Introduction
Mediastinal tumor is a common chest tumor.
Mediastinum, an area defined by anatomy (1), contains all organs and tissues of the
chest from the sternum to the spine and between the lungs. These
organs and tissues are derived from different viviparous tissues,
so there is no specific pathogenic factor and obvious disease zone
of a high incidence in mediastinal tumor. So far, there are no
clear data showing the number of patients with mediastinal tumor in
the world, and it was only reported that there were 2,800 patients
with the disease in the United States in 2017 (2). Mediastinal tumor grows in the
mediastinal region that basically covers the whole thoracic cavity
of human body, so mediastinal tumors are various. At present,
mediastinal tumors are divided into neurogenic tumor (21%), thymoma
(19%), mediastinal cyst (21%), teratoma (15%) and others (24%)
(3). The main early clinical
features of children with mediastinal tumor include cough, dyspnea
and dysphagia (4), which are the
result of the tumor obstructing the respiratory, nervous, digestive
and circulatory systems in the body (5). The prevalence of mediastinal tumor in
children is lower than that in adults, but the tumor growth rate
and the carcinogenic rate in children are much higher than those in
adults due to the small thoracic volume and the immaturity of
tissues and organs in children (6).
Therefore, there is no time to delay the treatment of mediastinal
tumor in children.
At present, the main treatment of mediastinal tumor
is surgical resection (7).
Thoracotomy, a conventional resection operation (8), has an intuitive and clear visual field
and is convenient to remove the tumor. However, during the
operation, thoracotomy causes serious damage to human bone
structure and exposes the tissues and organs for a long time, which
leads to a high postoperative infection rate and incidence of
complications and thereby prolongs the cure cycle. As the era of
minimal invasiveness comes, video-assisted thoracoscopic surgery
(VATS) makes up for the above shortcomings (9) and fundamentally reduces postoperative
infection. In addition, VATS has small wound and does not damage
the cutaneous branch of the intercostal nerve, so patients have
milder pain, less bleeding and faster postoperative recovery.
However, VATS is a traumatic operation, so there is still
postoperative infection and pain stress, especially in children.
The postoperative trauma leads to stress in the body, among which,
the increase in nitric oxide (NO), interleukin-1β (IL-1β) and IL-6
levels activates the phagocytosis of phagocytes and granulocytes,
thereby stimulating inflammation. Therefore, the observation and
study of infection and pain stress indicators after the VATS
surgery in children with mediastinal tumor, especially
postoperative serum NO, IL-1β and IL-6 levels, may improve the
surgical effect and the well-being of patients (10,11). In
this study, serum pain stress indicators were detected to evaluate
the application value of VATS in the clinical treatment of
mediastinal tumor in children.
Patients and methods
Clinical information
In this study, a retrospective analysis was
performed on 82 children with mediastinal tumor undergoing
operation in Children's Hospital Affiliated to Zhengzhou University
(Zhengzhou, China) from January 2012 to January 2016, including 43
males and 39 females, aged 5–8 years. Of them, 48 children
undergoing VATS were enrolled as the observation group and 34
children undergoing traditional thoracotomy were enrolled as the
control group. Clinical records of the children in Children's
Hospital Affiliated to Zhengzhou University, Henan Children's
Hospital were recalled, and the basic clinical information was
collected, including demographic data, lesion location and lesion
diameter. This study was approved by the Ethics Committee of
Children's Hospital Affiliated to Zhengzhou University, and the
informed consent was signed by subjects' parents or their
guardians.
Inclusion and exclusion criteria
Inclusion criteria (12): All the patients admitted were aged
less than 14 years, and the mediastinal tumor was clinically
diagnosed as positive by CT; the patients included and their family
members were informed of the treatment and consented before
operation. Exclusion criteria: Patients undergoing secondary
mediastinal tumor resection; patients who refused to receive
surgery; patients with a tumor that could not be completely
resected with surgery or who were unable to receive resection
surgery; patients who had undergone chemotherapy and radiotherapy
before operation; patients who were unwilling to participate in
this study or with understanding disorder; patients with severe
cardiovascular disease, cardiac dysfunction, and abnormal lung
function; patients with obvious intestinal obstruction in the
gastrointestinal tract, and dilatation of the intestine; patients
who were suffering from various types of hernia; patients with
coagulopathy, massive ascites, internal bleeding, hepatitis, and
obesity; patients who had other serious medical diseases, including
hyperthyroidism, and diabetes; and patients who were unable to
tolerate tube intubation were excluded.
