001) and tumor stage (P<0.001) were significantly
associated with DFS. Perineural invasion (P=0.004), adjuvant
chemotherapy (P=0.001) and tumor stage (P<0.001) were
significantly associated with OS (Table
IV).
| Table III.Comparison of probability values of
Kaplan-Meier survival analyses for stage II and III (n=343), stage
II (n=160) and stage III (n=183) patients. |
Table III.
Comparison of probability values of
Kaplan-Meier survival analyses for stage II and III (n=343), stage
II (n=160) and stage III (n=183) patients.
|
| P-value for BRCA1
IHC | P-value for BRCA2
IHC |
|---|
|
|
|
|
|---|
|
| OS | DFS | OS | DFS |
|---|
|
|
|
|
|
|
|---|
| Treatment | II+III | II | III | II+III | II | III | II+III | II | III | II+III | II | III |
|---|
| All patients | 0.384 | 0.752 | 0.513 | 0.781 | 0.355 | 0.605 | 0.474 | 0.386 | 0.738 | 0.143 | 0.262 | 0.398 |
| Adjuvant
chemotherapy | 0.146 | 0.475 | 0.318 | 0.549 | 0.144 | 0.75 | 0.205 | 0.25 | 0.394 | 0.146 | 0.336 | 0.318 |
| No adjuvant
chemotherapy | 0.597 | 0.336 | 0.633 | 0.503 | 0.822 | 0.392 | 0.539 | 0.952 | 0.007a | 0.597 | 0.475 | 0.633 |
| Platinum
regimen | 0.374 | 0.05b | 0.253 | 0.329 | 0.016 | 0.518 | 0.137 | 0.502 | 0.228 | 0.11 | 0.977 | 0.141 |
| Non-platinum
regimen | 0.242 | 0.586 | 0.349 | 0.148 | 0.378 | 0.281 | 0.528 | 0.488 | 0.984 | 0.796 | 0.272 | 0.175 |
| Table IV.Multivariate analysis of factors
associated with DFS and OS. |
Table IV.
Multivariate analysis of factors
associated with DFS and OS.
|
| DFS | OS |
|---|
|
|
|
|
|---|
| Variable | Hazard ratio | 95% CI | P-value | Hazard ratio | 95% CI | P-value |
|---|
| BRCA1
IHC-negative | 1.625 | 0.854–3.093 | 0.139 | 0.823 | 0.427–1.588 | 0.562 |
| BRCA2
IHC-negative | 0.668 | 0.316–1.413 | 0.292 | 0.971 | 0.473–1.996 | 0.937 |
| Age <60
years | 0.503 | 0.464–1.458 | 0.503 | 0.769 | 0.426–1.386 | 0.382 |
| Lymphatic
invasion | 1.205 | 0.633–2.293 | 0.57 | 1.257 | 0.662–2.386 | 0.485 |
| Vascular
invasion | 1.826 | 1.068–3.121 | 0.028 | 1.28 | 0.754–2.174 | 0.361 |
| Perineural
invasion | 2.704 | 1.477–4.95 | 0.001 | 2.234 | 1.294–3.856 | 0.004 |
| Adjuvant
chemotherapy | 0.834 | 0.422–1.652 | 0.603 | 0.349 | 0.193–0.633 | 0.001 |
| Stage III vs. stage
II | 3.564 | 1.828–6.946 | <0.001 | 4.689 | 2.388–9.211 | <0.001 |
BRCA1 and BRCA2 mRNA and protein
expression
Positive BRCA1 IHC staining was observed in the
cytoplasm and nuclei of tumor cells, whereas BRCA2 was only
detected in the cytoplasm of GC cells (Fig. 1). A lack of BRCA2 expression has been
associated with advanced Tumor-Node-Metastasis (TNM) stage.
BRCA1 and BRCA2 mRNA from 72 of the 110 cases were
successfully amplified using RT-qPCR (Fig. 3). Comparisons between the IHC, ISH
and RT-qPCR results were made by pairwise tabulation of BRCA1 and
BRAC2 ISH scores in columns, and BRCA1 and BRAC2 IHC, and BRCA1 and
BRAC2 RT-qPCR in rows (Table V). The
results demonstrated a significant association between BRCA1 mRNA
expressions measured by RT-qPCR and ISH score (P=0.009) and between
BRCA2 mRNA expressions measured by RT-qPCR and ISH score
(P=0.051).
| Table V.Comparison of methods to determine
BRCA1 and BRCA2 expression in formalin-fixed paraffin-embedded
tissues. |
Table V.
