Introduction
Pancreatic ductal adenocarcinoma (PDAC) is one of
the deadliest solid cancers, worldwide (1,2).
Surgery has long been considered a fundamental treatment option for
this lethal disease (3–5). Despite ongoing improvements (6–11),
pancreatic cancer surgery is often associated with significant
intraoperative blood loss and the subsequent need for allogeneic
blood transfusion (ABT) (12–14).
The transfusion rate in patients who have undergone a pancreatic
resection still falls in the 20 to 30% range, even when the
procedure was performed by experienced surgeons in high-volume
centers (13,15,16).
Although ABT can be a lifesaving treatment during cancer surgery,
it has been linked to a variety of negative outcomes from
transfusion-related immunomodulation (TRIM) (14,17).
Indeed, our previous study using propensity score matching analysis
demonstrated the negative effects of intraoperative ABT on
postoperative survival outcomes in patients with resectable PDAC
(18). In order to minimize the use
of ABT, the focus has been shifting to blood conservation
strategies (19–21).
Acute normovolemic hemodilution (ANH) is an
intraoperative blood conservation technique. ANH is performed
immediately before the procedure and involves the removal of whole
blood, while maintaining euvolemia with crystalloid and/or colloid
solutions. ANH has been successfully performed in open-heart
surgery since the 1970s (22,23).
Subsequently, several studies, including those describing ANH use
in various types of abdominal surgery, have shown that it is safe,
inexpensive, and effectively reduces the need for ABT (24–27).
ANH also offers a medical solution that respects religious and
cultural beliefs about the use of ABT. These results seem to
indicate that ANH can compensate for the disadvantages of ABT and
improve the prognosis of patients who undergo pancreatic resection
for PDAC.
However, in contrast to evaluations of short-term
performance, few reports have examined the association between ANH
and long-term outcomes in cancer patients (21,28).
Furthermore, there is no recorded evidence linking use of ANH with
PDAC patients. Therefore, this study aimed to assess the impact of
ANH on long-term outcomes in PDAC patients undergoing radical
surgery. We herein present the potentially negative impact of ANH
on long-term oncological outcomes in patients with PDAC.
Materials and methods
Patients and study design
This single-center, retrospective cohort study was
approved by the Committee of Medical Ethics of Hirosaki University
Graduate School of Medicine (Aomori, Japan; reference no.
2022-032). Informed consent was obtained in the form of an opt-out
system on our website (https://www.med.hirosaki-u.ac.jp/hospital/outline/resarch/resarch.html),
which also had the approval of the Committee of Medical Ethics of
Hirosaki University Graduate School of Medicine. Our study did not
include minors. This study was designed and carried out in
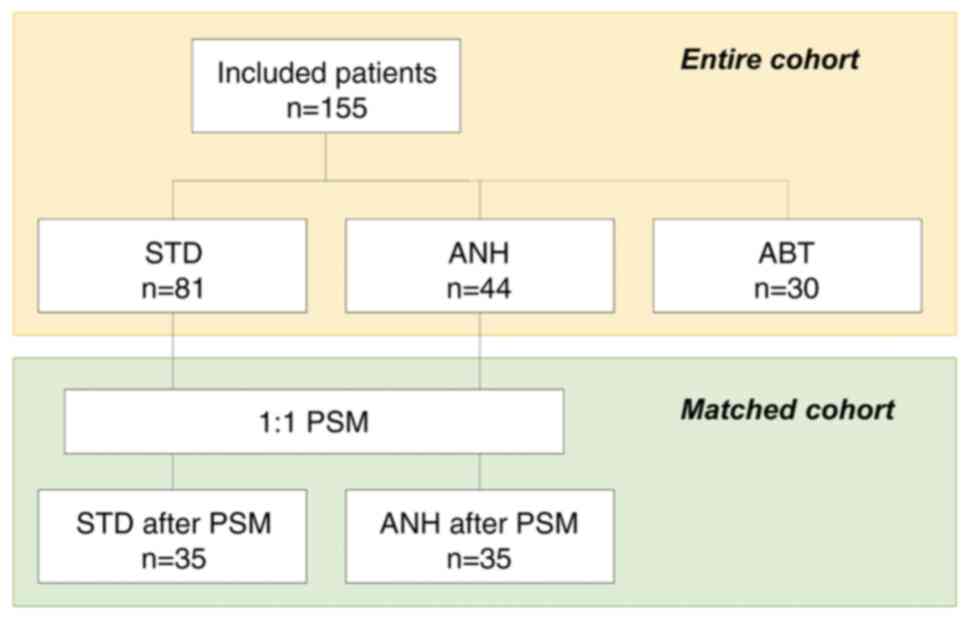
accordance with the Declaration of Helsinki. The study workflow is
shown in Fig. 1. A total of 155
patients undergoing curative pancreatic surgery for resectable PDAC
at our facility between January 2007 and May 2018 were included in
the study. A portion of the subjects in this study had been
included in our previous study (18,29).
Resectability status was made based on National Comprehensive
Cancer Network guidelines. All patients had a confirmed pathologic
diagnosis based on the 8th edition of the Union for International
Cancer Control staging system for PDAC (30). In this study, we excluded the
following cases: patients who had received neoadjuvant chemotherapy
or anyone with remnant pancreatic cancer. Baseline
clinicopathologic data were obtained from the medical records.
Patients were categorized according to whether or
not they had received intraoperative ABT. Furthermore, patients who
did not received intraoperative ABT were categorized according to
whether or not they received ANH, and then compared. In this study,
the patients who received both ANH and ABT were included in the ABT
group. The patients who received neither ANH nor ABT were included
in the standard management (STD) group. The primary analysis of
this study was a comparison of the STD and the ANH group; a
comparison of the ANH and the ABT group was performed as a
sub-analysis. A comparison of the STD and the ABT group was not
undertaken in this study because it had already been shown in
previous studies (14,18).
Surgical procedures
We selected the type of pancreatic resection based
on tumor location. Open pancreatoduodenectomy (PD) with lymph node
dissection was usually conducted on cases of pancreatic head cancer
during this study period. Reconstruction was typically done using a
modified Child's method with an end-to-side pancreaticojejunostomy
and an end-to-side choledochojejunostomy. All
pancreaticojejunostomy anastomoses were conducted using a
duct-to-mucosa technique. In cases of pancreatic body and tail
cancer, an open or minimally invasive distal pancreatectomy (DP)
was performed with lymph node dissection. If we detected swelling
paraaortic lymph nodes, we generally performed paraaortic lymph
node sampling during PD procedures whereas sampling was not
routinely done during DP surgeries. After a PD, paraaortic lymph
nodes were confirmed using standard histopathological assessment of
corresponding paraffin-embedded, hematoxylin and eosin-stained
material for surgical staging. Consequently, confirming whether or
not the paraaortic lymph nodes were positive always occurred
postoperatively. Regardless of whether there was paraaortic
swelling or the paraaortic lymph nodes ended up testing positive, a
pancreatectomy was performed in all cases. We performed a fresh
frozen section analysis to confirm whether or not the pancreatic
cut-end margin was clear of residual cancer. If residual cancer was
present at the pancreatic cut end margin, we cut the pancreas
further to reach negative margin status. If necessary, to achieve a
curative resection, we performed a total pancreatectomy with lymph
node dissection.
During this study, all surgical procedures were
carried out by board certified surgeons. We classified surgeons
into two groups in the same manner as a previous publication
(31): junior surgeons, those whose
surgical training experience was 10 years or less, and senior
surgeons, those who had over 10 years of surgical training. All
junior surgeons conducted surgeries with attending surgeons.
ANH protocol
Details of the ANH protocol are described in detail
in other papers (32). Briefly, the
principal indication for ANH at our institution is an estimated
blood loss of more than 500 ml or a request from a surgeon for a
patient with a hemoglobin (Hb) level of more than 10 g/dl. Patients
with uncontrolled congenital heart failure including active
ischemic heart disease, severe liver disease, or renal failure were
excluded. After anesthetic induction, blood was withdrawn through
the central venous line, and the withdrawn blood volume for ANH was
selected to avoid a Hb level of less than 8 g/dl after
hemodilution. The withdrawn blood volume was simultaneously
replaced with an equal volume of 6% hydroxyethyl starch solution
(130/4) (Volven; Fresenius Kabi, Bad Homburg, Germany). The blood
collected was stored in a standard blood collection pack (JMS Blood
Bag CPD400; JMS, Tokyo, Japan) at room temperature on a shaker in
the operating room. The collected blood was then reinfused into the
patients after specimen procurement.
Transfusion protocol
In the current study, intraoperative ABT was defined
as the transfusion of red blood cell concentrate during the
operation. At our institution, the intraoperative transfusion
trigger was set at Hb <7 g/dl. Additionally, for cases involving
an increased risk of ischemia, such as patients with preexisting
concomitant pulmonary disease, coronary artery disease, or cerebral
vascular disease, and those showing signs of cardiac ischemia based
on new electrocardiographic information, the transfusion threshold
was set at a Hb level of less than 9 g/dl. For the ANH group, if
the trigger point was reached, autologous blood was given first.
Allogeneic blood was used only after all autologous blood had been
reinfused and the Hb remained at less than 7 g/dl.
Definition of intraoperative blood
loss
Intraoperative blood loss was calculated based on
the in/out balance of the operative field. At our institution, any
fluid loss from the abdominal cavity including ascites, bile, and
lymphatics is considered to be intraoperative bleeding. In this
study, we estimated the circulating blood volume (CBV) using the
following formula: CBV (ml)=70 × body weight (kg).
Definition of postoperative
complications
In this study, postoperative complications were
graded using the Clavien-Dindo classification system (33). Pancreatic fistula was defined and
graded based on criteria outlined by the International Study Group
of Pancreatic Fistula (ISGPF) (34), while Delayed Gastric Emptying was
defined and graded according to criteria outlined by the
International Study Group of Pancreatic Surgery (ISGPS) (35).
Statistical analysis
Continuous variables were expressed as medians
(ranges) and analyzed using nonparametric methods for non-normally
distributed data (Mann-Whitney U-test). Categorical variables were
reported as numbers (percentages) and analyzed using the
chi-squared test or Fisher's exact test, as appropriate.
Additionally, in order to compare each group pairwise, Bonferroni
correction was applied to the Mann-Whitney U-test/chi-squared
test/Fisher's exact test (P-values were multiplied by three).
