Introduction
Primary liver cancer ranks as the sixth most
commonly diagnosed cancer and the third leading cause of
cancer-related deaths worldwide (1). Hepatocellular carcinoma (HCC) accounts
for approximately 80% of primary liver cancers (1). In recent years, there have been
remarkable advancements in systemic chemotherapy for HCC.
Specifically, the use of immune checkpoint inhibitors (ICIs) in
combination therapy has emerged as a pivotal component of systemic
chemotherapy, revolutionizing the treatment landscape for HCC. In
the IMbrave150 trial, the combination of atezolizumab plus
bevacizumab (Ate/Bev), incorporating anti-programmed death ligand 1
(PD-L1) and anti-vascular endothelial growth factor (VEGF),
demonstrated superior survival outcomes compared to sorafenib, with
a median survival time of 19.2 months, according to the updated
analysis (2,3). Similarly, tremelimumab plus durvalumab
(Dur/Tre), which targets both anti-cytotoxic T
lymphocyte-associated antigen 4 and anti-PD-L1, demonstrated
superior outcomes compared to sorafenib, showcasing a median
survival time of 16.4 months in the HIMALAYA trial (4). Accordingly, both regimens have been
recommended as first-line treatments for advanced HCC in the
Barcelona Clinic Liver Cancer guidelines (5). In clinical practice, the optimal
choice for first-line treatment and the most effective sequence for
multidisciplinary management of unresectable HCC remains
unclear.
HCC with bile duct tumor thrombus (BDTT) is a rare
occurrence, with reported incidences ranging from 0.4 to 12.9% in