Comparison of methods to determine
BRCA1 and BRCA2 expression in formalin-fixed paraffin-embedded
tissues.
|
| BRCA1 ISH
score |
| BRCA2 ISH
score |
|
|---|
|
|
|
|
|
|
|---|
| Expression | 0 | 1 | 2 | 3 | 4 | P-value | 0 | 1 | 2 | 3 | 4 | P-value |
|---|
| BRCA1 IHC, n
(%) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Negative | 19 (19.8) | 17 (15.5) | 7 (18.4) | 9 (14.3) | 9 (17.0) | 0.894 | 28 (19.3) | 10 (13.3) | 7 (20.6) | 10 (18.5) | 6 (11.5) | 0.597 |
|
Positive | 77 (80.2) | 93 (84.5) | 31 (81.6) | 54 (85.7) | 44 (83.0) |
| 117 (80.7) | 65 (86.7) | 27 (79.4) | 44 (81.5) | 46 (88.5) |
|
| BRCA2 IHC, n
(%) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Negative | 19 (19.8) | 19 (17.3) | 9 (23.7) | 10 (15.9) | 6 (11.3) | 0.579 | 29 (20.0) | 11 (14.7) | 7 (20.6) | 8 (14.8) | 8 (15.4) | 0.791 |
|
Positive | 77 (80.2) | 91 (82.7) | 29 (76.3) | 53 (84.1) | 47 (88.7) |
| 116 (80.0) | 64 (85.3) | 27 (79.4) | 46 (85.2) | 44 (84.6) |
|
| BRCA1 RT-qPCR, n
(%) |
|
|
|
|
|
|
|
|
|
|
|
|
| Low
expression | 14 (93.3) | 17 (60.7) | 1 (20.0) | 8 (61.5) | 10 (90.9) | 0.009 | 20 (83.3) | 12 (54.5) | 0 (0.0) | 8 (72.7) | 10 (76.9) | 0.051 |
| High
expression | 1 (6.7) | 11 (39.3) | 4 (80.0) | 5 (38.5) | 1 (9.1) |
| 4 (16.7) | 10 (45.5) | 2 (100.0) | 3 (27.3) | 3 (23.1) |
|
| BRCA2 RT-qPCR, n
(%) |
|
|
|
|
|
|
|
|
|
|
|
|
| Low
expression | 13 (86.7) | 20 (71.4) | 5 (100.0) | 10 (76.9) | 8 (72.7) | 0.569 | 19 (79.2) | 18 (81.8) | 1 (50.0) | 9 (81.8) | 9 (69.2) | 0.776 |
| High
expression | 2 (13.3) | 8 (28.6) | 0 (0.0) | 3 (23.1) | 3 (27.3) |
| 5 (20.8) | 4 (18.2) | 1 (50.0) | 2 (18.2) | 4 (30.8) |
|
Discussion
BRCA1, an essential component of numerous DNA damage
repair pathways, and pathways involved in cellular responses to
microtubule damage, is considered to be a differential modulator of
cancer survival following treatment with cisplatin and taxanes. In
particular, preclinical and clinical studies have reported that
BRCA1 expression level is associated with cisplatin and taxane
chemosensitivity (13). Moreover,
germline mutations in BRCA1 and BRCA2 are detected in
14.5% of serous ovarian carcinomas. However, in epithelial ovarian
cancer, a more favorable prognosis has been demonstrated for those
with BRCA1 and BRCA2 mutations (4). Although the mechanism driving the
association between BRCA1/2 mutations and survival is not
known, it has been suggested that the survival advantage of
mutation may be mediated by an improved response to platinum-based
agents (5).
Improved practical methods to determine BRCA1 and
BRCA2 mRNA and protein expression are currently required.
Therefore, the present study utilized IHC, ISH and RT-qPCR to
detect BRCA gene expression in FFPE GC tissues, and
evaluated the clinical relevance of these genes in sporadic GC. In
breast and ovarian cancer, it has been illustrated that mRNA
expression of BRCA1 and BRCA2 has prognostic value and clinical
impact in terms of chemotherapeutic response (18). From the identification of a reliable
antibody for BRCA1 protein IHC through the evaluation of the
specificity and sensitivity of available anti-BRCA1 antibodies
(19), BRCA1 expression was revealed
to be associated with certain molecular events in ovarian
high-grade serous carcinomas, with no cases of BRCA1
germline mutation displaying intact immunostaining (negative
predictive value, 100%) (20).