Patients in the STD and the ANH groups were classified using the
propensity score matching (PSM) method to minimize the impact of
possible selective bias in the survival analysis. Propensity scores
were based on the selected covariates, which were significantly
associated with ANH in univariate analysis (P<0.1), including
sex, age, body weight, C-reactive protein (CRP), and total
bilirubin. In addition, based on the consensus reached at expert
meetings during this study, the surgical procedure was also
included in the covariate with which propensity scores were
calculated. We did not include hemoglobin and hematocrit in the
covariate. Nearest neighbor matching was performed in a one-to-one
ratio without replacement. A caliper width of 0.08 was used to
avoid bad matches. Recurrence-free survival (RFS) and
Disease-specific survival (DSS) were calculated using the
Kaplan-Meier method, and differences in the survival rates were
compared using the log-rank test. We used Bonferroni correction for
survival analysis. RFS was defined as the time from the operation
to the date of disease recurrence. DSS was defined as the time from
the operation to the time of death due to PDAC, or the last
follow-up time. This study was planned with a maximum follow-up
period of five years. Both univariate and multivariate analyses
were conducted using Cox proportional hazards regression to
identify independent predictors of RFS and DSS, with only
significant variables from the univariate analysis included in the
multivariate analysis. In this analysis, we divided continuous
variables into two groups according to median values. A difference
was considered to be significant for values of P<0.05. The
statistical analyses were performed using IBM SPSS Statistics for
Windows, Version 26.0 (IBM Corp, Armonk, NY, USA).
Results
Comparison of the ABT rate between
patients with/without ANH
We collected a dataset from 155 resectable cases of
PDAC. First, we evaluated how much ANH reduced the need for ABT.
Among the 109 patients who did not receive ANH, eight (7.3%)
exhibited low hemoglobin levels (less than 10 g/dl) before surgery,
and 28 (25.7%) required ABT. On the other hand, of the 46 patients
who received ANH, only two patients (4.3%) needed ABT. The ABT rate
in the ANH implementation group was significantly lower than in the
non-implementation group (P=0.002). Of the total of 155 patients,
44 (28.4%) fell into the ANH group and 30 (19.4%) made up the ABT
group. Eighty-one (52.3%) patients received neither ANH nor
ABT.
Comparison of the clinicopathological
characteristics across the groups
Next, we investigated the clinical characteristics
across the groups (Table I). The
ANH group was significantly associated with higher preoperative Hb
and hematocrit levels compared to the other groups. The ANH group
had a higher mean age and showed higher CRP levels than the STD
group. Tumor biomarkers and pathological findings revealed minor
differences between the STD and the ANH groups. These data
indicated that the preoperative condition of the patients in the
ANH group was no worse than that of the STD group.
 | Table I.Comparison of clinicopathological
characteristics for the entire cohort. |
Table I.
Comparison of clinicopathological
characteristics for the entire cohort.
|
Characteristics | All (n=155) | STH (n=81) | ANH (n=44) | ABT (n=30) | P-value (STH vs.
ANH) | P-value (ANH vs.
ABT) |
|---|
| Sex, male | 79 (51.0) | 34 (42.0) | 29 (65.9) | 16 (53.3) | 0.021 | 0.553 |
| Age, years | 70 (49–85) | 71 (50–85) | 67 (49–78) | 71 (50–80) | 0.026 | 0.835 |
| Body mass index,
kg/m2 | 22.3
(14.1–36.3) | 22.0
(15.8–29.5) | 22.8
(14.1–33.3) | 24.2
(16.4–36.3) | 0.715 | 0.362 |
| ASA-PS |
|
|
|
| 0.354b | 0.415b |
|
PS2 | 126 (81.3) | 64 (79.0) | 39 (88.6) | 23 (76.7) |
|
|
|
PS3 | 29 (18.7) | 17 (21.0) | 5 (11.4) | 7 (23.3) |
|
|
| Preoperative
biliary drainage | 53 (34.2) | 22 (27.2) | 18 (40.9) | 13 (43.3) | 0.231 | >0.999 |
| Laboratory
values |
|
|
|
|
|
|
|
Hemoglobin, g/dl | 12.7
(7.2–16.5) | 12.7
(7.2–15.9) | 13.8
(10.8–16.3) | 11.6
(8.8–16.5) | 0.007 | <0.001 |
| CRP,
mg/dl | 0.12
(0.02–9.59) | 0.10
(0.02–9.59) | 0.31
(0.02–6.50) | 0.23
(0.02–4.91) | 0.010 | 0.857 |
|
Albumin, g/dl | 3.9 (2.0–5.7) | 3.9 (2.5–5.7) | 4.1 (2.4–4.9) | 3.8 (2.0–4.5) | 0.573 | 0.024 |
|
Hemoglobin A1c, % | 6.1 (4.4–12.8) | 6.1 (4.4–12.8) | 6.4 (4.4–11.9) | 5.9 (4.7–8.7) | >0.999 | 0.292 |
|
Creatinine, mg/dl | 0.67
(0.40–2.02) | 0.66
(0.43–2.02) | 0.70
(0.41–1.30) | 0.67
(0.40–1.43) | 0.636 | >0.999 |
| AST,
U/l | 29 (11–406) | 27 (13–406) | 27 (11–241) | 52 (12–260) | >0.999 | 0.051 |
| ALT,
U/l | 35 (9–627) | 25 (9–621) | 33 (12–616) | 68 (9–627) | 0.420 | 0.158 |
| Total
bilirubin, mg/dl | 0.7 (0.2–32.7) | 0.6 (0.2–32.7) | 0.8 (0.2–24.0) | 2.6 (0.3–24.1) | 0.066 | 0.391 |
| CA19-9,
U/ml | 92 (1–9,675) | 57 (1–3,199) | 118 (5–9,675) | 135 (1–6,370) | 0.345 | 0.969 |
| CEA,
ng/ml | 2.7 (0.5–37.0) | 2.8 (0.6–37.0) | 2.5 (0.5–23.9) | 3.6 (0.5–10.5) | 0.776 | 0.238 |
| Operative
variables |
|
|
|
|
|
|
|
Procedure |
|
|
|
| 0.178b | 0.044b |
|
Pancreaticoduodenectomy | 95 (61.3) | 39 (48.1) | 30 (68.2) | 26 (86.7) |
|
|
|
Distal
pancreatectomy | 52 (33.5) | 37 (45.7) | 13 (29.5) | 2 (6.7) |
|
|
|
Total
pancreatectomy | 8 (5.2) | 5 (6.2) | 1 (2.3) | 2 (6.7) |
|
|
| Portal
vein resection | 25 (16.1) | 8 (9.9) | 8 (18.2) | 9 (30.0) | 0.369 | 0.471 |
|
Grouping of surgeons |
|
|
|
|
>0.999b | 0.890b |
|
Junior
surgeon | 10 (6.5) | 6 (7.4) | 1 (2.3) | 3 (10.0) |
|
|
|
Senior
surgeon | 145 (93.5) | 75 (92.6) | 43 (97.7) | 27 (90.0) |
|
|
| Pathology |
|
|
|
|
|
|
| Tumor
size, mm | 30 (7–150) | 29 (7–150) | 33 (10–130) | 35 (15–57) | 0.753 | >0.999 |
| UICC
8th edition |
|
|
|
|
|
|
|
T category |
|
|
|
| 0.726b | 0.620b |
|
T1 | 20 (12.9) | 10 (12.3) | 8 (18.2) | 2 (6.7) |
|
|
|
T2 | 92 (59.4) | 51 (63.0) | 22 (50.0) | 19 (63.3) |
|
|
|
T3 | 43 (27.7) | 20 (24.7) | 14 (31.8) | 9 (30.0) |
|
|
|
T4 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
|
|
|
N category |
|
|
|
| 0.473 | 0.749 |
|
N0 | 62 (40.0) | 38 (46.9) | 17 (38.6) | 7 (23.3) |
|
|
|
N1 | 58 (37.4) | 31 (38.3) | 15 (34.1) | 12 (40.0) |
|
|
|
N2 | 35 (22.6) | 12 (14.8) | 12 (27.3) | 11 (36.7) |
|
|
|
M category |
|
|
|
| 0.065b | 0.263b |
|
M0 | 144 (92.9) | 78 (96.3) | 37 (84.1) | 29 (96.7) |
|
|
|
M1a | 11 (7.1) | 3 (3.7) | 7 (15.9) | 1 (3.3) |
|
|
|
UICC stage |
|
|
|
| 0.018b | 0.179b |
|
IA | 12 (7.7) | 6 (7.4) | 5 (11.4) | 1 (3.3) |
|
|
|
IB | 24 (15.5) | 17 (21.0) | 3 (6.8) | 4 (13.3) |
|
|
|
IIA | 12 (7.7) | 4 (4.9) | 7 (15.9) | 1 (3.3) |
|
|
|
IIB | 72 (46.5) | 41 (50.6) | 15 (34.1) | 16 (53.3) |
|
|
|
III | 24 (15.5) | 10 (12.3) | 7 (15.9) | 7 (23.3) |
|
|
|
IV | 11 (87.1) | 3 (3.7) | 7 (15.9) | 1 (3.3) |
|
|
| R0 resection | 141 (91.0) | 75 (92.6) | 38 (86.4) | 28 (93.3) | 0.683 | 0.921 |
Comparison of the operative and
postoperative outcomes across the groups
There was a trend toward a higher proportion of
distal pancreatectomy in the STD group than in the ANH group (45.7%
vs. 29.5%, P=0.157) (Table II). In
comparison with the STD group, one of the key features of the ANH
group was longer operation time (250 vs. 346 min, P<0.001) and
anesthesia time (317 vs. 405 min, P<0.001), with more
intraoperative blood loss (420 vs. 983 ml, P<0.001) and a higher
volume of intraoperative fluids administered (2,850 vs. 4,975 ml,
P<0.001). When we evaluated the intraoperative in-out balance by
correcting for body weight and anesthesia time, we found no
difference between the two groups.
| Table II.Comparison of operative and
postoperative outcomes for the entire cohort. |
Table II.
Comparison of operative and
postoperative outcomes for the entire cohort.
| Outcomes | All (n=155) | STH (n=81) | ANH (n=44) | ABT (n=30) | P-value (STH vs.
ANH) | P-value (ANH vs.
