Introduction
Neoadjuvant systemic therapy, either chemotherapy or
anti-hormonal therapy, is increasingly used as a first-line
therapeutic option in patients with locally advanced operable,
primarily non-operable and inflammatory primary breast cancer since
it may lead to a local downstage of the primary tumor, thus
increasing the rate of conservative surgical treatments (1).
Neoadjuvant therapy may also sterilize sites of
local and distant metastases and improve long-term and disease-free
survival (2).
Moreover, it offers the possibility of assessing
early in vivo tumor-response to systemic treatments, guiding
the oncologist in selecting the most appropriate post-surgical
therapies, since the degree of response to neoadjuvant therapy
represents an important prognostic factor (3).
Therefore, it is crucial to have an imaging method
able to predict and quantify tumor response to neoadjuvant
therapy.
The response of the primary tumor to neoadjuvant
treatment is generally assessed by both clinical examination and
conventional imaging procedures, such as mammography and breast
ultrasonography, which however rely only on changes in size or
morphological characteristics, demonstrating inherent limitations
in differentiating residual tumors from fibrotic replacement and
over or underestimating residual disease extent (4).
Radioisotopic imaging of the breast (breast
scintigraphy or scintimammography) with the technetium-labelled
cationic lipophilic radiotracers sestamibi and tetrofosmin provides
functional imaging, selectively identifying viable tumors and
increasing the specificity of morphological imaging methods
(5–7). Radiotracer uptake and accumulation in
neoplastic cells indeed depend on vascular, biochemical and
metabolic factors such as regional blood flow, angiogenesis, plasma
and mitochondrial membrane potential as well as tissue metabolism
(8–10).
However, scintimammography, when acquired with a
conventional general-purpose gamma camera, is recognized to have a
low sensitivity in the detection of primary breast carcinomas,
especially when lesions are non-palpable and subcentimetric, due to
the limited spatial resolution of the device (11,12).
At present, this limitation may be overcome with the
employment of high-resolution, small-field of view gamma-cameras
specifically designed for the imaging of the breasts (13). This imaging procedure, namely breast
specific gamma imaging (BSGI) or molecular breast imaging (MBI),
has been demonstrated to be more sensitive than conventional breast
scintigraphy, especially in detecting small size primary breast
carcinomas, while maintaining the same high specificity (14).
In clinical practice, MBI has been established to be
able to play an important complementary role to mammography in the
diagnosis of primary breast cancer, especially in indeterminate or
inconclusive mammography findings, increasing mammography
sensitivity in dense breast and in multifocal/multicentric disease
(15–18). MBI has also demonstrated similar
high sensitivity values as mammography in the detection of ductal
carcinoma in situ, irrespective of histological subtype, and
with a scintigraphic pattern of uptake that correlated well with
mammography findings (19).
Moreover, in some studies, MBI has provided a better
preoperative local staging than mammography, altering surgical
management and guiding the surgeon to a more appropriate surgical
treatment (17,18,20).
MBI acquired with the newly developed dual-headed
cadmium-zinc-telluride (CdZnTe or CZT) devices at a reduced
radiation dose, has also proved to be able to increase the
sensitivity of mammography in screening women with mammographically
dense breast, yielding a supplemental cancer detection rate of
8.8/1,000 screened women (21).
In the present study we retrospectively assessed the
usefulness of MBI in predicting complete tumor response to
treatment and residual tumor extent following neoadjuvant therapy
in a consecutive series of patients with large or locally advanced
primary breast cancer using surgical histopathological findings as
the gold standard.
Materials and methods
Patients
We retrospectively reviewed a consecutive series of
43 female patients with large or locally advanced primary breast
cancer scheduled to receive neoadjuvant therapy who preoperatively,
at the end of their neoadjuvant treatment regimen, were submitted
to MBI. All patients were followed by the same team of oncologists
who at baseline, before starting neoadjuvant therapy, submitted
patients to local (breast and axillary) clinical examination,
conventional diagnostic imaging procedures (including mammography
and breast ultrasonography) and tumor biopsy to assess histological
type, nuclear grade and the level of expression of estrogen
receptor (ER), progesterone receptor (PR) and HER2/neu
receptor. Ki-67 (MIB1) index of tumor proliferation was also
assessed on biopsy samples. Tumors were classified in three
molecular subtypes according to their receptor status: luminal
(ER+ or PR+), HER2 (ER−,
PR− and HER2/neu+), and
triple-negative (ER−, PR− and
HER2/neu−). MBI was performed also at baseline,
before starting the neoadjuvant treatment. All investigations were
performed in a University Hospital setting, as part of the clinical
care of breast cancer patients.
According to clinical, imaging and biopsy data,
35/43 patients were scheduled to receive neoadjuvant chemotherapy:
a cisplatin-based therapy in 19 cases and an anthracycline-based
therapy in 26 cases (plus paclitaxel in 10/26 cases); 6/35 patients
were also treated with trastuzumab. The remaining 8/43 patients,
all elderly in the post-menopausal phase and with ER-positive
tumors, were submitted to anti-hormonal treatment with the
aromatase inhibitor exemestane.
At the end of the neoadjuvant treatment, all
patients underwent breast surgery that was planned and performed by
the same team of surgeons. A total of 30/43 patients underwent a
mastectomy and 13/43 patients had breast-conserving surgery (BCS).
Axillary lymph node dissection (ALND) was also performed in 38/43
cases, while ALND was avoided in the remaining 5/43 patients, all
elderly, submitted to anti-hormonal therapy and with clinically
negative axillary lymph nodes.
Patients with concomitant distant metastases
ascertained at standard staging diagnostic procedures (chest
computed tomography, bone scan and abdomen ultrasound or computed
tomography) and patients scheduled for concomitant radiotherapy
were excluded from this study.
