Introduction
Hepatocellular carcinoma (HCC) ranks sixth among the
most common tumors worldwide and is responsible for ~700,000 deaths
each year (1). In China, the high
incidence and mortality rate of HCC are associated with the rapid
progression of malignant tumors caused by hepatitis B viral
infection (2). Liver resection,
liver transplantation and local ablation are common curative
approaches for early-stage patients. However, for most patients,
HCC is already of an intermediate or advanced stage at the time of
initial diagnosis; therefore, surgery is not an option for
treatment (3). The effectiveness of
systemic drug therapies has been limited; therefore, the emergence
of targeted and immunotherapy agents has held promise for the
non-surgical treatment of HCC. Among them, immune checkpoint
inhibitors (ICIs) and tyrosine kinase inhibitors (TKIs) have been
widely used in the treatment of advanced HCC (4).
Hepatic arterial infusion chemotherapy (HAIC) has
been used as a palliative chemotherapy in the treatment of patients
with intermediate or advanced HCC (5). HAIC enables the direct delivery of
chemotherapeutic drugs through the transplantable port system to
the feeding arteries of the liver tumor at higher local drug
concentrations. Notably, the incidence of adverse drug reactions in
response to systemic chemotherapy is relatively high, including
during the use of the FOLFOX regimen (fluorouracil, leucovorin, and
oxaliplatin) in patients with advanced HCC (6). HAIC has a stronger first-pass effect
than systemic chemotherapy, thus ensuring antitumor efficacy and
minimizing the toxicity associated with systemic chemotherapy
(7). It is necessary to explore and
evaluate novel therapies in the clinical treatment of HCC. At
present, because of the lack of data available from clinical drug
trials, HAIC for advanced liver cancer is not recommended by Grade
I specialists in the American Association for the Study of Liver
Diseases, European Association for Liver Diseases or Asian
Association for the Study of Liver Diseases (8–10).
However, HAIC has been used in some Asian countries, particularly
in China, Japan and South Korea, as a method to improve the
prognosis of patients with advanced HCC, and it has been included
in the relevant treatment guidelines (11). A number of studies have reported
that HAIC therapy serves an increasingly important role in the
treatment of liver cancer by improving its antitumor targeting
ability, reducing the impact on the surrounding normal tissues and
reducing the incidence of serious adverse events (AEs) (7,12).
Previous studies have evaluated the therapeutic
effect of HAIC in palliative and adjuvant chemotherapy in patients
with HCC (7,12). However, the results of analyses on
the efficacy and safety of HAIC vary significantly among different
studies (12,13). Moreover, clinical trials of ICI/TKI
treatment for advanced HCC have yielded a series of significant
results with moderate treatment-related AEs (14–19).
Therefore, the primary objective of the present systematic review
and meta-analysis was to evaluate the prognostic outcome and safety
analysis of combining HAIC with ICIs/TKIs in patients with HCC.
Materials and methods
Search strategy and literature
selection
Using PubMed (https://pubmed.ncbi.nlm.nih.gov/), the Cochrane
Library (https://www.cochranelibrary.com/), Embase (https://www.embase.com/), and Sinomed (http://www.sinomed.ac.cn/), clinical literature on the
treatment of HCC published before March 2023 was searched. The key
words searched included ‘hepatocellular carcinoma’, ‘HCC’, ‘HAIC’,
‘hepatic arterial infusion chemotherapy’, ‘ICI’, ‘PD-1’, ‘PD-L1’,
‘efficacy’ and ‘safety’, and the corresponding Chinese key words
were also searched. Furthermore, the search was supplemented by
manually reviewing the reference lists of the retrieved articles.
Two authors independently conducted the screening of the research
literature; in the case of a disagreement, this was discussed with
a third author and resolved.
Inclusion and exclusion criteria
The inclusion criteria were as follows: i) Study
subjects were patients with unresectable HCC; ii) officially
released clinical data, including registered clinical trial data
and investigator-initiated clinical study data; iii) first-line
treatment strategies for advanced liver cancer; iv) treatment
options included ICI combination therapy (PD-1/PD-L1 inhibitors),
HAIC therapy and HAIC combined with ICI/TKI therapy; v) the study
literature had complete efficacy or safety data. The exclusion
criteria were as follows: i) Study literature of non-HCC, including
cholangiocarcinoma and mixed liver cancer; ii) non-clinical study
literature, such as basic research and case reports; iii) studies
of second-line or multiline therapy; iv) the treatment strategy did
not meet the requirements of this study; v) efficacy or safety data
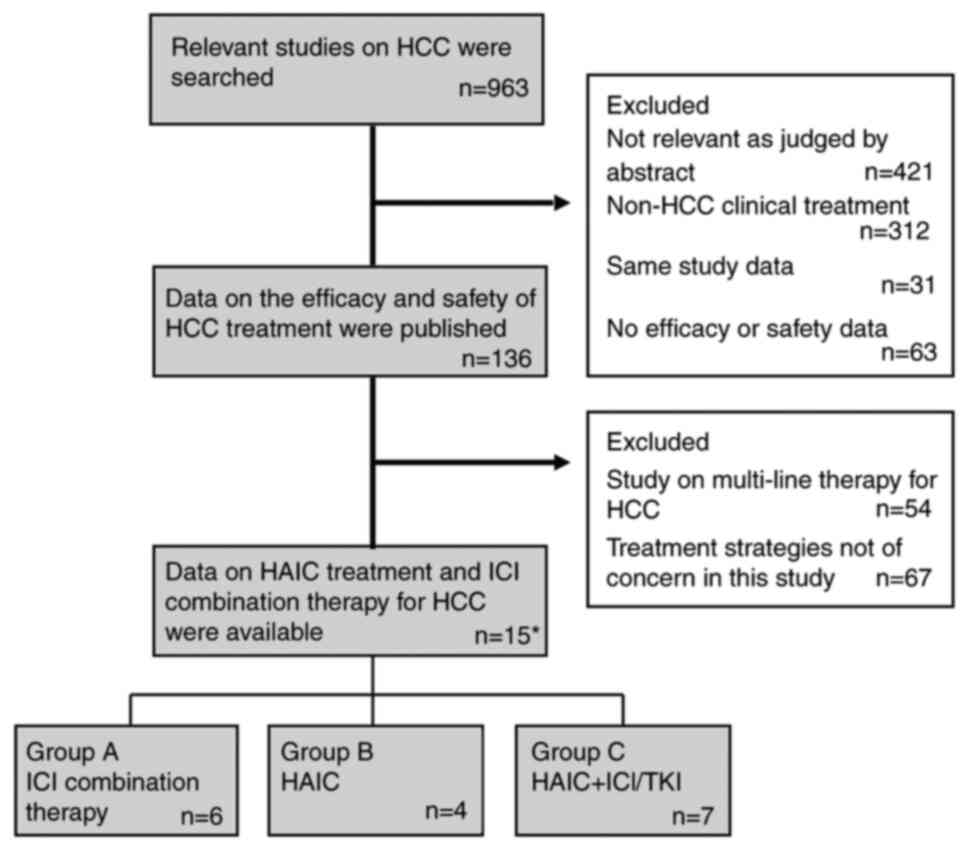
were not available. The literature screening process is shown in
Fig. 1. All treatments were divided
into three groups: ICIs + other systemic therapies (group A), HAIC
therapy alone (group B), and HAIC + ICI/TKI therapy (group C).