ABT) |
|---|
| Operative
results |
|
|
|
|
|
|
|
Operation time, min | 307 (91–647) | 250 (91–619) | 346 (129–587) | 368 (127–647) | <0.001 | 0.206 |
|
Anesthesia time, min | 372 (172–757) | 317 (172–676) | 405 (187–680) | 429 (209–757) | <0.001 | 0.327 |
|
Intraoperative blood loss,
ml | 750 (50–5,600) | 420 (50–2,400) | 983 (150–2,775) | 1,940 (540–5,600) | <0.001 | <0.001 |
|
Intraoperative blood loss,
ml/kg | 14.1
(0.8–77.6) | 7.9 (0.8–42.6) | 18.3
(2.3–39.0) | 29.5
(13.9–77.6) | <0.001 | <0.001 |
| IBL
>20% in CBV | 78 (50.3) | 20 (24.7) | 29 (65.9) | 29 (96.7) | <0.001 | 0.003 |
| Blood
volume removed, ml | 0 (0–800) | 0 (0–0) | 800 (400–800) | 0 (0–800) | <0.001 | <0.001 |
|
Intraoperative fluid | 3,600
(200–9,000) | 2,850 | 4,150 | 4,688 | <0.001 | >0.999 |
| given,
ml |
| (1,300–7,500) | (2,500–7,300) | (200–9,000) |
|
|
|
Intraoperative albumin,
ml | 0 (0–1,250) | 0 (0–500) | 0 (0–1,000) | 500 (0–1,250) | 0.001 | <0.001 |
|
Intraoperative RBC, ml | 0 (0–1,400) | 0 (0–0) | 0 (0–0) | 560 (80–1,400) | - | <0.001 |
|
Intraoperative FFP, ml | 0 (0–960) | 0 (0–480) | 0 (0–0) | 0 (0–960) | >0.999 | <0.001 |
|
Intraoperative PC, ml | 0 (0–200) | 0 (0–0) | 0 (0–0) | 0 (0–200) | - | 0.169 |
| Total
fluid volume | 3,900 | 2,850 | 4,975 | 5,885 | <0.001 | 0.411 |
|
administered, ml | (1,300–11,510) | (1,300–8,000) | (2,950–8,850) | (2,530–11,510) |
|
|
|
Intraoperative urine output,
ml | 480 (20–3,800) | 420 (56–1,550) | 545 (20–1,750) | 598 (70–3,800) | 0.080 | >0.999 |
| Total
in-out balance, ml | 2,300 | 1,880 | 2,735 | 3,072 | <0.001 | >0.999 |
| Total
in-out balance, | (410–7,714) | (485–5,500) | (1,190–4,700) | (410–7,714) |
|
|
|
ml/kg/ha | 6.7 (1.2–13.9) | 6.4 (1.8–12.4) | 6.7 (3.2–13.9) | 7.2 (1.2–13.7) | 0.627 | >0.999 |
| Postoperative
results |
|
|
|
|
|
|
|
Postoperative complications
(Clavien-Dindo classification grade ≥3) | 27 (17.4) | 6 (7.4) | 11 (25.0) | 10 (33.3) | 0.012 | 0.870 |
|
Pancreatic fistula | 24 (15.5) | 7 (8.6) | 9 (20.4) | 8 (26.7) | 0.118 | >0.999 |
| (ISGPF
grade ≥B) |
|
|
|
|
|
|
| Delayed
gastric emptying | 17 (11.0) | 7 (8.6) | 6 (13.6) | 4 (13.3) | 0.756 |
>0.999b |
| (ISGPS
grade ≥B) |
|
|
|
|
|
|
|
Postoperative hospital | 19 (6–73) | 17 (7–73) | 22 (6–64) | 31 (10–57) | 0.007 | 0.585 |
| stay,
days |
|
|
|
|
|
|
| 90-day
mortality | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - |
|
Adjuvant chemotherapy | 122 (80.3) | 64 (80.0) | 34 (79.1) | 24 (82.8) | >0.999 | >0.999 |
Regarding the postoperative short-term outcomes, the
ANH group displayed a higher frequency of postoperative
complications (Clavien-Dindo grade ≥3, 3.4-fold, P=0.012) compared
to the STD group. Specifically, there were more clinically relevant
postoperative pancreatic fistulas in the ANH group (2.4-fold,
P=0.118). Moreover, the ANH groups experienced longer postoperative
hospital stays (P=0.007). There was no in-hospital or 90-day
mortality for any patients in this study. In short, postoperative
short-term outcomes in the ANH group were less favorable than those
in the STD group, but not as poor as that of the ABT group.
Comparison of the survival outcomes of
the entire cohort
The groups were well matched in the proportion of
adjuvant chemotherapy (Table II).
The median follow-up period was 30.7 months (range: 4.2–60.0). A
total of 117 patients (75.5%) had recurrences. The median RFS time
was 13.0 months for the entire cohort. A total of 101 patients
(65.2%) died due to the primary disease during the follow-up
period. The median DSS time was 32.1 months for the entire cohort.
The RFS and DSS curves for patients classified as requiring
intraoperative blood management are shown in Fig. 2A and B. The RFS time was
significantly shorter in the ANH group than in the STD group
(median survival time (MST), 11.1 vs. 16.5 months, P=0.043 before
correction). Likewise, the DSS was significantly shorter in the ANH
group (MST, 28.6 vs. 41.6 months, P=0.029 before correction).
However, these differences were not significant after Bonferroni
correction (RFS, P=0.129; DSS, P=0.087). In the comparison between
ANH and ABT, RFS was not significantly different between the two
groups (MST, 11.1 vs. 9.5 months, P=0.143, before applying
Bonferroni correction; P=0.429, after correction). The ANH group
showed a longer DSS time than the ABT group, but it was not
significant (MST, 28.6 vs. 19.7 months, P=0.136, before applying
Bonferroni correction; P=0.408, after correction). Taken together,
these data suggest that ANH has a negative impact on the
postoperative long-term outcomes in PDAC, though not as severe as
ABT.
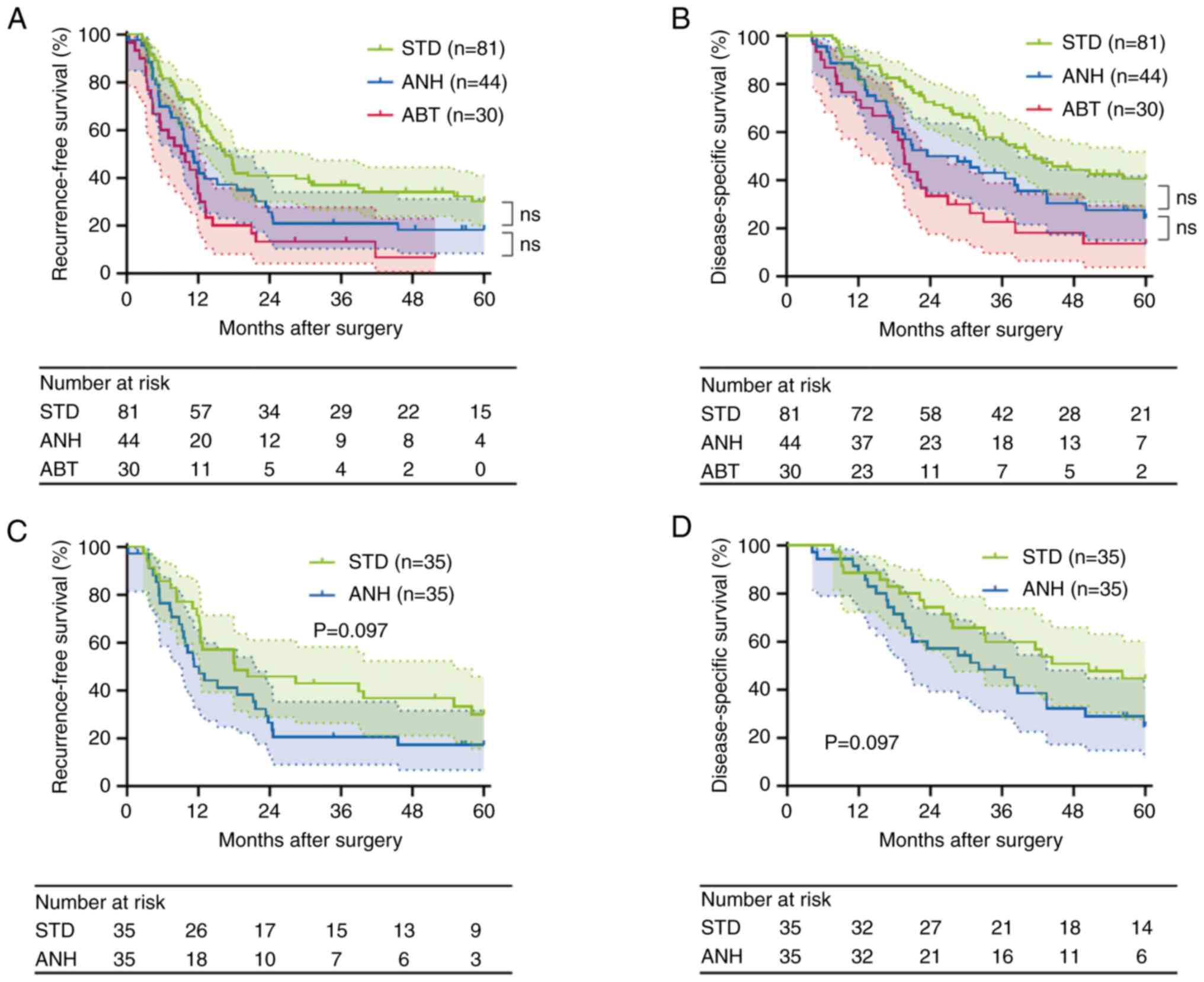 | Figure 2.Survival analysis. (A and B) Survival
cures of the STD, ANH and ABT groups for the entire cohort. (A)
Recurrence-free survival (STD vs. ANH, P=0.043; ANH vs. ABT,
P=0.143; log-rank test, before applying Bonferroni correction;
after correction: STD vs. ANH, P=0.129; ANH vs. ABT, P=0.429). (B)
Disease-specific survival (STD vs. ANH, P=0.029; ANH vs. ABT,
P=0.136; log-rank test, before applying Bonferroni correction;
after correction: STD vs. ANH, P=0.087; ANH vs. ABT, P=0.408). (C
and D) Survival cures of the STD and ANH groups in the propensity
score-matched cohort. (C) Recurrence-free survival (P=0.097;
log-rank test). (D) Disease-specific survival (P=0.097; log-rank
test). ABT, allogeneic blood transfusion; ANH, acute normovolemic
hemodilution; ns, not significant; STD, standard management. |
Clinicopathological characteristics
influencing RFS and DSS of the STD and ANH groups
To assess whether ANH influences RFS and DSS in
PDAC, we further performed Cox regression analysis. Since red blood
cell transfusion has been shown to affect cancer prognosis
negatively (18), we evaluated the
clinicopathological factors influencing RFS and DSS in subjects,
excluding the ABT group. In univariate analysis, significant
predictors of decreased RFS were preoperative CRP, preoperative
aspartate aminotransferase, preoperative carbohydrate antigen 19-9
(CA19-9), tumor size, Union for International Cancer Control (UICC)
T category, UICC N category, ANH, and adjuvant chemotherapy. In
multivariate analysis, preoperative CA19-9≥68 U/ml (relative risk
(RR)=1.796 (95% confidence interval (CI), 1.124–2.871), P=0.014),
UICC N1-2 (RR=2.207 (95% CI, 1.339–3.638), P=0.002), ANH (RR=1.696
(95% CI, 1.091–2.636), P=0.019), and adjuvant chemotherapy
(RR=0.345 (95% CI, 0.204–0.584), were independent prognostic
factors for RFS (Table III).
| Table III.Clinicopathological characteristics
predicting RFS in the standard management and ANH groups. |
Table III.