The clinicopathological characteristics of the 43
patients enrolled in the study are listed in Table I. The baseline clinical tumor (T)
and lymph node (N) classification was performed according to the
American Joint Committee on Cancer Criteria.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
|
Characteristics | No. of
patients |
|---|
| Age at diagnosis
(years) |
|
|
<50 | 10 |
|
≥50 | 33 |
| Menopausal
status |
|
|
Pre-menopausal | 17 |
|
Post-menopausal | 26 |
| Clinical TN
stage |
|
|
IIA | 24 |
|
IIB | 5 |
|
IIIA | 7 |
|
IIIB | 7 |
| Tumor
histology |
|
|
Invasive ductal | 36 |
|
Invasive lobular | 3 |
|
Invasive mucinous | 1 |
|
Tubular | 1 |
|
Epithelial | 1 |
|
Metaplastic | 1 |
| Molecular
subtype |
|
|
Luminal | 29 |
|
HER2 | 6 |
|
Triple-negative | 8 |
| Neoadjuvant
treatment |
|
|
Chemotherapy | 29 |
|
Chemotherapy plus
trastuzumab | 6 |
|
Anti-hormonal | 8 |
Breast scintigraphy
MBI was performed 10 min after the intravenous
injection of 740 MBq of 99mTc-tetrofosmin (Myoview; GE
Healthcare, Oslo, Norway) in the arm contralateral to the affected
breast. Radiolabelling and quality control procedures of the
radiotracer were carried out according to the manufacturer's
instructions. Labelling efficiency was always >95%. Breast
images were acquired using a high-resolution, solid-state dedicated
breast camera that is composed of a semiconductor detector with a
pixelated array of CZT coupled to an array of amplifiers, the
signals from which are conveyed on an electronic readout board. The
system is modelled to have an intrinsic spatial resolution of 1.6
mm and an energy resolution of <5%. In all cases the breast
images were acquired in both craniocaudal and mediolateral oblique
projections (600 sec/view), using a 128×128 matrix size, with mild
breast compression during acquisition. Additional projections could
be acquired when necessary (such as breasts bigger than the field
of view and areas of increased uptake at the border of the field of
view). Written informed patient consent was always obtained before
the scintigraphy.
Data analysis
MBI images were independently evaluated by two
experienced nuclear medicine physicians (AS and GM) who were
blinded to the final histopathological findings that represented
the gold standard. Disagreements were resolved by consensus.
MBI images were considered negative for residual
tumors in the absence of detectable uptake on the post-therapy scan
while they were considered positive in the presence of one or more
areas (either focal or patchy) of increased uptake (mild, moderate
or intense) at the level of the primary tumor site well distinct
from background breast activity. In presence of a focal area of
increased uptake with well-delineated contours, lesion size was
assessed manually using an image function present in the Xeleris
2.0 Workstation System (GE Healthcare) available in our Nuclear
Medicine Unit. The size was determined according to the largest
diameter measured on mediolateral oblique and craniocaudal
images.
MBI results were related to the histopathological
findings obtained from surgical samples.
Histopathology
Histopathological analysis was performed according
to standard procedures. A macroscopic analysis was performed with
the size of residual tumors determined according to the largest
diameter. According to the number of tumor foci, the carcinomas
were classified as unifocal (only one focus) or
multifocal/multicentric (two or more tumor foci within a single
breast or within different quadrants of the same breast). Breast
surgical specimens were then fixed in 10% buffered formalin and
stained with haematoxylin and eosin (H&E). A further
histochemical analysis was performed with microscopic
evaluation.
The pathological response to neoadjuvant therapy was
classified as follows: complete response, disappearance in surgical
specimens of target lesions observed at the baseline mammography;
partial response, at least a 30% decrease in the diameter of target
lesions, adopting as the reference the baseline mammographic
diameter; progressive disease, at least a 20% increase in the
diameter of target lesions; stable disease, neither sufficient
shrinkage to qualify for partial response nor sufficient increase
to qualify for progressive disease.
Statistical analysis
Post-therapy images obtained using MBI were
considered as positive, negative, false-positive or false-negative
for residual breast tumors considering the histopathological
findings obtained at surgery as the ‘gold standard’. Sensitivity,
specificity, positive predictive value (PPV), negative predictive
value (NPV) and accuracy were then calculated. The Spearman's
correlation coefficient was calculated to analyze the residual
tumor size with MBI and histopathological examination.
Results
Seven out of 43 patients (16.3%), 6 following chemo-
and 1 following anti-hormonal therapy, exhibited a pathological
complete response, while the remaining 36/43 patients (83.7%), 29
following chemo- and 7 following anti-hormonal therapy, were
classified as partial responders (28 cases) or with
stable/progressive disease (8 cases) and had residual tumors at
surgery. The latter was unifocal in 27/36 cases and
multicentric/multifocal in the remaining 9/36 cases.
The 27 unifocal residual tumors included 25 invasive
ductal carcinomas, 1 mucinous and 1 metaplastic carcinoma, and
ranged in size from 1.0 to 7.0 cm, with a mean lesion size of
2.411±2.361 cm at histopathological analysis.
The histopathological findings regarding the 9
patients with multifocal/multicentric residual disease, including
tumor histology, number of lesions and lesion size, are listed in
Table II.
| Table II.Histopathological findings regarding
the 9 patients with multifocal/multicentric residual tumors. |
Table II.
Histopathological findings regarding
the 9 patients with multifocal/multicentric residual tumors.
