Introduction
Gastric cancer (GC) is the third leading cause of
cancer-associated deaths worldwide (1). The 5-year survival rate of patients
with advanced GC is only 5–20%, with a median overall survival of
10 months worldwide (2,3). Therefore, early detection of GC is
crucial for improving patient survival rates (4). Currently, endoscopy and pathological
examination are the diagnostic gold standard; however, these
procedures are invasive and costly. The detection of biomarkers in
peripheral blood is a useful method for GC screening. The
traditional tumor markers used for GC detection include
carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9)
and carbohydrate antigen 72-4 (CA72-4) (5). However, previous studies by our group
(5) and Wang et al (6) have demonstrated that the sensitivity
and specificity of the three traditional markers are insufficient
for the diagnosis of GC, which limits their clinical utility. Thus,
the identification of a diagnostic marker with high sensitivity and
specificity for patients with GC is urgently required.
In the past decade, there has been notable progress
in the field of study of extracellular vesicles (EVs), which have
attracted increasing attention due to their widespread prevalence
in various body fluids (7,8), ease of access (9,10) and
association with various diseases (11). EVs are a heterogeneous population of
cell-derived vesicles secreted by various cell types to mediate
their intracellular communication (12). Following uptake by recipient cells,
EVs serve a certain role in cancer progression; for example, Abd
Elmageed et al (13) have
reported that microRNA (miRNA or miR)-125b, miR-130 and miR-155, as
well as HRas and Kras mRNAs in EVs from prostate cancer cells
participate in neoplastic reprogramming and tumor formation of
adipose stem cells. This hypothesis also has been supported by
Zhang et al (14), who
demonstrated that EVs derived from GC cells induce neutrophils to
polarize to N2 tumor-associated neutrophils, thus promoting GC cell
migration. EV membranes are enriched in various protein markers
including CD9, CD63 and tumor susceptibility gene 101 (TSG101)
(5). By means of EVs, various
molecules such as lipids, proteins and nucleic acids [(DNA, mRNA
and long non-coding RNA (lncRNA)] can be transferred from donor to
recipient cells (15), suggesting
that this mechanism may be involved in GC progression. In addition,
circulating EVs are present in liquid biopsies and may be used as
diagnostic markers of GC (16,17);
therefore, EVs may have potential diagnostic value in GC.
lncRNAs have been reported to serve crucial roles in
cancer development and progression (18). lncRNAs have a number of functions in
various biological processes, including the cis or trans
transcriptional and post-transcriptional regulation of RNA
(19). An increasing number of
lncRNAs have been demonstrated to participate in GC progression.
For example, knockdown of lncRNA AF147447 promotes GC cell
proliferation and invasion by directly binding to miR-34c (20). Gastric cancer metastasis-associated
lncRNA (GMAN) promotes the expression of EphrinA1 through the
GMAN-antisense pathway, promoting GC metastasis (21). In addition, circulating EVs loaded
with specific bioactive molecules reflect the status of GC
progression and metastasis (4). The
EV-mediated transfer of lncRNA HOX transcript antisense RNA
(HOTAIR) promotes cisplatin resistance in liver cancer cells by
regulating the high mobility group AT-hook (HMGA)1/miR-218 axis
(22). lncRNAs in EVs are stably
present in circulation and are regarded as useful markers that are
reflective of disease status. Previous studies have reported that
certain EV lncRNAs are highly expressed in the serum of patients
with GC, including LINC00152, lncRNA HOTTIP and lncUEGC1 (23–25). The
results of the aforementioned studies suggest that EV lncRNAs may
be used as auxiliary biomarkers of GC. However, certain
limitations, such as their lack of clinical efficiency and clinical
effect require further consideration.
lncRNA colon cancer-associated transcript-1 (CCAT1)
is an oncogenic lncRNA located on chromosome 8q24, close to the
gene encoding c-Myc (26). lncRNA
CCAT1 has been reported to be elevated in certain types of cancer,
such as GC (27), colorectal cancer
(CRC) (28) and hepatocellular
carcinoma (29). Additionally,
lncRNA CCAT1 serves a crucial role in various biological processes,
such as cell proliferation and invasion (30). Aberrant expression of lncRNA CCAT1
affects tumorigenesis, tumor size, lymph node metastasis,
Tumor-Node-Metastasis (TNM) stage, tumor differentiation and
invasion (31,32). A previous study by Shen et al
(33) has revealed that lncRNA CCAT1
serves a role in cervical cancer by promoting cell proliferation
and invasion via the regulation of the miR-181a-5p/MMP14 axis. You
et al (34) have also
demonstrated that CCAT1 promotes the proliferation of prostate
cancer cells by facilitating androgen receptor (AR) expression as a
scaffold for DEAD-box helicase 5 (P68) and the AR transcriptional
complex, and by acting as a sponge of miR-28-5p to prevent its
anticancer effects. lncRNA CCAT1 can be used as a diagnostic
marker; Abedini et al (35)
have demonstrated that the levels of plasma lncRNA CCAT1 in
patients with CRC are higher compared with those in healthy control
subjects. In GC, lncRNA CCAT1 contributes to tumor growth and
invasion by targeting miR-219-1 (36). This suggests that lncRNACCAT1 is
involved in the progression of GC and may serve as a potential
biomarker.
lncRNAs can exist stably in the peripheral
circulation and are protected by EVs. As markers, EVs have a good
diagnostic value in GC; for example, a previous study has
demonstrated that lncRNA zinc finger NFX1-type containing 1
antisense RNA 1 levels are elevated in the serum exosomes of
patients with GC compared with those in healthy controls (37). Furthermore, Li et al (23) have determined that plasma LINC00152
levels are significantly higher in patients with GC compared with
those in healthy controls. lncRNA CCAT1 has also been identified in
the plasma and serum EVs of patients with CRC (38,39).
However, to the best of our knowledge, there no studies are
currently available on EV lncRNA CCAT1 in patients with GC.
Therefore, the current study aimed to identify the levels of lncRNA
CCAT1 in the serum EVs of patients with GC and evaluate its
expression and diagnostic value. In addition, the correlation of
lncRNA CCAT1 with various clinicopathological variables was
assessed. The present study further aimed to identify a reliable
biomarker in the diagnosis of GC.
Materials and methods
Patients and control subjects
Serum samples of 27 healthy control subjects, 26
patients with chronic gastritis, 30 patients with atypical
hyperplasia and 113 patients with GC were collected at the Qilu
Hospital of Shandong University between January and December 2017.
Peripheral blood samples from the GC group were collected before
surgery. The age ranges in the subject groups were as follows:
Healthy controls, 29–62 (male subjects, n=8) and 30–66 (female
subjects, n=19); chronic gastritis, 32–69 (male patients, n=14) and
33–65 (female patients, n=12); atypical hyperplasia 33–73 (male
patients, n=21) and 41–73 (female patients, n=9); GC, 25–82 (male
patients, n=84) and 23–74 (female patients, n=29) years. In
addition, 16 paired GC and adjacent non-cancerous tissues were
collected during surgical resection and stored at −80°C
immediately. The distance between the tumor margin and the adjacent
non-tumor tissue ≥5 cm. The demographic and clinicopathological
characteristics of all participants were recorded. GC was diagnosed
by two pathologists and staged according to the Union for
International Cancer Control/American Joint Committee on Cancer TNM
staging system (8th edition) (40).