Study methods
The mediastinal tumor resection was clinically
carried out based on the clinical surgical guidelines (13) in accordance with the specifications,
with intraoperative operation time and blood loss and other
clinical real-time data observed and recorded. The fasting venous
blood from the children enrolled was collected before operation
(T0), at 12 h (T1) and 24 h (T2)
after operation and sent for examination to detect serum with
ELISA. The specific steps were as follows: the serum was separated
at room temperature, stored at −70°C and then slowly defrosted at
37°C when used. An automatic biochemical analyzer and corresponding
reagents (Mindray BS-220) were used to determine the expression
levels of serum NO (KS10788; Shanghai Keshun Biological Technology
Co., Ltd.), IL-1β (HL10417; Shanghai Haling Biological Technology
Co., Ltd.) and IL-6 (SBJ-H0465; Nanjing Senbeijia Biological
Technology Co., Ltd.), with the above operations carried out in
strict accordance with the instructions. The pain degree of the
children at T1 was observed, and then recorded using
visual analogue scale (VAS) (14),
and the length of stay and postoperative infection were
recorded.
Statistical analysis
SPSS 20.0 statistical software package (Yonghong
Technology Co., Ltd.) was used for processing the data. Measurement
data were expressed as mean ± standard deviation (mean ± SD), and
t-test was used for comparison between groups. Count data were
expressed as percentage [n/(%)], and Chi-square test was used for
comparison between groups. At P<0.05, the difference was
considered statistically significant.
Results
Comparison of basic clinical
information
In this study, 82 children with mediastinal tumor
were enrolled as subjects and separated into the observation group
(48 children) undergoing VATS and the control group (34 children)
undergoing conventional thoracotomy according to operation methods.
t-test and Chi-square test were used to analyze the clinical