| Tumor histology
(no. of patients) | No. of lesions and
lesion size |
|---|
| Invasive ductal
plus invasive lobular (n=1) | 1 focus 5 cm |
|
| 1 focus 1.5 cm |
| Invasive ductal
(n=1) | 2 foci 1.5 and 1.2
cm, respectively |
| Invasive lobular
(n=3) | Diffuse microscopic
foci (1 case) |
|
| Multiple
microscopic foci scattered in a 4-cm area (1 case) |
|
| Multiple
microscopic foci scattered in a 1.5-cm area (1 case) |
| Poor differentiated
DCSIS and small invasive carcinoma (n=1) | Rare microscopic
foci scattered in a fibrotic 3-cm area |
| Epithelial
carcinoma (n=1) | Multiple
microscopic foci scattered in a fibrotic 1-cm area |
| Tubular carcinoma
(n=1) | Multifocal
microscopic foci with a total extension of 4 cm |
| Invasive ductal
mixed with DCIS (n=1) | Multiple
microscopic foci scattered in a fibrotic 1-cm area |
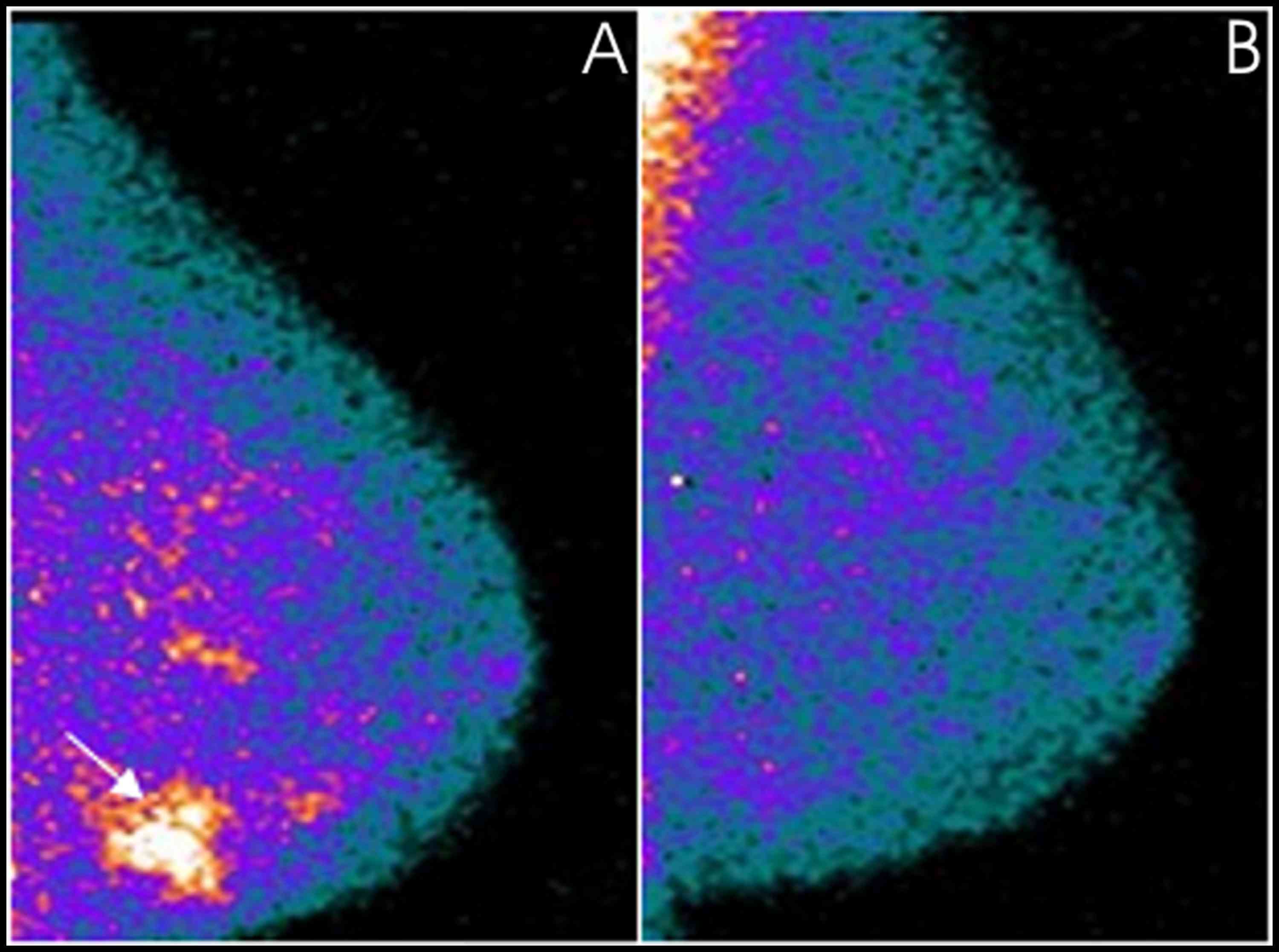
From the images obtained using MBI, 7 patients were
negative for residual tumors with pathological complete response,
demonstrating a complete disappearance of radiotracer uptake on the
post-therapy scan (one of these cases is illustrated in Fig. 1), while 34/36 patients were positive
for residual tumors. Sensitivity, specificity, PPV, NPV and
accuracy values are reported in Table
III.
| Table III.MBI results in residual breast cancer