previous reports (6,7). The survival outcomes of patients with
HCC with BDTT after curative resection were significantly inferior
to those of patients without BDTT (6). Owing to the rarity of HCC with BDTT,
evidence regarding the therapeutic efficacy of systemic
chemotherapy for this condition remains insufficient.
Here, we report a case of advanced HCC with BDTT
extending to the common bile duct, which shows a significant
response to Dur/Tre treatment.
Case report
A 68-year-old Japanese man sought medical attention
from his family physician due to abdominal pain. He had no family
or past medical history, including viral infections such as
hepatitis B or C. Blood tests revealed elevated serum bilirubin
levels (total bilirubin, 3.7 mg/dl; direct bilirubin, 2.3 mg/dl)
and C-reactive protein levels (5.6 mg/dl). Abdominal computed
tomography (CT) revealed two intrahepatic tumors in the right lobe
and an intraductal mass in the right hepatic duct, suggestive of
hilar cholangiocarcinoma or liver metastasis. After receiving
antibiotic treatment for cholangitis, the patient was referred to
our hospital for diagnosis and treatment.
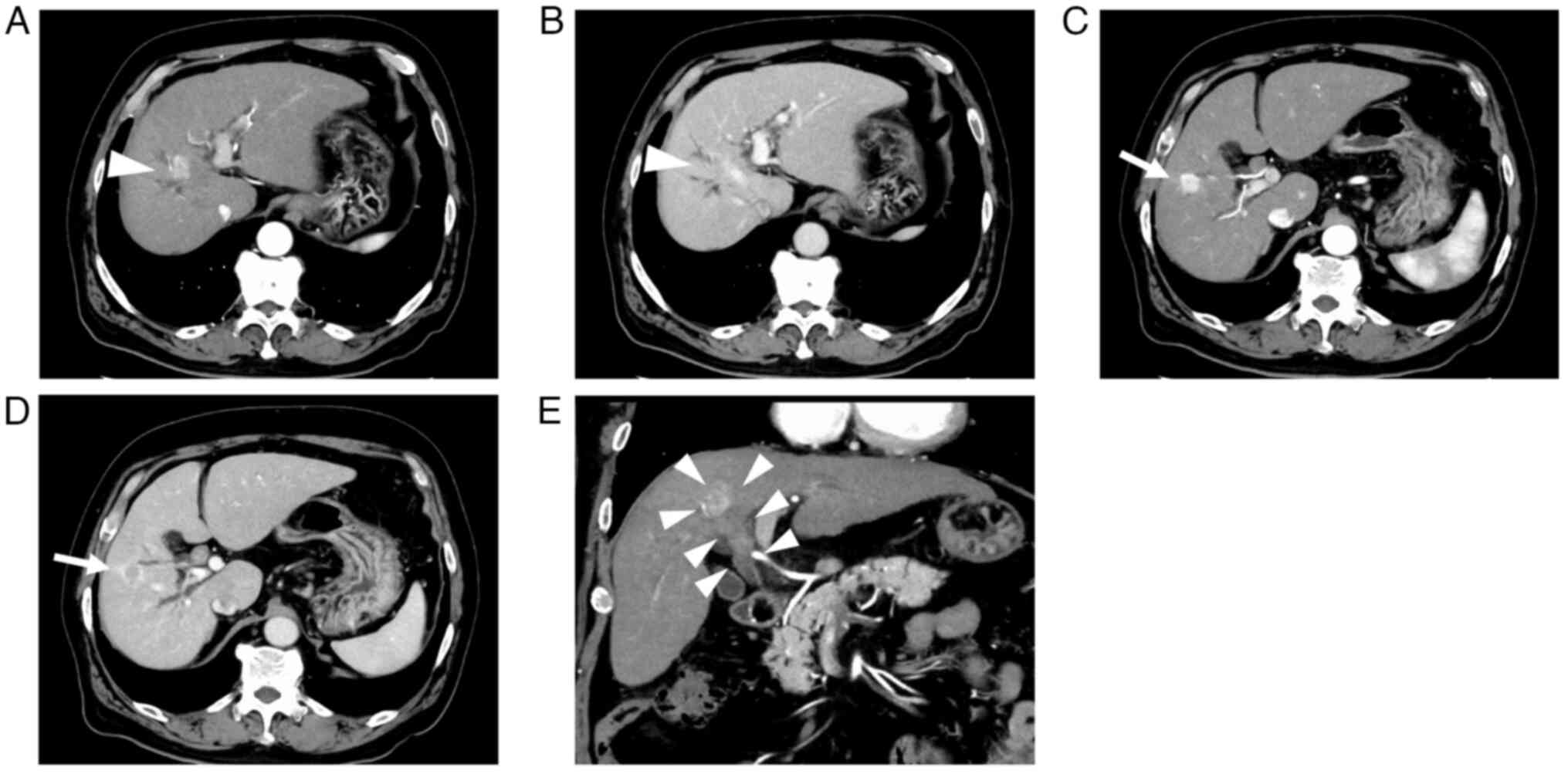
Abdominal contrast-enhanced CT (CECT) revealed two
intrahepatic tumors, one measuring 20.0 mm in segment 8 with BDTT
and the other measuring 18.8 mm in segment 5. These tumors
exhibited enhancement during the arterial phase and washout during
the late phase. Moreover, no extrahepatic metastases were detected
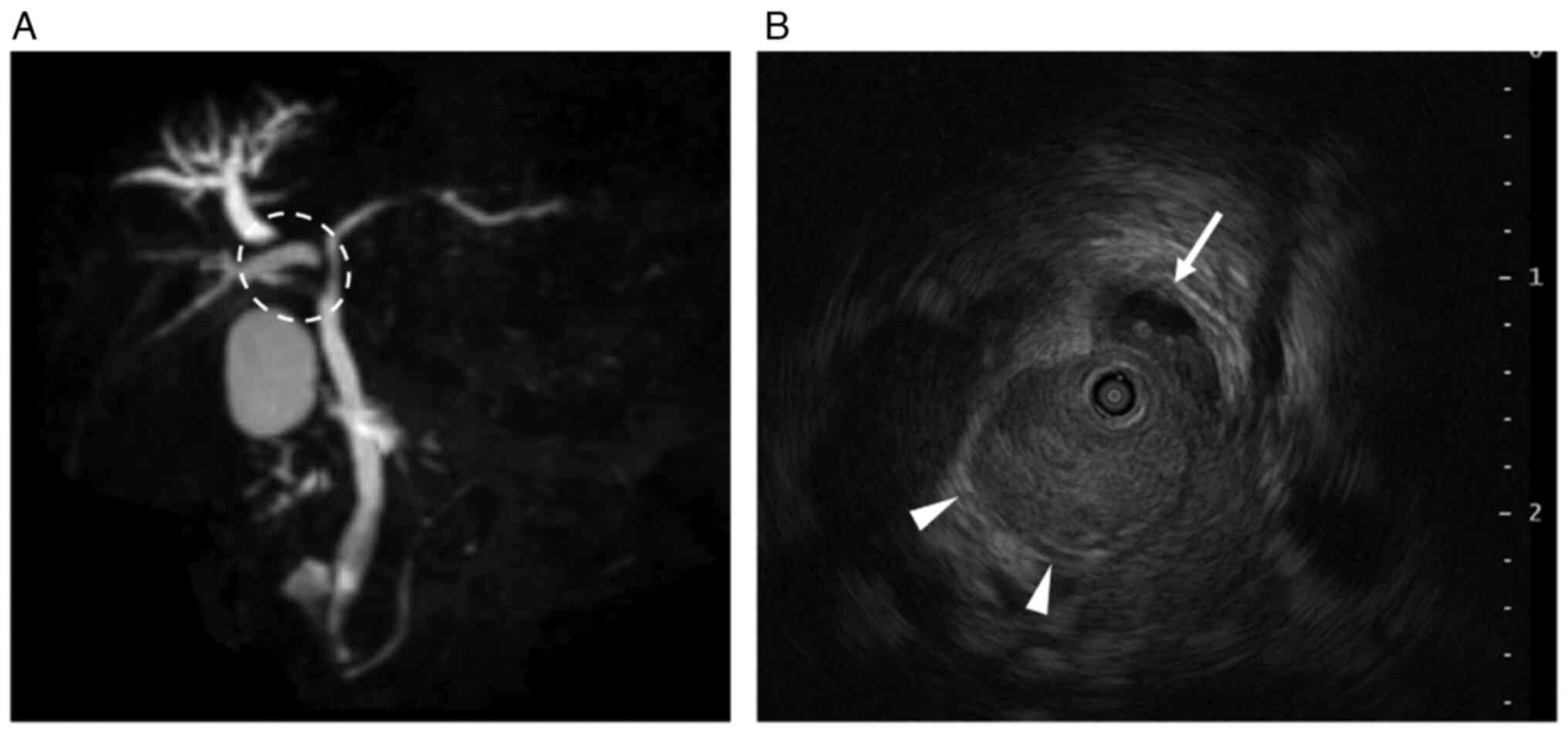
(Fig. 1). Magnetic resonance