Literature quality evaluation and data
extraction
The risk of bias was assessed using the Cochrane
Collaboration (version 5.1.0; The Cochrane Institute) (20). Two authors assessed each study for
bias and scored it as follows: Low risk of bias, high risk of bias,
or ambiguity. Ambiguity was defined as the lack of information on
ascertainment bias or uncertainty about bias. Through detailed
screening of the included literature, author information, year of
publication, study population, study design information, treatment
groups, sample size, progression-free survival (PFS), overall
survival (OS) and adverse event (AE) information were extracted.
This information was collected, checked by the second author and
then analyzed. Ultimately, the literature included in the present
study met the criteria for meta-analysis.
Statistical analysis
SPSS 20.0 statistical software (IBM Corp.) was used
to organize and analyze the data. Count data are presented as
frequency and percentage, and comparisons for occurrence of AEs
between groups were performed using the χ2 test. A
routine meta-analysis was performed using STATA 14.0 software
(StataCorp LLC). The expected median PFS (mPFS) and OS (mOS) with
95% CIs were calculated using a random effects model, and were used
as the primary study endpoints to assess the treatment effect of
the trial group (group C) vs. the control group (group A and B).
P<0.05 was considered to indicate a statistically significant
difference.
Results
General information
In the present systematic review, a total of 17
treatment groups from 15 studies were assessed, including 1,987
patients with HCC; specific information is shown in Table I (14–19,21–29).
The study was divided into three treatment groups: The ICIs + other
systemic therapies group, the HAIC therapy alone group and the HAIC
+ ICI/TKI therapy group. The year of publication for all studies
was between 2020 and 2022. With the exception of one study that
included global population data (atezolizumab + bevacizumab), the
remaining study populations were Chinese. Of the 17 treatment
groups within 15 studies, five groups underwent randomized
controlled clinical trials, five groups underwent cohort studies,
and the remaining seven groups underwent single-arm studies. Of
these, there were 1,068 subjects in group A, 472 subjects in group
B and 447 subjects in group C. The target population in all groups
in the present study was largely dominated by patients unsuitable
for surgical treatment, with Barcelona Clinic Liver Cancer stage B
or C, Eastern Cooperative Oncology Group performance status ≤2 or
Child-Pugh score A or B, as shown in Table I. The inclusion criteria remained
consistent for the target population in the three groups;
therefore, the efficacy and safety of the treatments could be
compared between the three groups in the present study.
 | Table I.Basic information of each study on the
first-line treatment of advanced HCC. |
Table I.
Basic information of each study on the
first-line treatment of advanced HCC.
| A, Group A |
|---|
|
|---|
| First author,
year | Study population | Study design | Treatment group | Sample size | Target patients | (Refs.) |
|---|
| Finn, 2020 | Global | RCT |
Atezolizumab/bevacizumab | 336 | 1.
Inoperable-resected advanced HCC; 2. Child-Pugh score A, B or C; 3.
ECOG score 0–1 | (14) |
| Ren, 2021 | Chinese | RCT |
Sintilimab/bevacizumab | 380 | 1.