detection after neoadjuvant therapy in the 43 patients enrolled in
the study, 7 without and 36 with residual disease after neoadjuvant
therapy. |
Table III.
MBI results in residual breast cancer
detection after neoadjuvant therapy in the 43 patients enrolled in
the study, 7 without and 36 with residual disease after neoadjuvant
therapy.
| Parameters | Data |
|---|
| Negative | 7 |
| False-positive | 0 |
| Positive | 34 |
| False-negative | 2 |
| Sensitivity | 94.4% (34/36) |
| Specificity | 100% (7/7) |
| Accuracy | 95.3% (41/43) |
| Positive predictive
value | 100% (34/34) |
| Negative predictive
value | 77.8% (7/9) |
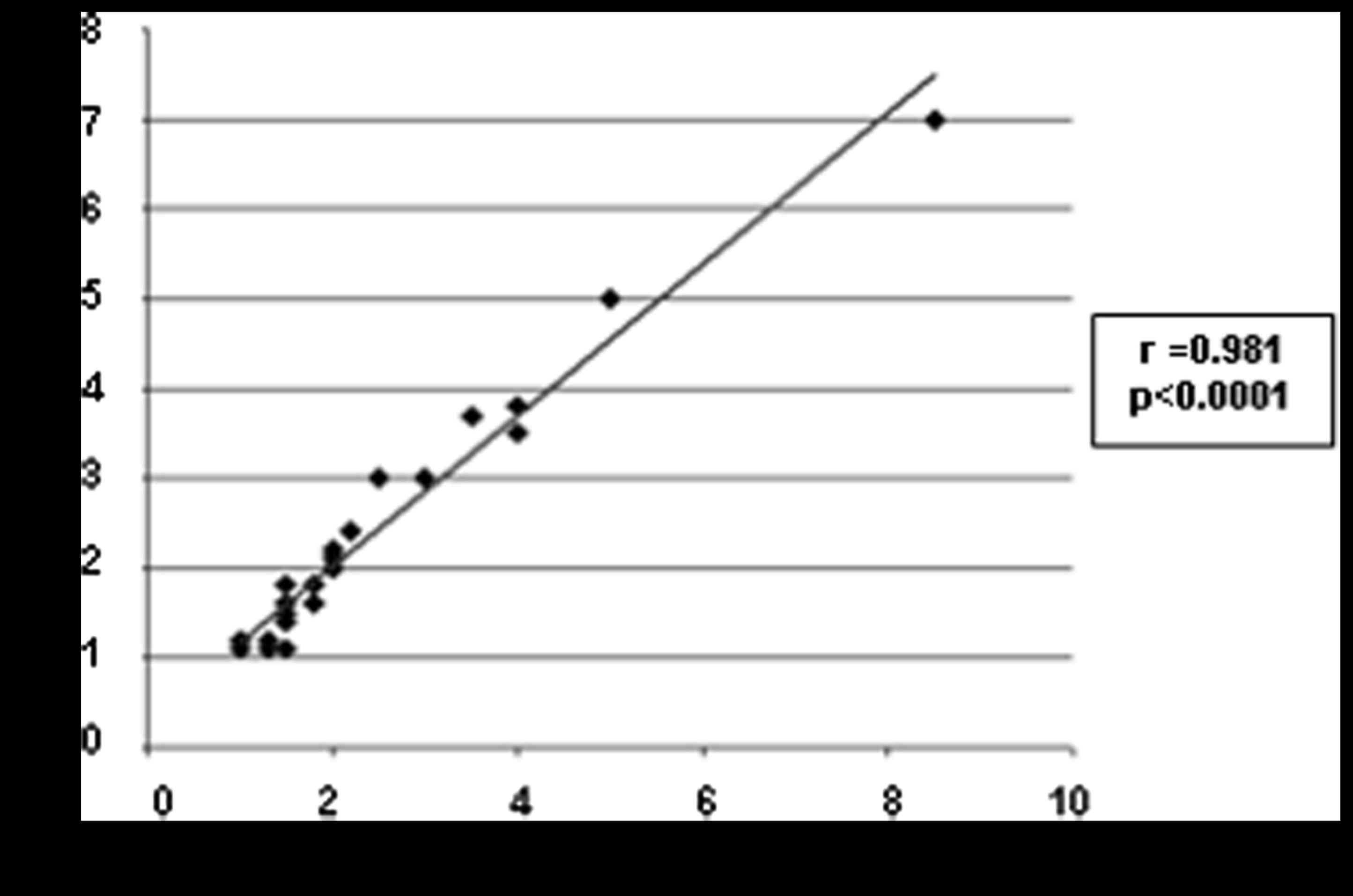
MBI detected 26/27 unifocal residues and failed in
the detection of one 2.5-cm invasive ductal carcinoma deeply
located in the internal mammary quadrant of the left breast,
excluded from the field of view during acquisition. The 26 positive
unifocal residual tumors appeared in MBI as focal areas of intense
increased uptake of the radiotracer with well-delineated contours,
with a mean lesion size of 2.361±1.374 cm. Scatter diagram and the
correlation of tumor size between MBI and histopathology is shown
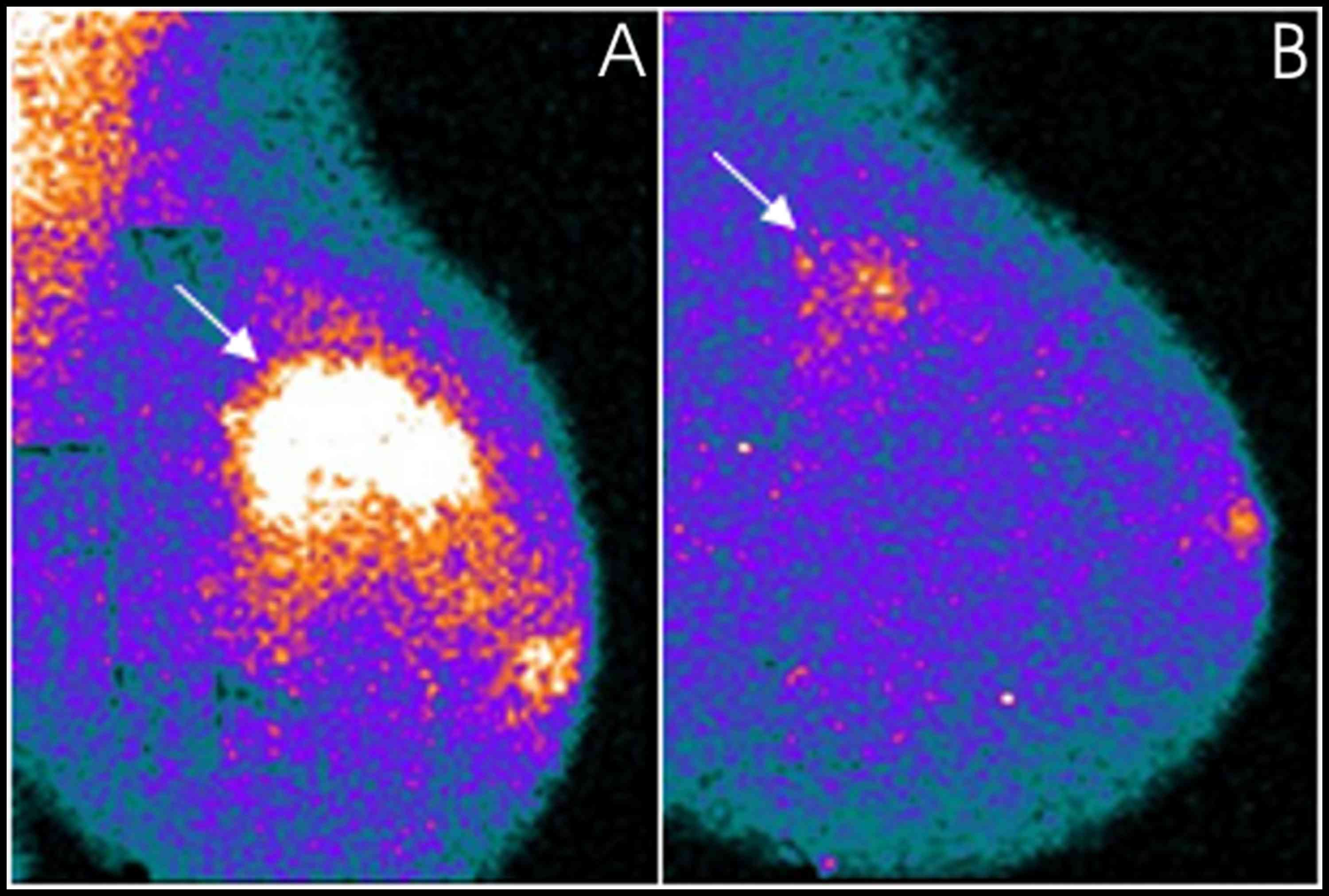
in Fig. 2. One of the patients with
unifocal residual tumors correctly visualized and assessed in size
with MBI is illustrated in Fig. 3.