cholangiopancreatography revealed the dilated peripheral
intrahepatic bile ducts in the right lobe (Fig. 2A). Intraductal ultrasonography
revealed that the BDTT had progressed to the bifurcation of the
left and right hepatic ducts and the right hepatic duct was
obstructed by the BDTT (Fig. 2B).
Subsequently, endoscopic retrograde cholangiopancreatography was
performed, and intraductal stents were inserted to prevent jaundice
progression. Thereafter, the serum bilirubin levels decreased to
normal levels (total bilirubin, 1.3 mg/dl; direct bilirubin, 0.3
mg/dl). Despite brush cytology of the bile duct showing malignant
components, BDTT biopsy did not confirm the presence of HCC.
Furthermore, the serum α-fetoprotein (AFP) and des-γ-carboxy
prothrombin (DCP) levels were 44 ng/ml and 57 mAU/ml, respectively,
while carcinoembryonic antigen and carbohydrate antigen 19–9 levels
were within normal ranges. Liver biopsy was not performed owing to
the risk of complications and delay in treatment initiation.
Accordingly, we diagnosed the tumors as HCC. The Child-Pugh score
was 6 (class A), and the albumin-bilirubin score was −1.64
(modified albumin-bilirubin grade 2b) (8). The indocyanine green retention rate at
15 min was 16.8%. Given that right hepatectomy with bile duct
reconstruction is necessary for curative surgery, we regarded these
tumors as unresectable HCC due to impaired liver function and
planned to administer systemic chemotherapy. We opted for Dur/Tre
treatment as the first-line approach because Ate/Bev seemed
unsuitable, given the biliary bleeding after the biopsy.