Inoperable-resected advanced HCC; 2. Child-Pugh score ≤7; 3. ECOG
score 0–1 | (15) |
| Liu, 2021 | Chinese | Cohort study |
Camrelizumab/sorafenib | 35 | 1. Child-Pugh score
A or B; 2. ECOG score 0–1 | (16) |
| Mei, 2021 | Chinese | Cohort study | Lenvatinib/PD-1
inhibitors | 25 | 1. BCLC stage B or
C; 2. Child-Pugh score A or B | (17) |
| Qin, 2022 | Chinese | RCT |
Camrelizumab/apatinib | 272 | 1. BCLC stage B or
C; 2. Child-Pugh score A; 3. ECOG score 0–1 | (18) |
| Chen, 2022 | Chinese | Single-arm |
Sintilimab/anlotinib | 20 | 1. BCLC stage B or
C; 2. Child-Pugh score ≤7; 3. ECOG score 0–1 | (19) |
|
| B, Group
B |
|
| First author,
year | Study
population | Study
design | Treatment
group | Sample
size | Target
patients | (Refs.) |
|
| Mei, 2021 | Chinese | Cohort study | HAIC:
Oxaliplatin/leucovorin/fluorouracil | 148 | 1. BCLC stage B or
C; 2. Child-Pugh score A | (21) |
| Wu, 2022 | Chinese | Single-arm | HAIC:
Oxaliplatin/raltitrexed | 35 | 1. Patients with
HCC for trans arterial chemoembolization failed; 2. Child-Pugh
score ≤6; 3. ECOG PS ≤1 | (22) |
| Lyu, 2021 | Chinese | RCT | HAIC:
Oxaliplatin/leucovorin/fluorouracil | 130 | 1. Patients with
advanced HCC; 2. Child-Pugh score ≤7; 3. ECOG PS ≤2 | (23) |
| Li, 2021 | Chinese | RCT | HAIC:
Oxaliplatin/leucovorin/fluorouracil | 159 | 1. Unresectable
late stage HCC; 2. BCLC stage A-B; 3. Maximum lesion ≥7 cm
(Response Evaluation Criteria in Solid Tumours 1.1); 4. Child-Pugh
score A; 5. ECOG score 0–1 | (24) |
|
| C, Group
C |
|
| First author,
year | Study
population | Study
design | Treatment
group | Sample
size | Target
patients | (Refs.) |
|
| Mei, 2021 | Chinese | Cohort study | HAIC + PD-1
inhibitors | 81 | 1. BCLC stage B or
C; 2. Child-Pugh score A | (21) |
| Xin, 2022 | Chinese | Single-arm | HAIC +
atezolizumab/bevacizumab | 52 | 1. First-treated
and untreated advanced HCC; 2. BCLC stage C; 3. Child-Pugh score
A | (25) |
| Xu, 2022 | Chinese | Single-arm | HAIC +
PD-1/lenvatinib | 61 | 1. Not suitable for
surgical treatment; 2. BCLC stage B or C; 3. ECOG PS ≤2; 4.
Child-Pugh score A or B | (26) |
| Luo, 2022 | Chinese | Single-arm | HAIC +
PD-1/TKIs | 145 | 1. Patients with
unresectable advanced HCC | (27) |
| Mei, 2021 | Chinese | Cohort study | HAIC +
PD-1/lenvatinib | 45 | 1. Not suitable for
surgical treatment; 2. BCLC stage B or C; 3. Child-Pugh score A or
B | (17) |
| Lai, 2022 | Chinese | Single-arm | HAIC +