Clinicopathological characteristics
predicting RFS in the standard management and ANH groups.
|
|
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|
|---|
|
Characteristics | No. | 5-year RFS, % | MST, months | RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| Sex |
|
|
| 0.766 | 0.505–1.162 | 0.235 |
|
|
|
|
Male | 63 | 24.9 | 12.4 |
|
|
|
|
|
|
|
Female | 62 | 27.6 | 16.5 |
|
|
|
|
|
|
| Age, years |
|
|
| 1.210 | 0.800–1.831 | 0.365 |
|
|
|
|
<70 | 65 | 28.1 | 17.9 |
|
|
|
|
|
|
|
≥70 | 60 | 23.7 | 13.0 |
|
|
|
|
|
|
| Body mass index,
kg/m2 |
|
|
| 1.019 | 0.674–1.541 | 0.871 |
|
|
|
|
<22.1 | 62 | 28.3 | 14.2 |
|
|
|
|
|
|
|
≥22.1 | 63 | 24.2 | 15.2 |
|
|
|
|
|
|
| Preoperative
biliary drainage |
|
|
| 1.148 | 0.737–1.788 | 0.540 |
|
|
|
| No | 85 | 26.7 | 15.8 |
|
|
|
|
|
|
|
Yes | 40 | 25.6 | 12.4 |
|
|
|
|
|
|
| Hemoglobin,
g/dl |
|
|
| 1.088 | 0.719–1.647 | 0.689 |
|
|
|
|
<12.9 | 65 | 25.0 | 15.8 |
|
|
|
|
|
|
|
≥12.9 | 60 | 28.8 | 12.4 |
|
|
|
|
|
|
| CRP, mg/dl |
|
|
| 1.613 | 1.050–2.478 | 0.022 | 0.982 | 0.619–1.556 | 0.937 |
|
<0.11 | 60 | 35.5 | 21.6 |
|
|
|
|
|
|
|
≥0.11 | 65 | 17.4 | 12.7 |
|
|
|
|
|
|
| Albumin, g/dl |
|
|
| 1.013 | 0.670–1.534 | 0.933 |
|
|
|
|
<3.9 | 64 | 22.2 | 15.7 |
|
|
|
|
|
|
|
≥3.9 | 61 | 30.2 | 14.2 |
|
|
|
|
|
|
| Hemoglobin A1c,
% |
|
|
| 1.240 | 0.799–1.924 | 0.477 |
|
|
|
|
<6.0 | 58 | 25.2 | 13.0 |
|
|
|
|
|
|
|
≥6.0 | 55 | 10.3 | 12.7 |
|
|
|
|
|
|
| Creatinine,
mg/dl |
|
|
| 0.822 | 0.542–1.247 | 0.356 |
|
|
|
|
<0.67 | 66 | 21.6 | 13.4 |
|
|
|
|
|
|
|
≥0.67 | 59 | 31.6 | 17.5 |
|
|
|
|
|
|
| AST, U/l |
|
|
| 1.775 | 1.168–2.700 | 0.006 | 1.108 | 0.669–1.834 | 0.691 |
|
<27 | 64 | 36.3 | 21.2 |
|
|
|
|
|
|
|
≥27 | 61 | 15.4 | 12.1 |
|
|
|
|
|
|
| ALT, U/l |
|
|
| 1.420 | 0.937–2.152 | 0.096 |
|
|
|
|
<28 | 63 | 32.4 | 17.7 |
|
|
|
|
|
|
|
≥28 | 62 | 19.6 | 12.4 |
|
|
|
|
|
|
| Total bilirubin,
mg/dl |
|
|
| 1.135 | 0.749–1.720 | 0.551 |
|
|
|
|
<0.7 | 67 | 24.8 | 17.5 |
|
|
|
|
|
|
|
≥0.7 | 58 | 27.1 | 12.3 |
|
|
|
|
|
|
| CA19-9, U/ml |
|
|
| 1.897 | 1.250–2.880 | 0.002 | 1.796 | 1.124–2.871 | 0.014 |
|
<68 | 63 | 35.1 | 21.6 |
|
|
|
|
|
|
|
≥68 | 62 | 17.4 | 11.2 |
|
|
|
|
|
|
| CEA, ng/ml |
|
|
| 1.316 | 0.870–1.990 | 0.192 |
|
|
|
|
<2.7 | 67 | 30.2 | 16.5 |
|
|
|
|
|
|
|
≥2.7 | 58 | 21.7 | 13.4 |
|
|
|
|
|
|
| Tumor size, mm |
|
|
| 1.807 | 1.193–2.737 | 0.005 | 1.229 | 0.777–1.944 | 0.379 |
|
<30 | 71 | 33.5 | 17.9 |
|
|
|
|
|
|
|
≥30 | 54 | 16.2 | 9.8 |
|
|
|
|
|
|
| UICC T
category |
|
|
| 3.300 | 1.522–7.154 | 0.001 | 2.026 | 0.864–4.750 | 0.104 |
| T1 | 18 | 58.3 | 42.8 |
|
|
|
|
|
|
|
T2-3 | 107 | 20.7 | 12.4 |
|
|
|
|
|
|
| UICC N
category |
|
|
| 2.552 | 1.635–3.983 | <0.001 | 2.207 | 1.339–3.638 | 0.002 |
| N0 | 55 | 43.9 | 39.8 |
|
|
|
|
|
|
|
N1-2 | 70 | 12.1 | 12.3 |
|
|
|
|
|
|
| UICC M
category |
|
|
| 1.804 | 0.903–3.607 | 0.090 |
|
|
|
| M0 | 115 | 27.5 | 15.2 |
|
|
|
|
|
|
|
M1a | 10 | 10.0 | 8.3 |
|
|
|
|
|
|
| R0 resection |
|
|
| 0.787 | 0.380–1.628 | 0.831 |
|
|
|
| No | 12 | 33.3 | 13.0 |
|
|
|
|
|
|
|
Yes | 113 | 25.4 | 14.5 |
|
|
|
|
|
|
| Procedure |
|
|
| 0.878 | 0.573–1.345 | 0.550 |
|
|
|
| PD,
TP | 75 | 22.4 | 13.6 |
|
|
|
|
|
|
| DP | 50 | 31.7 | 15.7 |
|
|
|
|
|
|
| Portal vein
resection |
|
|
| 1.235 | 0.686–2.225 | 0.480 |
|
|
|
| No | 109 | 28.2 | 14.5 |
|
|
|
|
|
|
|
Yes | 16 | 0.0 | 13.6 |
|
|
|
|
|
|
| Operation time,
min |
|
|
| 1.420 | 0.938–2.150 | 0.096 |
|
|
|
|
<275 | 63 | 33.3 | 17.5 |
|
|
|
|
|
|
|
≥275 | 62 | 17.4 | 12.4 |
|
|
|
|
|
|
| Anesthesia time,
min |
|
|
| 1.182 | 0.782–1.789 | 0.427 |
|
|
|
|
<363 | 63 | 30.6 | 15.8 |
|
|
|
|
|
|
|
≥363 | 62 | 20.6 | 12.4 |
|
|
|
|
|
|
| Intraoperative
blood loss, ml |
|
|
| 1.330 | 0.876–2.018 | 0.179 |
|
|
|
|
<600 | 63 | 34.3 | 15.1 |
|
|
|
|
|
|
|
≥600 | 62 | 17.9 | 14.2 |
|
|
|
|
|
|
| ANH |
|
|
| 1.545 | 1.010–2.364 | 0.043 | 1.696 | 1.091–2.636 | 0.019 |
| No | 81 | 30.3 | 16.5 |
|
|
|
|
|
|
|
Yes | 44 | 18.3 | 11.1 |
|
|
|
|
|
|
| Intraoperative
fluid given, ml |
|
| 0.951 | 0.627–1.441 | 0.812 |
|
|
|
|
|
<3,500 | 68 | 26.9 | 14.2 |
|
|
|
|
|
|
|
≥3,500 | 57 | 24.3 | 17.9 |
|
|
|
|
|
|
| Intraoperative
urine output, ml |
|
|
| 1.262 | 0.834–1.910 | 0.269 |
|
|
|
|
<465 | 64 | 29.6 | 16.5 |
|
|
|
|
|
|
|
≥465 | 61 | 22.2 | 12.7 |
|
|
|
|
|
|
| Total in-out
balance, ml |
|
|
| 1.067 | 0.705–1.615 | 0.759 |
|
|
|
|
<2,210 | 63 | 27.0 | 15.7 |
|
|
|
|
|
|
|
≥2,210 | 62 | 24.6 | 13.4 |
|
|
|
|
|
|
| Total in-out
balance, ml/kg/h |
|
|
| 1.354 | 0.894–2.048 | 0.213 |
|
|
|
|
<6.6 | 62 | 28.5 | 17.5 |
|
|
|
|
|
|
|
≥6.6 | 63 | 23.7 | 11.3 |
|
|
|
|
|
|
| Postoperative
complications |
|
|
| 1.302 | 0.723–2.346 | 0.377 |
|
|
|
|
Clavien-Dindo grade 0–2 | 108 | 26.5 | 15.7 |
|
|
|
|
|
|
|
Clavien-Dindo grade ≥3 | 17 | 23.5 | 12.1 |
|
|
|
|
|
|
| Pancreatic
fistula |
|
|
| 1.270 | 0.691–2.333 | 0.440 |
|
|
|
| ISGPF
grade non-A | 109 | 26.2 | 15.1 |
|
|
|
|
|
|
| ISGPF
grade B-C | 16 | 25.0 | 12.1 |
|
|
|
|
|
|
| Postoperative
hospital stay, days |
|
|
| 1.104 | 0.730–1.669 | 0.640 |
|
|
|
|
<17 | 64 | 26.6 | 15.7 |
|
|
|
|
|
|
|
≥17 | 61 | 25.2 | 13.0 |
|
|
|
|
|
|
| Adjuvant
chemotherapy |
|
|
| 0.535 | 0.332–0.862 | 0.003 | 0.345 | 0.204–0.584 | <0.001 |
| No | 27 | 8.0 | 9.3 |
|
|
|
|
|
|
|
Yes | 98 | 30.5 | 16.5 |
|
|
|
|
|
|
Likewise, in univariate analysis, significant
predictors of decreased DSS were preoperative CRP, preoperative
aspartate aminotransferase, UICC T category, UICC N category, ANH,
and adjuvant chemotherapy. In multivariate analysis, UICC T2-3
(RR=3.045 (95% CI, 1.071–8.657), P=0.037), UICC N1-2 (RR=2.225 (95%
CI, 1.275–3.883), P=0.005), ANH (RR=1.876 (95% CI, 1.174–2.998),
P=0.009), and adjuvant chemotherapy (RR=0.268 (95% CI,
0.151–0.477), P<0.001) were independent prognostic factors for
DSS (Table IV). These results
provide us with a warning that ANH falls in the poor prognostic
factor category with regard to the management of resectable
PDAC.