Moreover, IHC analysis is considered the most effective approach to
stratify patients with high-grade serous ovarian carcinoma for
germline genetic testing (20). By
contrast, the frequency of BRCA1 mutations among patients
with breast cancer is <5% (21),
whereas the loss of BRCA1 protein expression is ~20% (22). From a clinical perspective, IHC is
also the most accurate method for identifying the loss of gene
expression. In the present study, although no significant
association was identified between methods, the findings verified
that IHC determination of BRCA protein expression represents a
suitable method of detection in GC specimens. Moreover, IHC
evaluation of BRCA2 expression levels was more clinically
significant when compared with BRCA1. By contrast, other studies
have illustrated that BRCA1 expression (evaluated by IHC) is more
closely associated with clinical outcome (2,13,23).
Previously, Wang et al (23) studied a large cohort of patients with
cancer of the digestive system, including 627 stomach, 442
intestinal, 255 liver and 222 pancreatic cancer cases. BRCA1 and
BRCA2 expression was determined using IHC, and associations between
clinicopathological parameters and patient survival were
determined. The study revealed downregulation of cytoplasmic BRCA1
and BRCA2, and upregulation of nuclear BRCA1 in digestive tumors.
Low expression levels of cytoplasmic BRCA1 and BRCA2, and high
expression levels of nuclear BRCA1 were commonly associated with
advanced TNM stage. Cytoplasmic BRCA1 and BRCA2 were independent
favorable prognostic factors in gastric, colorectal and liver
cancer, and nuclear BRCA1 expression was an independent prognostic
factor predicting poor outcome in all of the cancer types
investigated.
By contrast, the present study involved 367 cases of
gastric cancer, and the IHC data were limited to revealing a
relatively close association between a lack of BRCA2 expression and
higher T stage. One of the aims of the study was to evaluate the
efficiency of the ISH method in determining BRCA1 and BRCA2 mRNA
expression levels in GC tissues, when compared with RT-qPCR.
Although not statistically significant, a link between BRCA1
expression levels determined by ISH and RT-qPCR was
demonstrated.
A number of studies used fresh tissues to quantify
BRCA1 mRNA expression levels with RT-qPCR (14,18),
although there is no evidence of previous studies performing a
paired evaluation of BRCA1 mRNA using ISH and RT-qPCR (24). Due to the effects of FFPE processing,
the present study was limited in terms of mRNA quality; BRCA1 and
BRCA2 mRNA were successfully amplified in only 72 of the 110
submitted cases, which was considered to have influenced the lack
of statistical significance between the results generated using ISH
and RT-qPCR.
BRCA1 protein is known to serve as a therapeutic
target for DNA-damaging chemotherapy in breast, ovarian and lung
cancer treatment (25,26). The loss or reduction of BRCA1 mRNA
and protein expression has been demonstrated in sporadic breast
cancer, and its prognostic significance has been reported (24,27).
Other DNA repair-associated biomarkers include ataxia
telangiectasia mutated (ATM), ATM-Rad3-related gene, mediator of
DNA damage checkpoint protein 1 and meiotic recombination 11
(12) along with DNA
repair-associated biomarkers induced by alcohol, including
transcription factor IIB-related factor 1 and myeloperoxidase
(28). In non-small cell lung cancer
and GC patients with malignant effusions, excision repair
cross-complementing group 1 and BRCA1 mRNA expression levels
correlated with in vitro chemosensitivity to cisplatin
and/or docetaxel (4).
BRCA1 and BRCA2 serve multi-aspect roles in a number
of DNA repair pathways, including those involved in homologous
recombination, non-homologous end joining and single-strand
annealing. During homologous recombination, BRCA1 acts as a linker
between the detection of DNA damage and the effectors that execute
DSB repair (29), whereas BRCA2
primarily triggers DSB repair through its interaction with DNA
repair protein RAD51 homolog 2 (30). When the homologous recombination
pathway is impaired, DSBs can result in genomic instability, which
further predisposes individuals to cancer.
In the present study, the loss of BRCA1 and BRCA2
expression correlated with certain clinicopathological parameters
in a cohort of Korean patients. The effects of platinum-based
agents in postoperative adjuvant chemotherapy was also evaluated.