toripalimab/lenvatinib | 36 | 1. Patients with
unresectable advanced HCC | (28) |
| Liu, 2021 | Chinese | Single-arm | HAIC +
PD-1/TKIs | 27 | 1. BCLC stage C
(presence of vascular invasion); 2. Child-Pugh score A or B | (29) |
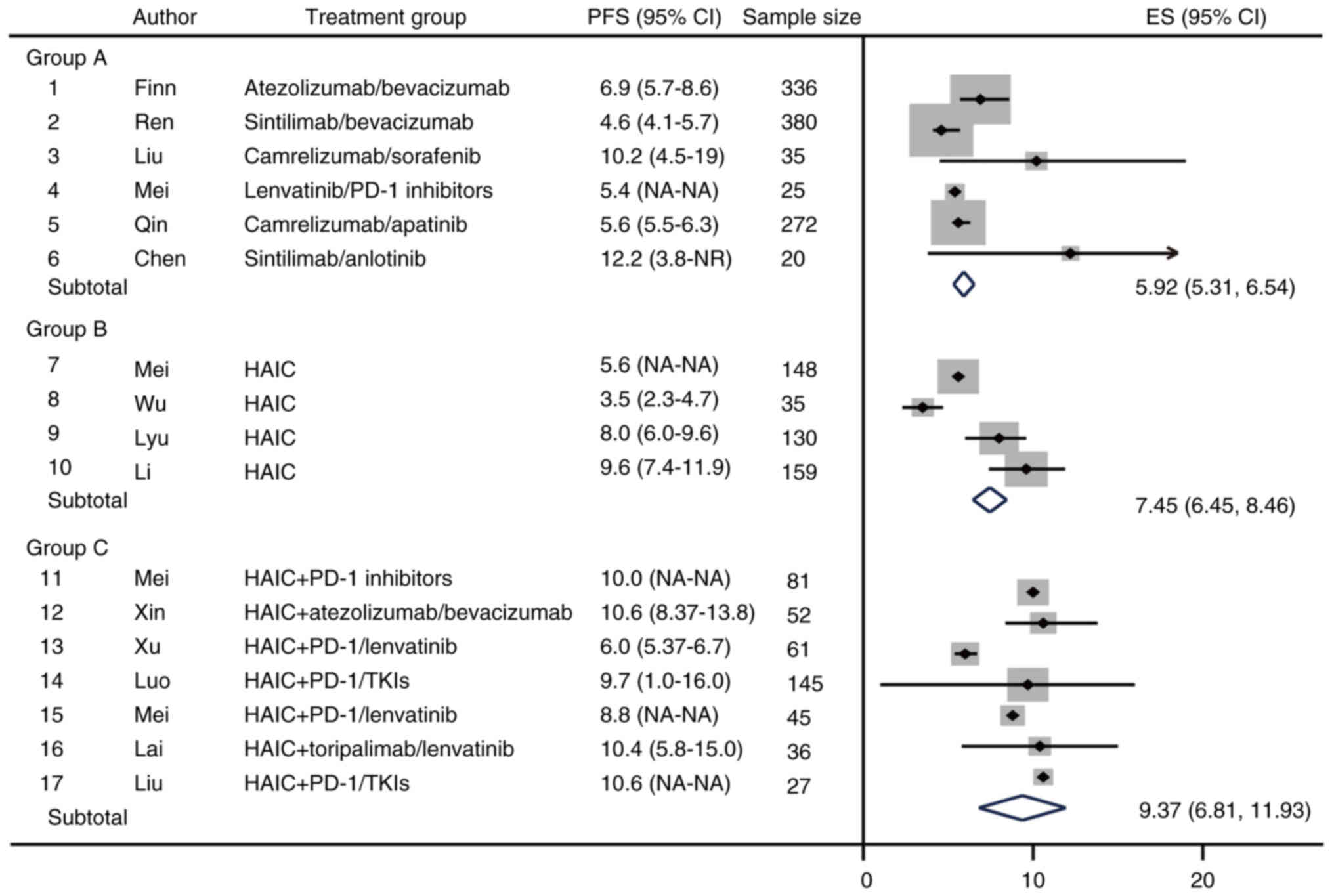
Effectiveness endpoint: PFS
The present study performed a meta-analysis on one
of the efficacy endpoints of the included studies, median PFS
(mPFS). The results showed that the estimated mPFS (95% CI) in
group C was 9.37 months (6.81–11.93); in group B was 7.45 months
(6.45–8.46); and in group A was 5.92 months (5.31–6.54) (Fig. 2). Specifically, the efficacy of
sintilimab combined with anlotinib was best in group A with a mPFS
of 12.2 months. However, sintilimab combined with anlotinib for HCC
was designed as a single-arm study with no data from the control
group (19). In group B, HAIC
therapy mainly consisted of oxaliplatin/leucovorin/fluorouracil,
with the longest mPFS of 9.6 months. In group C, HAIC + ICI/TKI
treatment the longest median PFS was 10.6 months (Fig. 2). These results indicated that for
the PFS of patients with advanced HCC, HAIC + ICI/TKI had the best
efficacy, followed by HAIC alone, while ICIs + other systemic
therapies was poor.
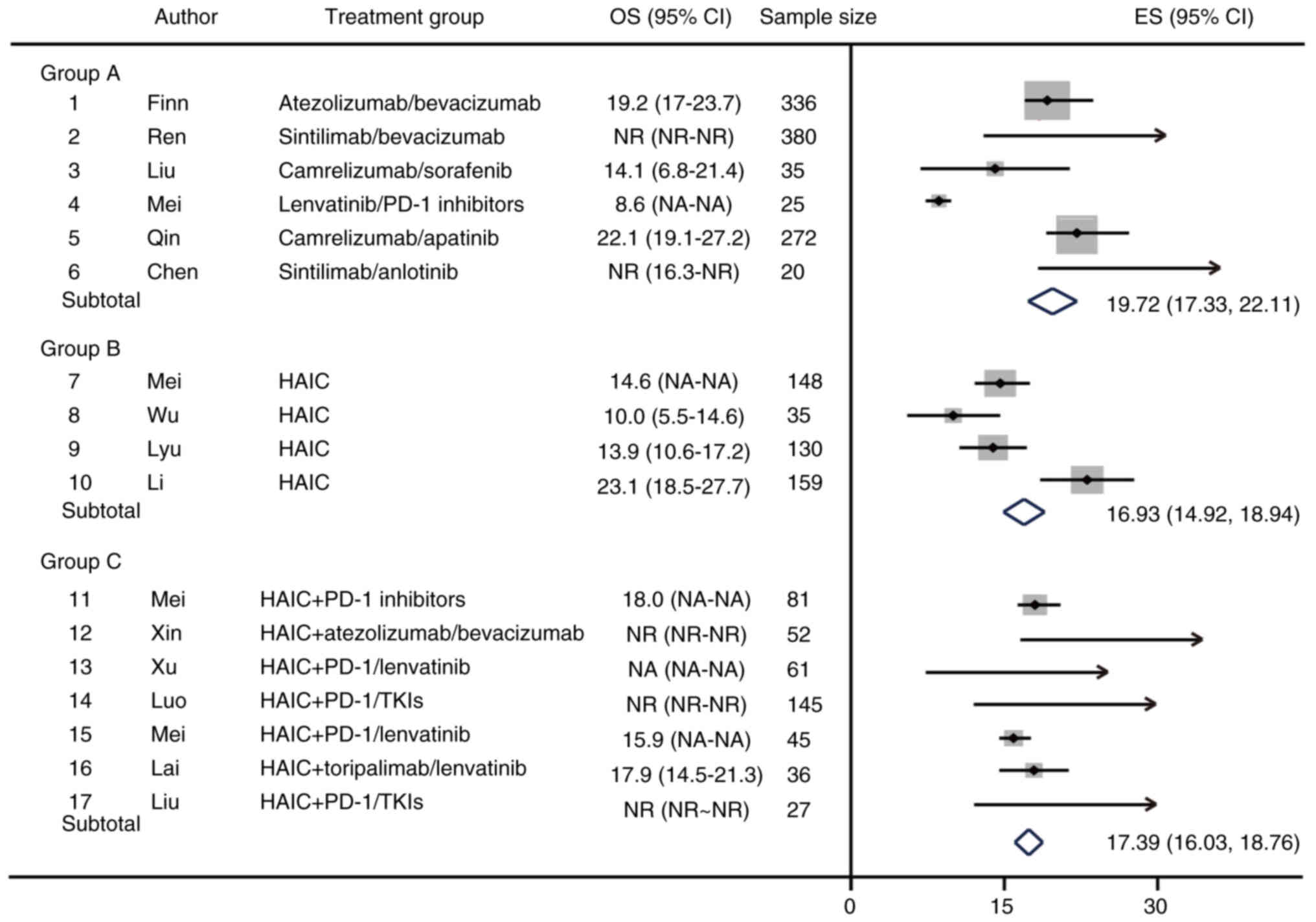
Effectiveness endpoint: OS
A meta-analysis of OS as a primary endpoint for the
included studies was also performed. In group A, the expected
median OS (mOS) (95% CI) was 19.72 months (17.33–22.11);
camrelizumab and apatinib had the best efficacy, with a mOS of 23.1
months (Fig. 3). However, in group
A, the mOS was not achieved in response to sintilimab/bevacizumab
and sintilimab/anlotinib therapies, and the median follow-up time
were 14.0 and 16.3 months, respectively. In group B, the expected
mOS (95% CI) was 16.93 months (14.92–18.94) and the longest median
OS was 23.1 months. Furthermore, in group C, mOS was not reached in
three studies, with median follow-up times of 15.6, 12.5 and 12.9
months, respectively. One study of HAIC + PD-1/lenvatinib did not
provide OS outcome data. The results of the remaining study showed
an expected median OS (95% CI) in group C of 17.39 months
(16.03–18.76) (Fig. 3). In group C,
the expected mOS was longer than that in group B, but shorter than
that in group A, and the possible reason is that the OS events in a
number of studies were not reached during the follow-up time.