information. The results showed that the differences were not
statistically significant in terms of age, sex or lesion between
the two groups (P>0.05) (Table
I). The two groups of patients were comparable.
 | Table I.Basic clinical information sheet of
patients [mean ± SD or n/(%)]. |
Table I.
Basic clinical information sheet of
patients [mean ± SD or n/(%)].
| Items | Observation group
(n=48) | Control group
(n=34) | t/χ2
value | P-value |
|---|
| Sex |
|
| 0.006 | 0.939 |
| Male | 25 (52.08) | 18 (52.94) |
|
|
|
Female | 23 (47.92) | 16 (47.06) |
|
|
| Age (years) | 5.1±1.6 | 5.5±1.2 | 0.186 | 0.853 |
| BMI
(kg/m2) | 21.3±1.5 | 22.1±1.3 | 0.382 | 0.703 |
| Lesion diameter
(cm) | 3.7±0.6 | 3.8±0.7 | 0.108 | 0.914 |
| Tumor metastasis |
|
| 0.009 | 0.909 |
| Yes | 12 (25.00) | 8 (23.53) |
|
|
| No | 36 (75.00) | 26 (76.47) |
|
|
| Tumor type |
|
Neurogenic tumor | 11 (22.92) | 11 (32.35) | 0.486 | 0.486 |
|
Teratoma | 16 (33.33) | 10 (29.41) | 0.018 | 0.893 |
|
Thymoma | 9 (18.75) | 7 (20.89) | 0.012 | 0.904 |
|
Others | 12 (25.00) | 6 (17.35) | 0.272 | 0.602 |
| Lesion
location |
|
Anterior mediastinum | 34 (70.83) | 26 (76.48) | 0.099 | 0.753 |
| Middle
mediastinum | 9 (18.75) | 4 (11.76) | 0.299 | 0.585 |
|
Posterior mediastinum | 5 (10.42) | 4 (11.76) | 0.088 | 0.918 |
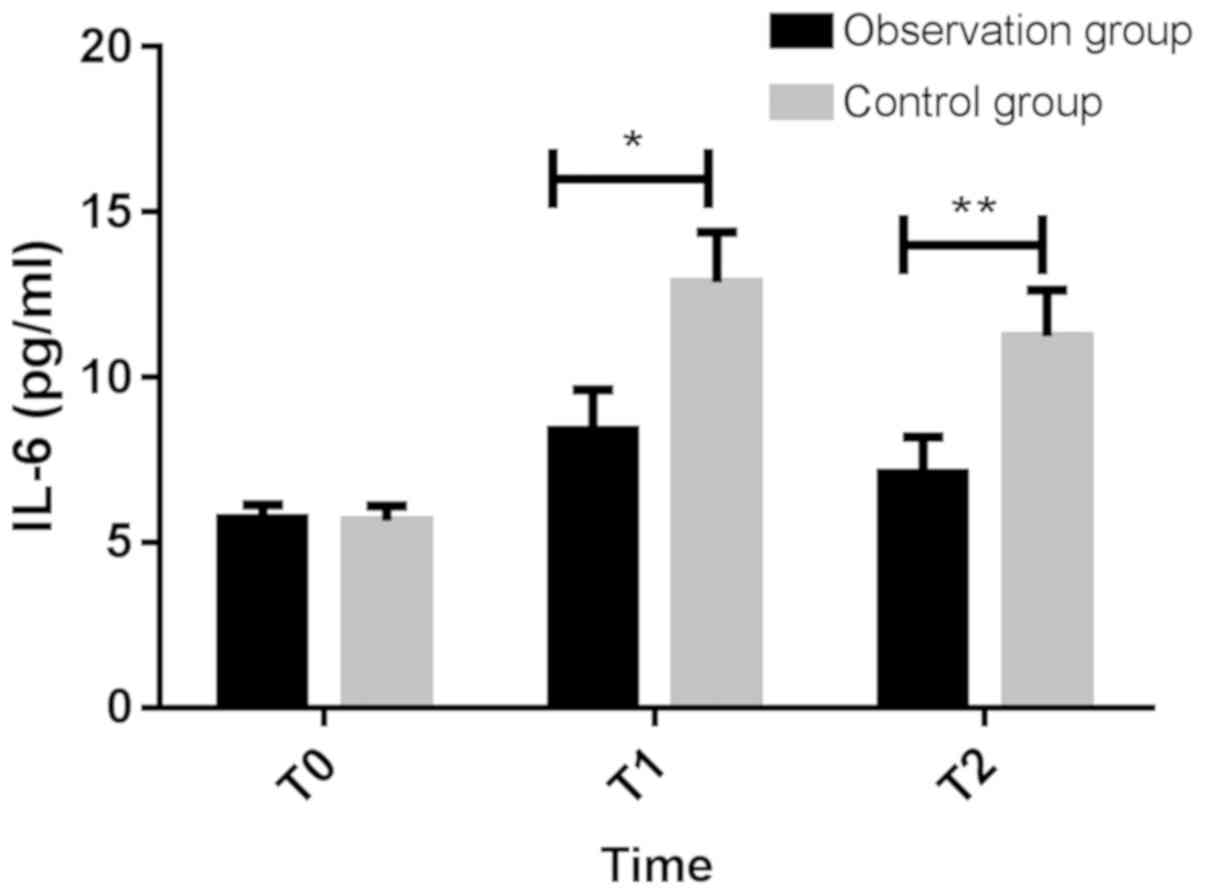
Comparison of stress indicators after
different operations
Pain stress indicators in the serum were detected at
T0 to T2 after operation (Table II and Figs. 1–3).
At T0, there were no significant differences between the
two groups with respect to NO, IL-1β and IL-6 (P>0.05), which
were lower in the observation group than those in the control group
at T1 and T2, with statistically significant
differences (P<0.05). The difference was the most significant at
T1 compared with that at T0. It showed that
VATS can effectively relieve postoperative pain thereby leading to
less pain stress.
| Table II.Serum NO, IL-1β and IL-6 levels
before and after operation (mean ± SD). |
Table II.