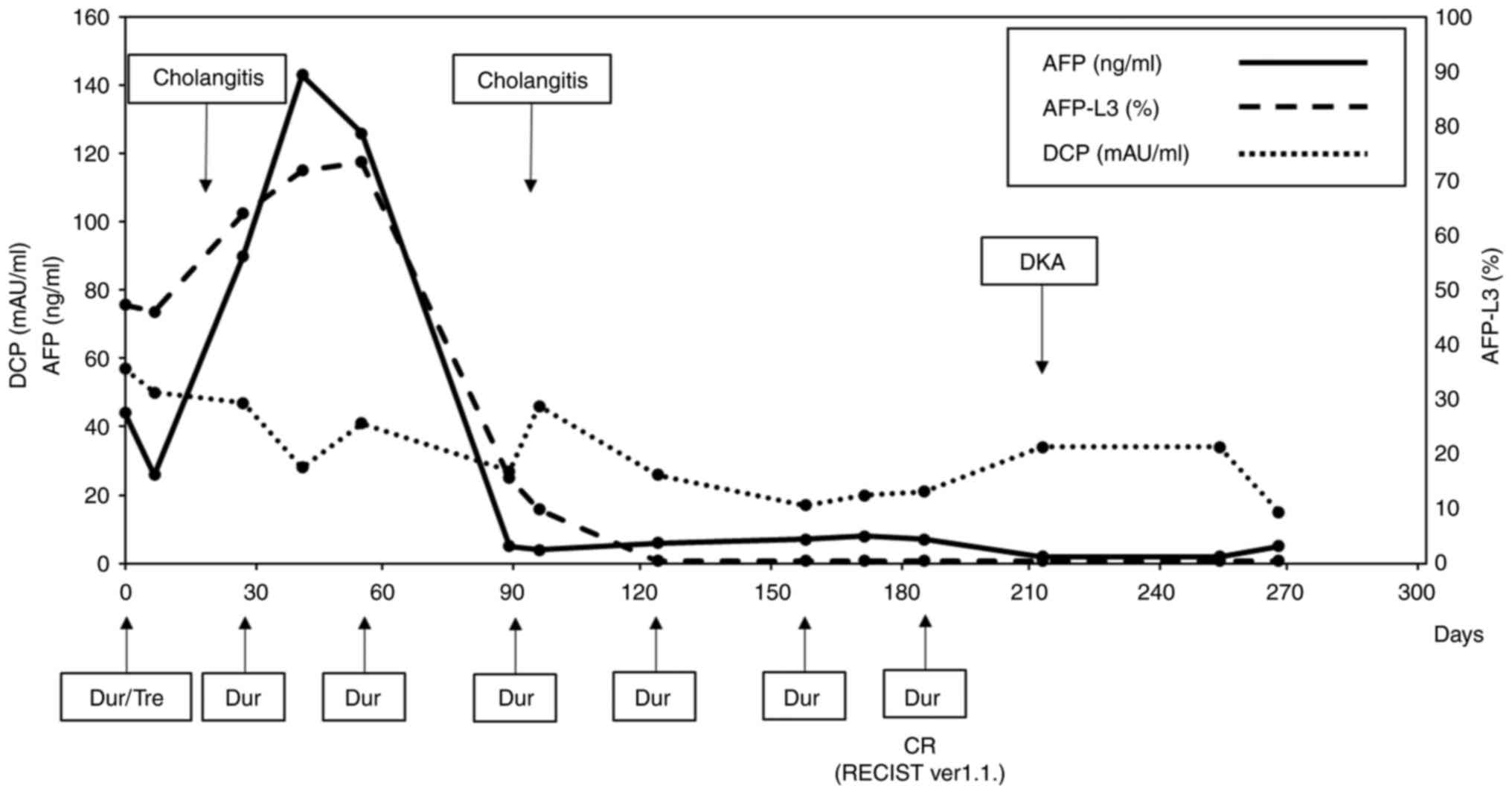
After treatment with tremelimumab (300 mg) and
durvalumab (1500 mg), durvalumab monotherapy was administered every
4 weeks. Although serum AFP levels increased from 44 ng/ml (before
treatment) to 143 ng/ml 1 month after treatment administration, the
response was evaluated as a stable disease according to the
Response Evaluation Criteria in Solid Tumors (RECIST; version 1.1)
(9) guidelines. Thereafter, the
serum AFP levels drastically decreased and normalized after three
courses of durvalumab monotherapy. The AFP L3 isoform followed a
similar course and normalized. The DCP levels also gradually
normalized after treatment. The clinical course and transition of
tumor marker levels are shown in Fig.