During conventional adjuvant chemotherapy, platinum-based agents
are administered to patients at higher clinical stages who are at a
higher risk. However, no statistical significance was demonstrated
between the expression of BRCA1 or BRCA2 and survival outcome. The
retrospective nature of the study was also somewhat limiting, and a
randomized prospective study is required to remove confounding
factors and subsequent bias.
In conclusion, the present study revealed that BRCA1
and BRCA2, as evaluated by IHC, constitute clinically useful
biomarkers for the detection of sporadic GC. A randomized
prospective clinical trial is necessary to evaluate the effects of
BRCA1 and BRCA2 expression on therapeutic sensitivity, and the
benefits of adjuvant chemotherapy or platinum regimens in patients
with GC.
Acknowledgements
The authors would like to thank Ms Hye Jung Lee and
Ms Seung Hee Jung in Seoul National University College of Medicine,
Seoul Korea for construction of the tissue array, and for
assistance in performing the IHC staining and ISH.
Funding
The present study was supported by a National
Research Foundation of Korea grant funded by the Korean government
(grant no. 2014R1A1A2057925).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HSK evaluated the IHC slides and ISH, performed
RT-qPCR and wrote the manuscript. IGH grouped the chemotherapy
regimen. HYM performed data analysis. YJB and WHK collected
clinicopathological information from patients, constructed tissue
array blocks, and conducted IHC and ISH.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board/Independent Ethics Committee of Seoul National
University Hospital (H-1706-105-860). The requirement for written
consent was waived.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Wang J, Li X, Li J, Zhou L, Qiu T,
Zhang M and Liu P: Prognostic significance of BRCA1 expression in
gastric cancer. Med Oncol. 30:4232013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Brose MS, Rebbeck TR, Calzone KA, Stopfer
JE, Nathanson KL and Weber BL: Cancer risk estimates for BRCA1
mutation carriers identified in a risk evaluation program. J Natl
Cancer Inst. 94:1365–1372. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang L, Wei J, Qian X, Yin H, Zhao Y, Yu
L, Wang T and Liu B: ERCC1 and BRCA1 mRNA expression levels in
metastatic malignant effusions is associated with chemosensitivity
to cisplatin and/or docetaxel. BMC Cancer. 8:972008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Semba S, Yokozaki H, Yasui W and Tahara E:
Frequent microsatellite instability and loss of heterozygosity in
the region including BRCA1 (17q21) in young patients with gastric
cancer. Int J Oncol. 12:1245–1251. 1998.PubMed/NCBI
|
|
6
|
Shim HJ, Yun JY, Hwang JE, Bae WK, Cho SH,
Lee JH, Kim HN, Shin MH, Kweon SS, Lee JH, et al: BRCA1 and XRCC1
polymorphisms associated with survival in advanced gastric cancer
treated with taxane and cisplatin. Cancer Sci. 101:1247–1254. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Goffin JR, Chappuis PO, Bégin LR, Wong N,
Brunet JS, Hamel N, Paradis AJ, Boyd J and Foulkes WD: Impact of
germline BRCA1 mutations and overexpression of p53 on prognosis and
response to treatment following breast carcinoma: 10-year follow up
data. Cancer. 97:527–536. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kennedy RD, Quinn JE, Mullan PB, Johnston
PG and Harkin DP: The role of BRCA1 in the cellular response to
chemotherapy. J Natl Cancer Inst. 96:1659–1668. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reguart N, Cardona AF, Carrasco E, Gomez
P, Taron M and Rosell R: BRCA1: A new genomic marker for
non-small-cell lung cancer. Clin Lung Cancer. 9:331–339. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Aly A and Ganesan S: BRCA1, PARP, and
53BP1: Conditional synthetic lethality and synthetic viability. J
Mol Cell Biol. 3:66–74. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Foulkes WD: BRCA1 and BRCA2:
Chemosensitivity, treatment outcomes and prognosis. Fam Cancer.