MBI was in agreement with surgery in identifying only one lesion in
25/26 positive cases; in the remaining patients, MBI correctly
identified and assessed the size of the residual tumor ascertained
at surgery (a 2-cm invasive ductal carcinoma) but overestimated
disease extent also identifying two small focal areas of increased
uptake surrounding the residual tumor.
Moreover, MBI was positive in 8/9
multicentric/multifical residual tumors and false-negative in one
patient with rare microscopic foci of epithelial carcinoma (luminal
subtype, MIB1: 15%) scattered in a fibrotic area 1-cm large. MBI
findings were concordant with histopathological analysis in
assessing the number of lesions and lesion size in the patient with
one large focus (5 cm) of invasive ductal carcinoma and one smaller
focus (1.5 cm) of invasive lobular carcinoma, while it
overestimated the number of lesions in the other patient with 2
surgically proven foci of invasive ductal carcinoma. In the
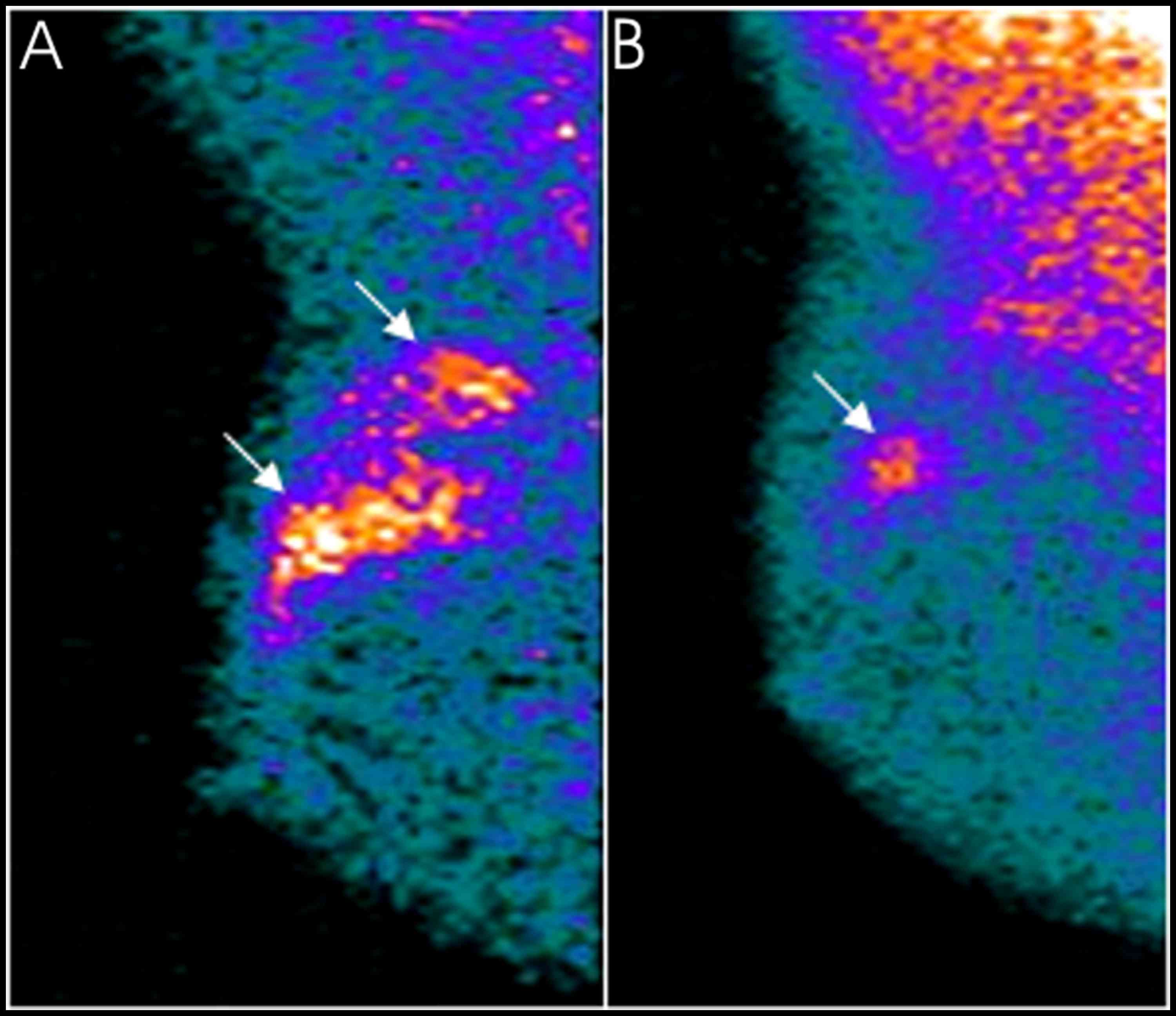
remaining 6/8 positive patients with microscopic
multifocal/multicentric tumoral foci, MBI revealed patchy areas
with irregular borders of radiotracer uptake of mild to moderate
intensity at the level of the residual disease. The largest
diameter of these areas was in agrrement with histopathological
analysis in 4/6 cases (one of these cases is shown in Fig. 4), while in the remaining 2/6 cases,
one with a multicentric invasive lobular carcinoma (luminal
subtype, MIB1: 3%) and one with rare microscopic foci of tubular
carcinoma (luminal subtype, MIB1: 8%), both scattered in a fibrotic
area of 4 cm in size, tumor extent was underestimated with MBI by 1
and by 1.5 cm, respectively.
Collectively, excluding the 2 false-negative
patients and the 4 overestimated or underestimated cases, MBI
findings were concordant with histopathological data in correctly
predicting complete response to treatment and residual tumor extent
in 37 of the 43 patients (86%) enrolled in the study.
Discussion
The recent development of high-resolution,
small-field of view dedicated breast cameras has opened a new era
for the radioisotopic imaging of the breasts with the
technetium-labelled cationic lipophilic radiotracers sestamibi and
tetrofosmin.
The advantages offered by these new devices in
respect to conventional general-purpose gamma cameras are numerous.
First of all, they offer the possibility of focalising the imaging
to the breast that is placed directly on the camera face, excluding
from the field of view the nearby organs that physiologically
accumulate on the radiotracer (i.e., liver and heart); this permits
the acquirement of images in projections similar to those of
mammography facilitating the correlation between the two types of
images (22).