No patients had received any adjuvant therapy such as radiotherapy
or chemotherapy prior to sample collection. The inclusion criteria
for the healthy control subjects were routine blood test,
biochemical index, tumor marker and imaging test results determined
to be within the reference range during physical examination.
Outliers were defined through Tukey's box-plot method (41), and 4, 5, 3 and 6 suspected outliers
were removed from healthy controls, patients with chronic
gastritis, atypical hyperplasia and GC, respectively. In addition,
four pairs of GC and adjacent non-cancerous tissues were removed as
outliers. The present study was approved by the Medical Ethics
Committee of Qilu Hospital of Shandong University (approval no.
KYLL-2015-097). All participants provided signed informed
consent.
Isolation of EVs from serum
Serum was collected from 5 ml venous blood by
centrifuging at 3,000 × g for 10 min at room temperature. The
samples were filtered through a 0.22-µm filter (Millipore Sigma) to
eliminate cell fragments and organelles. Two methods were used to
isolate EVs. For the commercial kit method, the serum was
centrifuged at 50,000 × g for 60 min to remove large microbubbles,
and the subsequent procedures were performed according to the
manufacturer's instructions of the exoEasyMaxi kit (cat. no. 76064;
Qiagen GmbH). Briefly, 1 ml serum was mixed with 1 ml XBP buffer
and added to the exoEasy spin column (in a 50-ml collection tube to
bind EVs). Following centrifugation at 500 × g for 60 sec, 10 ml
XWP buffer was added and centrifuged at 5,000 × g for 5 min, and
400 µl XE buffer was used to elute EVs at 500 × g for 5 min. For
ultracentrifugation, 1 ml serum was diluted 1:7 in PBS and
centrifuged at 120,000 × g for 2 h. A lamellar precipitate was
observed at the bottom of the tube, the main component of which was
EVs. The supernatant was discarded and the EVs were resuspended
with 100 µl PBS. All centrifugation steps were performed at 4°C
unless stated otherwise.
Transmission electron microscopy
(TEM)
A total of 10 µl EV suspension was added to a
200-mesh carbon film copper net. The carbon film was allowed to
absorb EVs for 20 min in a dry environment. The copper net was
sequentially placed in 50 µl 11% glutaraldehyde, 100 µl
ddH2O, 50 µl uranyl acetate and 50 µl
methylcellulose-uranyl acetate droplets. The excess liquid was
gently removed using filter paper, leaving a thin methylcellulose
film, which was dried for 5–10 min at room temperature. The samples
were observed in 5–10 fields per sample under a Hitachi HT7800
transmission electron microscope (Hitachi High-Tech Corporation) at
80 kV under ×40,000 magnification.
Measurement of size distribution
The size distribution of EVs was observed on a
ZetaView analyzer (Particle Metrix GmbH) according to the
manufacturer's instructions. Nanoparticle Tracking Analysis (NTA)
was used to capture the Brownian motion of each particle in the
video. Based on the different diffusion movements of large and
small particles in the surrounding liquid, the hydrodynamic
diameters of particles were determined. In addition, the charge
state of particle surface (zeta potential) was measured by
determining the movement of particles in an applied electric
field.
EV protein quantification and western
blot analysis
EVs were suspended in RIPA lysis buffer (cat. no.
P0013B; Beyotime Institute of Biotechnology) on ice to dissolve the
protein. Total protein concentration was determined by BCA protein
detection kit (cat. no. P0012; Beyotime Institute of
Biotechnology). The extracted protein was diluted with loading
buffer 4:1 and incubated at 100°C for 5 min. A total of ~20 µg EV
protein per lane was separated by 10% sodium dodecyl sulfate
polyacrylamide gel electrophoresis, transferred to PVDF membranes,
blocked in 5% non-fat milk for 1 h and incubated overnight at 4°C
with primary mouse anti-CD63 (cat. no. ab59479; 1:1,000; Abcam),
rabbit anti-TSG101 (cat. no. ab125011; 1:1,000; Abcam), rabbit
anti-CD9 (cat. no. 13403s; 1:1,000; Cell Signaling Technology,
Inc.), rabbit anti-GAPDH (cat. no. AB-P-R 001; 1:1,000; Hangzhou
Good Here Biotechnology Co., Ltd.) and rabbit anti-calnexin (cat.
no. 2679s; 1:1,000; Cell Signaling Technology, Inc.) antibodies.
The washing reagent TBST (cat. no. T1081; Beijing Solarbio Science
& Technology Co., Ltd.) used to remove the primary antibodies
The horseradish peroxidase-labeled goat anti mouse (cat. no. A0216;
1:2,000; Beyotime Institute of Biotechnology) or goat anti rabbit
antibody (cat. no. A0208; 1:2,000; Beyotime Institute of
Biotechnology) was used to imprint the target protein and incubated
at room temperature for 1 h. The diluent for the secondary antibody
(cat. no. WB100D) was purchased from New Cell & Molecular
Biotech Co., Ltd. The protein signals were detected by an enhanced
chemiluminescence detection system (Amersham Imager 680;
Cytiva).
RNA extraction and reverse
transcription-quantitative (RT-q)PCR
Serum and tissue RNAs were extracted using an
exoRNeasy Serum/Plasma Midi kit (cat. no. 77044; Qiagen GmbH) and
RNAprep pure FFPE kit [cat. no. DP439; TIANGEN Biotech (Beijing)
Co., Ltd.] according to the manufacturer's instructions. An
All-in-one™ First-Strand cDNA Synthesis kit (cat. no. QP006;
GeneCopoeia, Inc.) was used to reverse-transcribe an equal amount
of total RNA from each sample to cDNA according to the
manufacturer's instructions. cDNA was diluted 1:5 with
ddH2O, and qPCR was performed using a CFX96 qPCR
instrument (Bio-Rad Laboratories, Inc.) with an All-in-one™ qPCR
Mix (cat. no. QP001; GeneCopoeia, Inc.). The primers used were
lncRNA CCAT1 forward, 5′-AGGGGCTCTCCTTTTGTTCG-3′ and reverse,
5′-GATTTCAGCAGCGAGGGTCT-3′ (88 bp); GAPDH (cat. no. B662104; 138
bp) was purchased from Sangon Biotech Co., Ltd. The thermocycling
conditions were as follows: Initial denaturation at 95°C for 10
min, followed by 40 cycles of 95°C for 15 sec, 62°C for 20 sec and
72°C for 10 sec. The amplification specificity was determined by
melting curve analysis. Data were normalized to GAPDH, and relative
expression levels were evaluated using the 2−ΔΔCq method
(42). No template reaction and no
RT reaction were used as negative controls.