5:135–142. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bolton KL, Chenevix-Trench G, Goh C,
Sadetzki S, Ramus SJ, Karlan BY, Lambrechts D, Despierre E,
Barrowdale D, McGuffog L, et al: Association between BRCA1 and
BRCA2 mutations and survival in women with invasive epithelial
ovarian cancer. JAMA. 307:382–390. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim JW, Cho HJ, Kim M, Lee KH, Kim MA, Han
SW, Oh DY, Lee HJ, Im SA, Kim TY, et al: Differing effects of
adjuvant chemotherapy according to BRCA1 nuclear expression in
gastric cancer. Cancer Chemother Pharmacol. 71:1435–1443. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wei J, Costa C, Ding Y, Zou Z, Yu L,
Sanchez JJ, Qian X, Chen H, Gimenez-Capitan A, Meng F, et al: mRNA
expression of BRCA1, PIAS1, and PIAS4 and survival after
second-line docetaxel in advanced gastric cancer. J Natl Cancer
Inst. 103:1552–1556. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang ZZ, Liu YJ, Yin XL, Zhan P, Gu Y and
Ni XZ: Loss of BRCA1 expression leads to worse survival in patients
with gastric carcinoma. World J Gastroenterol. 19:1968–1974. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC cancer staging manual. 7th. France:
Springer; 2010
|
|
17
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tsibulak I, Wieser V, Degasper C,
Shivalingaiah G, Wenzel S, Sprung S, Lax SF, Marth C, Fiegl H and
Zeimet AG: BRCA1 and BRCA2 mRNA-expression prove to be of clinical
impact in ovarian cancer. Br J Cancer. 119:683–692. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Al-Mulla F, Abdulrahman M, Varadharaj G,
Akhter N and Anim JT: BRCA1 gene expression in breast cancer: A
correlative study between real-time RT-PCR and
immunohistochemistry. J Histochem Cytochem. 53:621–629. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Garg K, Levine DA, Olvera N, Dao F,
Bisogna M, Secord AA, Berchuck A, Cerami E, Schultz N and Soslow
RA: BRCA1 immunohistochemistry in a molecularly characterized
cohort of ovarian high-grade serous carcinomas. Am J Surg Pathol.
37:138–146. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Peshkin BN, Alabek ML and Isaacs C:
BRCA1/2 mutations and triple negative breast cancers. Breast Dis.
32:25–33. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Galizia E, Giorgetti G, Piccinini G,
Santinelli A, Loretelli C, Bianchi F, Gagliardini D, Carbonari G,
Pisa E, Belvederesi L, et al: BRCA1 expression in triple negative
sporadic breast cancers. Anal Quant Cytol Histol. 32:24–29.
2010.PubMed/NCBI
|
|
23
|
Wang GH, Zhao CM, Huang Y, Wang W, Zhang S
and Wang X: BRCA1 and BRCA2 expression patterns and prognostic
significance in digestive system cancers. Hum Pathol. 71:135–144.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Meijer TG, Verkaik NS, Sieuwerts AM, van
Riet J, Naipal KAT, van Deurzen CHM, den Bakker MA, Sleddens HFBM,
Dubbink HJ, den Toom TD, et al: Functional ex vivo assay reveals
homologous recombination deficiency in breast cancer beyond BRCA
gene defects. Clin Cancer Res. 24:6277–6287. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Clark-Knowles KV, O'Brien AM and Weberpals
JI: BRCA1 as a therapeutic target in sporadic epithelial ovarian
cancer. J Oncol. 2010:8910592010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pothuri B: BRCA1- and BRCA2-related
mutations: Therapeutic implications in ovarian cancer. Ann Oncol.
24 Suppl 8:viii22–viii27. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang Q, Sakurai T, Mori I, Yoshimura G,
Nakamura M, Nakamura Y, Suzuma T, Tamaki T, Umemura T and Kakudo K:
Prognostic significance of BRCA1 expression in Japanese sporadic
breast carcinomas. Cancer. 92:54–60. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang Y, Wu H, Yang F, Ning J, Li M, Zhao
C, Zhong S, Gu K and Wang H: Prognostic value of the expression of
DNA repair-related biomarkers mediated by alcohol in gastric cancer
patients. Am J Pathol. 188:367–377. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yoshida K and Miki Y: Role of BRCA1 and
BRCA2 as regulators of DNA repair, transcription, and cell cycle in
response to DNA damage. Cancer Sci. 95:866–871. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Takata M, Tachiiri S, Fujimori A, Thompson
LH, Miki Y, Hiraoka M, Takeda S and Yamazoe M: Conserved domains in
the chicken homologue of BRCA2. Oncogene. 21:1130–1134. 2002.
View Article : Google Scholar : PubMed/NCBI
|