Moreover, dedicated breast cameras are characterized
by a significantly higher intrinsic spatial resolution, especially
when solid-state semiconductor CZT devices are employed, increasing
the capacity of detecting subcentimetric lesions. Using the more
recently available dual-headed CZT breast cameras, that are
characterized by optimized collimation and a wide energy window,
sensitivity can be further increased and the administered dose of
radiotracer may be reduced minimizing radiation exposure to
patients (23,24).
Due to the aforementioned favourable
characteristics, MBI is now considered the radioisotopic imaging
method of choice in the diagnosis of primary breast cancer,
replacing conventional planar scintimammography.
The possible role of MBI in monitoring the local
response of breast cancer to neoadjuvant therapy is still under
investigation. At present, only a few studies have been reported in
literature focusing on this matter. Moreover, these studies are not
homogeneous with regard to the device employed and study design and
have presented conflicting results.
In a pilot study carried out on a series of 20
patients, 14 of whom exhibited residual tumors after therapy,
measurements of tumor size by MBI and decrements of T/B
(tumor-to-background) ratios in images acquired before and at
completion of neoadjuvant therapy demonstrated a limited predictive
value regarding the pathological extent of residual disease
(25).
Other researchers evaluated the accuracy of
preoperative MBI in assessing residual tumor presence and residual
tumor size in comparison with MRI in a series of 122 breast cancer
patients treated with neoadjuvant chemotherapy. The sensitivity and
the specificity of MBI for residual tumor detection were 74.0 and
72.2%, respectively, comparable to those of MRI, 81.7 and 72.2%
(26). In this series, the
assessment of residual tumor extent appeared to depend on the
molecular subtype, the residual tumor size being significantly
underestimated by MBI in the luminal subtype and by MRI in both
luminal and HER2 subtypes. Both procedures provided accurate tumor
size measurements in the triple-negative subtype (26). The higher rate of underestimation in
the luminal and/or HER2 subtypes by MBI was explained by the
researchers and attributed to low-residual cellularity (26).
The ability of MBI to accurately assess residual
disease was demonstrated to be associated with the molecular
subtype also in a more recent study carried out on 51 patients, in
which the highest accuracy was observed in the triple-negative and
HER2/neu positive subtypes (27).
In the present study, we retrospectively assessed
the usefulness of MBI, performed before and at the completion of
chemo- or anti-hormonal neoadjuvant therapy, in predicting complete
tumor response to treatment and residual tumor extent in a
consecutive series of 43 patients, considering histopathological
analysis on surgical samples as the gold standard.
In our series, a pathological complete response,
with total disappearance of the primary breast tumor, was observed
in 16.3% of the cases, while tumor residues, variable in size from
a few millimetres to several centimetres, were ascertained at
surgery in the remaining 83.7% of cases.
MBI proved to be a very high-specific imaging
method, resulting in accurate negative images in all patients
without residual disease, thus confirming the usefulness of
radioisotopic procedures with cationic lipophilic radiotracers in
differentiating tumor residues from areas of fibrotic tissue
replacement inducted by neoadjuvant treatments, as previously
observed in breast cancer and in other types of carcinomas
(28–30). The absence of false-positive results
in our series may be explained by the tetrofosmin cellular uptake
mechanism, the radiotracer accumulating only in viable cells, but
not in fibrotic tissues.
MBI also demonstrated a high sensitivity, detecting
residual disease in 94.4% of cases. We observed only 2
false-negative cases; one of these was probably related to the
tumor site, since the lesion was deeply located in the internal
mammary quadrant and not included in the field of view of the
detector, while the second case could be explained by the small
size of the residual tumor foci that were microscopic, besides
being rare and scattered in a relatively small (1 cm) fibrotic
area. The technical limitation of MBI in visualizing breast tumors
located close to the chest wall is well recognized (18); it is also known that the sensitivity
of the method is partially related to lesion size (18). However, in this series, MBI
demonstrated a high performance also in the identification of
microscopic and/or diffuse residual disease, confirming our
previous preliminary data (31).
Thus, it is likely that not only the size of neoplastic foci,
especially when under the spatial resolution of the detector, but
also other factors, specifically related to tumor biology (i.e.,
histological subtype, slow growth rate and low cellularity), can
affect the identification of residual breast tumors.
Moreover, in the present study, the extent of
residual disease identified with MBI correlated well with
histopathological analysis, particularly when residual tumors were
unifocal.
Collectively, MBI data concurred with
histopathological analysis from surgical samples in a high
percentage of cases (86%), thus suggesting that the procedure may
represent a useful diagnostic imaging test to assess the response
to neoadjuvant chemo- or anti-hormonal therapy in breast cancer
patients and in assessing residual tumor extent, guiding the
surgeon in planning the most appropriate surgical treatment of the
involved breast. In the era of BCS, the knowledge of the extent of
residual disease is of extreme importance, the goal being the
complete excision of residues with a clear margin excision.
In our series, disease extent was underestimated in
2 patients with microscopic foci of invasive carcinoma, lobular in
one case and tubular in the other, scattered in a fibrotic area.
Both underestimated cases belonged to the luminal subtype and had a
low cellularity. Thus, it is possible that molecular subtype and
cellularity degree may affect tumor size assessment in MBI, as also
hypothesized by other researchers (26,27).
In the present study, MBI was used at the end of the
therapeutic cycles, but in the future, it would be interesting to
perform MBI also during therapy in order to identify early in the
treatment method non-responder patients who could benefit from a
change of the therapeutic regimen. This approach has been tested by
some researchers in a series of 19 patients in whom MBI was
performed before (baseline), at 3–5 weeks after onset, and after
completion of therapy (32).
Changes in T/B ratios on MBI images performed at 3–5 weeks
following initiation of therapy were accurate in predicting the
presence or absence of residual disease at therapy completion
(32).
An important limitation of MBI remains its inability
in detecting axillary lymph node metastases. It is well known that
axillary lymph node status after neoadjuvant therapy represents
another important predictor of disease-free and overall survival in
breast cancer patients. Following neoadjuvant therapies, ALND is
thus generally performed for nodal staging at the time of breast
surgery, although a potential role has been recently hypothesized
for the radioguided sentinel node biopsy in selected cases.
