Introduction
Lung cancer is the leading cause of cancer-related
mortality worldwide and lymph node metastasis serves as the primary
mode of lung cancer spread; therefore, lymph node dissection is
important in surgery (1). Notably,
the chosen surgical approach depends on various factors. The Japan
Clinical Oncology Group (JCOG) 0802 study demonstrated that lung
segmentectomy can be an appropriate option for lung nodules sized
<2 cm and with a consolidation-to-tumor ratio of >0.5, as it
offers comparable survival outcomes to lung lobectomy (2). Additionally, intraoperative gross
appearance and the experience of the surgeon are factors that
should be considered. For example, if preoperative imaging does not
indicate significant enlargement of mediastinal lymph nodes and
meets the criteria for segmentectomy according to JCOG 0802, but
the surgeon encounters larger, harder or fused lymph nodes
intraoperatively, this may suggest a potential risk of lymph node
metastasis; in such cases, lobectomy coupled with systematic lymph
node dissection is recommended to ensure complete resection and to
minimize the risk of recurrence.
Cervical cancer is among the most dangerous types of
cancer in terms of female survival; it is the fourth leading cause
of cancer-associated death in women worldwide (1). Metastatic cervical cancer exhibits an
inferior 5-year survival rate compared to non-metastatic cervical
cancer, typically <20% (3,4), and
lacks standard treatment protocols. Oligometastatic cervical cancer
can be effectively managed through various treatment modalities,
including radical radiotherapy, surgical resection and systemic
therapy; among the latter, chemotherapy, such as cisplatin combined
with paclitaxel, and immunotherapy, such as bevacizumab or
pembrolizumab, are commonly used. These therapies have
significantly enhanced the survival rates of patients with
oligometastatic cervical cancer (5,6).
Cervical cancer primarily spreads through two mechanisms: Lymphatic
metastasis involving pelvic, supraclavicular, mediastinal and
para-aortic lymph nodes, and hematogenous metastasis to the lungs,
liver or brain. Typically, cervical cancer metastasizes to
neighboring tissues and organs; however, >10% of patients
develop distant extra-pelvic metastases (7). Notably, the chest, encompassing the
lungs and mediastinal lymph nodes, represents one potential site,
with the latter contributing to just 1% of metastatic cervical
cancer cases (8). Lymphatic
metastasis of cervical cancer usually occurs step by step, first
from pelvic lymph nodes to iliac common lymph nodes, then to
para-aortic lymph nodes, and it can continue to metastasize to
supraclavicular lymph nodes. Notably, skip metastasis, which refers
to metastasis that does not follow the normal direction of
lymphatic drainage step by step, but directly skips the primary
lymph node areas and occurs in the more distant lymph nodes, rarely
occurs (9). The present study
describes the rare case of primary lung adenocarcinoma with upper
mediastinal lymph node metastasis originating from early-stage
cervical squamous cell carcinoma.
Case report
A 72-year-old woman presented at the Department of
Thoracic Surgery, Union Hospital, Tongji Medical College, Huazhong
University of Science and Technology (Wuhan, China) in December
2020. A mass was discovered in their right upper lung during a
routine computed tomography (CT) scan 2 months ago. The patient had
undergone radical hysterectomy for cervical tumor at Sun Yat-sen
University Cancer Center (Guangzhou, China) in October 2018. The
postoperative pathology had revealed stage IB cervical squamous
cell carcinoma. The patient did not receive any adjuvant treatment
after surgery and had been regularly followed up. During each
follow-up, they underwent CT examinations of the lower abdomen and
pelvis, along with tumor marker tests for squamous cell carcinoma
(SCC) antigen, carcinoembryonic antigen (CEA), cancer antigen (CA)
125, and CA19-9. The results indicated no signs of metastasis or
recurrence. Given the advanced age and malignant tumor history of
the patient, comprehensive examinations were conducted after
discovery of the lung mass, including tumor marker tests,
echocardiography, CT coronary angiography and whole-body positron
emission tomography (PET)/CT. The tumor markers tested in December
2020, including CEA, SCC antigen, neuron-specific enolase-1 and
cytokeratin 19 fragment antigen 21-1, were within the normal range
(Table I). The PET/CT scan
indicated the presence of a tumor in the right superior lobe,
measuring ~1.5×1.6 cm. The tumor showed a visible cavity, increased
fluorodeoxyglucose (FDG) uptake, and a maximum standardized uptake
value (SUV) ranging from 1.5 to 2.1. No enlarged lymph nodes or
abnormal radioactive distribution were observed in the mediastinum,
and the uterus and bilateral adnexa exhibited normal postoperative
changes. No regional metabolic abnormalities were detected outside
the thoracic cavity, suggesting no malignant tumor recurrence. The
postoperative follow-up data for cervical cancer also showed no
signs of tumor recurrence. The results of preoperative CT coronary
angiography and electrocardiogram, and levels of tumor markers are
shown in Figs. S1 and S2, and Table
I, respectively.
 | Table I.Tumor markers. |
Table I.