Safety data: Occurrence of AEs above
level 3
The occurrence of treatment-related AEs was
collected from the included studies, and AEs were summarized
according to the groups A, B and C, as shown in Table II. Statistical analysis of AEs
above grade 3 with an incidence of >5% in group C were
statistically analyzed. Among them, the occurrence of AEs was
different between group C and group A/B (control group). In group
C, the incidence of hypertension [11/176 (6.25%)] was significantly
different from that in group A [207/1,036 (19.98%)] (P<0.001) or
in group B [0/128 (0%)] (P=0.004). Most of the remaining AEs above
grade 3 in group C were not significantly different compared with
that in the other two groups. For example, increased AST [14/221
(6.33%)], increased alanine transaminase (ALT) [13/221 (5.88%)],
and decreased platelet count [13/221 (5.88%)] in this group were
not significantly higher than those in groups A (P>0.05).
Moreover, group C was not statistically different compared with
group B (P>0.05)f regarding increased ALT and decreased platelet
count, whereas group C had a significantly lower incidence of
increased AST than group B (6.33% vs. 13.13%; P=0.003). Therefore,
the types of AEs in the HAIC + ICI/TKI group were not significantly
different from those in the other groups, indicating that this
treatment has a good safety profile.
| Table II.Summary of grade 3 or above AEs. |
Table II.
Summary of grade 3 or above AEs.
| AE | Group A | Group B | Group
Ca | P value, group C
vs. A | P value, group C
vs. B |
|---|
| Hypertension | 207/1,036
(19.98%) | 0/128 (0%) | 11/176 (6.25%) | <0.001 | 0.004 |
| Proteinuria | 47/1,001
(4.70%) | 0/128 (0%) | 5/115 (4.35%) | - | - |
| Decreased WBC
count | 11/732 (1.50%) | 15/285 (5.26%) | 2/97 (2.06%) | - | - |
| Fatigue | 12/769 (1.56%) | 0/320 (0%) | 3/221 (1.36%) | - | - |
| Hand-foot
syndrome | 36/1,061
(3.39%) | 0/128 (0%) | 3/169 (1.78%) | - | - |
| Increased blood
bilirubin | 57/1,061
(5.37%) | 8/320 (2.50%) | 4/221 (1.81%) | - | - |
| Pyrexia | 6/769 (0.78%) | 0/285 (0%) | 1/185 (0.54%) | - | - |
| Increased AST | 77/1,026
(7.50%) | 42/320
(13.13%) | 14/221 (6.33%) | 0.544 | 0.003 |
| Increased ALT | 53/1,026
(5.17%) | 19/320 (5.94%) | 13/221 (5.88%) | 0.666 | 0.979 |
| Decreased
neutrophil count | 24/697 (3.44%) | 14/285 (4.91%) | 8/221 (3.62%) | - | - |
| Decreased platelet
count | 77/1,061
(7.26%) | 20/320 (6.25%) | 13/221 (5.88%) | 0.467 | 0.861 |
|
Nausea/vomiting | 4/769 (5.20%) | 14/320 (4.38%) | 6/221 (2.71%) | - | - |
| Decreased
appetite | 6/734 (0.82%) | 1/163 (0.61%) | 1/97 (1.03%) | - | - |
| Abdominal pain | 8/744 (1.08%) | 2/285 (0.70%) | 8/221 (3.62%) | - | - |
| Diarrhea | 16/661 (2.42%) | 3/285 (1.05%) | 2/221 (0.90%) | - | - |
| Rash | 2/769 (0.26%) | 0/128 (0%) | 2/133 (1.50%) | - | - |
| Cutaneous vascular
hyperplasia | 7/272 (2.57%) | - | 1/88 (1.14%) | - | - |
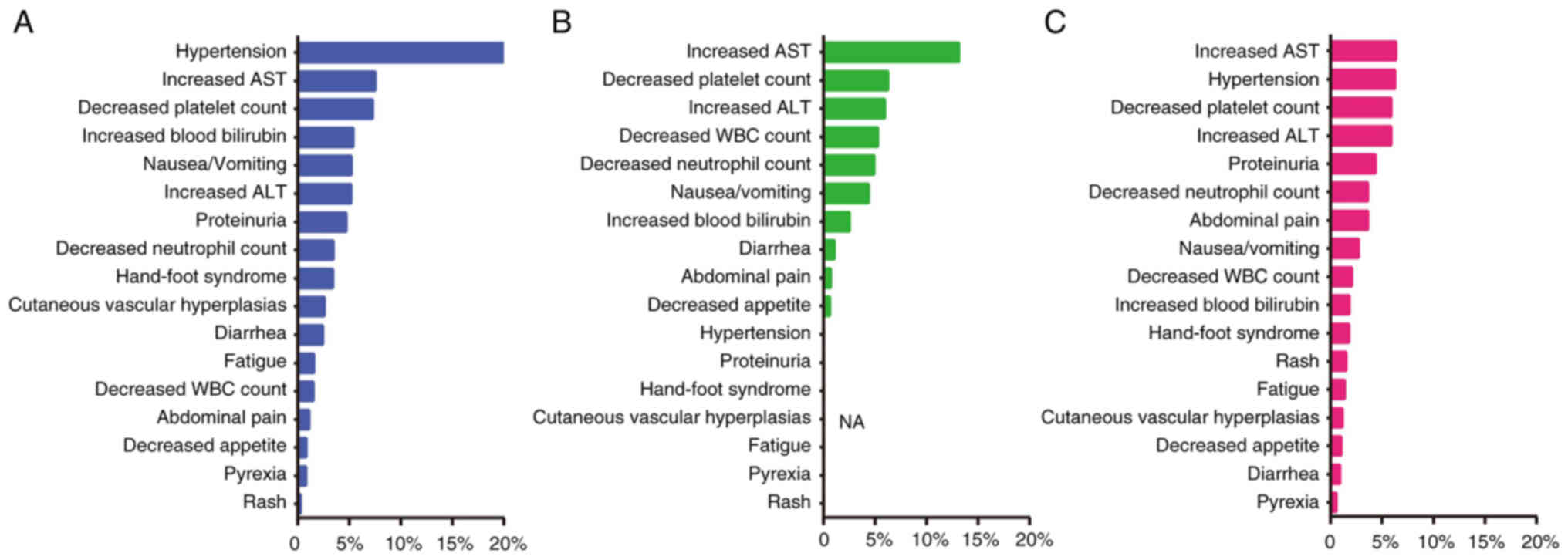
Ranking of treatment-related AEs among
the groups
The present study ranked the occurrence of AEs above
level 3 by groups, as shown in Fig.
4. The results showed that in group A, the top
treatment-related AEs were: Hypertension, increased AST, decreased
platelet count, increased blood bilirubin and nausea/vomiting. In
group B, the occurrence of AEs above grade 3 were different from
those in group A; the top AEs in this group were: Increased AST,
decreased platelet count, increased ALT, decreased white blood cell
count and decreased neutrophil count. In group C, the overall
incidence of AEs above grade 3 was low, and the ranking was as
follows: Increased AST, hypertension, decreased platelet count,
increased ALT and proteinuria.
Discussion
Due to the lack of clinical randomized controlled