3. During treatment, the patient was hospitalized twice for
acute cholangitis treatment, during which intraductal stents were
replaced. Cholangiography, conducted 106 days after initiating
Dur/Tre treatment, showed improvement in bile duct obstruction.
Abdominal CECT showed continued shrinkage of the tumors and BDTT,
confirming complete response (CR) after six courses of durvalumab
monotherapy according to RECIST (version 1.1). The patient
presented to our emergency unit with a 4-day history of appetite
loss, vomiting, and impaired consciousness 215 days after the first
Dur/Tre treatment. Blood tests revealed hyperglycemia (987 mg/dl),
severe metabolic acidosis (pH: 6.88), and renal failure (blood urea
nitrogen, 71.5 mg/dl; serum creatinine, 3.05 mg/dl). The patient
was diagnosed with diabetic ketoacidosis (DKA) induced by an ICI
and was treated with fluid resuscitation and intravenous insulin
administration in the intensive care unit. The patient was
discharged home with insulin injection therapy for ICI-induced type
1 diabetes mellitus (T1DM) and was followed up without any systemic
chemotherapy for HCC.
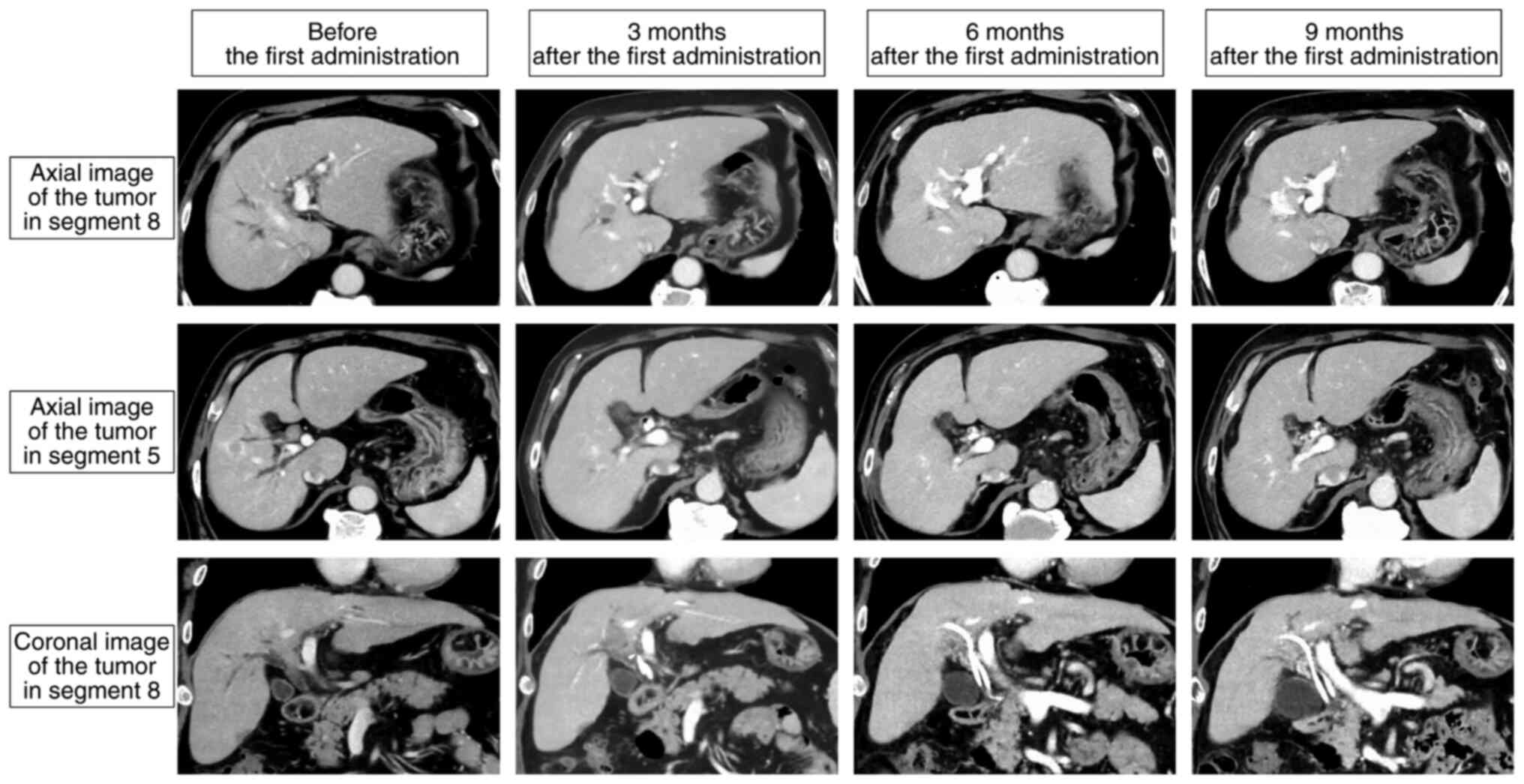
The patient is currently being followed up as an
outpatient in a drug-free state 290 days after the initial
administration of Dur/Tre without any sign of recurrence and other
new adverse events (Fig. 4).