Tumor markers.
| Marker | Result | Reference |
|---|
| CEA | 1.80 µg/ml | <5.0 µg/ml |
| SCC antigen | 1.00 ng/ml | <1.5 ng/ml |
| CYFRA 21-1 | 1.55 ng/ml | <2.5 ng/ml |
| NSE-1 | 9.60 µg/l | <16.3 µg/l |
After adequate preoperative preparation, the initial
surgical method was performance of an apical segmentectomy of the
right superior lobe and systematic lymph node dissection. The
surgery was conducted using video-assisted thoracoscopic surgery
(VATS) according to the planned approach. During the procedure,
enlarged and hardened upper mediastinal lymph nodes were observed,
which were firmly adhered to the surrounding tissues, indicating a
possible metastasis. To ensure an R0 resection and minimize the
risk of recurrence, a decision was made to instead perform a right
upper lobe resection. There was no significant hemorrhage during
the operation, and the vital signs of the patient remained stable.
A chest X-ray conducted on day 2 post-surgery revealed satisfactory
lung re-expansion (Fig. S3). The
chest tube was removed the following day, and the patient was
discharged on postoperative day 5.
Based on a comprehensive evaluation, it was
suspected that the patient had lymph node metastasis in the N2
region, suggestive of stage IIIA lung cancer (pT1bN2M0). However,
the pathology report indicated that the initial assessment was not
accurate. Although lymph node metastasis in the upper mediastinum
was confirmed, it was not metastasis of primary lung
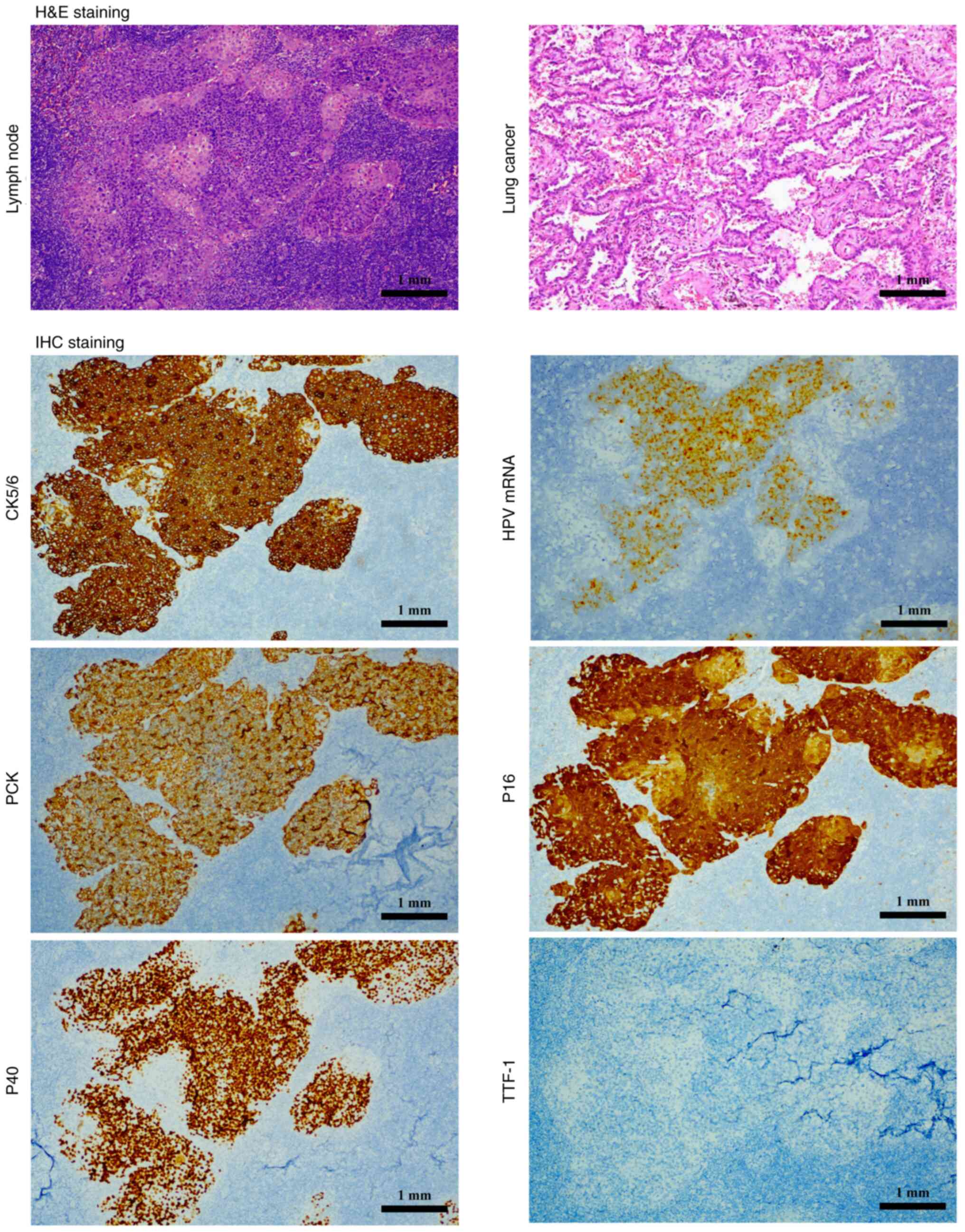
adenocarcinoma. As shown in Fig. 1,
immunohistochemical staining, performed as described previously
(10–12), exhibited positive reactions for pan
cytokeratin (CK), CK5/6 and P40, whereas thyroid transcription
factor-1 staining was negative, indicating that there was
metastasis of SCC in the lymph node. In addition, persistent human
papillomavirus (HPV) infection causes upregulation of P16 (13); therefore, P16 positivity of the
patient's specimen can be a marker for cervical lesions. As for the
protocol of hematoxylin and eosin staining, the tumor tissue was
excised and immersed in 10% formalin at room temperature for 24 h
for fixation, followed by dehydration in alcohol of increasing
concentrations. Subsequently, it was placed in xylene and embedded
in paraffin wax; the embedded wax block was fixed on a microtome
and sliced into 4-µm sections. The thin sections were then
flattened in 40°C water and adhered to microscope slides, and were
finally dried in a 60°C incubator for 3 h. The sections then
underwent a series of deparaffinization and hydration steps in a
descending series of ethanol. The sections were stained with
hematoxylin solution for 2 min, dipped briefly in hydrochloric acid
alcohol for differentiation (1 sec), and rinsed in water for
bluing. Next, they were immersed in 1% aqueous eosin stain for 2
min, followed by a quick rinse in tap water (30 sec). Subsequently,
the sections were dehydrated again in an ascending series of
ethanol. Finally, the prepared slides were observed under an
optical microscope.