| Table IV.Clinicopathological characteristics
predicting DSS in the standard management and ANH groups. |
Table IV.
Clinicopathological characteristics
predicting DSS in the standard management and ANH groups.
|
|
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|
|
|---|
|
Characteristics | No. | 5-year DSS, % | MST, months | RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| Sex |
|
|
| 0.645 | 0.408–1.020 | 0.070 |
|
|
|
|
Male | 63 | 28.8 | 32.1 |
|
|
|
|
|
|
|
Female | 62 | 41.6 | 40.0 |
|
|
|
|
|
|
| Age, years |
|
|
| 1.427 | 0.908–2.242 | 0.121 |
|
|
|
|
<70 | 65 | 42.0 | 42.6 |
|
|
|
|
|
|
|
≥70 | 60 | 27.1 | 32.2 |
|
|
|
|
|
|
| Body mass index,
kg/m2 |
|
|
| 0.920 | 0.586–1.442 | 0.811 |
|
|
|
|
<22.1 | 62 | 36.0 | 33.2 |
|
|
|
|
|
|
|
≥22.1 | 63 | 33.9 | 42.6 |
|
|
|
|
|
|
| Preoperative
biliary drainage |
|
|
| 1.418 | 0.889–2.263 | 0.141 |
|
|
|
| No | 85 | 39.1 | 38.6 |
|
|
|
|
|
|
|
Yes | 40 | 25.5 | 28.6 |
|
|
|
|
|
|
| Hemoglobin,
g/dl |
|
|
| 0.957 | 0.609–1.505 | 0.850 |
|
|
|
|
<12.9 | 65 | 33.7 | 36.5 |
|
|
|
|
|
|
|
≥12.9 | 60 | 35.9 | 38.6 |
|
|
|
|
|
|
| CRP, mg/dl |
|
|
| 1.617 | 1.013–2.581 | 0.025 | 0.931 | 0.566–1.532 | 0.779 |
|
<0.11 | 60 | 44.8 | 50.0 |
|
|
|
|
|
|
|
≥0.11 | 65 | 24.2 | 32.2 |
|
|
|
|
|
|
| Albumin, g/dl |
|
|
| 1.063 | 0.677–1.668 | 0.913 |
|
|
|
|
<3.9 | 64 | 32.7 | 38.6 |
|
|
|
|
|
|
|
≥3.9 | 61 | 37.2 | 36.5 |
|
|
|
|
|
|
| Hemoglobin A1c,
% |
|
|
| 1.134 | 0.703–1.832 | 0.254 |
|
|
|
|
<6.0 | 58 | 41.6 | 42.6 |
|
|
|
|
|
|
|
≥6.0 | 55 | 28.7 | 33.2 |
|
|
|
|
|
|
| Creatinine,
mg/dl |
|
|
| 0.891 | 0.567–1.400 | 0.616 |
|
|
|
|
<0.67 | 66 | 30.2 | 38.1 |
|
|
|
|
|
|
|
≥0.67 | 59 | 40.0 | 36.5 |
|
|
|
|
|
|
| AST, U/l |
|
|
| 1.609 | 1.023–2.531 | 0.038 | 1.422 | 0.831–2.434 | 0.119 |
|
<27 | 64 | 42.0 | 43.5 |
|
|
|
|
|
|
|
≥27 | 61 | 26.9 | 29.4 |
|
|
|
|
|
|
| ALT, U/l |
|
|
| 1.349 | 0.859–2.119 | 0.192 |
|
|
|
|
<28 | 63 | 40.0 | 41.6 |
|
|
|
|
|
|
|
≥28 | 62 | 29.5 | 32.2 |
|
|
|
|
|
|
| Total bilirubin,
mg/dl |
|
|
| 1.236 | 0.788–1.939 | 0.355 |
|
|
|
|
<0.7 | 67 | 35.7 | 40.0 |
|
|
|
|
|
|
|
≥0.7 | 58 | 33.1 | 32.2 |
|
|
|
|
|
|
| CA19-9, U/ml |
|
|
| 1.524 | 0.970–2.395 | 0.066 |
|
|
|
|
<68 | 63 | 40.4 | 42.6 |
|
|
|
|
|
|
|
≥68 | 62 | 29.4 | 31.4 |
|
|
|
|
|
|
| CEA, ng/ml |
|
|
| 1.418 | 0.904–2.224 | 0.126 |
|
|
|
|
<2.7 | 67 | 40.2 | 40.0 |
|
|
|
|
|
|
|
≥2.7 | 58 | 28.2 | 31.4 |
|
|
|
|
|
|
| Tumor size, mm |
|
|
| 1.499 | 0.955–2.352 | 0.076 |
|
|
|
|
<30 | 71 | 41.6 | 38.1 |
|
|
|
|
|
|
|
≥30 | 54 | 26.0 | 36.5 |
|
|
|
|
|
|
| UICC T
category |
|
|
| 4.570 | 1.667–12.530 | 0.001 | 3.045 | 1.071–8.657 | 0.037 |
| T1 | 18 | 73.8 | 53.0 |
|
|
|
|
|
|
|
T2-3 | 107 | 28.4 | 32.1 |
|
|
|
|
|
|
| UICC N
category |
|
|
| 2.245 | 1.387–3.634 | 0.001 | 2.225 | 1.275–3.883 | 0.005 |
| N0 | 55 | 52.1 | 42.8 |
|
|
|
|
|
|
|
N1-2 | 70 | 20.8 | 28.6 |
|
|
|
|
|
|
| UICC M
category |
|
|
| 1.521 | 0.758–3.051 | 0.235 |
|
|
|
| M0 | 115 | 37.8 | 38.1 |
|
|
|
|
|
|
|
M1a | 10 | 0 | 30.8 |
|
|
|
|
|
|
| R0 resection |
|
|
| 1.239 | 0.595–2.578 | 0.278 |
|
|
|
| No | 12 | 31.3 | 21.0 |
|
|
|
|
|
|
|
Yes | 113 | 35.3 | 38.3 |
|
|
|
|
|
|
| Procedure |
|
|
| 0.829 | 0.520–1.322 | 0.430 |
|
|
|
| PD,
TP | 75 | 31.6 | 36.1 |
|
|
|
|
|
|
| DP | 50 | 39.6 | 38.6 |
|
|
|
|
|
|
| Portal vein
resection |
|
|
| 1.015 | 0.487–2.112 | 0.969 |
|
|
|
| No | 109 | 34.0 | 38.1 |
|
|
|
|
|
|
|
Yes | 16 | 44.4 | 33.0 |
|
|
|
|
|
|
| Operation time,
min |
|
|
| 1.357 | 0.864–2.129 | 0.183 |
|
|
|
|
<275 | 63 | 39.5 | 40.4 |
|
|
|
|
|
|
|
≥275 | 62 | 29.6 | 33.0 |
|
|
|
|
|
|
| Anesthesia time,
min |
|
|
| 1.131 | 0.721–1.774 | 0.591 |
|
|
|
|
<363 | 63 | 37.5 | 38.3 |
|
|
|
|
|
|
|
≥363 | 62 | 31.8 | 36.5 |
|
|
|
|
|
|
| Intraoperative
blood loss, ml |
|
|
| 1.180 | 0.752–1.851 | 0.471 |
|
|
|
|
<600 | 63 | 37.8 | 38.6 |
|
|
|
|
|
|
|
≥600 | 62 | 31.8 | 36.5 |
|
|
|
|
|
|
| ANH |
|
|
| 1.651 | 1.046–2.605 | 0.029 | 1.876 | 1.174–2.998 | 0.009 |
| No | 81 | 40.6 | 41.6 |
|
|
|
|
|
|
|
Yes | 44 | 24.1 | 23.5 |
|
|
|
|
|
|
| Intraoperative
fluid given, ml |
|
|
| 1.017 | 0.647–1.600 | 0.941 |
|
|
|
|
<3,500 | 68 | 33.1 | 36.7 |
|
|
|
|
|
|
|
≥3,500 | 57 | 36.7 | 36.5 |
|
|
|
|
|
|
| Intraoperative
urine output, ml |
|
|
| 1.461 | 0.930–2.295 | 0.098 |
|
|
|
|
<465 | 64 | 40.8 | 42.6 |
|
|
|
|
|
|
|
≥465 | 61 | 27.9 | 33.2 |
|
|
|
|
|
|
| Total in-out
balance, ml |
|
|
| 1.174 | 0.748–1.842 | 0.484 |
|
|
|
|
<2,210 | 63 | 35.0 | 40.0 |
|
|
|
|
|
|
|
≥2,210 | 62 | 34.8 | 36.1 |
|
|
|
|
|
|
| Total in-out
balance, ml/kg/h |
|
|
| 1.405 | 0.895–2.204 | 0.260 |
|
|
|
|
<6.6 | 62 | 37.2 | 40.4 |
|
|
|
|
|
|
|
≥6.6 | 63 | 32.6 | 33.0 |
|
|
|
|
|
|
| Postoperative
complications |
|
|
| 1.440 | 0.792–2.620 | 0.229 |
|
|
|
|
Clavien-Dindo grade 0–2 | 108 | 37.7 | 36.7 |
|
|
|
|
|
|
|
Clavien-Dindo grade ≥3 | 17 | 19.9 | 43.5 |
|
|
|
|
|
|
| Pancreatic
fistula |
|
|
| 1.421 | 0.767–2.635 | 0.262 |
|
|
|
| ISGPF
grade non-A | 109 | 37.2 | 36.7 |
|
|
|
|
|
|
| ISGPF
grade B-C | 16 | 21.4 | 21.2 |
|
|
|
|
|
|
| Postoperative
hospital stay, days |
|
|
| 1.201 | 0.765–1.885 | 0.425 |
|
|
|
|
<17 | 64 | 39.8 | 38.1 |
|
|
|
|
|
|
|
≥17 | 61 | 29.9 | 36.5 |
|
|
|
|
|
|
| Adjuvant
chemotherapy |
|
|
| 0.407 | 0.247–0.671 | <0.001 | 0.268 | 0.151–0.477 | <0.001 |
| No | 27 | 9.1 | 20.8 |
|
|
|
|
|
|
|
Yes | 98 | 41.2 | 42.6 |
|
|
|
|
|
|
Propensity score matching
analysis
To reduce confounding biases and confirm the
influence of ANH, we further performed PSM analysis between the STD
and the ANH groups. After one-to-one PSM, 35 pairs of patients were
included in further analysis. The comparison of the
clinicopathological characteristics between the STD group and the
ANH group, after matching, is shown in Table V. After PSM, the ANH group showed a
longer operation time (327 vs. 261 min, P=0.042), with more
intraoperative blood loss (970 vs. 570 ml, P<0.001) compared to
the STD group. The ANH group was also administered a higher volume
of intraoperative fluids (4,850 vs. 3,200 ml, P<0.001) and
showed more intraoperative in-out balance than the STD group.