Other radioisotopic procedures, such as
single-photon emission computed tomography (SPECT), preferably with
pinhole collimator (pinhole-SPECT), and SPECT combined with
computed tomography (SPECT/CT), have proved more suitable than both
conventional planar scintimammography and MBI in axillary lymph
node metastasis detection, facilitating the identification of
non-palpable and deeply located axillary lymph node metastases
(33–37). An acquisition protocol that includes
an MBI study followed by a SPECT scan of the axillary regions,
could represent a useful diagnostic option to obtain information
regarding both residual breast disease and axillary lymph node
status concurrently, thus optimizing the surgical approach not only
at the level of the breast but also at the level of the axilla.
The present study has some limitations. It is a
retrospective single-institution study that involves a limited
number of cases. Thus, larger prospective multi-centre trials are
warranted to further determine the utility of MBI in patients with
large or locally advanced primary breast cancer following
neoadjuvant therapy and its effect on patient management.
In conclusion, MBI proved to be a highly accurate
diagnostic tool in predicting complete tumor response to treatment
and residual tumor extent following neoadjuvant chemotherapy or
anti-hormonal therapy in patients with large or locally advanced
primary breast cancer, concurring with surgical histopathological
findings in 86% of overall cases. A positive result was always
associated with the presence of residual disease and MBI tumor size
was strongly correlated with histopathological analysis mainly in
unifocal tumors.
Our data revealed a wider application of this
procedure in the preoperative management of breast cancer patients
scheduled to receive surgery following neoadjuvant therapy, to
guide the surgeon to the most appropriate breast surgical
treatment. However, these data need to be confirmed in larger
prospective studies.
Acknowledgements
Not applicable.
References
|
1
|
Untch M, Konecny GE, Paepke S and von
Minckwitz G: Current and future role of neoadjuvant therapy for
breast cancer. Breast. 23:526–537. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Newman LA: Management of patients with
locally advanced breast cancer. Curr Oncol Rep. 6:53–61. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kong X, Moran MS, Zhang N, Haffty B and
Yang Q: Meta-analysis confirms achieving pathological complete
response after neoadjuvant chemotherapy predicts favourable
prognosis for breast cancer patients. Eur J Cancer. 47:2084–2090.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chagpar AB, Middleton LP, Sahin AA,
Dempsey P, Buzdar AU, Mirza AN, Ames FC, Babiera GV, Feig BW, Hunt
KK, et al: Accuracy of physical examination, ultrasonography, and
mammography in predicting residual pathologic tumor size in
patients treated with neoadjuvant chemotherapy. Ann Surg.
243:257–264. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Spanu A, Farris A, Schillaci O, Chessa F,
Solinas ME, Falchi A and Madeddu G, Nuvoli S and Madeddu G: The
usefulness of 99mTc tetrofosmin scintigraphy in patients
with breast cancer recurrences. Nucl Med Commun. 24:145–154. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Spanu A, Schillaci O and Madeddu G:
99mTc labelled cationic lipophilic complexes in
malignant and benign tumors: The role of SPET and pinhole-SPET in
breast cancer, differentiated thyroid carcinoma and
hyperparathyroidism. Q J Nucl Med Mol Imaging. 49:145–169.
2005.PubMed/NCBI
|
|
7
|
Schillaci O, Spanu A, Danieli R and
Madeddu G: Molecular breast imaging with gamma emitters. Q J Nucl
Med Mol Imaging. 57:340–351. 2013.PubMed/NCBI
|
|
8
|
Arbab AS, Koizumi K, Toyama K, Arai T and
Araki T: Ion transport systems in the uptake of
99Tcm-tetrofosmin, 99Tcm-MIBI and 201Tl in a
tumour cell line. Nucl Med Commun. 18:235–240. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bernard BF, Krenning EP, Breeman WA,
Ensing G, Benjamins H, Bakker WH, Visser TJ and de Jong M:
99mTc-MIBI, 99mTc-tetrofosmin and
99mTc-Q12 in vitro and in vivo. Nucl Med Biol.
25:233–240. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Arbab AS, Koizumi K, Toyama K, Arai T and
Araki T: Technetium-99m-tetrofosmin, technetium-99m-MIBI and
thallium-201 uptake in rat myocardial cells. J Nucl Med.
39:266–271. 1998.PubMed/NCBI
|
|
11
|
Spanu A, Dettori G, Nuvoli S, Porcu A,
Falchi A, Cottu P, Solinas ME, Scanu AM, Chessa F and Madeddu G:
(99)mTc-tetrofosmin SPET in the detection of both primary breast
cancer and axillary lymph node metastasis. Eur J Nucl Med.
28:1781–1794. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Spanu A, Schillaci O, Meloni GB, Porcu A,
Cottu P, Nuvoli S, Falchi A, Chessa F, Solinas ME and Madeddu G:
The usefulness of 99mTc-tetrofosmin SPECT
scintimammography in the detection of small size primary breast
carcinomas. Int J Oncol. 21:831–840. 2002.PubMed/NCBI
|
|
13
|
Goldsmith SJ, Parsons W, Guiberteau MJ,
Stern LH, Lanzkowsky L, Weigert J, Heston TF, Jones E, Buscombe J
and Stabin MG: Society of Nuclear Medicine: SNM practice guideline
for breast scintigraphy with breast-specific gamma-cameras 1.0. J
Nucl Med Technol. 38:219–224. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Brem RF, Schoonjans JM, Kieper DA,
Majewski S, Goodman S and Civelek C: High-resolution
scintimammography: A pilot study. J Nucl Med. 43:909–915.
2002.PubMed/NCBI
|
|
15
|
Spanu A, Cottu P, Manca A, Chessa F, Sanna
D and Madeddu G: Scintimammography with dedicated breast camera in
unifocal and multifocal/multicentric primary breast cancer
detection: A comparative study with SPECT. Int J Oncol. 31:369–377.