Given the patient's prior history of cervical
cancer, the pathologist performed HPV mRNA in situ
hybridization using the RNAscope HPV HR18 Multi-Subtype Detection
Kit (cat. no. RS-8002; OriGene Technologies, Inc.) and HPV HR-18
probes, which encompass 18 high-risk HPV subtypes (HPV16, 18, 26,
31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73 and 82)
(14). The lymph nodes tissue was
excised and immersed in 10% formalin at room temperature for 24 h
for fixation, followed by dehydration in alcohol of increasing
concentrations. Subsequently, the tissue was placed in xylene and
embedded in paraffin wax; the embedded wax block was fixed on a
microtome and sliced into 4-µm sections. These sections were
dewaxed, followed by the addition of pepsin and heat treatment at
40°C. Each slide was then incubated with ~50 µl probe, followed by
incubation with Amplification (Amp) 1 (pre-amplifier step) for 30
min at 40°C, Amp2 (signal enhancer step) for 15 min at 40°C, Amp3
(amplifier step) for 30 min at 40°C, Amp4 (probe labeling step) for
15 min at 40°C, Amp5 for 30 min at 40°C and Amp6 for 15 min at 40°C
(signal amplifications steps), before the formation of a brown
insoluble product via HRP-catalyzed substrate reaction with DAB.
All of the Amps were included in the kit. Finally, the slides were
counterstained with hematoxylin. The results indicated that the SCC
was associated with HPV infection (Fig.
1), confirming that the metastatic cancer originated from
cervical cancer. Taking all factors into consideration, it was
concluded that the pathological staging of the patient was
IA2-stage lung adenocarcinoma combined with IVB-stage cervical
cancer. A schematic diagram of the pathway of metastasis is shown
in Fig. 2. Additionally, the PET/CT
and CT images of the patient's lung mass are shown in Fig. 2.
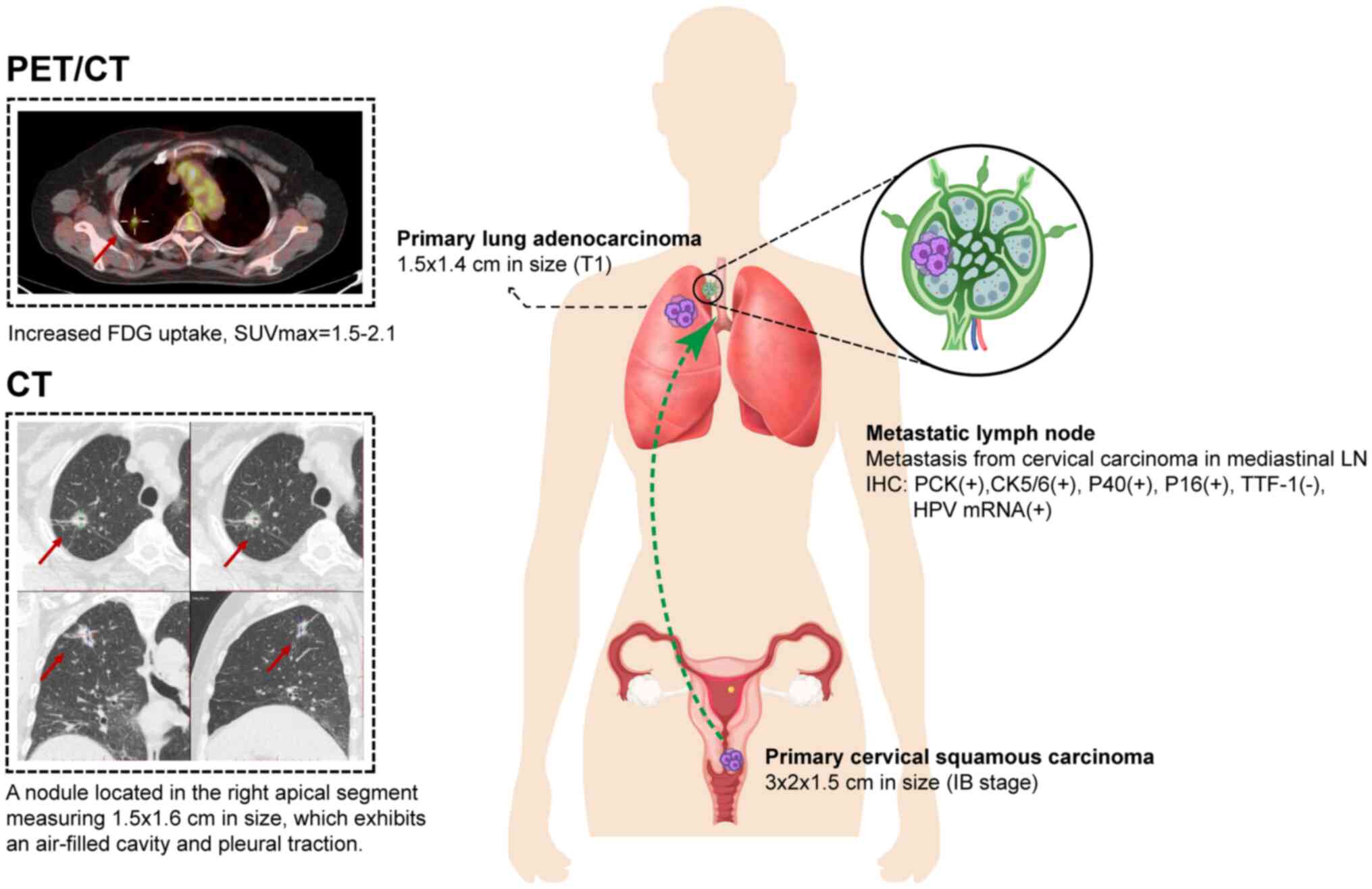 | Figure 2.Cervical cancer metastasis pathway and
preoperative PET/CT. The patient underwent radical resection of
cervical cancer in 2018, and was diagnosed with stage IB cervical
squamous cell carcinoma by postoperative pathology. In 2020, a
nodule in the right upper lung was found. Preoperative PET/CT
showed nodules of soft tissue density with a visible cavity and
abnormal FDG uptake in the apical segment of the right upper lobe,
which was considered to be a malignant tumor, and there were no
obviously enlarged LNs in the mediastinum. At the same time, no
signs of malignant tumor recurrence were found in the uterus and
bilateral adnexa, and the pathological diagnosis of an invasive
adenocarcinoma was confirmed after right upper lobectomy. CT,
computed tomography; CK, cytokeratin; FDG, fluorodeoxyglucose; HPV,
human papillomavirus; IHC, immunohistochemistry; LN, lymph node;
PET, positron emission tomography; SUVmax, maximum standardized
uptake value; TTF-1, thyroid transcription factor-1. |
Due to the rarity of this case, standardized
treatment protocols are currently unavailable. Consequently,
rigorous follow-ups have been conducted with the patient, including