However, after correcting the balance by body weight and anesthesia
time, there was no difference between the two groups (Table VI).
| Table V.Comparison of clinicopathological
characteristics after propensity score matching. |
Table V.
Comparison of clinicopathological
characteristics after propensity score matching.
|
Characteristics | Post-match all
(n=70) | STH (n=35) | ANH (n=35) | P-value | ASD |
|---|
| Sex, male | 40 (57.1) | 19 (54.3) | 21 (60.0) | 0.629 | 0.116 |
| Age, years | 69 (49–85) | 69 (52–85) | 69 (49–78) | 0.668 | 0.146 |
| Body mass index,
kg/m2 | 22.3
(14.1–33.3) | 22.0
(18.8–28.4) | 22.5
(14.1–33.3) | 0.729 | 0.074 |
| ASA-PS |
|
|
| 0.324b | 0.237 |
|
PS2 | 59 (84.3) | 28 (80.0) | 31 (88.6) |
|
|
|
PS3 | 11 (15.7) | 7 (20.0) | 4 (11.4) |
|
|
| Preoperative
biliary drainage | 32 (45.7) | 17 (48.6) | 15 (42.9) | 0.631 | 0.115 |
| Laboratory
values |
|
|
|
|
|
|
Hemoglobin, g/dl | 12.9
(8.8–16.3) | 12.5
(8.8–15.6) | 13.6
(10.8–16.3) | 0.011 | 0.675 |
| CRP,
mg/dl | 0.20
(0.02–9.59) | 0.16
(0.02–9.59) | 0.27
(0.02–5.45) | 0.375 | 0.068 |
|
Albumin, g/dl | 3.9 (2.4–5.0) | 3.8 (2.5–5.0) | 4.0 (2.4–4.9) | 0.110 | 0.193 |
|
Hemoglobin A1c, % | 5.8 (4.4–11.8) | 5.8 (4.4–11.8) | 6.2 (4.4–9.0) | 0.273 | 0.227 |
|
Creatinine, mg/dl | 0.67
(0.41–1.30) | 0.67
(0.43–1.21) | 0.66
(0.41–1.30) | 0.934 | 0.073 |
| AST,
U/l | 32 (14–406) | 36 (14–406) | 27 (16–241) | 0.526 | 0.131 |
| ALT,
U/l | 45 (12–621) | 51 (12–621) | 35 (12–616) | 0.991 | 0.105 |
| Total
bilirubin, mg/dl | 0.8 (0.2–32.7) | 0.8 (0.3–32.7) | 0.9 (0.2–24.0) | 0.684 | 0.093 |
| CA19-9,
U/ml | 73 (1–9,675) | 60 (1–3,199) | 112 (5–9,675) | 0.277 | 0.279 |
| CEA,
ng/ml | 2.5 (0.5–37.0) | 2.7 (0.7–37.0) | 2.4 (0.5–23.9) | 0.577 | 0.002 |
| Operative
variables |
|
|
|
|
|
|
Procedure |
|
|
| 0.568b | 0.256 |
|
Pancreaticoduodenectomy | 50 (71.4) | 26 (74.3) | 24 (68.6) |
|
|
|
Distal
pancreatectomy | 19 (27.1) | 9 (25.7) | 10 (28.6) |
|
|
|
Total
pancreatectomy | 1 (1.4) | 0 (0.0) | 1 (2.9) |
|
|
| Portal
vein resection | 9 (12.9) | 4 (11.4) | 5 (14.3) |
>0.999b | 0.085 |
|
Grouping of surgeons |
|
|
|
|
|
|
Junior
surgeon | 4 (5.7) | 3 (8.6) | 1 (2.9) | 0.614b | 0.248 |
|
Senior
surgeon | 66 (94.3) | 32 (91.4) | 34 (97.1) |
|
|
| Pathology |
|
|
|
|
|
| Tumor
size, mm | 28 (7–130) | 26 (7–56) | 30 (10–130) | 0.331 | 0.344 |
| UICC
8th edition |
|
|
|
|
|
|
T category |
|
|
| 0.228b | 0.420 |
|
T1 | 11 (15.7) | 4 (11.4) | 7 (20.0) |
|
|
|
T2 | 43 (61.4) | 25 (71.4) | 18 (51.4) |
|
|
|
T3 | 16 (22.9) | 6 (17.1) | 10 (28.6) |
|
|
|
T4 | 0 (0.0) | 0 (0.0) | 0 (0.0) |
|
|
|
N category |
|
|
| 0.679 | 0.211 |
|
N0 | 30 (42.9) | 16 (45.7) | 14 (40.0) |
|
|
|
N1 | 25 (35.7) | 13 (37.1) | 12 (34.3) |
|
|
|
N2 | 15 (21.4) | 6 (17.1) | 9 (25.7) |
|
|
|
M category |
|
|
| 0.284b | 0.258 |
|
M0 | 61 (87.1) | 32 (91.4) | 29 (82.9) |
|
|
|
M1a | 9 (12.9) | 3 (8.6) | 6 (17.1) |
|
|
|
UICC stage |
|
|
| 0.061b | 0.842 |
|
IA | 8 (11.4) | 3 (8.6) | 5 (14.3) |
|
|
|
IB | 13 (18.6) | 11 (31.4) | 2 (5.7) |
|
|
|
IIA | 6 (8.6) | 1 (2.9) | 5 (14.3) |
|
|
|
IIB | 25 (35.7) | 13 (37.1) | 12 (34.3) |
|
|
|
III | 9 (12.9) | 4 (11.4) | 5 (14.3) |
|
|
|
IV | 9 (12.9) | 3 (8.6) | 6 (17.1) |
|
|
| R0 resection | 63 (90.0) | 31 (88.6) | 32 (91.4) |
>0.999b | 0.093 |
| Table VI.Comparison of operative and
postoperative outcomes after propensity score matching. |
Table VI.
Comparison of operative and
postoperative outcomes after propensity score matching.
| Outcomes | Post-match all
(n=70) | STH (n=35) | ANH (n=35) | P-value |
|---|
| Operative
results |
|
|
|
|
|
Procedure |
|
|
| 0.568b |
|
Pancreaticoduodenectomy | 50 (71.4) | 26 (74.3) | 24 (68.6) |
|
|
Distal
pancreatectomy | 19 (27.1) | 9 (25.7) | 10 (28.6) |
|
|
Total
pancreatectomy | 1 (1.4) | 0 (0.0) | 1 (2.9) |
|
| Portal
vein resection | 9 (12.9) | 4 (11.4) | 5 (14.3) |
>0.999b |
|
Operation time, min | 310 (129–619) | 261 (139–619) | 327 (129–587) | 0.042 |
|
Anesthesia time, min | 374 (187–680) | 368 (226–676) | 392 (187–680) | 0.086 |
|
Intraoperative blood loss,
ml | 728
(130–2,200) | 570
(130–2,000) | 970
(150–2,200) | <0.001 |
| IBL
>20% in CBV | 33 (47.1) | 10 (28.6) | 23 (65.7) | 0.002 |
| Blood
volume removed, ml | 0 (0–800) | 0 (0–0) | 800 (400–800) | <0.001 |
|
Intraoperative fluid given,
ml | 3,700
(1,300–7,500) | 3,200
(1,300-7.500) | 4,000
(2,550–6,300) | <0.001 |
|
Intraoperative albumin,
ml | 0 (0–750) | 0 (0–500) | 0 (0–750) | 0.138 |
|
Intraoperative FFP, ml | 0 (0–0) | 0 (0–0) | 0 (0–0) | - |
|
Intraoperative PC, ml | 0 (0–0) | 0 (0–0) | 0 (0–0) | - |
| Total
fluid volume administered, ml | 4,075
(1,300–8,000) | 3,200
(1,300–8,000) | 4,850
(2,950–7,600) | <0.001 |
|
Intraoperative urine output,
ml | 500 (20–1,550) | 430
(188–1,550) | 530 (20–1,550) | 0.332 |
| Total
in-out balance, ml | 2,368
(485–5,500) | 1,935
(485–5,500) | 2,670
(1,190–4,555) | 0.003 |
| Total
in-out balance, ml/kg/ha | 6.5 (1.8–13.9) | 6.3 (1.8–11.2) | 6.6 (3.2–13.9) | 0.104 |
| Postoperative
results |
|
|
|
|
|
Postoperative complications
(Clavien- | 13 (18.6) | 4 (11.4) | 9 (25.7) | 0.124b |
| Dindo
classification grade ≥3) |
|
|
|
|
|
Pancreatic fistula (ISGPF
grade ≥B) | 11 (15.7) | 4 (11.4) | 7 (20.0) | 0.324b |
| Delayed
gastric emptying (ISGPS grade ≥B) | 9 (12.9) | 3 (8.6) | 6 (17.1) | 0.477b |
|
Postoperative hospital stay,
days | 17 (6–64) | 17 (8–61) | 19 (6–64) | 0.101 |
|
Adjuvant chemotherapy | 54 (78.3) | 29 (82.9) | 25 (73.5) | 0.348 |
Next, we evaluated the postoperative complications
in the matched cohort. As a result, there were no significant
differences in the incidences of postoperative complications
between the two groups after PSM (Table VI). Furthermore, we performed a
survival analysis of the matched cohort. RFS time was slightly but
not significantly poorer in the ANH group compared with the STD
group (MST, 12.1 vs. 18.1 months, P=0.097; Fig. 2C). In addition, a similar trend was
noted in the DSS rate (MST, 32.1 vs. 50.5 months, P=0.097; Fig. 2D). After PSM, in contrast with
short-term outcomes, postoperative long-term outcomes in the ANH
group were less favorable than those in the STD group.