trials directly comparing different treatments of HCC, the present
meta-analysis used data from three treatment groups, generated from
17 published treatment groups, to indirectly evaluate the efficacy
and safety of ICI + other systemic therapy, HAIC alone and HAIC +
ICI/TKI therapy.
HAIC was first proposed in Japan, and has been used
in Japan, South Korea and other Asian countries for >30 years.
Notably, it is recommended by the Japanese Society for Liver
Disease consensus clinical practice guidelines as the standard
treatment for liver cancer with portal venous tumor thrombosis
(30). Currently, there is no
universal standard for HAIC therapy, either with a single drug or
with a combination of different drugs. The most widely used
regimens include cisplatin monotherapy, the FAIT regimen
(interferon and fluorouracil) and the FOLFOX regimen (31–33).
The present results showed that group C had the
longest estimated mPFS (95% CI) at 9.37 months (6.81–11.93); much
higher than that in groups A and B. However, there was no
significant difference in the expected mOS among the three groups,
which may be because the OS events in a number of studies were not
reached during the follow-up time. For example, in group C, the
median follow-up time of three studies was 15.6, 12.5 and 12.9
months, respectively, but the mOS was not reached. It is clear that
the final mOS of these studies may be markedly higher than the
follow-up duration, thus directly affecting the overall OS outcome
in this group. OS is usually recommended as the primary endpoint of
phase 2/3 clinical trials for the treatment of advanced liver
cancer. However, OS also has limitations, such as the need for
long-term follow-up to obtain the number of events. Surrogate
endpoints are often used by the Food and Drug Administration and
National Medical Products Administration for the approval of drug
marketing applications under an accelerated plan. In the clinical
study design of advanced liver cancer, surrogate endpoints are
widely used, such as PFS (34). In
a number of studies regarding the clinical treatment of tumors,
there is a significant association between PFS and OS (35,36).
In order to analyze the occurrence of AEs above
grade 3 in group C, the occurrence of AEs in groups A and B were
compared in the present study. The results showed that the
incidence of AEs above grade 3 in group C was not significantly
different compared with those in the other two groups, showing a
good safety profile. In other studies, the effectiveness and high
safety profile of HAIC combined with ICI/TKI therapy has been
verified in the treatment of advanced HCC (21,27).
The present study has several limitations. First,
only 17 treatment groups from 15 studies met the inclusion criteria
for the meta-analysis, and potential bias in these studies may have
influenced the study findings. As the pathogenesis and prevalence
of HCC vary widely across regions and populations, the population
in the present study was mostly Chinese. In addition, the target
population of the present study included patients with
intermediate/advanced HCC with no surgical options and systemic
medication strategies preferred for first-line therapy. Notably,
these facts may limit the generalizability of the present findings.
Second, some of the included study designs were observational,
which led to some selection bias. In addition, the present
meta-analysis lacks a direct ‘head-to-head’ design of the three
treatment options, thus the relative differences between the groups
could only be obtained by indirect comparisons. Moreover, among the
OS results in the present study, several treatment groups had short
follow-up times and did not reach mOS within these times. These
factors all had a direct effect on the final result.