Stability of serum EV lncRNA CCAT1 in
harsh environments
EVs from patient serum were divided into three
groups that were untreated (control), treated with RNase A or
treated with RNase A plus 0.1% Triton X-100 for 45 min at 37°C,
respectively. In order to evaluate the stability of lncRNA CCAT1 in
serum EVs in harsh environments, serum samples were stored at room
temperature or 4°C for 24 or 48 h. In addition, serum samples were
frozen and thawed three times at −80°C, and fresh serum used as a
control. Following these treatments, the expression levels of
lncRNA CCAT1 were detected by RT-qPCR.
Fecal occult blood tests
The bleeding of digestive tract was measured by
colloidal gold-based Fecal Occult Blood diagnostic kit (Shanghai
Chemtron Biotech Co., Ltd.).
Online bioinformatics analysis
The expression levels of EV lncRNA CCAT1 were
assessed in various diseases using the online database exoRBase
(http://www.exorbase.org/), which is a
repository of lncRNAs derived from RNA-seq data analyses of human
blood exosomes (43). GEPIA
(http://gepia.cancer-pku.cn/index.html) was used to
obtain the Kaplan-Meier curve to analyze the association between
the expression of CCAT1 and survival times (months) of patients,
including overall survival (OS) and disease-free survival
(DFS).
Statistical analysis
Data are presented as the median and interquartile
ranges or the mean ± SD. SPSS version 25.0 (IBM Corp.) and MedCalc
version 8.0 (MedCalc Software, Ltd.) were used for statistical
analyses. The Kolmogorov-Smirnov test was used to determine the
data distribution in each group. Serum EV lncRNA CCAT1 levels were
evaluated by the Mann Whitney U or Kruskal Wallis test in different
groups based on patient clinicopathological characteristics. Data
on the stability of serum EV lncRNA CCAT1 were analyzed using
one-way ANOVA followed by Tukey's post hoc test or two-way ANOVA
followed by Bonferroni post hoc test. lncRNA CCAT1 levels in paired
samples of GC tissues were analyzed with Wilcoxon's signed rank
test. Receiver operating characteristic (ROC) curves were used to
evaluate the diagnostic value of biomarkers in GC, and area under
the curve (AUC) was calculated. The cut-off value was calculated
using the Jordan index (sensitivity + specificity-1). OS and DFS
were analyzed by Kaplan-Meier estimates and examined by log-rank
test. The correlations between EV lncRNA CCAT1 in the serum of
patients with GC and CCAT1 in GC tissues were determined by
Spearman's correlation analysis. P<0.05 was considered to
indicate a statistically significant difference.
Results
Characterization of serum EVs
EVs were extracted using a commercial kit and
ultracentrifugation. The results of TEM analysis demonstrated that
EVs presented with a unique morphology with dish-like vesicles and
a double-lipid layer (Fig. 1A). In
addition, NTA revealed that the diameters of EVs extracted using a
commercial kit and ultracentrifugation were 125.6±51.7 and
119.5±51.8 nm, respectively (Fig.
1B). The zeta potentials for the commercial kit and
ultracentrifugation were-21.41±1.93 and −16.46±1.90 mV (P=0.061),
respectively (data not shown). Surface marker proteins including
CD9, CD63, TSG101, the negative control protein calnexin and GAPDH
(used as a loading control) were identified in the two groups of
EVs (Fig. 1C). The EVs obtained
using the commercial kit were similar to those obtained by
ultracentrifugation.
Serum EV lncRNA CCAT1 levels in
patients with GC, chronic gastritis and atypical hyperplasia as
well as healthy control subjects
The results of the bioinformatics analysis revealed
that the levels of lncRNA CCAT1 were upregulated in hepatocellular
carcinoma and pancreatic adenocarcinoma compared with those in
healthy controls (Fig. S1).
However, there no data were available for lncRNA CCAT1 expression
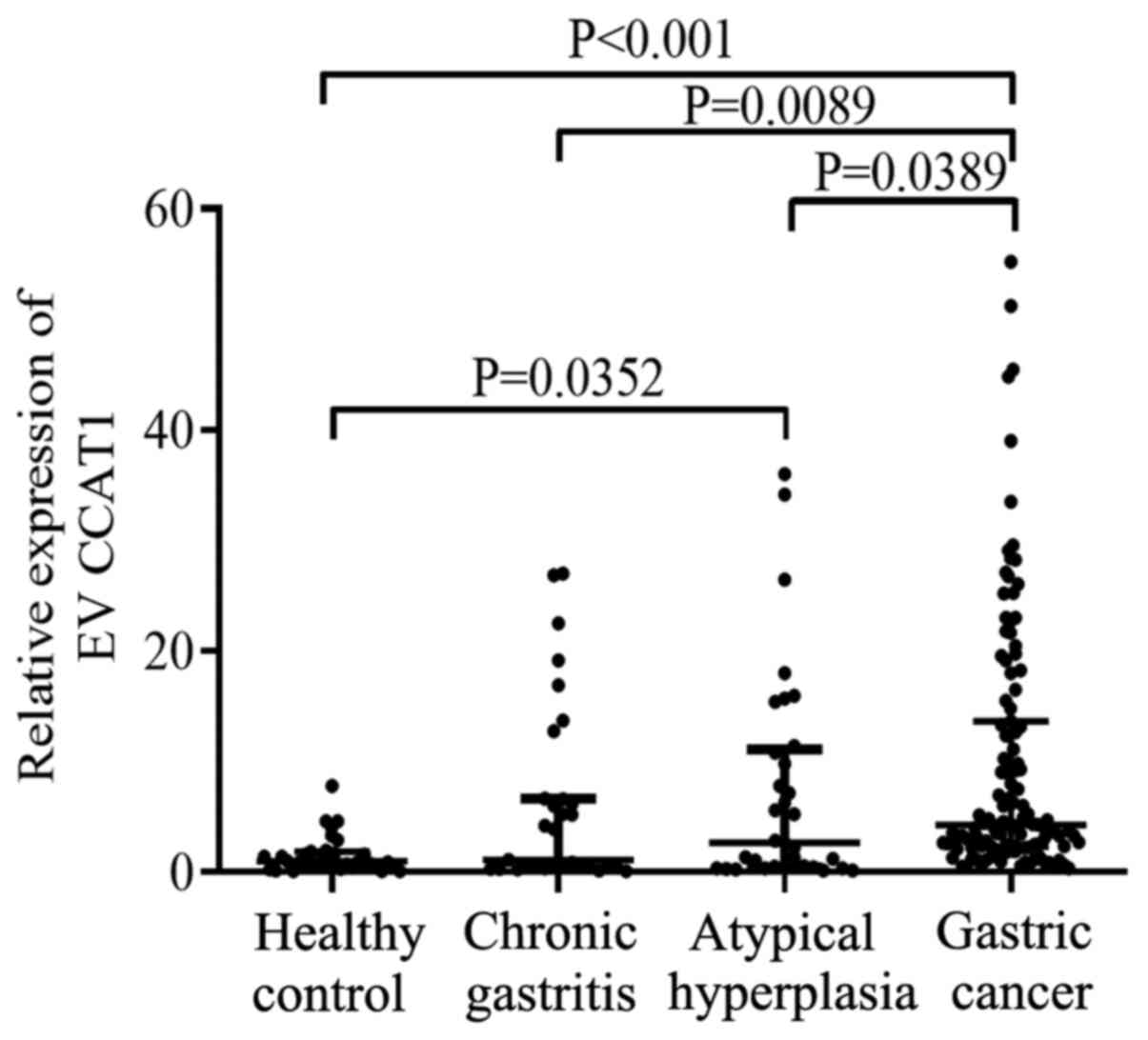
in patients with GC. The data obtained in the current study
revealed that serum EV lncRNA CCAT1 levels in patients with GC
[4.170 (2.250–11.740)] were significantly higher compared with
those in the healthy controls [0.910 (0.400–1.630)], patients with
chronic gastritis [0.710 (0.406–5.453)] and atypical hyperplasia
[1.812 (0.434–8.321)] (all P<0.05). Furthermore, lncRNA CCAT1
expression levels were higher in patients with atypical hyperplasia
compared with those in healthy controls (P<0.05; Fig. 2). No differences were observed in the
CCAT1 expression levels between patients with chronic gastritis and
healthy controls or patients with atypical hyperplasia.