To assess whether ANH influences RFS and DSS in the
matched cohort, we performed a Cox regression analysis. As a
result, we identified some factors that had a greater effect on
poor prognosis than ANH (Table
SI).
Discussion
This report represents the first study to examine
the effect of ANH on PDAC prognosis longitudinally. This study
demonstrated that ANH has a negative impact on long-term outcomes
in PDAC compared to standard management, though not as negative as
ABT. Similar results were confirmed even after propensity score
matching analysis. These results elucidate the potential negative
effects of ANH compared to management without transfusion in
resectable PDAC.
Despite the proven short-term outcomes (36,37),
there are surprisingly few studies evaluating the long-term effects
of ANH on cancer patients. A recent post-hoc analysis from a
prospective trial demonstrated that ANH did not have any
detrimental effects on long-term oncologic outcomes in patients
undergoing primary debulking surgery for advanced ovarian cancer
(21). In the field of
gastroenterology, an RCT evaluating ANH during major hepatectomy
procedures for metastatic colorectal cancer showed no detrimental
impact of ANH on survival outcomes (28). These findings are the opposite of
our results. However, the studies were originally conducted to
determine if ANH reduced the need for ABT. In short, these post-hoc
analyses comparing the long-term outcomes between the STD and ANH
groups included patients who received ABT. This heterogeneity may
have affected the survival outcomes, because ABT can cause an
immunomodulatory effect leading to worse oncologic outcomes
(17). Thus, we excluded patients
who received ABT and then directly compared the ANH and STD groups.
As a result, our study figured out the potential differences in
prognosis between the STD and ANH groups.
How does ANH affect the prognosis in PDAC patients
who have undergone pancreatic resection? Direct and indirect
effects can be assumed. One of the possible direct effects is the
immunosuppressive effect of ANH (38). Additionally, compared to standard
management, ANH is logically associated with circulatory overload.
The only prospective RCT, in which every assessed ANH inpatient
underwent PD, determined that ANH was related to greater
intraoperative fluid management, and resulted in more pancreatic
anastomotic complications (19). A
similar trend was observed in this study as well. Postoperative
complications may have a negative effect on survival outcomes in
cancer patients (28,39,40),
including PDAC (41,42). It has been suggested that
postoperative complications could have immunosuppressive effects
(39,40,43).
Therefore, in terms of postoperative complications after ANH,
immunosuppressive effects may be an additional consideration.
In our cohort, after PSM, the ANH group was
associated with great intraoperative blood loss compared to the STD
group. This trend was observed in a previous RCT of ANH in patients
undergoing PD (19). Conversely,
this trend was not observed in another liver surgery RCT (27). Several lines of evidence have shown
an association between increased blood loss and poor outcomes in
PDAC surgery (15,16,44).
Our previous study also demonstrated those relationships (29). These data suggest that more
intraoperative blood loss may negatively influence the prognosis of
ANH. At the same time, we must be deliberate and critically
consider that ANH can potentially cause increased intraoperative
blood loss.
The present study has several limitations. First,
this is a retrospective single-institution cohort study and not a
randomized control trial. The patient population was not large. In
this study, we performed propensity score matching using caliper
matching, achieving a satisfactory balance of pre-ANH variables
between the STD and ANH groups. However, despite our best efforts,
there are instances where standardized difference scores exceed 0.2
for certain variables. One possible explanation for this is that
large variations in certain variables, such as CA19-9, may
contribute to such an imbalance. In addition, not having a large
sample size may have created a non-ideal balance after PSM. These
results speak to the desirability of a larger sample size for
achieving optimal balance. However, if we had added the borderline
resectable PDAC cohort to the current resectable PDAC cohort, the
borderline cases would have greatly increased the ANH group due to
the estimated increased blood loss associated with vascular
resection. Adding borderline cases, however, would make it
difficult to validate the true impact of ANH on long-term outcomes
in PDAC patients. Moreover, typical study biases, such as fluid
overloading, more intraoperative blood loss, longer operation time,
etc., were not excluded from this study. These biases make drawing
definitive conclusions difficult. Nonetheless, there have been no
previous studies examining the effect of ANH on the long-term
prognosis of PDAC. Accordingly, the suggestions from this study
should not be ignored.
In conclusion, the present study, using PSM
analysis, showed that ANH could be associated with poor
postoperative long-term outcomes in resectable PDAC patients
compared to STD. Various biases make it difficult to conclude
whether or not ANH is inherently harmful. However, the one thing we
can say without hesitation is that management without transfusion
is the best course of action. Furthermore, ABT has the worst
negative impact. Thus, we should make every effort to avoid ABT,
and ANH is certainly a valuable approach to achieve this goal. In
general, at least until a definitive conclusion is reached, it is
better to limit the use of ANH in certain specific PDAC cases.
Supplementary Material
Supporting Data
Acknowledgements
The authors would like to thank Professor Shari Joy
Berman (Hirosaki University Graduate School of Medicine, Hirosaki,
Japan) for professionally editing the English draft of this
manuscript.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
TW, KI, NK and KHa contributed to the study
conception and design. TW, KI, NK, HN and KHa performed surgical
resection. TW, KI, NK, HN, TK, SK, HF, YT, TY, KC, JS, KHi and KHa
collected the clinical data. TW, KI, NK, HN, TK, SK, HF, YT, TY,
KC, JS, KHi and KHa analyzed and interpreted the data. TW wrote the
first draft of the manuscript. KI, NK, HN, TK, SK, HF, YT, TY, KC,
JS, KHi and KHa contributed to the review and/or critical revision
of the manuscript. All authors agreed to be accountable for all
aspects of the work in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved. TW and KI confirm the authenticity of
all the raw data. All authors have read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Committee of
Medical Ethics of Hirosaki University Graduate School of Medicine
(reference no. 2022-032; Aomori, Japan). Informed consent was
obtained in the form of an opt-out feature on our website, with the
approval of the Committee of Medical Ethics of Hirosaki University
Graduate School of Medicine. The present study did not include
minors. The present study was designed and carried out in
accordance with the Declaration of Helsinki.
Patient consent for publication
Informed consent for publication was obtained in the
form of an opt-out feature on our website, with the approval of the
Committee of Medical Ethics of Hirosaki University Graduate School
of Medicine (Aomori, Japan).
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ABT
|
allogeneic blood transfusion
|
|
ANH
|
acute normovolemic hemodilution
|
|
DP
|
distal pancreatectomy
|
|
DSS
|
disease-specific survival
|
|
MST
|
median survival time
|
|
RFS
|
recurrence-free survival
|
|
RR
|
relative risk
|
|
PD
|
pancreatoduodenectomy
|
|
PDAC
|
pancreatic ductal adenocarcinoma
|
|
PSM
|
propensity score matching
|
|
STD
|
standard management
|
|
UICC
|
Union for International Cancer
Control
|
References
|
1
|
GBD 2017 Pancreatic Cancer Collaborator, .
The global, regional, and national burden of pancreatic cancer and
its attributable risk factors in 195 countries and territories,
1990–2017: A systematic analysis for the Global Burden of Disease
Study 2017. Lancet Gastroenterol Hepatol. 4:934–947. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2022. CA Cancer J Clin. 72:7–33. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kleeff J, Korc M, Apte M, La Vecchia C,
Johnson CD, Biankin AV, Neale RE, Tempero M, Tuveson DA, Hruban RH
and Neoptolemos JP: Pancreatic cancer. Nat Rev Dis Primers.
2:160222016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Doi R, Imamura M, Hosotani R, Imaizumi T,
Hatori T, Takasaki K, Funakoshi A, Wakasugi H, Asano T, Hishinuma
S, et al: Surgery versus radiochemotherapy for resectable locally
invasive pancreatic cancer: Final results of a randomized
multi-institutional trial. Surg Today. 38:1021–1028. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bilimoria KY, Bentrem DJ, Ko CY, Stewart
AK, Winchester DP and Talamonti MS: National failure to operate on
early stage pancreatic cancer. Ann Surg. 246:173–180. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ahola R, Sand J and Laukkarinen J:
Pancreatic resections are not only safest but also most
cost-effective when performed in a high-volume centre: A Finnish
register study. Pancreatology. 19:769–774. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Amini N, Spolverato G, Gupta R, Margonis
GA, Kim Y, Wagner D, Rezaee N, Weiss MJ, Wolfgang CL, Makary MM, et
al: Impact total psoas volume on short- and long-term outcomes in
patients undergoing curative resection for pancreatic
adenocarcinoma: A new tool to assess sarcopenia. J Gastrointest
Surg. 19:1593–1602. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
de Wilde RF, Besselink MG, van der Tweel
I, de Hingh IH, van Eijck CH, Dejong CH, Porte RJ, Gouma DJ, Busch
OR and Molenaar IQ; Dutch Pancreatic Cancer Group, : Impact of
nationwide centralization of pancreaticoduodenectomy on hospital
mortality. Br J Surg. 99:404–410. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gooiker GA, Lemmens VE, Besselink MG,
Busch OR, Bonsing BA, Molenaar IQ, Tollenaar RA, de Hingh IH and
Wouters MW: Impact of centralization of pancreatic cancer surgery
on resection rates and survival. Br J Surg. 101:1000–1005. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Onete VG, Besselink MG, Salsbach CM, Van
Eijck CH, Busch OR, Gouma DJ, de Hingh IH, Sieders E, Dejong CH,
Offerhaus JG, et al: Impact of centralization of
pancreatoduodenectomy on reported radical resections rates in a
nationwide pathology database. HPB (Oxford). 17:736–742. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hachey K, Morgan R, Rosen A, Rao SR,
McAneny D, Tseng J, Doherty G and Sachs T: Quality comes with the
(Anatomic) territory: Evaluating the impact of surgeon operative
mix on patient outcomes after pancreaticoduodenectomy. Ann Surg
Oncol. 25:3795–3803. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Snyder RA, Prakash LR, Nogueras-Gonzalez
GM, Kim MP, Aloia TA, Vauthey JN, Lee JE, Fleming JB, Katz MHG and
Tzeng CD: Perioperative blood transfusions for vein resection
during pancreaticoduodenectomy for pancreatic adenocarcinoma:
Identification of clinical targets for optimization. HPB (Oxford).