Discussion
We present a rare case demonstrating a significant
response to Dur/Tre treatment in HCC with BDTT. Although serum AFP
levels increased after the first administration of Dur/Tre, the
tumor size remained unchanged at the first CECT evaluation.
Subsequently, serum AFP levels drastically decreased to normal
levels. Intrahepatic tumors and BDTT shrank following the tumor
markers and ultimately became undetectable. To the best of our
knowledge, this is the first HCC case with BDTT to achieve
‘clinical CR’ (10) using Dur/Tre
without sequential local therapy. Despite Dur/Tre exhibiting an
objective response of 20.1% and a progressive disease rate of
39.9%, respectively, which may appear inferior to those reported
for Ate/Bev (objective response rate: 27.3%, progressive disease
rate: 19.6%) (2,4), Dur/Tre demonstrated superiority in
overall survival's long-tail effect owing to the synergistic action
of anti-CTLA4 and anti-PD-L1 agents (11). Moreover, Dur/Tre is preferable for
patients at risk of bleeding or proteinuria, conditions for which
bevacizumab, a VEGF inhibitor, might be contraindicated (12). In this specific case, owing to the
bleeding risk from the BDTT post-biopsy, Dur/Tre emerged as an
ideal first-line option over Ate/Bev.
ICIs play an important role in enhancing the cancer
immunity cycle (13), leading to
various immune-related adverse events (irAEs). In the HIMALAYA
trial, grade 3 or 4 irAEs occurred in 12.6% of the patients
(4), but the incidence of
ICI-induced T1DM in patients who received Dur/Tre for HCC remains
unknown. The occurrence of ICI-induced T1DM is exceptionally rare,
with a reported frequency of approximately 1% after administration
of ICIs (14). In a clinical trial
of lung cancer using tremelimumab, durvalumab, or both, T1DM was
observed in a few patients (15).
Although the mechanism underlying ICI-induced T1DM is not yet fully
understood, it may involve unintended immune responses against
pancreatic islets. ICI-induced T1DM occurs several weeks to months
after the initiation of ICI, and the onset is exceptionally rapid
due to DKA; therefore, careful glucose level monitoring becomes
mandatory (14). In this case, it
might be difficult to re-introduce Dur/Tre or change the regimen in
the event tumor progression emerges. Long-time follow-up for other
potential irAEs is also required.