2007.PubMed/NCBI
|
|
16
|
Spanu A, Chessa F, Meloni GB, Sanna D,
Cottu P, Manca A, Nuvoli S and Madeddu G: The role of planar
scintimammography with high-resolution dedicated breast camera in
the diagnosis of primary breast cancer. Clin Nucl Med. 33:739–742.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Spanu A, Sanna D, Chessa F, Manca A, Cottu
P, Fancellu A, Nuvoli S and Madeddu G: The clinical impact of
breast scintigraphy acquired with a breast specific γ-camera (BSGC)
in the diagnosis of breast cancer: Incremental value versus
mammography. Int J Oncol. 41:483–489. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sun Y, Wei W, Yang HW and Liu JL: Clinical
usefulness of breast-specific gamma imaging as an adjunct modality
to mammography for diagnosis of breast cancer: A systemic review
and meta-analysis. Eur J Nucl Med Mol Imaging. 40:450–463. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Spanu A, Sanna D, Chessa F, Cottu P, Manca
A and Madeddu G: Breast scintigraphy with breast-specific γ-camera
in the detection of ductal carcinoma in situ: A correlation with
mammography and histologic subtype. J Nucl Med. 53:1528–1533. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Edwards C, Williams S, McSwain AP, Damle
S, Rapelyea JA, Downs K, Torrente J, Sambamurty A, Brem RF and Teal
CB: Breast-specific gamma imaging influences surgical management in
patients with breast cancer. Breast J. 19:512–519. 2013.PubMed/NCBI
|
|
21
|
Rhodes DJ, Hruska CB, Conners AL,
Tortorelli CL, Maxwell RW, Jones KN, Toledano AY and O'Connor MK:
Journal club: Molecular breast imaging at reduced radiation dose
for supplemental screening in mammographically dense breasts. AJR
Am J Roentgenol. 204:241–251. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hsu DF, Freese DL and Levin CS:
Breast-Dedicated Radionuclide Imaging Systems. J Nucl Med. 57 Suppl
1:40S–45S. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hruska CB, Phillips SW, Whaley DH, Rhodes
DJ and O'Connor MK: Molecular breast imaging: Use of a dual-head
dedicated gamma camera to detect small breast tumors. AJR Am J
Roentgenol. 191:1805–1815. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hruska CB, Weinmann AL, Skjerseth Tello
CM, Wagenaar EM, Conners AL, Tortorelli CL, Maxwell RW, Rhodes DJ
and O'Connor MK: Proof of concept for low-dose molecular breast
imaging with a dual-head CZT gamma camera. Part II. Evaluation in
patients. Med Phys. 39:3476–3483. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wahner-Roedler DL, Boughey JC, Hruska CB,
Chen B, Rhodes DJ, Tortorelli CL, Maxwell RW, Cha SS and O'Connor
MK: The use of molecular breast imaging to assess response in women
undergoing neoadjuvant therapy for breast cancer: A pilot study.
Clin Nucl Med. 37:344–350. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lee HS, Ko BS, Ahn SH, Son BH, Lee JW, Kim
HJ, Yu JH, Kim SB, Jung KH, Ahn JH, et al: Diagnostic performance
of breast-specific gamma imaging in the assessment of residual
tumor after neoadjuvant chemotherapy in breast cancer patients.
Breast Cancer Res Treat. 145:91–100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Menes TS, Golan O, Vainer G, Lerman H,
Schneebaum S, Klausner J and Even-Sapir E: Assessment of residual
disease with molecular breast imaging in patients undergoing
neoadjuvant therapy: Association with molecular subtypes. Clin
Breast Cancer. 16:389–395. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Spanu A, Ginesu F, Pirina P, Solinas ME,
Schillaci O, Farris A, Chessa F, Madeddu G, Marongiu P, Falchi A,
et al: The usefulness of 99mTc-tetrofosmin SPECT in the
detection of intrathoracic malignant lesions. Int J Oncol.
22:639–649. 2003.PubMed/NCBI
|
|
29
|
Schillaci O, Spanu A and Madeddu G:
[99mTc]sestamibi and [99mTc]tetrofosmin in
oncology: SPET and fusion imaging in lung cancer, malignant
lymphomas and brain tumors. Q J Nucl Med Mol Imaging. 49:133–144.
2005.PubMed/NCBI
|
|
30
|
Spanu A, Sanna D, Chessa F, Farris A,
Nuvoli S and Madeddu G: The usefulness of Tc-99m-tetrofosmin
SPECT/CT in the detection of residual tumors and axillary lymph
node metastases in breast cancer patients following neoadjuvant
therapy. Clin Nucl Med. 36:997–1002. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Spanu A, Farris A, Chessa F, Sanna D,
Pittalis M, Manca A and Madeddu G: Planar scintimammography and
SPECT in neoadjuvant chemo or hormonotherapy response evaluation in
locally advanced primary breast cancer. Int J Oncol. 32:1275–1283.
2008.PubMed/NCBI
|
|
32
|
Mitchell D, Hruska CB, Boughey JC,
Wahner-Roedler DL, Jones KN, Tortorelli C, Conners AL and O'Connor
MK: 99mTc-sestamibi using a direct conversion molecular
breast imaging system to assess tumor response to neoadjuvant
chemotherapy in women with locally advanced breast cancer. Clin
Nucl Med. 38:949–956. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Schillaci O, Scopinaro F, Spanu A,
Donnetti M, Danieli R, Di Luzio E, Madeddu G and David V: Detection
of axillary lymph node metastases in breast cancer with Tc-99m
tetrofosmin scintigraphy. Int J Oncol. 20:483–487. 2002.PubMed/NCBI
|
|
34
|
Spanu A, Tanda F, Dettori G, Manca A,
Chessa F, Porcu A, Falchi A, Nuvoli S and Madeddu G: The role of
(99m)Tc-tetrofosmin pinhole-SPECT in breast cancer non palpable
axillary lymph node metastases detection. Q J Nucl Med. 47:116–128.
2003.PubMed/NCBI
|
|
35
|
Madeddu G and Spanu A: Use of tomographic
nuclear medicine procedures, SPECT and pinhole SPECT, with cationic
lipophilic radiotracers for the evaluation of axillary lymph node
status in breast cancer patients. Eur J Nucl Med Mol Imaging. 31
Suppl 1:S23–S34. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Spanu A, Chessa F, Sanna D, Cottu P, Manca
A, Nuvoli S and Madeddu G: Breast cancer axillary lymph node
metastasis detection by a high-resolution dedicated breast camera:
A comparative study with SPECT and pinhole SPECT. Cancer Biother
Radiopharm. 22:799–811. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Spanu A, Chessa F, Sanna D, Cottu P, Manca
A, Nuvoli S and Madeddu G: Scintimammography with a high resolution
dedicated breast camera in comparison with SPECT/CT in primary
breast cancer detection. Q J Nucl Med Mol Imaging. 53:271–280.
2009.PubMed/NCBI
|