21:841–848. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ecker BL, Simmons KD, Zaheer S, Poe SL,
Bartlett EK, Drebin JA, Fraker DL, Kelz RR, Roses RE and Karakousis
GC: Blood transfusion in major abdominal surgery for malignant
tumors: A trend analysis using the national surgical quality
improvement program. JAMA Surg. 151:518–525. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kneuertz PJ, Patel SH, Chu CK, Maithel SK,
Sarmiento JM, Delman KA, Staley CA III and Kooby DA: Effects of
perioperative red blood cell transfusion on disease recurrence and
survival after pancreaticoduodenectomy for ductal adenocarcinoma.
Ann Surg Oncol. 18:1327–1334. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Seykora TF, Ecker BL, McMillan MT, Maggino
L, Beane JD, Fong ZV, Hollis RH, Jamieson NB, Javed AA, Kowalsky
SJ, et al: The beneficial effects of minimizing blood loss in
pancreatoduodenectomy. Ann Surg. 270:147–157. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rystedt J, Tingstedt B, Ansorge C, Nilsson
J and Andersson B: Major intraoperative bleeding during
pancreatoduodenectomy-preoperative biliary drainage is the only
modifiable risk factor. HPB (Oxford). 21:268–274. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Remy KE, Hall MW, Cholette J, Juffermans
NP, Nicol K, Doctor A, Blumberg N, Spinella PC, Norris PJ, Dahmer
MK, et al: Mechanisms of red blood cell transfusion-related
immunomodulation. Transfusion. 58:804–815. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kanda T, Wakiya T, Ishido K, Brierley,
Kimura N, Nagase H, Kubota S, Fujita H, Hagiwara Y and Hakamada K:
Intraoperative allogeneic red blood cell transfusion negatively
influences prognosis after radical surgery for pancreatic cancer: A
propensity score matching analysis. Pancreas. 50:1314–1325. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fischer M, Matsuo K, Gonen M, Grant F,
Dematteo RP, D'Angelica MI, Mascarenhas J, Brennan MF, Allen PJ,
Blumgart LH and Jarnagin WR: Relationship between intraoperative
fluid administration and perioperative outcome after
pancreaticoduodenectomy: Results of a prospective randomized trial
of acute normovolemic hemodilution compared with standard
intraoperative management. Ann Surg. 252:952–958. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tanner EJ, Filippova OT, Gardner GJ, Long
Roche KC, Sonoda Y, Zivanovic O, Fischer M and Chi DS: A
prospective trial of acute normovolemic hemodilution in patients
undergoing primary cytoreductive surgery for advanced ovarian
cancer. Gynecol Oncol. 151:433–437. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Boerner T, Tanner E, Filippova O, Zhou QC,
Iasonos A, Tew WP, O'Cearbhaill RE, Grisham RN, Gardner GJ, Sonoda
Y, et al: Survival outcomes of acute normovolemic hemodilution in
patients undergoing primary debulking surgery for advanced ovarian
cancer: A Memorial Sloan Kettering Cancer Center Team Ovary study.
Gynecol Oncol. 160:51–55. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lawson NW, Ochsner JL, Mills NL and
Leonard GL: The use of hemodilution and fresh autologous blood in
open-heart surgery. Anesth Analg. 53:672–683. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Grant MC, Resar LM and Frank SM: The
efficacy and utility of acute normovolemic hemodilution. Anesth
Analg. 121:1412–1414. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Spahn DR and Casutt M: Eliminating blood
transfusions: New aspects and perspectives. Anesthesiology.
93:242–255. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
American Society of Anesthesiologists Task
Force on Perioperative Blood Transfusion and Adjuvant Therapies, .
Practice guidelines for perioperative blood transfusion and
adjuvant therapies: An updated report by the American society of
anesthesiologists task force on perioperative blood transfusion and
adjuvant therapies. Anesthesiology. 105:198–208. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Barile L, Fominskiy E, Di Tomasso N,
Alpìzar Castro LE, Landoni G, De Luca M, Bignami E, Sala A,
Zangrillo A and Monaco F: Acute normovolemic hemodilution reduces
allogeneic red blood cell transfusion in cardiac surgery: A
systematic review and meta-analysis of randomized trials. Anesth
Analg. 124:743–752. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jarnagin WR, Gonen M, Maithel SK, Fong Y,
D'Angelica MI, Dematteo RP, Grant F, Wuest D, Kundu K, Blumgart LH
and Fischer M: A prospective randomized trial of acute normovolemic
hemodilution compared to standard intraoperative management in
patients undergoing major hepatic resection. Ann Surg. 248:360–369.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Correa-Gallego C, Gonen M, Fischer M,
Grant F, Kemeny NE, Arslan-Carlon V, Kingham TP, Dematteo RP, Fong
Y, Allen PJ, et al: Perioperative complications influence
recurrence and survival after resection of hepatic colorectal
metastases. Ann Surg Oncol. 20:2477–2484. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wakiya T, Ishido K, Kimura N, Nagase H,
Kubota S, Fujita H, Hagiwara Y, Kanda T, Matsuzaka M, Sasaki Y and
Hakamada K: Prediction of massive bleeding in pancreatic surgery
based on preoperative patient characteristics using a decision
tree. PLoS One. 16:e02596822021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM classification of malignant tumours. John Wiley
& Sons; Hoboken, NJ, USA: pp. 93–95. 2017, PubMed/NCBI
|
|
31
|
Shirai Y, Shiba H, Horiuchi T, Saito N,
Furukawa K, Sakamoto T, Gocho T, Ishida Y and Yanaga K: Assessment
of outcome after pancreaticoduodenectomy by junior surgeons.
Anticancer Res. 36:3505–3510. 2016.PubMed/NCBI
|
|
32
|
Takekawa D, Saito J, Kinoshita H, Hashiba
EI, Hirai N, Yamazaki Y, Kushikata T and Hirota K: Acute
normovolemic hemodilution reduced allogeneic blood transfusion
without increasing perioperative complications in patients
undergoing free-flap reconstruction of the head and neck. J Anesth.
34:187–194. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Dindo D, Demartines N and Clavien PA:
Classification of surgical complications: A new proposal with
evaluation in a cohort of 6336 patients and results of a survey.
Ann Surg. 240:205–213. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bassi C, Dervenis C, Butturini G,
Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, Sarr M, Traverso W
and Buchler M; International Study Group on Pancreatic Fistula
Definition, : Postoperative pancreatic fistula: An international
study group (ISGPF) definition. Surgery. 138:8–13. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wente MN, Bassi C, Dervenis C, Fingerhut
A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG,
Traverso LW, et al: Delayed gastric emptying (DGE) after pancreatic
surgery: A suggested definition by the International Study Group of
Pancreatic Surgery (ISGPS). Surgery. 142:761–768. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Ni Y, Ding XH, Xu ZJ, Zhang ZF, Zhang Y
and Gui B: Association of acute normovolemic hemodilution with
decreased length of hospital stay in rhesus-negative patients
undergoing major cancer surgeries: A retrospective study. Ann
Palliat Med. 10:1815–1824. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ni Y, Xu ZJ, Zhang ZF, Yang C, Liu CM and
Gui B: Acute normovolemic hemodilution for major cancer surgeries
during the COVID-19 pandemic: A beacon of hope. J Clin Anesth.
65:1098712020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Vamvakas EC: Meta-analysis of randomized
controlled trials comparing the risk of postoperative infection
between recipients of allogeneic and autologous blood transfusion.
Vox Sang. 83:339–346. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pucher PH, Aggarwal R, Qurashi M and Darzi
A: Meta-analysis of the effect of postoperative in-hospital
morbidity on long-term patient survival. Br J Surg. 101:1499–1508.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Artinyan A, Orcutt ST, Anaya DA,
Richardson P, Chen GJ and Berger DH: Infectious postoperative
complications decrease long-term survival in patients undergoing
curative surgery for colorectal cancer: A study of 12,075 patients.
Ann Surg. 261:497–505. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Aahlin EK, Olsen F, Uleberg B, Jacobsen BK
and Lassen K: Major postoperative complications are associated with
impaired long-term survival after gastro-esophageal and pancreatic
cancer surgery: A complete national cohort study. BMC Surg.
16:322016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lubrano J, Bachelier P, Paye F, Le Treut
YP, Chiche L, Sa-Cunha A, Turrini O, Menahem B, Launoy G and
Delpero JR: Severe postoperative complications decrease overall and
disease free survival in pancreatic ductal adenocarcinoma after
pancreaticoduodenectomy. Eur J Surg Oncol. 44:1078–1082. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Goldfarb Y, Sorski L, Benish M, Levi B,
Melamed R and Ben-Eliyahu S: Improving postoperative immune status
and resistance to cancer metastasis: A combined perioperative
approach of immunostimulation and prevention of excessive surgical
stress responses. Ann Surg. 253:798–810. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kazanjian KK, Hines OJ, Duffy JP, Yoon DY,
Cortina G and Reber HA: Improved survival following
pancreaticoduodenectomy to treat adenocarcinoma of the pancreas:
The influence of operative blood loss. Arch Surg. 143:1166–1171.
2008. View Article : Google Scholar : PubMed/NCBI
|