Introduction
Non-small cell lung cancer (NSCLC) accounts for
80–90% of lung cancer which is the leading cause of cancer-related
deaths worldwide (1).
Platinum-based chemotherapy had only provided a modest survival
benefit, but recent advances in systemic treatment have improved
the prognosis of patients with advanced NSCLC. Immunotherapy with
or without platinum-based chemotherapy is recommended for patients
with NSCLC harboring no oncogenic gene alteration (2).
Cancer immunity is co-regulated through a balance in
stimulatory and inhibitory signals (‘immune checkpoints’).
Programmed cell death 1 (PD-1) is the most important
immune-inhibitory molecule expressed on activated cytotoxic
T-lymphocytes (CTLs). When PD-1 binds to its ligand such as
programmed death-ligand 1 (PD-L1), the ability of CTLs to kill
cancer cells is inhibited. Cancer cells expressing PD-L1 may evade
immune attack by CTLs, which leads to tumor progression. Blockade
of the PD-1/PD-L1 axis may restore cancer immunity to kill cancer
cells, and plays a pivotal role in modern systemic treatment for a
variety of malignant tumors including NSCLC (3,4).
However, only ~30% of all NSCLC patients may respond to
immunotherapy using an anti-PD-1/PD-L1 antibody (2,5).
The T-cell immunoglobulin and immunoreceptor
tyrosine-based inhibitory domain (TIGIT) is also an
immune-inhibitory molecule on CTLs. Cancer cells may evade cancer
immunity by expressing their ligands, such as CD155 [also known as
poliovirus receptor (PVR)] (6–8).
Accordingly, blockade of the TIGIT/CD155 axis has emerged as a
novel therapeutic strategy for a variety of malignant tumors
(6,7,9). A
recent randomized phase 2 study (CITYSCAPE trial) assessing the
efficacy of an anti-TIGIT antibody (tiragolumab) in addition to an
anti-PD-L1 antibody (atezolizumab) for advanced NSCLC showed
promising results. The study revealed a higher overall response
rate (ORR, 37 vs. 20%) and longer progression-free survival (PFS,
5.6 vs. 3.9 months) in the group receiving combination therapy
compared to the control group receiving placebo, respectively
(9). Despite the potential
clinical significance of CD155 expression on cancer cells as a
biomarker for the prediction of prognosis and response to
anti-TIGIT/CD155 antibody, the clinical significance of CD155
expression in NSCLC remains unclear. We previously reported the
prognostic significance of PD-L1 expression in completely resected
pathologic (p-) stage I lung adenocarcinoma that was the most
common histological subtype of NSCLC (10). Here, we examined CD155 expression
in the same patient population, and assessed its clinical
significance in correlation with PD-L1 expression.
Patients and methods
Patients
We retrospectively evaluated consecutive patients
with p-stage I lung adenocarcinoma who underwent complete resection
without preoperative treatment at our hospital [Second Department
of Surgery (Chest Surgery), University of Occupational and
Environmental Health, Japan] from January 2003 through December
2006. All patients underwent lung resection through minimal
thoracotomy. Lobectomy was performed in the 89 (92.7%) patients who
were fit for lobectomy. Sub-lobar resection was performed in the
remaining 7 patients who did not tolerate lobectomy (segmentectomy
in 5 patients and wedge resection in 2 patients).
Patients who did not agree to give informed consent
for participating in the study were excluded. In addition, patients
who did not provide sufficient tumor samples for
immunohistochemistry (IHC) were deemed ineligible. A total of 96
patients were finally included in this study. P-stage was
determined according to the TNM classification (Union for
International Cancer Control TNM staging system, 7th edition).
Patients with p-stage IB disease who were eligible for adjuvant
chemotherapy were encouraged to participate in clinical trials
(11,12), and 10 patients received adjuvant
chemotherapy (carboplatin-based chemotherapy in 8 patients and
tegafur plus uracil in 2 patients). Other patient characteristics
are shown in Table I.
 | Table I.Patient characteristics according to
tumoral CD155 status. |
Table I.
Patient characteristics according to
tumoral CD155 status.