Correlation between serum EV lncRNA
CCAT1 levels and the clinicopathological features of patients with
GC
The current study evaluated the clinical value of
CEA and EV lncRNA CCAT1 in patients with GC. The results
demonstrated that high expression levels of EV lncRNA CCAT1 were
significantly associated with the depth of invasion (P=0.040),
distant metastasis (P<0.001) and TNM stage (P<0.001).
However, there was no significant association between EV lncRNA
CCAT1 levels and patient sex, age, cancer location, Bormann
classification, tumor diameter, differentiation, lymphatic
metastasis, hypertension or fecal occult blood (Table I). CEA levels were associated with
tumor diameter, depth of invasion and TNM stage (5).
 | Table I.Extracellular vesicle long non-coding
RNA CCAT1 expression levels and patient clinicopathological
characteristics. |
Table I.
Extracellular vesicle long non-coding
RNA CCAT1 expression levels and patient clinicopathological
characteristics.
| Variable | n | CCAT1, median
(interquartile range) | U value | P-value |
|---|
| Sex |
|
| 1,171.500 | 0.760 |
|
Male | 84 | 4.200 (2.285,
10.910) |
|
|
|
Female | 29 | 4.070 (2.200,
13.505) |
|
|
| Age, years |
|
| 1,315.500 | 0.111 |
|
≤61 | 59 | 3.560 (2.200,
9.080) |
|
|
|
>61 | 54 | 4.465 (2.493,
16.155) |
|
|
| Cancer
location |
|
| 5.625a | 0.131 |
|
Antrum | 44 | 3.405 (2.026,
7.400) |
|
|
|
Angulus | 21 | 3.690 (1.300,
10.190) |
|
|
|
Cardia | 27 | 6.020 (2.610,
21.690) |
|
|
|
Body | 21 | 4.280 (2.740,
16.180) |
|
|
| Tumor diameter |
|
| 1,352.000 | 0.161 |
| ≤3
cm | 56 | 3.625 (2.255,
6.603) |
|
|
| >3
cm | 57 | 4.370 (2.235,
15.185) |
|
|
|
Differentiation |
|
| 3.821a | 0.148 |
| Well
differentiated | 12 | 3.565 (1.678,
4.583) |
|
|
|
Moderately differentiated | 25 | 2.700 (1.715,
11.090) |
|
|
| Poorly
differentiated | 76 | 4.715 (2.345,
14.553) |
|
|
| Bormann type |
|
| 0.180a | 0.981 |
| I | 18 | 4.085 (2.330,
7.472) |
|
|
| II | 55 | 4.230 (2.200,
14.840) |
|
|
|
III | 25 | 4.340 (2.420,
12.780) |
|
|
| IV | 15 | 3.580 (2.110,
12.670) |
|
|
| Invasion depth |
|
| 8.307a | 0.040 |
| T1 | 26 | 3.525 (2.350,
5.618) |
|
|
| T2 | 21 | 3.040 (1.210,
4.715) |
|
|
| T3 | 22 | 6.650 (2.790,
17.353) |
|
|
| T4 | 44 | 4.705 (2.268,
17.405) |
|
|
| Lymphatic
metastasis |
|
| 1,252.500 | 0.074 |
| No | 48 | 3.445 (2.028,
6.525) |
|
|
|
Yes | 65 | 4.470 (2.400,
15.185) |
|
|
| Distant
metastasis |
|
| 289 | <0.001 |
| No | 95 | 3.560 (2.110,
6.690) |
|
|
|
Yes | 18 | 20.135 (8.815,
25.645) |
|
|
|
Tumor-Node-Metastasis stage |
|
| 21.851a | <0.001 |
| I | 37 | 3.140 (1.685,
4.995) |
|
|
| II | 28 | 3.935 (2.038,
11.840) |
|
|
|
III | 30 | 3.905 (2.178,
9.135) |
|
|
| IV | 18 | 20.135 (8.815,
25.645) |
|
|
| Hypertension |
|
| 1,018.500 | 0.190 |
| No | 84 | 3.775 (2.208,
9.228) |
|
|
|
Yes | 29 | 6.020 (2.360,
18.150) |
|
|
| Fecal occult
blood |
|
| 1,017.500 | 0.076 |
| No | 81 | 4.340 (2.455,
13.260) |
|
|
|
Yes | 32 | 3.090 (1.978,
7.328) |
|
|
Diagnostic value of serum EV lncRNA
CCAT1 levels in GC
Serum EV lncRNA CCAT1 levels were significantly
higher in patients with stage III+IV GC [7.250 (2.525–19.630)]
compared with those in patients with stage I+II GC [3.490
(1.955–6.185)] (P=0.012; Fig. 3A).
This suggested that EV lncRNA CCAT1 may be a reliable biomarker of
GC. The predictive value of EV lncRNA CCAT1 was subsequently
determined. The AUC of EV lncRNA CCAT1 was [0.890; 95% confidence
interval (CI), 0.826–0.937)], which indicated a good capability to
diagnose patients with GC. The cut-off, sensitivity and specificity
values of EV lncRNA CCAT1 were 1.990, 79.6 and 92.6%, respectively
(Table II). lncRNA CCAT1 and CEA
were combined to assess their ability to diagnose GC. ROC analysis
demonstrated that the AUC of the combined markers was 0.910 (95%
CI, 0.849–0.951; Fig. 3B). The
sensitivity and specificity of combined lncRNA CCAT1 and CEA were
80.5 and 92.6%, respectively.
| Table II.Predictive value of CEA and long
non-coding RNA CCAT1 in extracellular vesicles in gastric
cancer. |
Table II.