chest and whole abdomen contrast-enhanced CT scans every 3 months
and PET/CT scans annually, to promptly detect any new metastases.
Additionally, multidisciplinary consultations have been organized
to devise subsequent treatment for the patient. Following
discussions with oncologists and gynecologists, it was recommended
that the patient undergo systemic chemotherapy with paclitaxel and
platinum, and external irradiation radiotherapy (dosage of 41.4 Gy
in 23 fractions) according to the National Comprehensive Cancer
Network guidelines (15). However,
due to personal factors, the patient did not undergo any
recommended adjuvant treatment. In summary, the patient underwent
surgical dissection of the oligometastatic lymph node without any
additional adjuvant treatment. During the 3-year continuous
follow-up period following surgery, there has been no recurrence of
the tumor or metastasis to other areas.
Discussion
The accurate identification of lymph node metastasis
in preoperative images is important when selecting appropriate
surgical methods for patients with lung cancer. Nevertheless,
occult lymph node metastases are clinically observed in ~20% of
cases (16). Consequently,
intraoperative assessment of lymph node morphology and texture,
coupled with the surgeon's experience, or more specifically, the
utilization of intraoperative rapid freezing techniques, is
imperative to determine the presence of metastasis and guide final
surgical decisions. However, a particular challenge emerges when
dealing with patients who have a prior history of malignant tumors,
especially when the initial primary tumor has already spread to the
same regional lymph nodes where subsequent primary tumors tend to
spread. As aforementioned, in the present case report, the patient
presented with two consecutive independent early-stage primary
tumors. Routine postoperative follow-up examinations and
pre-operative evaluations did not reveal any signs of recurrence or
distant metastasis; however, occult mediastinal lymph node
involvement from cervical cancer was eventually detected.
Retrospective studies have indicated that ~14% of early-stage
cervical cancer cases exhibit lymph node metastasis (17), whereas para-aortic lymph node
involvement ranges from 8.4 to 11.1% in stage IB (18). Moreover, mediastinal lymph node
involvement from cervical cancer is even rarer than para-aortic
lymph node involvement. For patients with lung cancer who have a
concurrent history of other tumors, if it is found that there are
lymph nodes that may be involved in metastasis during
intraoperative exploration of the chest, in addition to performing
a lobectomy instead of a segmentectomy, the clinician must also be
alert to the source of the metastatic lymph nodes, especially when
the previous tumor is still under follow-up and remains at risk of
recurrence and metastasis. Currently, based on intraoperative
frozen sections, it is possible to determine whether there is
metastasis in the lymph nodes; however, the source of the
metastasis cannot be determined.