|
|
| Tumoral CD155
expression |
|
|---|
|
|
|
|
|
|---|
| Variables | Total | Positive | Negative | P-value |
|---|
| All patients, n
(%) | 96 | 37 (38.5) | 59 (61.5) |
|
| Age, years |
|
|
|
|
|
Median | 72 | 73 | 70 | 0.232 |
|
Range | 40-88 | 45-86 | 40-88 |
|
| Sex, n (%) |
|
|
|
|
|
Male | 54 | 25 (46.3) | 29 (53.7) | 0.093 |
|
Female | 42 | 12 (28.6) | 30 (71.4) |
|
| Smoking, n (%) |
|
|
|
|
| Former
or current | 55 | 27 (49.1) | 28 (50.9) | 0.019 |
|
Never | 41 | 10 (24.4) | 31 (75.6) |
|
| Cell
differentiation, n (%) |
|
|
|
|
|
Well | 51 | 13 (25.5) | 38 (74.5) | 0.005 |
|
Moderately or poorly | 33 | 19 (57.6) | 14 (42.4) |
|
| Tumor size, n
(%) |
|
|
|
|
| >2
cm | 54 | 29 (53.7) | 25 (46.3) | <0.001 |
| ≤2
cm | 42 | 8 (19.0) | 34 (81.0) |
|
| Lympho-vascular
invasion, n (%) |
|
|
|
|
|
Yes | 23 | 12 (52.2) | 11 (47.8) | 0.302 |
| No | 47 | 17 (36.2) | 30 (63.8) |
|
| Vascular invasion,
n (%) |
|
|
|
|
|
Yes | 15 | 11 (73.3) | 4 (26.7) | 0.007 |
|
None | 58 | 19 (32.8) | 39 (67.2) |
|
| Pleural invasion, n
(%) |
|
|
|
|
|
Yes | 14 | 9 (64.3) | 5 (35.7) | 0.040 |
|
None | 82 | 28 (34.1) | 54 (65.9) |
|
| Pathologic stage, n
(%) |
|
|
|
|
| IA | 69 | 16 (23.2) | 53 (76.8) | <0.001 |
| IB | 27 | 21 (77.8) | 6 (22.2) |
|
| Tumoral PD-L1
expression, n (%) |
|
|
|
|
|
Positive | 14 | 9 (64.2) | 5 (35.7) | 0.041 |
|
Negative | 82 | 28 (34.1) | 54 (65.9) |
|
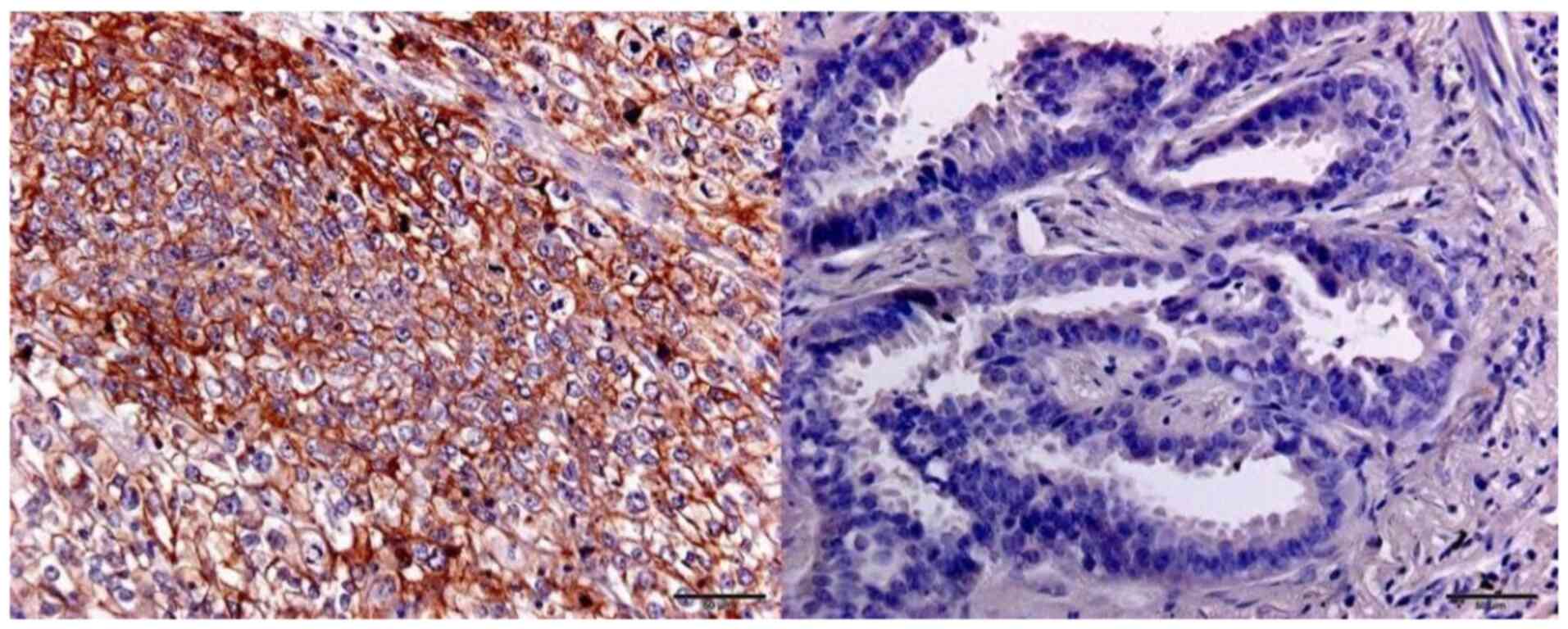
Immunohistochemistry (IHC)
For evaluation of CD155 expression, serial sections
were cut from each formalin-fixed and paraffin-embedded primary
tumor specimen and served for IHC using the Histofine Simple Stain,
MAX-PO (Nichirei Biosciences, Inc.) according to the manufacturer's
protocol. Sections were incubated with an anti-CD155 antibody
(clone B6; Santa Cruz Biotechnology, Inc.) diluted at 1:100 for 1 h
at room temperature.
Each slide was examined independently by two
investigators (R.O. and M.M.) who were blinded for any clinical
data. In case of disagreement between the two investigators, a
consensus was reached through the simultaneous examination by both
investigators using a double-headed microscope. Each cancer cell
was judged as positively stained for CD155 if the membrane or
cytoplasm was stained at any intensity. Each patient was classified
into ‘CD155-negative (CD155−)’ group or ‘CD155-positive
(CD155+)’ group according to the percentage of
CD155-positive cancer cells [tumor proportion score (TPS) for
CD155], and the optimal cut-off value was determined using a
receiver operating characteristic (ROC) curve analysis.
PD-L1 expression was also evaluated with IHC as
described in a previous study (10). Briefly, an anti-PD-L1 antibody
(clone E1L3N; Cell Signaling Technology, Inc.) was used as a
primary antibody, and each patient was also classified into
‘PD-L1-positive (PD-L1+)’ group or ‘PD-L1-negative
(PD-L1−)’ group with the cut-off value of 5% as the
percentage of cancer cells with membrane-staining for PD-L1 (TPS
for PD-L1).
Statistical analysis
The proportions of the categorical data were
compared using the chi-square test. Continuous data were compared
using a non-parametric test (Mann-Whitney U test). To determine an
optimal cut-off value of TPS for CD155, an ROC curve was generated
by plotting the false-positive rate of a model against its true
positive rate for prediction of tumor recurrence and the area under
the curve (AUC) was calculated.