Predictive value of CEA and long
non-coding RNA CCAT1 in extracellular vesicles in gastric
cancer.
| Marker | Cut-off | Sens (95% CI) | Spec (95% CI) | AUC (95% CI) |
|---|
| CCAT1 | 1.990 | 79.600
(71.000–86.600) | 92.600
(75.700–98.900) | 0.890
(0.826–0.937) |
| CCAT1 + CEA |
| 80.500
(72.000–87.400) | 92.600
(75.700–98.900) | 0.910
(0.849–0.951) |
Stability of serum EV lncRNA CCAT1 in
harsh environments
To determine the stability of serum EV lncRNA CCAT1,
EVs from patient serum were divided into three groups. The results
revealed that there was no significant differences between the
RNase A treatment and control groups; however, when TritonX-100
penetrated the EVs, the expression levels of EV lncRNA CCAT1
decreased significantly (Fig. S2).
These results confirmed that lncRNA CCAT1 was present in serum EVs.
To verify the stability of lncRNA CCAT1 in serum EVs in harsh
environments, serum samples were stored at room temperature or 4°C
for 24 or 48 h (Fig. S3A). With
fresh serum as a control, serum samples were frozen and thawed
three times at −80°C (Fig. S3B).
The results demonstrated that the aforementioned treatments had no
significant effects on the expression of lncRNA CCAT1 in EVs, which
confirmed that the expression levels of serum EV lncRNA CCAT1 were
stable.
Expression of lncRNA CCAT1 in GC
tissues
A previous study has suggested that circulating EV
lncRNA may be secreted from GC tissues (44). Therefore, the current study assessed
the source of serum EV lncRNA CCAT1. The results demonstrated that
lncRNA CCAT1 levels in GC tissues were significantly higher
compared with those in the adjacent tissues (P<0.001; Fig. S4A). The correlation analysis between
lncRNA CCAT1 in GC tissues and serum EVs revealed a positive
correlation (r=0.685; P=0.003; Fig.
S4B). These results suggested that serum EV lncRNA CCAT1 may be
secreted from GC cells.
Prognostic value of lncRNA CCAT1
expression in GC
To evaluate the value of lncRNA CCAT1 in GC
prognosis, GEPIA (http://gepia.cancer-pku.cn/index.html) was used. As
presented in Fig. 4A, low expression
levels of lncRNA CCAT1 were significantly associated with a
favorable DFS outcome compared with high expression levels of
lncRNA CCAT1 in patients with GC [hazard ratio (HR)=1.7; log-rank
P=0.038]. However, it exhibited no significance in predicting OS
(HR=1.3; log-rank P=0.310; Fig. 4B).
These results suggested that lncRNA CCAT1 may be a useful biomarker
for predicting the DFS of patients with GC.
Discussion
Recent studies have demonstrated that EV lncRNAs are
reliable biomarkers for various types of cancer including breast
cancer, CRC and hepatocellular carcinoma (45–47).
Previous studies have reported that lncRNA LINC00152, HOTTIP and
lncUEGC1 in EVs may be suitable biomarkers for GC, and their AUC
values were 0.657, 0.827 and 0.876, respectively (23–25).
Furthermore, the sensitivity and specificity of the aforementioned
three lncRNAs were 48.1 and 85.2, 69.8 and 85.0, and 88.24 and
83.33%, respectively (23–25). Notably, the AUC, sensitivity and
specificity of lncRNA CCAT1 in the current study were 0.890, 79.6
and 92.6%, respectively, which were higher compared with those of
the aforementioned three lncRNAs, suggesting that it may be a
reliable potential biomarker. Furthermore, the levels of EV lncRNA
CCAT1 were associated with depth of invasion, distal metastasis and
TNM stage, but not associated with other clinicopathological
features, such as patient age and sex in the present study. Serum
EV lncRNA CCAT1 was also positively correlated with its expression
in GC tissues and associated with the prognosis of patients with
GC. These results suggested that EV lncRNA CCAT1 may be a reliable
tumor marker for GC.
EVs are involved in the key steps of cancer
progression and have numerous potential applications in diagnosis
and treatment. A previous study has demonstrated that tumor cells
secrete EVs into various body fluids, including the blood and urine
(48). In the current study, EVs
were successfully isolated from the serum, which was consistent
with previous studies (49,50). EVs contain a wide range of DNA, mRNA,
proteins, miRNA, lncRNA, circular RNA and metabolites (51). EVs are involved in the development of
GC through intercellular communication (16). Therefore, EVs are regarded as
suitable non-invasive biomarkers for GC. Multiple methods to obtain
EVs are available, including density-gradient centrifugation,
sucrose cushion centrifugation, gel-permeation chromatography,
affinity capture, microfluidic devices, synthetic polymer-based
precipitation and membrane filtration (52). The current study compared the
efficiency of EV extraction by ultracentrifugation and a commercial
kit. The results demonstrated that EVs were successfully obtained
by both methods, and that their characteristics were similar, as
determined by TEM, surface marker proteins, size distribution and
zeta potential. Compared with the that obtained using the
commercial kit, the yield of EVs extracted by ultracentrifugation
was higher; however, the purity was lower. In addition,
ultracentrifugation is time-consuming, thus it is recommended that
commercial kits are used to obtain EVs in future studies.
lncRNA CCAT1 silencing inhibits PANC-1 and Aspc-1 PC
cell proliferation and migration, and rescues cyclin D1 expression
(32). Another study has revealed
that lncRNA CCAT1 promotes the proliferation and migration of HCC
cells in vitro by depressing the expression levels of let-7,
targeting high mobility group AT-hook 2 and c-Myc (31). The development of GC is a complex
process, starting with chronic gastritis, which subsequently
progresses to atypical hyperplasia and finally GC. Alterations in
the resulting EV lncRNAs of these processes that are secreted into
the periphery may therefore serve as suitable biomarkers.
The present study assessed the potential clinical
value of EV lncRNA CCAT1. The results revealed that EV lncRNA CCAT1
levels in patients with GC were significantly higher compared with
those in healthy control subjects, as well as in patients with
chronic gastritis and atypical hyperplasia. These results suggested
that EV lncRNA CCAT1 may be involved in GC progression. It is
hypothesized that during GC progression, abnormal cells release EVs
containing lncRNA CCAT1, which enter the periphery; once EVs bind
to target cells, their contents can be transferred to the cytoplasm
through a variety of pathways, thus altering the physiological
state of the receptor cells (53).
Kalluri and LeBleu (54) have
demonstrated that EVs downregulate the levels of major
histocompatibility complex-II transcription factor regulatory
factor X associated protein in dendritic cells, potentially
promoting immune evasion by cancer cells. In addition, EVs activate
macrophages and increase the levels of proinflammatory cytokines,
which in turn promote the proliferation and migration of tumor
cells, leading to the reconstruction of the tumor microenvironment
(55). In addition, atypical
hyperplasia is a key step for the progression from a healthy state
to GC (56). The results of the
present study revealed that the expression levels of lncRNA CCAT1
in atypical hyperplasia were higher compared with those in healthy
control subjects, which further confirmed its role in GC
progression. A previous study has demonstrated that lncRNAs exist
stably in the blood, possibly to protect EVs from degradation
(44). The results of the current
study demonstrated that serum EV lncRNA CCAT1 was expressed at
stable levels, and that there were no significant changes in the
expression levels of lncRNA CCAT1 at different times, temperatures
and conditions of repeated freezing and thawing, suggesting that
serum EV lncRNA CCAT1 may be suitable as a biomarker of GC. The
results of the present study also demonstrated that lncRNA CCAT1
was associated with various clinical parameters that may be
involved in the invasion and metastasis of GC. The mechanism by
which lncRNA CCAT1 exerts its functions may be activated by c-Myc
or the upregulation of Bmi-1 to promotes the proliferation,
migration and invasion of GC cells (36,57,58).