Serum NO, IL-1β and IL-6 levels
before and after operation (mean ± SD).
| Indicators | Time | Observation
group | Control group | t value | P-value |
|---|
| NO (normal range,
28.00–50.00 µmol/ml) |
|
| T° | 121.63±10.65 | 121.56±10.78 | 0.0005 | 0.996 |
|
| T1 | 152.69±16.86 | 207.11±18.50 | 2.145 | 0.035 |
|
| T2 | 137.35±13.66 | 184.60±17.28 | 2.168 | 0.033 |
| IL-1β (normal
range, 0.01–0.25 pg/ml) |
|
| T° | 1.63±0.14 | 1.61±0.16 | 0.0934 | 0.926 |
|
| T1 | 2.45±0.21 | 3.25±0.27 | 2.371 | 0.020 |
|
| T2 | 2.40±0.17 | 3.11±0.23 | 2.539 | 0.013 |
| IL-6 (normal range,
1.00–3.00 pg/ml) |
|
| T° | 5.71±0.43 | 5.65±0.46 | 0.0936 | 0.926 |
|
| T1 | 8.39±1.23 | 12.87±1.53 | 2.300 | 0.024 |
|
| T2 | 7.08±1.12 | 11.24±1.40 | 2.341 | 0.022 |
Intraoperative and postoperative
clinical indicators of children in the two groups
The intraoperative and postoperative clinical data
of children in the two groups were recorded, including operation
time, intraoperative blood loss, and pain score at T2
(Table III). Compared with the
control group, the largest blade opening, intraoperative blood
loss, drainage duration, length of stay and postoperative pain were
significantly improved in the observation group (P<0.05), and
the operation time was also shortened, indicating that VATS has a
higher clinical application value for the clinical resection of
mediastinal tumor in children within a certain range.
| Table III.Clinically relevant indicators of
children in the two groups (mean ± SD). |
Table III.
Clinically relevant indicators of
children in the two groups (mean ± SD).
| Clinical
information | Observation group
(n=48) | Control group
(n=34) | t value | P-value |
|---|
| Largest blade
opening (cm) | 5.13±0.48 | 15.32±3.46 | 3.442 | 0.0009 |
| Operation time
(min) | 90.49±29.00 | 173.94±28.72 | 1.999 | 0.050 |
| Intraoperative
blood loss (ml) | 81.99±30.28 | 172.37±32.64 | 1.996 | 0.049 |
| Postoperative
thoracic drainage duration (days) | 2.56±0.47 | 4.03±0.57 | 1.997 | 0.049 |
| Postoperative
length of stay (days) | 4.25±0.34 | 6.46±0.53 | 3.674 | 0.0004 |
| VAS score at
T2 | 2.93±0.66 | 5.37±0.63 | 2.530 | 0.013 |
Postoperative infection rate
The infection in children was recorded within 1
month after operation. The results showed that there were 8 cases
of postoperative infection in the two groups. Two cases were in the
observation group, and both cases were pulmonary infection. Six
cases were in the control group, including 3 cases of wound
infection, 1 case of pulmonary infection, and 2 cases of other
infection. IL-1β, NO and IL-6 were significantly higher in children
with infection than those without infection (P<0.001) (Table IV).
| Table IV.Comparison of infection. |
Table IV.
Comparison of infection.
| Indicators | Infection
(n=8) | No infection
(n=74) | t value | P-value |
|---|
| NO (µmol/ml) | 107.62±15.74 | 86.93±8.24 | 6.079 | <0.001 |
| IL-1β (pg/m) | 6.32±1.58 | 3.06±0.79 | 9.868 | <0.001 |
| IL-6 (pg/m) | 5.12±2.24 | 2.13±1.05 | 6.683 | <0.001 |
Discussion
Due to the promotion of medical knowledge in recent
years, people's awareness of minimally invasive surgery has
gradually developed. For operation methods, most parents of
children with mediastinal tumor are more likely to choose VATS
(15) that has a small wound area
and non-direct contact operation, with low trauma and infection
(16). However, VATS has some known
and unknown adverse effects on the quality of operation. Therefore,
paying close attention to the postoperative relevant indicators
remains a hot issue in medical studies. It has been shown that
(17) NO, IL-1β and IL-6 are
clinically common indicators for inflammatory pain stress, mainly
because they can better reflect the contraction and relaxation of
the smooth muscle during the inflammatory response. When the
content exceeds a certain amount, they stimulate the muscle to
contract and reflex, and reflect the pain in real time.