The Kaplan-Meier method was used to estimate the
probability of OS and recurrence-free survival (RFS), and survival
differences were analyzed using the log-rank test.
To identify independent prognostic factors,
univariate and multivariate analyses were performed using a Cox
proportional hazards regression model. Sex, smoking status and
pathologic stage (IA or IB), which have been already founded to be
a significant prognostic factors, were included in the multivariate
analyses (13).
All statistical analyses were performed using EZR
software (Saitama Medical Center, Jichi Medical University,
Saitama, Japan), a modified version of R (The R Foundation for
Statistical Computing).
For each patient, a routine follow-up was performed
at the outpatient clinic as follows: chest roentgenography every 3
months, as well as chest computed tomography, brain magnetic
resonance imaging, and bone scan every 6 months for the first 3
years after surgery; all examinations were performed annually
thereafter. Additional examinations were performed when any
symptoms or signs of recurrence were detected. A telephone
follow-up would be made if the patient did not come to our clinic
for a routine follow-up.
Results
CD155 expression in lung
adenocarcinoma
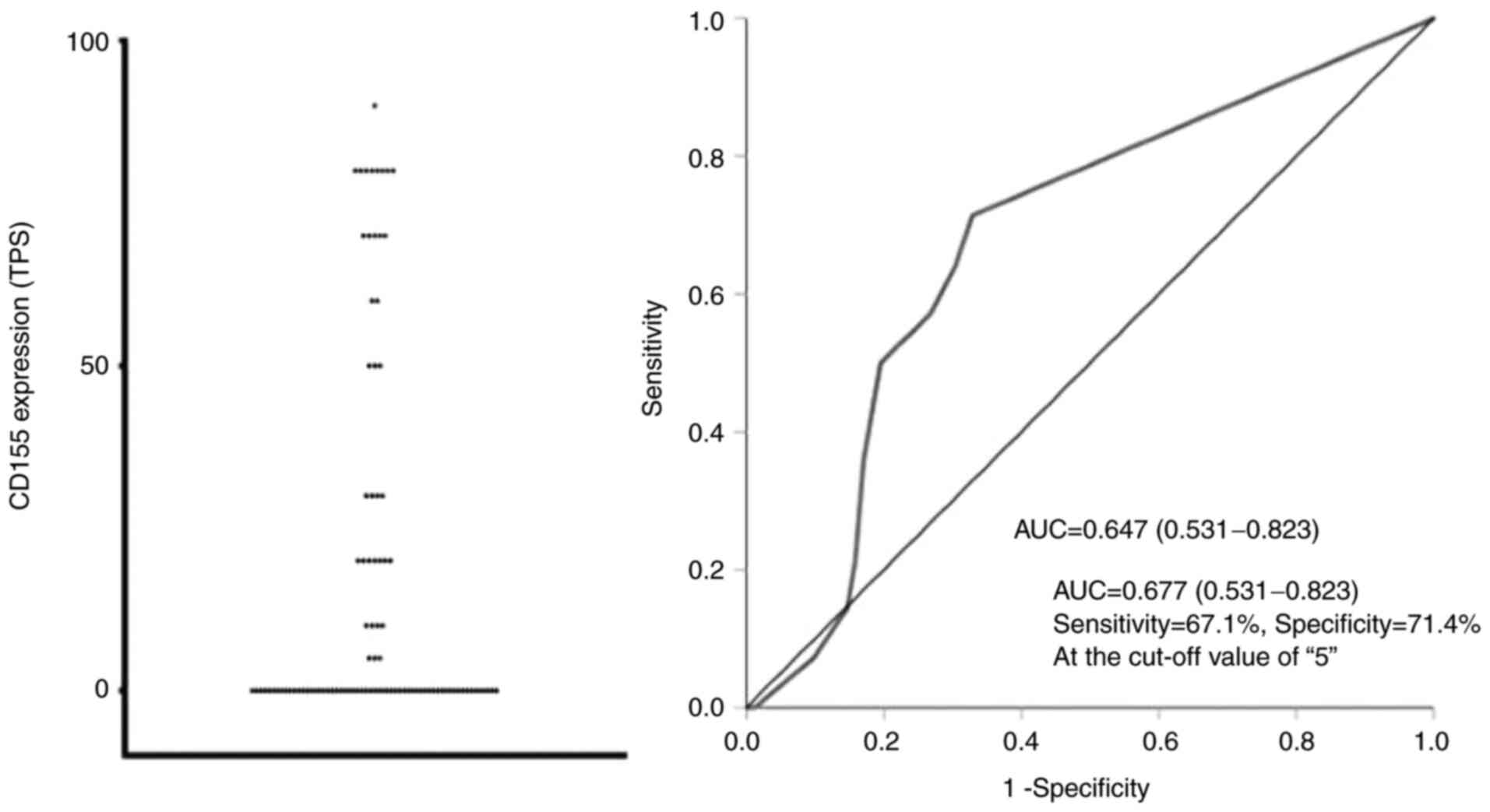
The distribution of TPS for CD155 is indicated in
Figs. 1 and 2. The area under the ROC curve (AUC-ROC)
for prediction of recurrence was 0.677 with a 95% confidence
interval (CI) of 0.531-0.823, suggesting that CD155 was a
significant prognostic marker. The ROC curve also indicated that
the TPS value of 5% was the optimal cut-off value with sensitivity
of 71.4% and specificity of 67.1% (Fig. 2). Based on these results, each
patient was classified according to the TPS value into the
CD155+ group (TPS, ≥5%) or the CD155− group
(TPS, <5%). Thirty-seven patients (38.5%) were classified into
the CD155+ group. When CD155+ patients were
further classified by using the cut-off TPS value of 50%, the
number of CD155-low (TPS, 5–49%) patients and CD155-high (TPS,
≥50%) patients were 18 and 19, respectively.