In conclusion, the present study demonstrated that,
in patients with advanced HCC, treatment with HAIC + ICI/TKI
therapy significantly improved the PFS compared with the other
treatment options. Although mOS was not reached because of the
follow-up times of the available studies, the available data
indicated that the OS of group C was not significantly different
from that in the other treatment groups. In addition, the safety
data showed that the treatment-related AEs in group C were not
significantly higher compared with those in the other treatment
groups. Therefore, the results of the present study suggested that
HAIC combined with ICI/TKI therapy has a notable efficacy and a
high safety profile in the treatment of patients with advanced
HCC.
Acknowledgements
Not applicable.
Funding
This study was supported by the Natural Science Foundation of
Jiangsu Province (grant no. BK20200275) and the Foundation of
Jinling Hospital (grant no. 22LCZLXJS57).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XL conceived of and designed the study. ZL, YX and
WQ performed data acquisition, data analysis and manuscript
preparation. PL, YZ, HL and YG assisted with data acquisition, data
analysis and statistical analysis. YX and WQ confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tian T, Song C, Jiang L, Dai J, Lin Y, Xu
X, Yu C, Ge Z, Ding Y, Wen Y, et al: Hepatitis B virus infection
and the risk of cancer among the Chinese population. Int J Cancer.
147:3075–3084. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Vogel A, Meyer T, Sapisochin G, Salem R
and Saborowski A: Hepatocellular carcinoma. Lancet. 400:1345–1362.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liu Y, Pan J, Gao F, Xu W, Li H and Qi X:
Efficacy and Safety of PD-1/PD-L1 inhibitors in advanced
hepatocellular carcinoma: A systematic review and meta-analysis.
Adv Ther. 40:521–549. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liu J, Zhang J, Wang Y, Shu G, Lou C and
Du Z: HAIC vs. TACE for patients with unresectable hepatocellular
carcinoma: A systematic review and meta-analysis. Medicine
(Baltimore). 101:e323902022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lin CC, Yang TS, Yen CJ, Cheng R, Liu J
and Hsu C: Safety and preliminary efficacy of ramucirumab in
combination with FOLFOX4 in patients with advanced hepatocellular
carcinoma: A nonrandomized, open-label, phase Ib study. Oncologist.
25:e1921–e1929. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang Z, Tong Y, Yang L, He X, Bao G and Du
X: Identifying optimal therapies in patients with advanced
hepatocellular carcinoma: A systematic review and network
meta-analysis. Transl Gastroenterol Hepatol. 7:382022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
European Association for the Study of the
Liver. Electronic address, . simpleeasloffice@easloffice.eu:
Corrigendum to ‘EASL clinical practice guidelines: Management of
hepatocellular carcinoma’ [J Hepatol 69 (2018) 182–236]. J Hepatol.
70:8172019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Benson AB, D'Angelica MI, Abbott DE,
Abrams TA, Alberts SR, Anaya DA, Anders R, Are C, Brown D, Chang
DT, et al: Guidelines Insights: Hepatobiliary cancers, version
2.2019. J Natl Compr Canc Netw. 17:302–310. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Omata M, Cheng AL, Kokudo N, Kudo M, Lee
JM, Jia J, Tateishi R, Han KH, Chawla YK, Shiina S, et al:
Asia-Pacific clinical practice guidelines on the management of
hepatocellular carcinoma: A 2017 update. Hepatol Int. 11:317–370.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kokudo N, Takemura N, Hasegawa K, Takayama
T, Kubo S, Shimada M, Nagano H, Hatano E, Izumi N, Kaneko S, et al:
Clinical practice guidelines for hepatocellular carcinoma: The
Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019
update. Hepatol Res. 49:1109–1113. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu H, Qin X, Jiang H, Sun C, Wu M, Xu Z,
Lu T, Ma X and Han Z: Comparison of hepatic arterial infusion
chemotherapy and transarterial chemoembolization for advanced
hepatocellular carcinoma: A systematic review and meta-analysis. J
Gastrointestin Liver Dis. 31:336–343. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kong S, Yu H, Wang H, Song J and Yan J:
Hepatic arterial infusion chemotherapy combined with sorafenib vs.
sorafenib alone for advanced hepatocellular carcinoma: A systematic
review and meta-analysis. Clin J Gastroenterol. Sep 23–2023.(Epub
ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux
M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al: Atezolizumab
plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J
Med. 382:1894–1905. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ren Z, Xu J, Bai Y, Xu A, Cang S, Du C, Li
Q, Lu Y, Chen Y, Guo Y, et al: Sintilimab plus a bevacizumab
biosimilar (IBI305) vs. sorafenib in unresectable hepatocellular
carcinoma (ORIENT-32): A randomised, open-label, phase 2–3 study.
Lancet Oncol. 22:977–990. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liu Q, You N, Li J, Wu K, Peng X, Wang Z,
Wang L, Zhu Y and Zheng L: Camrelizumab plus sorafenib vs.
sorafenib monotherapy for advanced hepatocellular carcinoma: A
retrospective analysis. Front Oncol. 11:6944092021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mei J, Tang YH, Wei W, Shi M, Zheng L, Li
SH and Guo RP: Hepatic arterial infusion chemotherapy combined with
PD-1 inhibitors plus lenvatinib vs. PD-1 inhibitors plus lenvatinib
for advanced hepatocellular carcinoma. Front Oncol. 11:6182062021.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qin S: Camrelizumab combined with apatinib
for first-line treatment of unresectable or metastatic
hepatocellular carcinoma: Total population and Chinese subgroup
results. 2022.CSCO Annual Meeting 2 oral report. Available:.
http://meeting.csco.org.cn/Resource/
|
|
19
|
Chen X, Li W, Wu X, Zhao F, Wang D, Wu H,
Gu Y, Li X, Qian X, Hu J, et al: Safety and efficacy of sintilimab
and anlotinib as first line treatment for advanced hepatocellular
carcinoma (KEEP-G04): A single-arm phase 2 study. Front Oncol.