In the present study, EV lncRNA CCAT1 levels were
markedly higher in patients with stage III+IV GC compared with
those with stage I+II GC. These results suggested that with GC
development, the expression levels of lncRNA CCAT1 in the serum
were increased; thus, lncRNA CCAT1 may be associated with GC
progression. ROC curve analysis revealed that EV lncRNA CCAT1 had a
markedly higher diagnostic value compared with that of CEA. An
increasing body of evidence has demonstrated that a combination of
multiple tumor markers may improve the accuracy of diagnosis. For
examples, Zhao et al (59)
have reported that the combination of lncRNA CCAT1 and lncRNA HOX
transcript antisense RNA provides more effective screening for CRC
compared with HOTAIR or CCAT1 alone. In addition, Li et al
(60) have demonstrated that the
diagnostic value of EV lnc-GNAQ-6:1 was higher compared with that
of traditional tumor markers CEA, CA 19–9 and CA72-4, and that the
combination of these markers may provide an effective screening
method for GC. The current study combined lncRNA CCAT1 and CEA to
evaluate the diagnostic value of this combination in GC, and
reached similar conclusions; the markers were more effective in
combination compared with the results obtained with each marker
alone.
Previous studies have suggested that serum/plasma EV
lncRNA is secreted from tumor tissues. Tong et al (61) have reported that the expression of
lncRNA POU class 3 homeobox 3 is consistent in the tissues and
serum of patients with esophageal squamous cell carcinoma. The
results of the present study demonstrated that the expression
levels of lncRNA CCAT1 in GC tissues were higher compared with
those in adjacent non-cancerous tissues and were positively
correlated with those in the serum. It was hypothesized that lncRNA
CCAT1 may be secreted by cancer cells during GC progression. The
online database exoRBase analysis revealed that EV lncRNA CCAT1
levels were upregulated in hepatocellular carcinoma and pancreatic
adenocarcinoma compared those in healthy subjects. However, there
was a lack of data from patients with GC. Therefore, the current
study may provide novel information for the GC diagnosis.
A previous study has demonstrated that lncRNAs are
associated with the poor prognosis of several types of cancer
including lung adenocarcinoma, hepatocellular carcinoma and
melanoma (62). In the present
study, patients with high expression levels of lncRNA CCAT1
presented with a poor prognosis. Similarly, a study by Ozawa et
al (63) has determined that
high lncRNA CCAT1 expression levels are significantly associated
with low remission-free survival and OS rates in patients with CRC.
Taken together, these results suggested lncRNA CCAT1 may be used as
a biomarker to diagnose and determine the prognosis of patients
with GC. However, there were limitations to the present study,
including its retrospective nature and a relatively small sample
size. Further studies with a larger sample size that aim to
determine the underlying mechanism of EV lncRNA CCAT1 in GC
progression are therefore required.
In conclusion, the results of the current study
demonstrated that the levels of serum EV lncRNA CCAT1 were
significantly upregulated in patients with GC compared with those
in healthy subjects and patients with other illnesses,
demonstrating the diagnostic value of this lncRNA. In addition, the
levels of EV lncRNA CCAT1 were associated with the depth of
invasion and metastasis. lncRNA CCAT1 existed stably in serum EVs
and may be derived from GC cells. These results provide a
foundation for further analysis of the clinical value of EV lncRNA
CCAT1 in the diagnosis and prognosis of patients with GC.
Supplementary Material
Supporting Data
Acknowledgements
The authors would like to thank Professor Dong Sun
(Department of General Surgery, Qilu Hospital of Shandong
University, Jinan, China) for their technical assistance.
Funding
This study was supported by The National Natural
Science Foundation of China (grant nos. 82072358, 81972005 and
81572070), The Natural Science Foundation of Shandong Province
(grant no. ZR2017MH044), the Key Research and Development Project
of Shandong Province (grant nos. 2016GSF201122 and 2016GSF201124),
the Science and Technology Development Project in Jinan (grant no.
201805084) and the Latitudinal Research Project of Shandong
University (grant no. 6010119015).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YZ conceived the study, analyzed the data and
reviewed the manuscript. KX designed the methodology, performed the
analysis, prepared the original draft and was responsible for the
project administration. DW was responsible for the bioinformatics
and part of the statistical analysis. KX, ZD and DW extracted and
identified EVs. WC, ZS and CY performed validation experiments,
revised the manuscript and were involved in all the stages of the
study. ZD and ML provided the information of patients and collected
tissue samples of patients. JD, ZS collected blood samples of
patients. KX prepared the graphs and figures. YZ supervised the
study. ML and JD interpreted the data and participated in the
writing of the manuscript. KX, ZD and DW confirm the authenticity
of all the raw data. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
This study was approved by Medical Ethics Committee
of Qilu Hospital of Shandong University (approval no.
KYLL-2015-097). All samples were anonymized during the analysis.
All participants provided signed informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
lncRNA
|
long non-coding RNA
|
|
EVs
|
extracellular vesicles
|
|
GC
|
gastric cancer
|
|
CCAT1
|
colon cancer-associated transcript
1
|
|
OS
|
overall survival
|
|
DFS
|
disease-free survival
|
|
CEA
|
carcinoembryonic antigen
|
|
CA19-9
|
carbohydrate antigen 19-9
|
|
CA72-4
|
carbohydrate antigen 72-4
|
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Smyth EC, Nilsson M, Grabsch HI, van
Grieken NC and Lordick F: Gastric cancer. Lancet. 396:635–648.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fu M, Gu J, Jiang P, Qian H, Xu W and
Zhang X: Exosomes in gastric cancer: Roles, mechanisms, and
applications. Mol Cancer. 18:412019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dong Z, Sun X, Xu J, Han X, Xing Z, Wang
D, Ge J, Meng L and Xu X: Serum membrane type 1-matrix
metalloproteinase (MT1-MMP) mRNA protected by exosomes as a
potential biomarker for gastric cancer. Med Sci Monit.
25:7770–7783. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang J, Liu Y, Sun W, Zhang Q, Gu T and Li
G: Plasma exosomes as novel biomarker for the early diagnosis of
gastric cancer. Cancer Biomark. 21:805–812. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hernández A, Arab JP, Reyes D, Lapitz A,
Moshage H, Bañales JM and Arrese M: Extracellular vesicles in
NAFLD/ALD: From pathobiology to therapy. Cells. 9:8172020.