CD155-positivity was significantly associated with
advanced stage (p-stage IB) and pleural/vascular invasion.
CD155+ patients were less frequent in never smoker and
in patients with well-differentiated tumor. CD155-positivity was
significantly correlated with PD-L1 positivity (Table I).
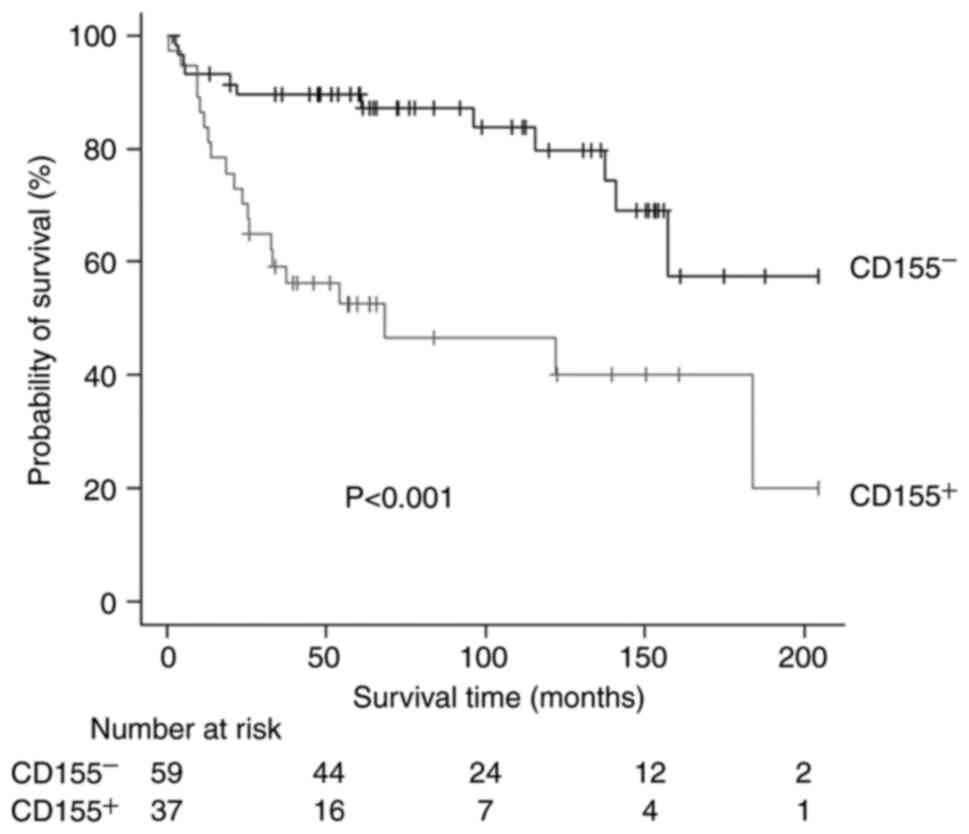
CD155-status and prognosis
The median follow-up time after surgery was 1,835
days. Twenty patients (9 patients in the CD155+ group
and 11 patients in the CD155− group) were lost to
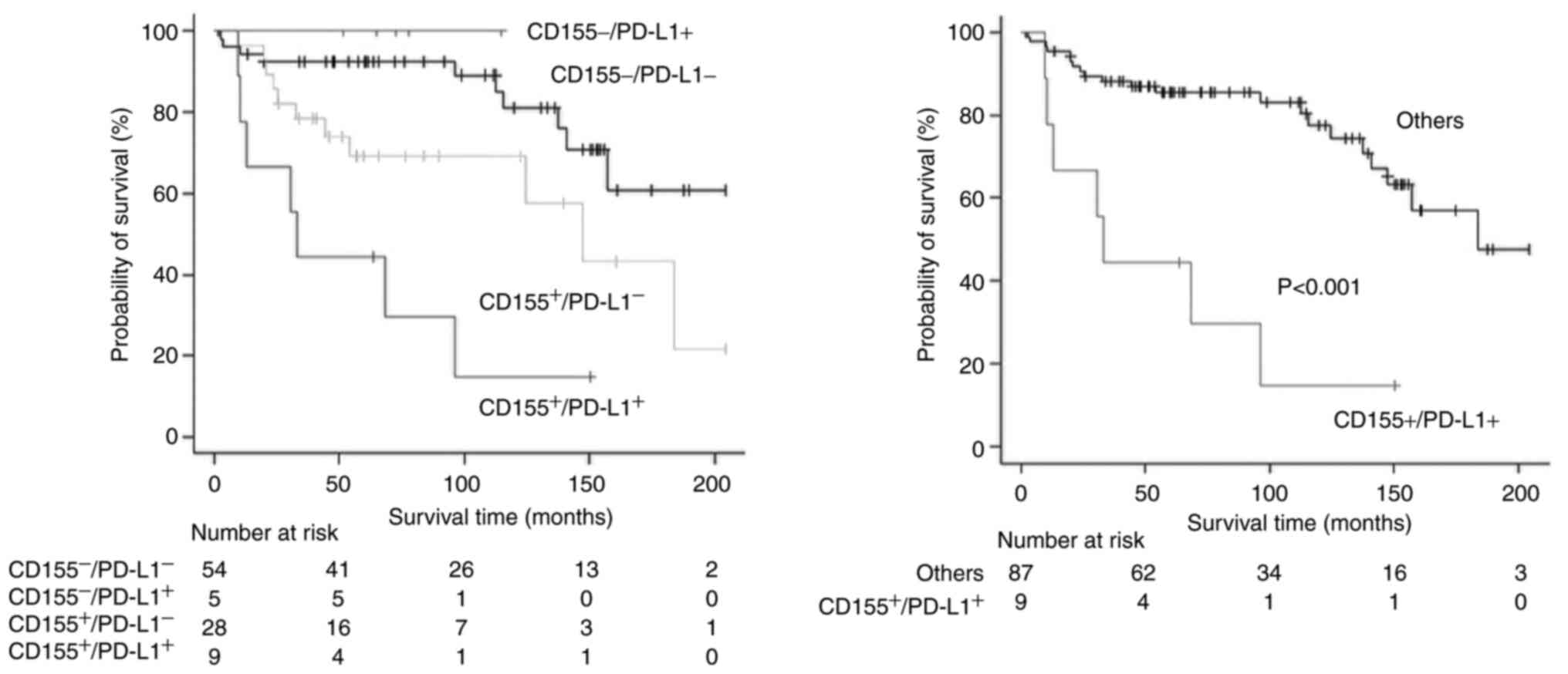
follow-up within 5 years after surgery. The 5-year RFS rates of
CD155+ patients and CD155− patients were 52.5
and 89.6%, respectively. There was a significant difference in the
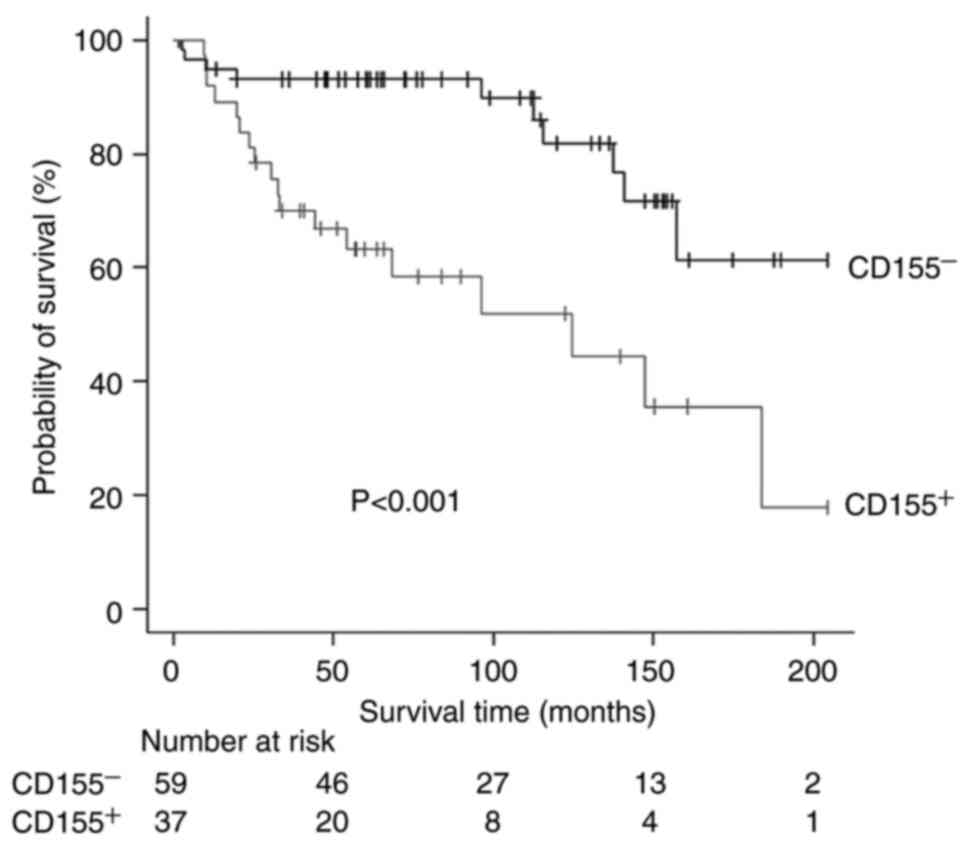
RFS according to the CD155-status (P<0.001, Fig. 3). Similarly, the 5-year OS rates
were 63.3 and 93.1%, respectively, with a significant difference in
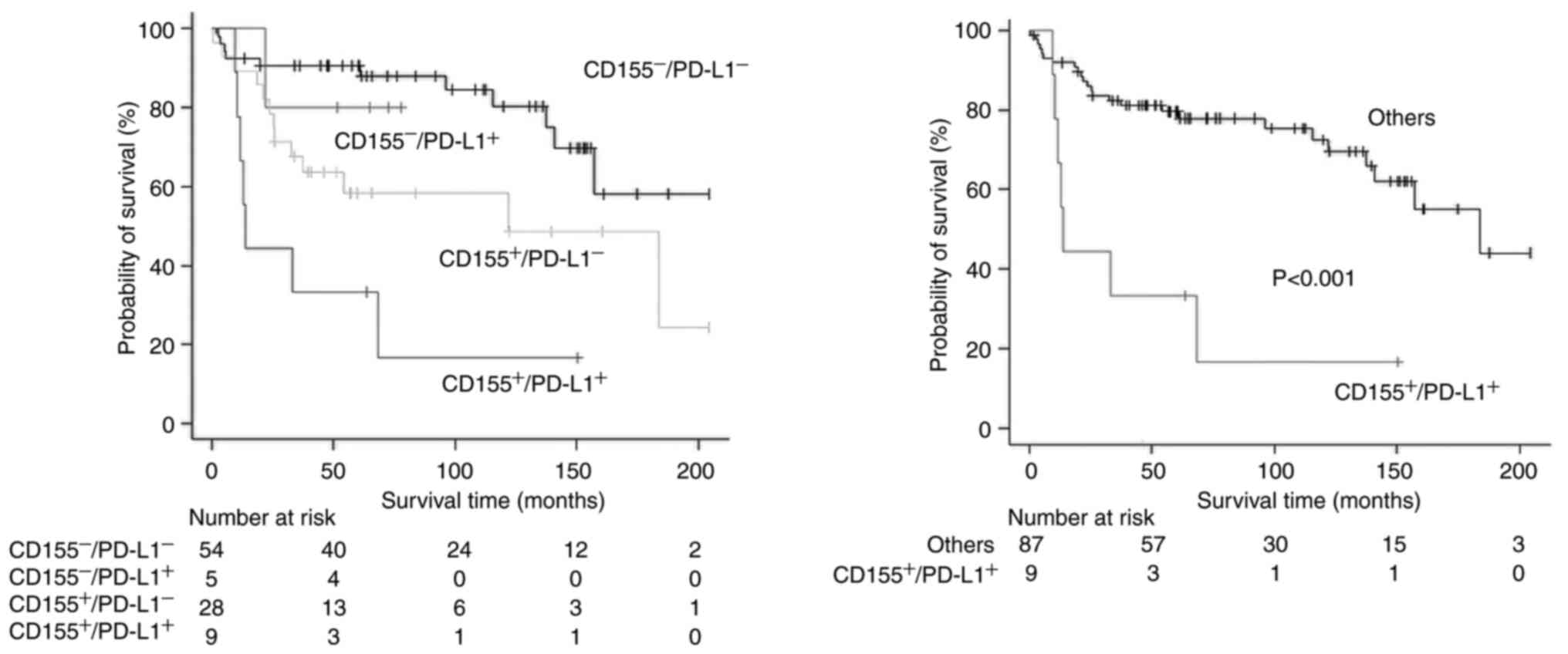
the OS according to the CD155-status (P<0.001, Fig. 4). In multivariate analyses, the
prognostic impact of the CD155 status was not significant with the
hazard ratio (HR) of 2.33 (95% CI, 0.97-5.57; P=0.056) for
RFS and with the HR of 2.18 (95% CI, 0.84-5.67; P=0.107) for