PET/CT has a robust ability in identifying
metastasis, operating on the principle of dynamic glucose
metabolism at the lesion site (19). When a glucose-like substance labeled
with 18F-FDG is administered as an imaging agent into the human
body, the malignant tumor avidly accumulates this agent, resulting
in an elevated uptake value. This elevation enables the deduction
of the existence of metastasis. One clinical study showed that,
although FDG-PET/CT is increasingly used to assess the presence or
absence of metastases, FDG-PET/CT alone is insufficient to assess
isolated mediastinal lymph nodes in patients with cervical cancer,
with a false positive rate of 75% (20). Although PET/CT is an important tool
for lymph node staging and assessment of distant metastases,
particular caution is advisable in cases involving isolated
mediastinal involvement. It is crucial to note that positive PET/CT
results do not definitively indicate the presence of metastasis.
There is currently insufficient evidence to support the assertion
that negative PET/CT findings accurately predict the absence of
mediastinal lymph node metastasis in patients with cervical
cancer.
In addition to the lack of effective imaging
evaluation tools, mediastinal lymph node metastasis of cervical
cancer also lacks typical signs and symptoms. A previous case
report has suggested that enlargement of mediastinal lymph nodes
can lead to dysphagia, potentially indicating the presence of
metastatic lesions following surgical treatment for cervical cancer
(8). In summary, cervical cancer
with mediastinal metastasis lacks distinctive signs, symptoms and
clear imaging evidence, rendering diagnosis challenging.
Furthermore, metastasis is uncommon in early-stage cervical cancer,
making the detection of tumor recurrence particularly difficult,
even with routine follow-ups. The conventional radiological
assessment has some limitations in detecting the presence of lymph
node metastasis, including low specificity and accuracy (21–23);
however, artificial intelligence may offer a potential solution to
this challenge. Zhang et al (24) successfully developed a model that
extracts radiomic and deep learning features from both intratumoral
and peritumoral regions in cervical cancer. This model aims to
predict early recurrence risk factors, and has been shown to
achieve a maximum area under the curve value of 0.944,
demonstrating its promising predictive capabilities (24). However, it is worth noting that this
previous study was conducted retrospectively, and despite its
promising predictive performance, further validation and
confirmation of its reliability in actual clinical application are
crucial. Moreover, studies have demonstrated an association between
SCC antigen levels, the maximum SUV on PET/CT, and risk of
recurrence. Elevated levels of both SCC antigen and maximum SUV of
PET/CT may be indicative of a poorer prognosis and a heightened
risk of recurrence (25,26). Additionally, colon cancer-associated
transcript 2 has been implicated in lymph node metastasis in
cervical cancer, serving as a predictor of adverse outcomes
(27). In the future, the potential
integration of artificial intelligence biomarkers with serological
markers could provide a more comprehensive and precise foundation
for clinical decision-making. However, despite these advances,
pathology remains the gold standard, ensuring the accuracy and
reliability of diagnosis.
According to the staging criteria established by the
American Joint Committee on Cancer and the International Federation
of Gynecology and Obstetrics (28,29),
cervical cancer is classified as stage IVB when mediastinal lymph
node metastasis is present, and the optimal treatment approach for
these patients remains under exploration. Tewari et al
(30) proposed that patients with
metastatic cervical cancer can benefit from systemic chemotherapy
with cisplatin and paclitaxel, along with bevacizumab. Furthermore,
Gadducci et al (31)
indicated that combination chemotherapy based on cisplatin can have
a higher overall response rate than single agents. In addition, a
meta-analysis has suggested that combined chemotherapy is generally
more favored than single-agent treatment (32). However, some patients experience
severe side effects from cisplatin. To mitigate these side effects,
enhance safety and maintain efficacy, carboplatin may be considered
as an alternative to cisplatin (33). Case reports have highlighted a
potentially superior treatment regimen for patients with
mediastinal oligometastasis. Bonilla et al (34) presented two rare cases, which
provide some valuable insights for the treatment of mediastinal
oligometastasis: One patient with stage IB cervical cancer
presented with mediastinal metastasis and underwent mediastinal
intensity-modulated radiotherapy with a total dose of 60 Gy (2.0
Gy/fraction), along with weekly intravenous cisplatin at a dose of
40 mg/ml for 6 weeks. Notably, the patient demonstrated a favorable
prognosis and remained alive until June 2020. The second case
involved another patient who initially received 6 weeks of
chemotherapy with carboplatin and paclitaxel, followed by
mediastinal intensity-modulated radiation therapy with a dosage of
60 Gy and cisplatin administration; finally, the patient achieved a
complete response (34). Although
these are isolated case reports, they provide valuable insights for
clinical practice (32). A clinical
study conducted in Korea on oligometastatic cervical cancer
revealed that stereotactic body radiotherapy exerted a positive
impact on patients, with a disease progression-free survival (DPFS)
time of 14.3 months. Specifically, the 2- and 5-year DPFS rates
were 42.4 and 34.4%, respectively, whereas the median overall
survival (OS) time was 32.7 months. Notably, the 2-year OS rate
stood at 57.5%, surpassing the 5-year OS rate of 32.9%. Given the
rarity of mediastinal oligometastasis, the associated findings may
not conclusively demonstrate the efficacy of radiotherapy combined
with or without chemotherapy. Nevertheless, they hold significant
reference value for clinical practice (35).
Surgical management may be considered a viable
treatment option for metastatic tumors located in the mediastinum.
Kanzaki et al (36)
described two cases where patients with early-stage clear cell
renal cell carcinoma (RCC) underwent radical nephrectomy.