12:9090352022. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
van Tulder M, Furlan A, Bombardier C and
Bouter L; Editorial Board of the Cochrane Collaboration Back Review
Group, : Updated method guidelines for systematic reviews in the
cochrane collaboration back review group. Spine (Phila Pa 1976).
28:1290–1299. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mei J, Li SH, Li QJ, Sun XQ, Lu LH, Lin
WP, Zheng L, Chen MS, Shi M, Wei W and Guo RP: Anti-PD-1
immunotherapy improves the efficacy of hepatic artery infusion
chemotherapy in advanced hepatocellular carcinoma. J Hepatocell
Carcinoma. 8:167–176. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wu Y, Zheng S, Zhang Z, Chen G, Chen X,
Zheng T, Guo X, Chen H, Wang M, Xie X and Zhang B: Hepatic arterial
infusion chemotherapy with oxaliplatin plus raltitrexed as an
alternative option in advanced hepatocellular carcinoma patients
with failure of, or unsuitability for, transarterial
chemoembolization. Medicina (Kaunas). 58:13432022. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lyu N, Wang X, Li JB, Lai JF, Chen QF, Li
SL, Deng HJ, He M, Mu LW and Zhao M: Arterial chemotherapy of
oxaliplatin plus fluorouracil vs. sorafenib in advanced
hepatocellular carcinoma: A biomolecular exploratory, Randomized,
phase III trial (FOHAIC-1). J Clin Oncol. 40:468–480. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li QJ, He MK, Chen HW, Fang WQ, Zhou YM,
Xu L, Wei W, Zhang YJ, Guo Y, Guo RP, et al: Hepatic arterial
infusion of oxaliplatin, fluorouracil, and leucovorin vs.
transarterial chemoembolization for large hepatocellular carcinoma:
A Randomized phase III trial. J Clin Oncol. 40:150–160. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xin Y, Cao F, Yang H, Zhang X, Chen Y, Cao
X, Zhou X, Li X and Zhou J: Efficacy and safety of atezolizumab
plus bevacizumab combined with hepatic arterial infusion
chemotherapy for advanced hepatocellular carcinoma. Front Immunol.
13:9291412022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Xu Y, Fu S, Mao Y, Huang S, Li D and Wu J:
Efficacy and safety of hepatic arterial infusion chemotherapy
combined with programmed cell death protein-1 antibody and
lenvatinib for advanced hepatocellular carcinoma. Front Med
(Lausanne). 9:9190692022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Luo L, Xiao Y, Zhu G, Huang A, Song S,
Wang T, Ge X, Xie J, Deng W, Hu Z, et al: Hepatic arterial infusion
chemotherapy combined with PD-1 inhibitors and tyrosine kinase
inhibitors for unresectable hepatocellular carcinoma: A tertiary
medical center experience. Front Oncol. 12:10046522022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lai Z, He M, Bu X, Xu Y, Huang Y, Wen D,
Li Q, Xu L, Zhang Y, Wei W, et al: Lenvatinib, toripalimab plus
hepatic arterial infusion chemotherapy in patients with high-risk
advanced hepatocellular carcinoma: A biomolecular exploratory,
phase II trial. Eur J Cancer. 174:68–77. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Liu BJ, Gao S, Zhu X, Guo JH, Kou FX, Liu
SX, Zhang X, Wang XD, Cao G, Chen H, et al: Real-world study of
hepatic artery infusion chemotherapy combined with anti-PD-1
immunotherapy and tyrosine kinase inhibitors for advanced
hepatocellular carcinoma. Immunotherapy. 13:1395–1405. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kokudo N, Hasegawa K, Akahane M, Igaki H,
Izumi N, Ichida T, Uemoto S, Kaneko S, Kawasaki S, Ku Y, et al:
Evidence-based Clinical Practice Guidelines for Hepatocellular
Carcinoma: The Japan Society of Hepatology 2013 update (3rd JSH-HCC
Guidelines). Hepatol Res. 45:2015. View Article : Google Scholar
|
|
31
|
Long F, Chen S, Li R, Lin Y, Han J, Guo J,
Chen Y, Li C and Song P: Efficacy and safety of HAIC alone vs. HAIC
combined with lenvatinib for treatment of advanced hepatocellular
carcinoma. Med Oncol. 40:1472023. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhang W, Ouyang D, Huang Z and Che X:
Hepatic arterial infusion chemotherapy vs. sorafenib for advanced
hepatocellular carcinoma with portal vein tumor thrombus: An
updated meta-analysis and systematic review. Front Oncol.
13:10851662023. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zheng K, Zhu X, Fu S, Cao G, Li WQ, Xu L,
Chen H, Wu D, Yang R, Wang K, et al: Sorafenib plus hepatic
arterial infusion chemotherapy vs. sorafenib for hepatocellular
carcinoma with major portal vein tumor thrombosis: A Randomized
trial. Radiology. 303:455–464. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Llovet JM, Villanueva A, Marrero JA,
Schwartz M, Meyer T, Galle PR, Lencioni R, Greten TF, Kudo M,
Mandrekar SJ, et al: Trial design and endpoints in hepatocellular
carcinoma: AASLD consensus conference. Hepatology. 73 (Suppl
1):S158–S191. 2021. View Article : Google Scholar
|
|
35
|
Wang ZX, Wu HX, Xie L, Lin WH, Liang F, Li
J, Yang ZM and Xu RH: Exploration of modified progression-free
survival as a novel surrogate endpoint for overall survival in
immuno-oncology trials. J Immunother Cancer. 9:e0021142021.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Llovet JM, Montal R and Villanueva A:
Randomized trials and endpoints in advanced HCC: Role of PFS as a
surrogate of survival. J Hepatol. 70:1262–1277. 2019. View Article : Google Scholar : PubMed/NCBI
|