OS. Exploratory analyses showed no significant difference in the
prognosis between CD155-low patients and CD155-high patients
(5-year RFS rate, 42.9% vs. 62.2%; P=0.096; 5-year OS rate,
48.6 vs. 77.7%; P=0.083).
PD-L1-expression status was also significantly
associated with a poor prognosis in univariate analyses (Tables II and III), but the prognostic impact failed
to be significant in multivariate analyses (HR=2.12 [95% CI,
0.89-5.01] and P=0.087 for RFS; HR=2.24 [95% CI, 0.90-5.57]
and P=0.080 for OS). As PD-L1-positivity was a potential
prognostic factor (10), survival
analyses according to a combination of CD155 status and PD-L1
status were conducted. Patients with both-positive
(CD155+/PD-L1+) tumor showed a significantly
poor prognosis (Figs. 5 and
6). The status of
CD155+/PD-L1+ was a significant factor to
predict poor prognosis in both univariate and multivariate analyses
(Tables II and III).
| Table II.Univariate and multivariate Cox model
of prognostic factors for overall survival (OS). |
Table II.
Univariate and multivariate Cox model
of prognostic factors for overall survival (OS).
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age
(continuous) | 1.02
(0.98-1.06) | 0.291 |
|
|
| Sex (male vs.
female) | 3.14
(1.27-7.76) | 0.013 | 3.12
(1.24-7.81) | 0.014 |
| Smoking
(former/current vs. never) | 2.04
(0.89-4.64) | 0.089 |
|
|
| Cell
differentiation (well vs. others) | 1.56
(0.69-3.49) | 0.279 |
|
|
| Tumor size (>2
cm vs. ≤2 cm) | 3.70
(1.49-9.16) | 0.005 |
|
|
| Lympho-vascular
invasion (no vs. yes) | 0.44
(0.26-1.79) | 0.449 |
|
|
| Vascular invasion
(no vs. yes) | 0.85
(0.28-2.54) | 0.782 |
|
|
| Pleural invasion
(no vs. yes) | 0.88
(0.26-2.95) | 0.845 |
|
|
| Pathologic stage
(IB vs. IA) | 3.09
(1.46-6.51) | 0.003 | 2.28
(1.03-5.03) | 0.041 |
| CD155 expression
(positive vs. negative) | 3.74
(1.71-8.15) | <0.001 |
|
|
| PD-L1 (positive vs.
negative) | 3.04
(1.25-7.34) | 0.014 |
|
|
| CD155 expression
and PD-L1 expression (CD155+/PD-L1+ vs.
others) | 5.26
(2.19-12.61) | <0.001 | 3.86
(1.51-9.89) | 0.004 |
| Mode of lung
resection (sub-lobar resection vs. lobectomy) | 0.58
(0.13-2.54) | 0.477 |
|
|
| Adjuvant
chemotherapy (not performed vs. performed) | 1.28
(0.38-4.27) | 0.682 |
|
|
| Table III.Univariate and multivariate Cox model
of prognostic factors for recurrence-free survival (RFS). |
Table III.
Univariate and multivariate Cox model
of prognostic factors for recurrence-free survival (RFS).