View Article : Google Scholar
|
|
8
|
Martinez RM, Hauser R, Liang L, Mansur A,
Adir M, Dioni L, Racowsky C, Bollati V, Baccarelli AA and
Machtinger R: Urinary concentrations of phenols and phthalate
metabolites reflect extracellular vesicle microRNA expression in
follicular fluid. Environ Int. 123:20–28. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jun JH, Kim JY, Choi JH, Lim JY, Kim K and
Kim GJ: Exosomes from placenta-derived mesenchymal stem cells are
involved in liver regeneration in hepatic failure induced by bile
duct ligation. Stem Cells Int. 2020:54857382020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gholami L, Nooshabadi VT, Shahabi S,
Jazayeri M, Tarzemany R, Afsartala Z and Khorsandi K: Extracellular
vesicles in bone and periodontal regeneration: Current and
potential therapeutic applications. Cell Biosci. 11:162021.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Samanta S, Rajasingh S, Drosos N, Zhou Z,
Dawn B and Rajasingh J: Exosomes: new molecular targets of
diseases. Acta Pharmacol Sin. 39:501–513. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Maacha S, Bhat AA, Jimenez L, Raza A,
Haris M, Uddin S and Grivel JC: Extracellular vesicles-mediated
intercellular communication: Roles in the tumor microenvironment
and anti-cancer drug resistance. Mol Cancer. 18:552019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Abd Elmageed ZY, Yang Y, Thomas R, Ranjan
M, Mondal D, Moroz K, Fang Z, Rezk BM, Moparty K, Sikka SC, et al:
Neoplastic Reprogramming of Patient-Derived Adipose Stem Cells by
Prostate Cancer Cell-Associated Exosomes. Stem Cells. 32:983–997.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang X, Shi H, Yuan X, Jiang P, Qian H
and Xu W: Tumor-derived exosomes induce N2 polarization of
neutrophils to promote gastric cancer cell migration. Mol Cancer.
17:1462018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mulcahy LA, Pink RC and Carter DR: Routes
and mechanisms of extracellular vesicle uptake. J Extracell
Vesicles. 3:246412014. View Article : Google Scholar
|
|
16
|
Huang T, Song C, Zheng L, Xia L, Li Y and
Zhou Y: The roles of extracellular vesicles in gastric cancer
development, microenvironment, anti-cancer drug resistance, and
therapy. Mol Cancer. 18:622019. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu R, Rai A, Chen M, Suwakulsiri W,
Greening DW and Simpson RJ: Extracellular vesicles in
cancer-implications for future improvements in cancer care. Nat Rev
Clin Oncol. 15:617–638. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lin MT, Song HJ and Ding XY: Long
non-coding RNAs involved in metastasis of gastric cancer. World J
Gastroenterol. 24:3724–3737. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jiang S, Cheng SJ, Ren LC, Wang Q, Kang
YJ, Ding Y, Hou M, Yang XX, Lin Y, Liang N and Gao G: An expanded
landscape of human long noncoding RNA. Nucleic Acids Res.
47:7842–7856. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhou X, Chen H, Zhu L, Hao B, Zhang W, Hua
J, Gu H, Jin W and Zhang G: Helicobacter pylori infection related
long noncoding RNA (lncRNA) AF147447 inhibits gastric cancer
proliferation and invasion by targeting MUC2 and up-regulating
miR-34c. Oncotarget. 7:82770–82782. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhuo W, Liu Y, Li S, Guo D, Sun Q, Jin J,
Rao X, Li M, Sun M, Jiang M, et al: Long noncoding RNA GMAN,
up-regulated in gastric cancer tissues, is associated with
metastasis in patients and promotes translation of ephrin A1 by
competitively binding GMAN-AS. Gastroenterology. 156:676–691.e11.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yang L, Peng X, Li Y, Zhang X, Ma Y, Wu C,
Fan Q, Wei S, Li H and Liu J: Long non-coding RNA HOTAIR promotes
exosome secretion by regulating RAB35 and SNAP23 in hepatocellular
carcinoma. Mol Cancer. 18:782019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li Q, Shao Y, Zhang X, Zheng T, Miao M,
Qin L, Wang B, Ye G, Xiao B and Guo J: Plasma long noncoding RNA
protected by exosomes as a potential stable biomarker for gastric
cancer. Tumour Biol. 36:2007–2012. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lin LY, Yang L, Zeng Q, Wang L, Chen ML,
Zhao ZH, Ye GD, Luo QC, Lv PY, Guo QW, et al: Tumor-originated
exosomal lncUEGC1 as a circulating biomarker for early-stage
gastric cancer. Mol Cancer. 17:842018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhao R and Zhang Y, Zhang X, Yang Y, Zheng
X, Li X, Liu Y and Zhang Y: Exosomal long noncoding RNA HOTTIP as
potential novel diagnostic and prognostic biomarker test for
gastric cancer. Mol Cancer. 17:682018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Arunkumar G, Murugan AK, Prasanna
Srinivasa Rao H, Subbiah S, Rajaraman R and Munirajan AK: Long
non-coding RNA CCAT1 is overexpressed in oral squamous cell
carcinomas and predicts poor prognosis. Biomed Rep. 6:455–462.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mizrahi I, Mazeh H, Grinbaum R, Beglaibter
N, Wilschanski M, Pavlov V, Adileh M, Stojadinovic A, Avital I,
Gure AO, et al: Colon cancer associated transcript-1 (CCAT1)
expression in adenocarcinoma of the stomach. J Cancer. 6:105–110.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chen S, Liu Y, Wang Y and Xue Z: LncRNA
CCAT1 promotes colorectal cancer tumorigenesis via a
miR-181b-5p/TUSC3 axis. Onco Targets Ther. 12:9215–9225. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Deng L, Yang SB, Xu FF and Zhang JH: Long
noncoding RNA CCAT1 promotes hepatocellular carcinoma progression
by functioning as let-7 sponge. J Exp Clin Cancer Res. 34:182015.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhang C, Wang W, Lin J, Xiao J and Tian Y:
lncRNA CCAT1 promotes bladder cancer cell proliferation, migration
and invasion. Int Braz J Urol. 45:549–559. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Xin Y, Li Z, Shen J, Chan MT and Wu WK:
CCAT1: A pivotal oncogenic long non-coding RNA in human cancers.
Cell Prolif. 49:255–260. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Liu Z, Chen Q and Hann SS: The functions
and oncogenic roles of CCAT1 in human cancer. Biomed Pharmacother.
115:1089432019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Shen H, Wang L, Xiong J, Ren C, Gao C,
Ding W, Zhu D, Ma D and Wang H: Long non-coding RNA CCAT1 promotes
cervical cancer cell proliferation and invasion by regulating the
miR-181a-5p/MMP14 axis. Cell Cycle. 18:1110–1121. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
You Z, Liu C, Wang C, Ling Z, Wang Y, Wang
Y, Zhang M, Chen S, Xu B, Guan H and Chen M: LncRNA CCAT1 promotes
prostate cancer cell proliferation by interacting with DDX5 and
MIR-28-5P. Mol Cancer Ther. 18:2469–2479. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Abedini P, Fattahi A, Agah S, Talebi A,
Beygi AH, Amini SM, Mirzaei A and Akbari A: Expression analysis of
circulating plasma long noncoding RNAs in colorectal cancer: The
relevance of lncRNAs ATB and CCAT1 as potential clinical hallmarks.