Because pediatric mediastinal tumor is not common in
clinical practice, existing studies mainly focus on the comparison
of the clinical efficacy of different treatment for mediastinal
tumors. For example, Fuchs et al (18) proposed that the laparoscopic
minimally invasive surgery has a good clinical effect in the
treatment of mediastinal tumors, and Christison-Lagay et al
(19) compared the effects of
different openings on pediatric mediastinal tumors. The
significance of the clinical indicators of postoperative pediatric
medial tumors is relatively rare. In this study, subjects were
enrolled through rigorous inclusion of exclusion criteria. The
differences between VATS and conventional thoracotomy in the
treatment of children with mediastinal tumor were compared, and the
significance of inflammatory factors NO, IL-1β and IL-6 for
perioperative period was analyzed, which provides reference for
future clinical treatment of pediatric mediastinal tumors.
Monitoring of common inflammatory factors may improve the quality
of surgical treatment. In this study, serum NO, IL-1β and IL-6
levels were used to investigate the adaptability of VATS or
traditional thoracotomy to mediastinal tumors.
The results of the study showed that postoperative
NO, IL-1β and IL-6 levels in the observation group (VATS) were
lower than those in the control group (conventional thoracotomy)
(P<0.05). Patients undergoing conventional thoracotomy have a
stronger postoperative stress response than those undergoing VATS,
suggesting that VATS can effectively reduce the postoperative pain
in children. Under normal circumstances, the human body responds to
external trauma, and operative trauma stimulates the patient to
secrete NO, IL-1β, IL-6 and other stress factors that stimulate the
nerve ending and thereby shows pain once exceeding normal content
(20,21). Rondón et al (22) have found that in the central nervous
system, NO, glutamic acid and polyamines are commonly mediated by
N-methyl-D-aspartate (NMDA) receptor, and the increase in NO
enhances the sensitivity to pain in the body. Gopalsamy et
al (11) reported that the
inhibition of IL-1β and IL-6 expression effectively inhibits the
pain stress response. In the study of different operation methods
for mediastinal tumor resection, Uchida et al (23) and Kamata et al (24) found that VATS is the first choice for
tumor resection. In the present study, a judgement of pain stress
indicators was added in the confirmation of results, which enhanced
the real-time control of operation. The VAS score at T2
also reflected that VATS was more suitable for children, and the
pain value was lower in the observation group at T2
(P<0.05). This is because the operative trauma of VATS is weak
and the recovery of children is better in a short time. The levels
of NO, IL-β and IL-6 in patients with postoperative infection were
significantly higher than those in patients without postoperative
infection, suggesting that the future clinical monitoring of NO,
IL-β and IL-6 concentrations in children can be used to judge the
occurrence of perioperative infections, so the recovery of patients
could be improved.
There is a study showing that painkillers reduce
cytokine levels (25). In this
study, children with a VAS score greater than 3 points were treated
with 0.15–0.20% ropivacaine (initial dose, 6–10 ml; maintenance
dose, 4–6 ml/h; aggressive dose: is 2–4 ml; the lockout time, 20–30
min; and the maximum dose, 12 ml/h). In this study, the analgesic
dose was selected in reference to the study of Kim et al
(26) who applied this dose in the
investigation of children with lower extremity orthopaedic surgery,
which significantly reduced the pain of children and has extremely
high application value. The VAS score at T2 was
2.93±0.66 in the observation group and 5.37±0.63 in the control
group. It can be seen that children in the control group generally
take more analgesic drugs than those in the observation group, so
NO, IL-1β and IL-6 levels measured in the control group should be
lower than their actual levels. However, postoperative NO, IL-1β
and IL-6 levels in the observation group were significantly lower
than those in the control group, indicating that their levels in
the observation group are significantly lower than the actual
levels in the control group.