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age
(continuous) | 1.01
(0.97-1.04) | 0.651 |
|
|
| Sex (male vs.
female) | 2.76
(1.23-6.16) | 0.013 | 2.46
(1.00-6.05) | 0.048 |
| Smoking
(former/current vs. never) | 2.26
(1.04-4.89) | 0.038 | 1.14
(0.47-2.78) | 0.758 |
| Cell
differentiation (well vs. others) | 1.72
(0.80-3.68) | 0.157 |
|
|
| Tumor size (>2
cm vs. ≤2 cm) | 2.42
(1.11-5.25) | 0.025 |
|
|
| Lympho-vascular
invasion (no vs. yes) | 1.06
(0.44-2.51) | 0.889 |
|
|
| Vascular invasion
(no vs. yes) | 0.70
(0.24-2.07) | 0.527 |
|
|
| Pleural invasion
(no vs. yes) | 0.97
(0.33-2.78) | 0.956 |
|
|
| Pathologic stage
(IB vs. IA) | 2.69
(1.34-5.39) | 0.005 | 1.89
(0.88-4.05) | 0.099 |
| CD155 expression
(positive vs. negative) | 3.44
(1.67-7.09) | <0.001 |
|
|
| PD-L1 (positive vs.
negative) | 2.92
(1.28-6.64) | 0.011 |
|
|
| CD155 expression
and PD-L1 expression (CD155+/PD-L1+ vs.
others) | 4.41
(1.8-10.30) | <0.001 | 3.20
(1.24-8.22) | 0.016 |
| Mode of lung
resection (sub-lobar resection vs. lobectomy) | 0.78
(0.18-3.32) | 0.741 |
|
|
| Adjuvant
chemotherapy (not performed vs. performed) | 1.36
(0.41-4.47) | 0.612 |
|
|
Discussion
The present study revealed the detailed CD155
expression in lung adenocarcinoma. As the TIGIT/CD155 axis has
emerged as a novel therapeutic target in a variety of malignant
tumors, several studies on the CD155 expression in NSCLC including
lung adenocarcinoma have been reported (14–21).
However, no study has previously reported detailed distribution of
tumoral CD155 expression. Accordingly, we quantitatively evaluated
tumoral CD155, and determined the optimal cut-off value (TPS, 5%)
using ROC-curve analysis.
Next, we showed that CD155-positivity was
significantly associated with aggressive cancer behavior such as
pleural/vascular invasion and was a significant factor to predict a
poor prognosis. Previous clinical studies in NSCLC also showed that
CD155-positivity was correlated with a poor prognosis (14,16–21).
However, characteristics of patients included in previous studies
were too heterogenous to draw a definitive conclusion. For example,
stage I–IV patients were included in 3 studies (14,18,19).
Accordingly, the present study is the first clinical study to
reveal the prognostic impact of CD155 status in homogenous patients
with early-stage lung adenocarcinoma. CD155 is a member of the
immunoglobulin superfamily, and plays important biological roles in
cell proliferation and migration as well as modulation of immune
responses (6–8,22).
CD155 expression is not detected in most normal tissues, but is
upregulated in a variety of malignant tumors. Several experimental
studies have shown that CD155 overexpression cause tumor
progression through promoting migration and invasion of cancer
cells and through inducing immune escape (22), which may reasonably explain the
poor prognosis associated with CD155-positivity.
Finally, we found that the status of
CD155+/PD-L1+ was a significant factor to
predict the poorest prognosis, and that the status of
CD155+/PD-L1+ was a significant factor to
predict a poor prognosis. Lee and coworkers also reported that
CD155+/PD-L1+ patients showed the poorest
prognosis in lung squamous cell carcinoma (19). Cancer cells may survive by
expressing PD-L1 to evade immune attack, which may be associated
with aggressive cancer behavior. Accordingly, when CD155-status and
PD-L1-status were combined, CD155+/PD-L1+
tumor may represent a highly aggressive behavior associated with
the poorest prognosis.
There are several limitations in the present study.
First, this study is a retrospective, single-center study on a
small number of patients. Second, a large proportion of patients
were lost to follow-up. Finally, the present study provided no data
on CD155 expression in p-stage II–III diseases, although two
previous studies showed that CD155 expression was significantly
higher in more advanced stages (14,18).
We are now planning to conduct a large-scale study to assess CD155
expression in other histological types of NSCLC such as squamous
cell carcinoma in addition to that in p-stage II–III diseases.
In conclusion, CD155 expression was positive in 37
patients (38.5%) of all the 96 patients with completely resected
p-stage I adenocarcinoma of the lung. CD155-positivity was
associated with aggressive tumor behavior, and was a significant
predictor of a poor prognosis. Its prognostic impact was enhanced
when it was combined with the expression status of PD-L1, where
CD155+/PD-L1+ patients showed the poorest
prognosis. A large-scale study should be conducted to draw a
convinced conclusion.
Acknowledgements
Not applicable.
Funding
This work was supported in part by the Japan Society for the
Promotion of Science (Grants-in-Aid for Scientific Research; grant
nos. 18K08806, 19K09293, 19K16786 and 20K97688), and Research Grant
for Promotion of Occupational Health by the University of
Occupational and Environmental Health (grant no. UOEH-R3).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
KK, KY and FT designed the study. RO, MK and AT
performed immunohistochemical staining. RO, KY, MT and MM evaluated
the results of IHS. HM, AT, SS, MT and KK collected the clinical
data. RO, MM, MT and KK confirm the authenticity of all the raw
data. HM, AT and SS performed statistical analyses. KY, AT and FT
wrote the manuscript. SS and MT helped to write the manuscript. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of the University of Occupational and Environmental
Health (approval no. H26-15; Kitakyushu, Japan). All participants
provided written informed consent to participate in the present
study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
NSCLC
|
non-small cell lung cancer
|
|
PD-1
|
programmed cell death 1
|
|
PD-L1
|
programmed death-ligand 1
|
|
CTL
|
cytotoxic T-lymphocyte
|
|
TIGIT
|
T-cell immunoglobulin and
immunoreceptor tyrosine-based inhibitory domain
|
|
PVR
|
poliovirus receptor
|
|
IHC
|
immunohistochemistry
|
|
TPS
|
tumor proportion score
|
|
ROC
|
receiver operating characteristic
|
|
AUC-ROC
|
area under receiver operating
characteristic curve
|
|
OS
|
overall survival
|
|
RFS
|
recurrence-free survival
|
References
|
1
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2021. CA Cancer J Clin. 71:7–33. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Planchard D, Popat S, Kerr K, Novello S,
Smit EF, Faivre-Finn C, Mok TS, Reck M, Van Schil PE, Hellmann MD,
et al: Metastatic non-small cell lung cancer: ESMO clinical
practice guidelines for diagnosis, treatment and follow-up. Ann
Oncol. 29 (Suppl 4):iv192–iv237. 2018. View Article : Google Scholar
|
|
3
|
Beatty GL and Gladney WL: Immune escape
mechanisms as a guide for cancer immunotherapy. Clin Cancer Res.