J Cell Physiol. 234:22028–22033. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Li Y, Zhu G, Ma Y and Qu H: lncRNA CCAT1
contributes to the growth and invasion of gastric cancer via
targeting miR-219-1. J Cell Biochem. 120:19457–19468. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Xie Y, Dang W, Zhang S, Yue W, Yang L,
Zhai X, Yan Q and Lu J: The role of exosomal noncoding RNAs in
cancer. Mol Cancer. 18:372019. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Barbagallo C, Brex D, Caponnetto A,
Cirnigliaro M, Scalia M, Magnano A, Caltabiano R, Barbagallo D,
Biondi A, Cappellani A, et al: LncRNA UCA1, upregulated in CRC
biopsies and downregulated in serum exosomes, controls mRNA
expression by RNA-RNA interactions. Mol Ther Nucleic Acids.
12:229–241. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Galamb O, Barták BK, Kalmár A, Nagy ZB,
Szigeti KA, Tulassay Z, Igaz P and Molnár B: Diagnostic and
prognostic potential of tissue and circulating long non-coding RNAs
in colorectal tumors. World J Gastroenterol. 25:5026–5048. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The eighth edition AJCC cancer staging manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhang J, Arends RH, Kubiak RJ, Roskos LK,
Liang M, Lee N, Chen CC and Yang H: A new method for identification
of outliers in immunogenicity assay cut point data. J Immunol
Methods. 484-485:1128172020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Li S, Li Y, Chen B, Zhao J, Yu S, Tang Y,
Zheng Q, Li Y, Wang P, He X and Huang S: ExoRBase: A database of
circRNA, lncRNA and mRNA in human blood exosomes. Nucleic Acids
Res. 46(D1): D106–D112. 2018. View Article : Google Scholar
|
|
44
|
Arita T, Ichikawa D, Konishi H, Komatsu S,
Shiozaki A, Shoda K, Kawaguchi T, Hirajima S, Nagata H, Kubota T,
et al: Circulating long non-coding RNAs in plasma of patients with
gastric cancer. Anticancer Res. 33:3185–3193. 2013.PubMed/NCBI
|
|
45
|
Zhong G, Wang K, Li J, Xiao S, Wei W and
Liu J: Determination of serum exosomal H19 as a noninvasive
biomarker for breast cancer diagnosis. Onco Targets Ther.
13:2563–2571. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Li N, Li J, Mi Q, Xie Y, Li P, Wang L,
Binang H, Wang Q, Wang Y, Chen Y, et al: Long non-coding RNA
ADAMTS9-AS1 suppresses colorectal cancer by inhibiting the
Wnt/β-catenin signalling pathway and is a potential diagnostic
biomarker. J Cell Mol Med. 24:11318–11329. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Wang J, Pu J, Zhang Y, Yao T, Luo Z, Li W,
Xu G, Liu J, Wei W and Deng Y: Exosome-transmitted long non-coding
RNA SENP3-EIF4A1 suppresses the progression of hepatocellular
carcinoma. Aging (Albany NY). 12:11550–11567. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Taylor DD and Gercel-Taylor C: MicroRNA
signatures of tumor-derived exosomes as diagnostic biomarkers of
ovarian cancer. Gynecol Oncol. 110:13–21. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Scavo MP, Cigliano A, Depalo N, Fanizza E,
Bianco MG, Denora N, Laquintana V, Curri ML, Lorusso D, Lotesoriere
C, et al: Frizzled-10 extracellular vesicles plasma concentration
is associated with tumoral progression in patients with colorectal
and gastric cancer. J Oncol. 2019:27159682019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Chung KY, Quek JM, Neo SH and Too HP:
Polymer-based precipitation of extracellular vesicular miRNAs from
serum improve gastric cancer miRNA biomarker performance. J Mol
Diagn. 22:610–618. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Pegtel DM and Gould SJ: Exosomes. Annu Rev
Biochem. 88:487–514. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Xu R, Greening DW, Zhu HJ, Takahashi N and
Simpson RJ: Extracellular vesicle isolation and characterization:
Toward clinical application. J Clin Invest. 126:1152–1162. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Tkach M and Théry C: Communication by
extracellular vesicles: Where we are and where we need to go? Cell.
164:1226–1232. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Kalluri R and LeBleu VS: The biology,
function, and biomedical applications of exosomes. Science.
367:eaau69772020. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Wu L, Zhang X, Zhang B, Shi H, Yuan X, Sun
Y, Pan Z, Qian H and Xu W: Exosomes derived from gastric cancer
cells activate NF-κB pathway in macrophages to promote cancer
progression. Tumour Biol. 37:12169–12180. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Kinoshita H, Hayakawa Y and Koike K:
Metaplasia in the stomach-precursor of gastric cancer? Int J Mol
Sci. 18:20632017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Yang F, Xue X, Bi J, Zheng L, Zhi K, Gu Y
and Fang G: Long noncoding RNA CCAT1, which could be activated by
c-Myc, promotes the progression of gastric carcinoma. J Cancer Res
Clin Oncol. 139:437–445. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Li N, Jiang K, Fang LP, Yao LL and Yu Z:
Knockdown of long noncoding RNA CCAT1 inhibits cell growth,
invasion and peritoneal metastasis via downregulation of Bmi-1 in
gastric cancer. Neoplasma. 65:736–744. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Zhao W, Song M, Zhang J, Kuerban M and
Wang H: Combined identification of long non-coding RNA CCAT1 and
HOTAIR in serum as an effective screening for colorectal carcinoma.
Int J Clin Exp Pathol. 8:14131–14140. 2015.PubMed/NCBI
|
|
60
|
Li S, Zhang M, Zhang H, Hu K, Cai C, Wang
J, Shi L, Ma P, Xu Y and Zheng P: Exosomal long noncoding RNA
lnc-GNAQ-6:1 may serve as a diagnostic marker for gastric cancer.
Clin Chim Acta. 501:252–257. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Tong YS, Wang XW, Zhou XL, Liu ZH, Yang
TX, Shi WH, Xie HW, Lv J, Wu QQ and Cao XF: Identification of the
long non-coding RNA POU3F3 in plasma as a novel biomarker for
diagnosis of esophageal squamous cell carcinoma. Mol Cancer.
14:32015. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Zhang Z, Xie H, Liang D, Huang L, Liang F,
Qi Q and Yang X: Long non-coding RNA CCAT1 as a diagnostic and
prognostic molecular marker in various cancers: A meta-analysis.
Oncotarget. 9:23695–23703. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Ozawa T, Matsuyama T, Toiyama Y, Takahashi
N, Ishikawa T, Uetake H, Yamada Y, Kusunoki M, Calin G and Goel A:
CCAT1 and CCAT2 long noncoding RNAs, located within the 8q.24.21
‘gene desert’, serve as important prognostic biomarkers in
colorectal cancer. Ann Oncol. 28:1882–1888. 2017. View Article : Google Scholar : PubMed/NCBI
|