The study of VATS in children with mediastinal tumor
is of great importance and value, and further in-depth research is
expected. Of course, not all children with mediastinal tumor are
suitable for VATS (27). For
example, children with a large tumor area, tumor metastasis and
proliferation and children who are too young (the body volume is
too small) can only choose thoracotomy or chemotherapy. Therefore,
the promotion of VATS in the clinic still needs to take the
condition of the patient into consideration. Since the pathogenesis
of pediatric mediastinal tumor is not completely clear, the exact
mechanism of NO, IL-1β, IL-6 in mediastinal tumor requires to be
further explored. Because pediatric mediastinal tumor is not
common, we are unable to expand the sample size, and the results
could be slightly different with more subjects included.
In conclusion, compared with thoracotomy, VATS is
more suitable for children with the disease, the recovery and
infection of children could be monitored by detecting the
inflammatory factors NO, IL-1β, IL-6, which has a higher promotion
value in clinical practice.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
BZ drafted this manuscript. BZ, YZ and ZhenliangC
were mainly devoted on collecting and interpreting the data. FY, XD
and ZhongjianC performed ELISA. YC and PW helped with the pain
degree of patients analysis. LS and WY were responsible for
statistical analysis. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Children's Hospital Affiliated to Zhengzhou University (Zhengzhou,
China). Signed informed consents were obtained from their parents
or legal guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bohnenberger Η, Dinter Η, König A and
Ströbel P: Neuroendocrine tumors of the thymus and mediastinum. J
Thorac Dis. 9 (Suppl 15):S1448–S1457. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siddiqi MS, Al Badai Y, Al Kemyani NA and
Al Kindi AH: Combined transcervical and thoracoscopic mediastinal
parathyroid adenoma resection. Asian Cardiovasc Thorac Ann.
24:593–596. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chen L, Wang M, Fan H, Hu F and Liu T:
Comparison of pediatric and adult lymphomas involving the
mediastinum characterized by distinctive clinicopathological and
radiological features. Sci Rep. 7:25772017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Madariaga ML, Borges LF, Rabinov JD, Chang
DC, Lanuti M, Mathisen DJ and Gaissert HA: Angiography before
posterior mediastinal tumor resection: Selection criteria and
patient outcomes. Ann Thorac Surg. 105:1000–1007. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jaramillo D: Soft tissue tumors in
children. Musculo-skeletal Diseases 2017–2020. Hodler J, Kubik-Huch
R and von Schulthess G: Springer; Cham: pp. 167–172. 2017,
View Article : Google Scholar
|
|
7
|
Zhang L, Liu X, Li X, Tang Z, Shi C and
Wang G: Diagnosis and surgical treatment of mediastinal solitary
fibrous tumor. Asia Pac J Clin Oncol. 13:e473–e480. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Clark A, Ozdirik J and Cao C: Thoracotomy,
video-assisted thoracoscopic surgery and robotic video-assisted
thoracoscopic surgery: Does literature provide an argument for any
approach? Video-assist Thorac Surg. 2:212017. View Article : Google Scholar
|
|
9
|
Brodsky JB and Cohen E: Video-assisted
thoracoscopic surgery. Curr Opin Anaesthesiol. 13:41–45. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Waltz P, Escobar D, Botero AM and
Zuckerbraun BS: Nitrate/nitrite as critical mediators to limit
oxidative injury and inflammation. Antioxid Redox Signal.
23:328–339. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gopalsamy B, Farouk AA, Tengku Mohamad TA,
Sulaiman MR and Perimal EK: Antiallodynic and antihyperalgesic
activities of zerumbone via the suppression of IL-1β, IL-6, and
TNF-α in a mouse model of neuropathic pain. J Pain Res.