21:687–692. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sharma P, Hu-Lieskovan S, Wargo JA and
Ribas A: Primary, adaptive, and acquired resistance to cancer
immunotherapy. Cell. 168:707–723. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Andrews LP, Yano H and Vignali DAA:
Inhibitory receptors and ligands beyond PD-1, PD-L1 and CTLA-4:
Breakthroughs or backups. Nat Immunol. 20:1425–1434. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yeo J, Ko M, Lee DH, Park Y and Jin HS:
TIGIT/CD226 axis regulates anti-tumor immunity. Pharmaceuticals
(Basel). 14:2002021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Johnston RJ, Comps-Agrar L, Hackney J, Yu
X, Huseni M, Yang Y, Park S, Javinal V, Chiu H, Irving B, et al:
The immunoreceptor TIGIT regulates antitumor and antiviral
CD8+ T cell effector function. Cancer Cell. 26:923–937.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Attili I, Tarantino P, Passaro A, Stati V,
Curigliano G and de Marinis F: Strategies to overcome resistance to
immune checkpoint blockade in lung cancer. Lung Cancer.
154:151–160. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hirai A, Yoneda K, Shimajiri S, Kuroda K,
Hanagiri T, Fujino Y and Tanaka F: Prognostic impact of programmed
death-ligand 1 expression in correlation with human leukocyte
antigen class I expression status in stage I adenocarcinoma of the
lung. J Thorac Cardiovasc Surg. 155:382–392.e1. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sugaya M, Uramoto H, Uchiyama A, Nagashima
A, Nakanishi R, Sakata H, Nakanishi K, Hanagiri T and Yasumoto K:
Phase II trial of adjuvant chemotherapy with bi-weekly carboplatin
plus paclitaxel in patients with completely resected non-small cell
lung cancer. Anticancer Res. 30:3039–3044. 2010.PubMed/NCBI
|
|
12
|
Uramoto H, Nakanishi R, Nagashima A,
Uchiyama A, Inoue M, Osaki T, Yoshimatsu T, Sakata H, Nakanishi K
and Yasumoto K: A randomized phase II trial of adjuvant
chemotherapy with bi-weekly carboplatin plus paclitaxel versus
carboplatin plus gemcitabine in patients with completely resected
non-small cell lung cancer. Anticancer Res. 30:4695–4699.
2010.PubMed/NCBI
|
|
13
|
Talbot D and Massamba VK: A descriptive
review of variable selection methods in four epidemiologic
journals: There is still room for improvement. Eur J Epidemiol.
34:725–730. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nakai R, Maniwa Y, Tanaka Y, Nishio W,
Yoshimura M, Okita Y, Ohbayashi C, Satoh N, Ogita H, Takai Y and
Hayashi Y: Overexpression of Necl-5 correlates with unfavorable
prognosis in patients with lung adenocarcinoma. Cancer Sci.
101:1326–1330. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sun Y, Luo J, Chen Y, Cui J, Lei Y, Cui Y,
Jiang N, Jiang W, Chen L, Chen Y, et al: Combined evaluation of the
expression status of CD155 and TIGIT plays an important role in the
prognosis of LUAD (lung adenocarcinoma). Int Immunopharmacol.
80:1061982020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lee BR, Chae S, Moon J, Kim MJ, Lee H, Ko
HW, Cho BC, Shim HS, Hwang D, Kim HR and Ha SJ: Combination of
PD-L1 and PVR determines sensitivity to PD-1 blockade. JCI Insight.
5:e128632020. View Article : Google Scholar
|
|
17
|
Huang WC, Kuo KT, Wang CH, Yeh CT and Wang
Y: Cisplatin resistant lung cancer cells promoted M2 polarization
of tumor-associated macrophages via the Src/CD155/MIF functional
pathway. J Exp Clin Cancer Res. 38:1802019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
You H, Zhang YZ, Lai HL, Li D, Liu YQ, Li
RZ, Khan I, Hsiao WW, Duan FG, Fan XX, et al: Prognostic
significance of tumor poliovirus receptor and CTLA4 expression in
patients with surgically resected non-small-cell lung cancer. J
Cancer Res Clin Oncol. 146:1441–1450. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lee JB, Hong MH, Park SY, Chae S, Hwang D,
Ha SJ, Shim HS and Kim HR: Overexpression of PVR and PD-L1 and its
association with prognosis in surgically resected squamous cell
lung carcinoma. Sci Rep. 11:85512021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang H, Yang Z, Du G, Cao L and Tan B:
CD155-prognostic and immunotherapeutic implications based on
multiple analyses of databases across 33 human cancers. Technol
Cancer Res Treat. 20:15330338209800882021.PubMed/NCBI
|
|
21
|
Müller S, Mayer S, Möller P, Barth TFE and
Marienfeld R: Spatial distribution of immune checkpoint proteins in
histological subtypes of lung adenocarcinoma. Neoplasia.
23:584–593. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gao J, Zheng Q, Xin N, Wang W and Zhao C:
CD155, an onco-immunologic molecule in human tumors. Cancer Sci.
108:1934–1938. 2017. View Article : Google Scholar : PubMed/NCBI
|