Subsequently, during the postoperative follow-up period, both
patients were diagnosed with mediastinal masses, which were
successfully resected through a minimally invasive thoracotomy
approach. Intraoperative rapid pathological examination confirmed
that the metastases were derived from clear cell RCC. Notably,
neither patient received adjuvant therapy following surgery. One of
the patients developed pulmonary and lymphatic metastases 5 years
after the initial procedure but survived until the last follow-up,
having responded well to treatment with interferon α (34). Furthermore, Lin et al
(37) presented a case study of a
patient with early-stage RCC who subsequently developed posterior
mediastinal lymphatic metastasis following radical nephrectomy. The
patient was diagnosed with Castleman's disease and underwent VATS.
Postoperative pathology confirmed that the metastasis originated
from clear cell RCC. The patient did not receive any treatment
after surgery, and remained free of recurrence and metastasis at
the 10-month follow-up (37). These
studies indicate that surgical management of isolated mediastinal
lymph node metastases arising from clear cell RCC may offer a
potentially effective treatment option. However, Mori et al
(38) reported on a unique case
involving a patient with lung squamous cell carcinoma who also
suffered from mediastinal lymph node metastasis from RCC. Notably,
despite surgery, the patient developed metastasis to the left
inferior paratracheal lymph node after 4 months, necessitating
radiotherapy (60 Gy) and immunotherapy. Despite this, the patient
maintained a good condition at the 10-month follow-up. This case
underscores that surgical resection alone may not be sufficient in
certain instances, and the employment of adjunctive therapies may
be necessary to optimize patient survival outcomes (38). The present case is akin to the
aforementioned studies, featuring isolated mediastinal lymph node
metastasis in early-stage cancer. Nevertheless, the precise
effectiveness of surgical treatment for mediastinal metastasis
stemming from cervical cancer remains an area requiring further
investigation and elucidation.
The immune system serves a critical role in
combating cancer, as tumors often manipulate the immune system to
evade detection. Immune therapy has transformed cancer treatment by
repairing the immune-escape defect. Broadly defined, immune therapy
encompasses active and passive immunization strategies that
directly target tumors based on immune mechanisms. Immune
checkpoint therapy has made revolutionary advances in cancer
treatment, fundamentally changing the way cancer is viewed and
treated. Additionally, the immune system can impact cancer
treatment outcomes (39).
Specifically, in the present case report, a patient underwent
radical hysterectomy for cervical cancer, and pathological analysis
revealed early-stage cervical cancer with no signs of recurrence
detected after surgery. Skip metastasis for IB cervical cancer is
rare; however, in this case, the patient developed metastasis in
upper mediastinal lymph nodes 2 years later. Hence, it may be
hypothesized that secondary malignancies can potentially exert an
influence on the immune system, altering the immune
microenvironment and potentially triggering the reactivation of the
previously suppressed primary tumor. This reactivation can
ultimately lead to recurrence or metastasis. Tumor cells are
well-known modulators of immune activity, and macrophages, for
instance, can adapt to different environments, primarily
transforming into M1 or M2 subsets. The majority of macrophages
found within tumor tissues belong to the M2 subtype, which tends to
suppress immune responses and facilitate tumor growth.
Tumor-associated macrophages, a subtype of M2 macrophages, have
been demonstrated to secrete cytokines, such as IL-10, PGE2 and
TGFβ, participating in tumor immune evasion and various biological
activities (40). Nevertheless, it
is important to note that these findings represent a preliminary
hypothesis, and further rigorous experiments are required to
validate and consolidate the understanding of these complex
interactions.
The present case report exhibits some limitations.
Firstly, the patient solely underwent surgical resection without
receiving any adjuvant therapy, which undoubtedly affects the
comprehensiveness and reliability of the treatment outcomes.
Secondly, given that there is only one case described, its use in
the guidance for the treatment of similar patients may have certain
constraints.
In conclusion, the present case report describes a
patient who was diagnosed with a primary lung adenocarcinoma that
was accompanied by mediastinal lymph node metastasis, which
originated from early-stage cervical squamous cell carcinoma. For
patients with lung cancer and concurrent malignancies, metastatic
lymph nodes discovered during surgery may originate from the
previous malignancy. Surgical management of oligometastatic lymph
nodes in the mediastinum can be a potential therapeutic option,
albeit one that may necessitate the integration of adjuvant
treatment modalities as warranted by the individual case.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This work was supported by the Grant of National Natural Science
Foundation of China (grant no. 82303353).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
CZ and QFH conceived and designed the study. GCY,
XJW and YH collected all relevant clinical, laboratory and imaging
data. YDL interpreted all relevant data in the present case. CZ,
QFH, GCY and YDL prepared the manuscript. CZ, QFH and YDL confirm
the authenticity of all the raw data. All authors read and approved
the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and the accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
JCOG
|
Japan Clinical Oncology Group
|
|
PET/CT
|
positron emission tomography/computed
tomography
|
|
SUV
|
standardized uptake value
|
|
VATS
|
video-assisted thoracoscopic
surgery
|
|
SCC
|
squamous cell carcinoma
|
|
DPFS
|
disease progression-free survival
|
|
OS
|
overall survival
|
|
RCC
|
renal cell carcinoma
|
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Saji H, Okada M, Tsuboi M, Nakajima R,
Suzuki K, Aokage K, Aoki T, Okami J, Yoshino I, Ito H, et al:
Segmentectomy versus lobectomy in small-sized peripheral
non-small-cell lung cancer (JCOG0802/WJOG4607L): A multicentre,
open-label, phase 3, randomised, controlled, non-inferiority trial.