10:2605–2619. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Baxter KJ, Gale BF, Travers CD, Heiss KF
and Raval MV: Ramifications of the children's surgery verification
program for patients and hospitals. J Am Coll Surg. 226:917–924.e1.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mayo JR, Clifton JC, Powell TI, English
JC, Evans KG, Yee J, McWilliams AM, Lam SC and Finley RJ: Lung
nodules: CT-guided placement of microcoils to direct video-assisted
thoracoscopic surgical resection. Radiology. 250:576–585. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Price DD, McGrath PA, Rafii A and
Buckingham B: The validation of visual analogue scales as ratio
scale measures for chronic and experimental pain. Pain. 17:45–56.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hanna AM and VanderWel B: Thoracoscopic
approach to pediatric mediastinal masses. The SAGES Manual of
Pediatric Minimally Invasive Surgery. Walsh D, Ponsky T and Bruns
N: Springer; Cham: pp. 239–259. 2017, View Article : Google Scholar
|
|
16
|
Wang L, Liu D, Lu J, Zhang S and Yang X:
The feasibility and advantage of uniportal video-assisted
thoracoscopic surgery (VATS) in pulmonary lobectomy. BMC Cancer.
17:752017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Thobakgale C and Naidoo K, McKinnon LR,
Werner L, Samsunder N, Karim SA, Ndung'u T, Altfeld M and Naidoo K:
Interleukin 1-beta (IL-1β) production by innate cells following TLR
stimulation correlates with TB recurrence in ART-treated
HIV-infected patients. J Acquir Immune Defic Syndr. 74:213–220.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fuchs J, Schafbuch L, Ebinger M, Schäfer
JF, Seitz G and Warmann SW: Minimally invasive surgery for
pediatric tumors - current state of the art. Front Pediatr.
2:482014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Christison-Lagay ER, Darcy DG, Stanelle
EJ, Dasilva S, Avila E and La Quaglia MP: ‘Trap-door’ and
‘clamshell’ surgical approaches for the management of pediatric
tumors of the cervicothoracic junction and mediastinum. J Pediatr
Surg. 49:172–176; discussion 176–177. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mann E and Carr E: Pain management.
Foundation Studies for Caring: Using Student-Centred Learning.
Palgrave Macmillan; New York, NY: pp. p2592018
|
|
21
|
Salman AH, Iqbal MN and Bakir WA: The
in situ expression of IL-6 and IL-1β in breast cancer
patients. Iraqi J Pharm Sci. 17:55–62. 2017.
|
|
22
|
Rondón LJ, Farges MC, Davin N, Sion B,
Privat AM, Vasson MP, Eschalier A and Courteix C: L-Arginine
supplementation prevents allodynia and hyperalgesia in painful
diabetic neuropathic rats by normalizing plasma nitric oxide
concentration and increasing plasma agmatine concentration. Eur J
Nutr. 57:2353–2363. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Uchida T, Matsubara H, Nagasaka S, Kina S,
Ichihara T, Matsuoka H and Nakajima H: Video-assisted thoracoscopic
surgery can help enable the complete resection of a mediastinal
tumor caused by immunoglobulin G4-related disease and avoid the
need for postoperative medication: A case report. Asian J Endosc
Surg. 11:248–251. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kamata T, Shiba M, Fujiwara T, Nagato K,
Yoshida S, Inoue T and Iida T: Chylopericardium following
thoracoscopic resection of a mediastinal cyst: A case report. Int J
Surg Case Rep. 39:126–130. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang LZ, Hu XX, Liu X, Qian P, Ge JM and
Tang BL: Influence of epidural dexamethasone on maternal
temperature and serum cytokine concentration after labor epidural
analgesia. Int J Gynaecol Obstet. 113:40–43. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim DH, Kim N, Lee JH, Jo M and Choi YS:
Efficacy of preemptive analgesia on acute postoperative pain in
children undergoing major orthopedic surgery of the lower
extremities. J Pain Res. 11:2061–2070. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Doğusoy I, Yıldırım M, Ustaalioğlu R and
Demirbağ H: A comparison of axillary thoracotomy versus
video-assisted thoracoscopic surgery in the surgical treatment of
primary spontaneous pneumothorax. Turk Gogus Kalp Dama. 26:132–137.
2018. View Article : Google Scholar
|