Bile duct invasion is associated with malignant
features such as portal vein invasion, intrahepatic metastasis,
poor tumor differentiation, and gross classification (6,7). Yeh
et al (16) demonstrated
that silencing of the microRNA-200 family was related to BDTT via
ZEB1-mediated epithelial-to-mesenchymal transition. Recently, Xu
et al (17) demonstrated
that tumor-initiating cells expressing high BMI1 induced
trans-intrahepatic biliary epithelial migration via secreting
lysosomal cathepsin B. Evidence regarding the pathophysiology of
HCC with BDTT is currently limited, especially regarding the
efficacy of systemic chemotherapy, including ICIs. Among a cohort
of 10 patients with HCC and BDTT treated with sorafenib, the
objective response and disease control rates were 20.0 and 70.0%,
respectively. The overall survival and time to progression of
patients with HCC and BDTT were comparable to those of patients
without BDTT (18). Another cohort
study of patients with HCC ineligible for the REFLECT trial
demonstrated more promising outcomes with lenvatinib treatment,
revealing an 85.7% objective response rate and a 100% disease
control rate for patients with BDTT (19). In the IMbrave150 trial, patients
with high-risk statuses, including tumor invasion of the main trunk
of the portal vein, tumor occupancy of ≥50%, and bile duct
invasion, were treated with Ate/Bev. They had an overall survival
of 7.6 months and an objective response rate of 25.0% (3). Although there have been reports of HCC
cases with portal vein tumor thrombus achieving CR with Ate/Bev
(20,21), reports regarding CR to HCC with BDTT
are lacking. Robust analyses with larger sample sizes are needed to
elucidate the biological features and identify suitable treatment
strategies for HCC with BDTT.
In conclusion, we reported a rare case of HCC with
BDTT exhibiting a significant response to Dur/Tre treatment,
accompanied by severe irAEs in the form of ICI-induced T1DM.
Although long-term and further careful observations are required,
the present findings may have a substantial impact on the selection
of systemic chemotherapy for advanced HCC.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
NI and SK conceptualized the case report. NI wrote
the manuscript and performed additional data analysis. SK, MK, HG,
KF, TU, TY, KA, HY, HT and TF were involved in the treatment and
follow-up in this case. MK, HG, KF, TU, TY, KA, HY and HT
critically revised the manuscript and provided valuable feedback.
TF provided supervision and approved the final manuscript for
publication. NI and SK confirm the authenticity of all the raw
data. All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent for publication of
individual data and any accompanying images was obtained from the
patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
ICI
|
immune checkpoint inhibitor
|
|
Ate/Bev
|
atezolizumab plus bevacizumab
|
|
PD-L1
|
programmed cell death-ligand 1
|
|
VEGF
|
vascular endothelial growth factor
|
|
Dur/Tre
|
tremelimumab plus durvalumab
|
|
BDTT
|
bile duct tumor thrombus
|
|
CT
|
computed tomography
|
|
CECT
|
contrast-enhanced CT
|
|
AFP
|
α-fetoprotein
|
|
DCP
|
des-γ-carboxy prothrombin
|
|
RECIST
|
Response Evaluation Criteria in Solid
Tumors
|
|
CR
|
complete response
|
|
DKA
|
diabetic ketoacidosis
|
|
T1DM
|
type 1 diabetes mellitus
|
|
irAE
|
immune-related adverse events
|
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux
M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al: Atezolizumab
plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J
Med. 382:1894–1905. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cheng AL, Qin S, Ikeda M, Galle PR,
Ducreux M, Kim TY, Lim HY, Kudo M, Breder V, Merle P, et al:
Updated efficacy and safety data from IMbrave150: Atezolizumab plus
bevacizumab vs. sorafenib for unresectable hepatocellular
carcinoma. J Hepatol. 76:862–873. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Abou-Alfa GK, Lau G, Kudo M, Chan SL,
Kelley RK, Furuse J, Sukeepaisarnjaroen W, Kang YK, Dao TV, De Toni
EN, et al: Tremelimumab plus durvalumab in unresected
hepatocellular carcinoma. N Eng J Med Evid.
1:EVIDoa21000702022.