Lancet. 399:1607–1617. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
van Meir H, Kenter GG, Burggraaf J, Kroep
JR, Welters MJ, Melief CJ, van der Burg SH and van Poelgeest MI:
The need for improvement of the treatment of advanced and
metastatic cervical cancer, the rationale for combined
chemo-immunotherapy. Anticancer Agents Med Chem. 14:190–203. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Perkins V, Moore K, Vesely S, Matsuo K,
Mostofizadeh S, Sims TT, Lea J, Barnes D, Chen S, Carlson M, et al:
Incorporation of whole pelvic radiation into treatment of stage IVB
cervical cancer: A novel treatment strategy. Gynecol Oncol.
156:100–106. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chopra S, Mangaj A, Sharma A, Tan LT,
Sturdza A, Jürgenliemk-Schulz I, Han K, Huang F, Schmid MP, Fokdal
L, et al: Management of oligo-metastatic and oligo-recurrent
cervical cancer: A pattern of care survey within the EMBRACE
research network. Radiother Oncol. 155:151–159. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mangaj A, Chopra S and Nout RA: Defining
the role of high-dose radiation in oligometastatic &
oligorecurrent cervical cancer. Indian J Med Res. 154:303–318.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Grigsby PW, Siegel BA and Dehdashti F:
Lymph node staging by positron emission tomography in patients with
carcinoma of the cervix. J Clin Oncol. 19:3745–3749. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Singh V, Gor D, Azad S, Ricca A, Xu Y and
Meghal T: Dysphagia as a rare presentation of cervical cancer with
mediastinal metastasis. Eur J Case Rep Intern Med.
9:0031362022.PubMed/NCBI
|
|
9
|
Plentl AA and Friedman EA: Lymphatic
system of the female genitalia. The morphologic basis of oncologic
diagnosis and therapy. Major Probl Obstet Gynecol. 2:1–223.
1971.PubMed/NCBI
|
|
10
|
Shibayama T, Hayashi A, Toki M, Kitahama
K, Ho YJ, Kato K, Yamada T, Kawamoto S, Kambayashi K, Ochiai K, et
al: Combination immunohistochemistry for CK5/6, p63, GATA6, and
HNF4a predicts clinical outcome in treatment-naïve pancreatic
ductal adenocarcinoma. Sci Rep. 14:155982024. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vahadane A, Sharma S, Mandal D, Dabbeeru
M, Jakthong J, Garcia-Guzman M, Majumdar S and Lee CW: Development
of an automated combined positive score prediction pipeline using
artificial intelligence on multiplexed immunofluorescence images.
Comput Biol Med. 152:1063372023. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Xu QQ, Li QJ, Xu Z, Lan LL, Hou Z, Liu J,
Lu L, Chen YY, Chen RZ and Wen X: Prognostic value of the
immunohistochemical score based on four markers in head and neck
squamous cell carcinoma. Front Immunol. 14:10768902023. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Benevolo M, Mottolese M, Marandino F,
Vocaturo G, Sindico R, Piperno G, Mariani L, Sperduti I, Canalini
P, Donnorso RP and Vocaturo A: Immunohistochemical expression of
p16(INK4a) is predictive of HR-HPV infection in cervical low-grade
lesions. Mod Pathol. 19:384–391. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Evans MF, Peng Z, Clark KM, Adamson CS, Ma
XJ, Wu X, Wang H, Luo Y and Cooper K: HPV E6/E7 RNA in situ
hybridization signal patterns as biomarkers of three-tier cervical
intraepithelial neoplasia grade. PLoS One. 9:e911422014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Abu-Rustum NR, Yashar CM, Bean S, Bradley
K, Campos SM, Chon HS, Chu C, Cohn D, Crispens MA, Damast S, et al:
NCCN guidelines insights: Cervical cancer, version 1.2020. J Natl
Compr Canc Netw. 18:660–666. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Beyaz F, Verhoeven RLJ, Schuurbiers OCJ,
Verhagen AFTM and van der Heijden EHFM: Occult lymph node
metastases in clinical N0/N1 NSCLC; A single center in-depth
analysis. Lung Cancer. 150:186–194. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Du R, Li L, Ma S, Tan X, Zhong S and Wu M:
Lymph nodes metastasis in cervical cancer: Incidences, risk
factors, consequences and imaging evaluations. Asia Pac J Clin
Oncol. 14:e380–e385. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Han X, Wen H, Ju X, Chen X, Ke G, Zhou Y,
Li J, Xia L, Tang J, Liang S and Wu X: Predictive factors of
para-aortic lymph nodes metastasis in cervical cancer patients: A
retrospective analysis based on 723 para-aortic lymphadenectomy
cases. Oncotarget. 8:51840–51847. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ming Y and Wu N, Qian T, Li X, Wan DQ, Li
C, Li Y, Wu Z, Wang X, Liu J and Wu N: Progress and future trends
in PET/CT and PET/MRI molecular imaging approaches for breast
cancer. Front Oncol. 10:13012020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Onal C, Oymak E, Findikcioglu A and Reyhan
M: Isolated mediastinal lymph node false positivity of
[18F]-fluorodeoxyglucose-positron emission tomography/computed
tomography in patients with cervical cancer. Int J Gynecol Cancer.