|
|
5
|
Reig M, Forner A, Rimola J, Ferrer-Fàbrega
J, Burrel M, Garcia-Criado A, Kelley RK, Galle PR, Mazzaferro V,
Salem R, et al: BCLB strategy for prognosis prediction and
treatment recommendation: The 2022 update. J Hepatol. 76:681–693.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ikenaga N, Chijiwa K, Otani K, Ohuchida J,
Uchiyama S and Kondo K: Clinicopathologic characteristics of
hepatocellular carcinoma with bile duct invasion. J Gastrointest
Surg. 13:492–497. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wu JY, Sun JX, Wu JY, Huang XX, Bai YN,
Wei YG, Zhang ZB, Zhou JY, Cheng SQ and Yan ML: Impact of bile duct
tumor thrombus on the long-term surgical outcomes of hepatocellular
carcinoma patients: A propensity score matching analysis. Ann Surg
Oncol. 29:949–958. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hiraoka A, Michitaka K, Kumada T, Izumi N,
Kadoya M, Kokudo N, Kubo S, Matsuyama Y, Nakashima O, Sakamoto M,
et al: Validation and potential of albumin-bilirubin grade and
prognostication in a nationwide survey of 46,681 hepatocellular
carcinoma patients in Japan: The need for a more detailed
evaluation of hepatic function. Liver Cancer. 6:325–36. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eisenheauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1.). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kudo M, Aoki T, Ueshima K, Tsuchiya K,
Morita M, Chishina H, Takita M, Hagiwara S, Minami Y, Ida H, et al:
Achievement of complete response and drug-free status by
atezolizumab plus bevacizumab combined with or without curative
conversion in patients with transarterial
chemoembolization-unsuitable, intermediate-stage hepatocellular
carcinoma: A multicenter proof-of-concept study. Liver Cancer.
12:321–338. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kelley RK, Sangro B, Harris W, Ikeda M,
Okusaka T, Kang YK, Qin S, Tai DWM, Lim HY, Yau T, et al: Safety,
efficacy, and pharmacodynamics of tremelimumab plus durvalumab for
patients with unresectable hepatocellular carcinoma: Randomized
expansion of a phase I/II study. J Clin Oncol. 39:2991–3001. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kudo M: Current therapeutic strategies for
hepatocellular carcinoma in Japan. Liver Cancer. 12:497–509. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kudo M: Scientific rationale for combined
immunotherapy with PD-1/PD-L1 antibodies and VEGF inhibitors in
advanced hepatocellular carcinoma. Cancers. 12:10892020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cho YK and Jung CH: Immune-checkpoint
inhibitors-induced type 1 diabetes mellitus: From its molecular
mechanisms to clinical practice. Diabetes Metab J. 47:757–766.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Johnson ML, Cho BC, Luft A,
Alatorre-Alexander J, Geater SL, Laktionov K, Kim SW, Ursol G,
Hussein M, Lim FL, et al: Durvalumab with or without tremelimumab
in combination with chemotherapy as first-line therapy for
metastatic non-small-cell lung cancer: The phase III POSEIDON
study. J Clin Oncol. 41:1213–1227. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yeh TS, Wang F, Chen TC, Yeh CN, Yu MC,
Jan YY and Chen MF: Expression profile of microRNA-200 family in
hepatocellular carcinoma with bile duct tumor thrombus. Ann Surg.
259:346–354. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu LB, Qin YF, Su L, Huang C, Xu Q, Zhang
R, Shi XD, Sun R, Chen J, Song Z, et al: Cathepsin-facilitated
invasion of BMI1-high hepatocellular carcinoma cells drives bile
duct tumor thrombi formation. Nat Commun. 14:70332023. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tanaka T, Kuzuya T, Ishigami M, Ito T,
Ishizu Y, Honda T, Ishikawa T and Fujishiro M: Efficacy and safety
of sorafenib in unresectable hepatocellular carcinoma with bile
duct invasion. Oncology. 98:621–629. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sho T, Suda G, Ogawa K, Shigesawa T,
Suzuki K, Nakamura A, Ohara M, Umemura M, Kawagishi N, Natsuizaka
M, et al: Lenvatinib in patients with unresectable hepatocellular
carcinoma who do not meet the REFLECT trial eligibility criteria.
Hepatol Res. 50:966–977. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Komatsu S, Fujishima Y, Kido M, Kuramitsu
K, Goto T, Yanagimoto H, Toyama H and Fukumoto T: Significant
response to atezolizumab plus bevacizumab treatment in unresectable
hepatocellular carcinoma with portal vein tumor thrombus: A case
report. BMC Gastroenterol. 21:4702021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kurisaki K, Soyama A, Hara T, Matsushima
H, Imamura H, Tanaka T, Adachi T, Ito S, Kanetaka K, Hidaka M, et
al: Pathologic complete response after chemotherapy with
atezolizumab plus bevacizumab for hepatocellular carcinoma with
tumor thrombus in the main portal trunk. Dig Surg. 40:84–89. 2023.
View Article : Google Scholar : PubMed/NCBI
|