23:337–342. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Noji T, Kondo S, Hirano S, Tanaka E,
Suzuki O and Shichinohe T: Computed tomography evaluation of
regional lymph node metastases in patients with biliary cancer. Br
J Surg. 95:92–96. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
22
|
Liu J, Wang Z, Shao H, Qu D, Liu J and Yao
L: Improving CT detection sensitivity for nodal metastases in
oesophageal cancer with combination of smaller size and lymph node
axial ratio. Eur Radiol. 28:188–195. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
King MJ, Hectors S, Lee KM, Omidele O,
Babb JS, Schwartz M, Tabrizian P, Taouli B and Lewis S: Outcomes
assessment in intrahepatic cholangiocarcinoma using qualitative and
quantitative imaging features. Cancer Imaging. 20:432020.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang Y, Wu C, Du J, Xiao Z, Lv F and Liu
Y: Prediction of recurrence risk factors in patients with
early-stage cervical cancers by nomogram based on MRI handcrafted
radiomics features and deep learning features: A dual-center study.
Abdom Radiol (NY). 49:258–270. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nakamura K, Okumura Y, Kodama J, Hongo A,
Kanazawa S and Hiramatsu Y: The predictive value of measurement of
SUVmax and SCC-antigen in patients with pretreatment of primary
squamous cell carcinoma of cervix. Gynecol Oncol. 119:81–86. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fu J, Wang W, Wang Y, Liu C and Wang P:
The role of squamous cell carcinoma antigen (SCC Ag) in outcome
prediction after concurrent chemoradiotherapy and treatment
decisions for patients with cervical cancer. Radiat Oncol.
14:1462019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cao X, Yao J, Jia M, Shen X, Zhang J and
Ju S: Serum CCAT2 as a biomarker for adjuvant diagnosis and
prognostic prediction of cervical cancer. J Ovarian Res. 15:202022.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Olawaiye AB, Baker TP, Washington MK and
Mutch DG: The new (version 9) American joint committee on cancer
tumor, node, metastasis staging for cervical cancer. CA Cancer J
Clin. 71:287–298. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Saleh M, Virarkar M, Javadi S, Elsherif
SB, de Castro Faria S and Bhosale P: Cervical cancer: 2018 revised
international federation of gynecology and obstetrics staging
system and the role of imaging. AJR Am J Roentgenol. 214:1182–1195.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tewari KS, Sill MW, Long HJ 3rd, Penson
RT, Huang H, Ramondetta LM, Landrum LM, Oaknin A, Reid TJ, Leitai
MM, et al: Improved survival with bevacizumab in advanced cervical
cancer. N Engl J Med. 370:734–743. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gadducci A, Tana R, Cosio S and Cionini L:
Treatment options in recurrent cervical cancer (Review). Oncol
Lett. 1:3–11. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Scatchard K, Forrest JL, Flubacher M,
Cornes P and Williams C: Chemotherapy for metastatic and recurrent
cervical cancer. Cochrane Database Syst Rev.
10:CD0064692012.PubMed/NCBI
|
|
33
|
Kitagawa R, Katsumata N, Shibata T, Kamura
T, Kasamatsu T, Nakanishi T, Nishimura S, Ushijima K, Takano M,
Satoh T and Yoshikawa H: Paclitaxel plus carboplatin versus
paclitaxel plus cisplatin in metastatic or recurrent cervical
cancer: The open-label randomized phase III trial JCOG0505. J Clin
Oncol. 33:2129–2135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bonilla CE, Zapata Laguado M and Paez
Quintero H: Concurrent chemoradiation for mediastinal
oligometastases from cervical cancer: A potentially curative
treatment. Cureus. 12:e105962020.PubMed/NCBI
|
|
35
|
Park HJ, Chang AR, Seo Y, Cho CK, Jang WI,
Kim MS and Choi C: Stereotactic body radiotherapy for recurrent or
oligometastatic uterine cervix cancer: A cooperative study of the
Korean radiation oncology group (KROG 14-11). Anticancer Res.
35:5103–5110. 2015.PubMed/NCBI
|
|
36
|
Kanzaki R, Higashiyama M, Okami J and
Kodama K: Surgical treatment for patients with solitary metastasis
in the mediastinal lymph node from renal cell carcinoma. Interact
Cardiovasc Thorac Surg. 8:485–487. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lin H, Zhang H, Cheng Y and Zhang C:
Solitary metastasis in the mediastinal lymph node after radical
nephrectomy for clear cell renal cell carcinoma: A case report and
literature review. Front Oncol. 10:5931422020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mori Y, Sano Y, Sugimoto R, Sakao N, Ryuko
T, Takeda M, Kitazawa R, Yukumi S and Izutani H: Mediastinal and
hilar lymph node metastases from renal cell carcinoma with
concomitant lung carcinoma: A rare case with unique diagnostic
challenges. Acta Med Okayama. 76:225–228. 2022.PubMed/NCBI
|
|
39
|
Disis ML: Mechanism of action of
immunotherapy. Semin Oncol. 41 (Suppl 5):S3–S13. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chen Y, Song Y, Du W, Gong L, Chang H and
Zou Z: Tumor-associated macrophages: An accomplice in solid tumor
progression. J Biomed Sci. 26:782019. View Article : Google Scholar : PubMed/NCBI
|