Introduction
Vanadium is a grey metal that exists in a number of
different states of oxidation: −1, 0, +2, +3, +4 and +5. The most
common form in commercial products is vanadium pentoxide
(V2O5). All vanadium compounds have been
considered toxic. The maximum amount of human
V2O5 exposure has been established by the
Occupational Safety and Health Administration of the US Department
of Labor as 0.05 mg/m3 for dust and 0.1 mg/m3
for fumes, in workplace air for an 8 h workday/40 h work week
(1). Exposure to a 35
mg/m3 dose of vanadium is considered life-threatening
and could provoke serious and perpetual health issues including
death, as determined by The National Institute for Occupational
Safety and Health (1).
The respiratory system is the most vulnerable system
to the toxic effect of vanadium whereas there is inconsequential
action on the gastrointestinal system due to the minimal gut
absorption rate of the substance (2–4).
Unfortunately, we lack satisfactory data to determine the reference
range of a subchronic or chronic inhaled dose. The effects
resulting from an oral or inhaled vanadium exposure on serum
parameters (5,6), the liver (7), nervous system (8) and development of other tissues have
been described in rat models (9).
Recently, the increase in the incidence of thyroid
cancer in areas of volcanic activity suggest a carcinogenic effect
of volcanic pollution. In the Mount Etna volcanic area, the
incidence of thyroid cancer was higher than that in control areas
(18.5 and 9.6/105 inhabitants, respectively). In volcanic areas,
various trace elements are increased (with respect to control
areas) in both lichens and drinking water, indicating atmospheric
and water pollution. The amounts of trace elements are
significantly increased, among them vanadium which was increased 8
times, and its possible carcinogenic role on the thyroid has been
hypothesized (10,11).
However, no in vivo or in vitro
studies have evaluated thyroid/endocrine disruption in humans
and/or animals after exposure to vanadium. In the present study, we
evaluated the effect of V2O5 on the
proliferation and chemokine secretion of normal thyrocytes.
Materials and methods
Thyroid follicular cells (TFCs)
We collected 10 specimens of thyroid tissue from 10
euthyroid patients (mean age, 41 years, range 24–61; 5 females, 5
males) (8 undergoing parathyroidectomy, 2 laryngeal intervention).
We obtained informed consent from all participants, and the local
ethics committee of the University of Pisa provided approval for
the study. Thyrocytes were prepared as previously described
(12–14). The digestion of tissue samples was
carried out by collagenase (Roche Diagnostics GmbH, Mannheim,
Germany; 1 mg/ml) with RPMI-1640 (Whittaker Bioproducts, Inc.,
Walkersville, MD, USA) for 1 h at 37°C. The semi-digested follicles
were removed and sedimented for 2 min; they were then washed and
cultured with RPMI-1640 medium in the presence of fetal bovine
serum (FBS) 10% (Seromed Biochrome, Berlin, Germany), 50 mg/ml
penicillin/streptomycin, 2 mM glutamine, with 5% CO2 at
37°C.
Cell viability and proliferation
assay
Cell viability and proliferation were evaluated
using the WST-1 (Roche Diagnostics, Almere, The Netherlands) assay
(which uses 3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium
bromide, in the MTT assay) (15–17).
TFCs were seeded at a density of 35,000 cells/ml (in a final volume
of 100 µl) in each well of 96-well plates. To determine how
V2O5 affects TFC proliferation, the cells
were treated (24 h) with increasing concentrations of
V2O5 (1, 10 and 100 nM). For each cell
preparation, the experiments were performed in triplicate. Cells
were plated and treated for 24 h with V2O5 or
with its vehicle alone.
Proliferation assay: Cell
counting
Cell number counting was also used to evaluate the
proliferation of TFCs as previously described (15–17).
Chemokine secretion assays
To successfully perform the chemokine (C-X-C motif)
ligand (CXCL)9, or CXCL10 secretion assays, 30,000 cells/ml were
seeded (in 96-well plates) in a final volume of 100 µl/well, in
growth medium, which was then removed (after 24 h). Cells were then
washed with phosphate-buffered saline (PBS) and incubated (for 24
h) in serum and phenol red-free medium with interferon (IFN)γ (500,
1,000, 5,000 and 10,000 IU/ml; R&D Systems, Minneapolis, MN,
USA) and tumor necrosis factor (TNF)α (10 ng/ml) (R&D Systems),
in combination (13) or alone. The
TNFα concentration was chosen to obtain the highest secretion in
preliminary experiments. The supernatant was then obtained (after
24 h), and kept frozen at −20°C (until chemokine assay).
To understand how V2O5 affects
the chemokine secretion induced by IFNγ, the cells were treated
(for 24 h) with increasing concentrations of
V2O5 (1, 10 and 100 nM), in the
presence/absence of IFNγ (1,000 IU/ml) and/or TNFα (10 ng/ml).
CXCL9 and CXCL10 in the supernatants were measured by ELISA. The
experiments were conducted 3 times with each different cell
preparation.
ELISA for CXCL9 and CXCL10
CXCL9 or CXCL10 was assessed in the supernatants
from cell cultures by commercially prepared kits (R&D Systems).
The minimum (mean) detectable doses were 1.5 or 1.2 pg/ml, for
CXCL9, or CXCL10 (respectively). The intra- and inter-assay
coefficients of variation were for 3.5 and 6.4%, respectively, for
CXCL9, while these coefficients for CXCL10 were 4.5 and 7.3%,
respectively. Quality control pools of normal, low and high
concentrations were also included in each assay.
Data analysis
For normally distributed variables, the values are
expressed in the text as mean (± SD), or mean (± SEM) in figures,
otherwise as median [and interquartile range]. Mean group values
were compared by using one-way analysis of variance (ANOVA) for
variables normally distributed, or with the Kruskal-Wallis test, or
Mann-Whitney U test. Proportions were compared by the Chi-square
test. The Bonferroni-Dunn test was used for post hoc comparison of
normally distributed variables.
Results
Cell proliferation
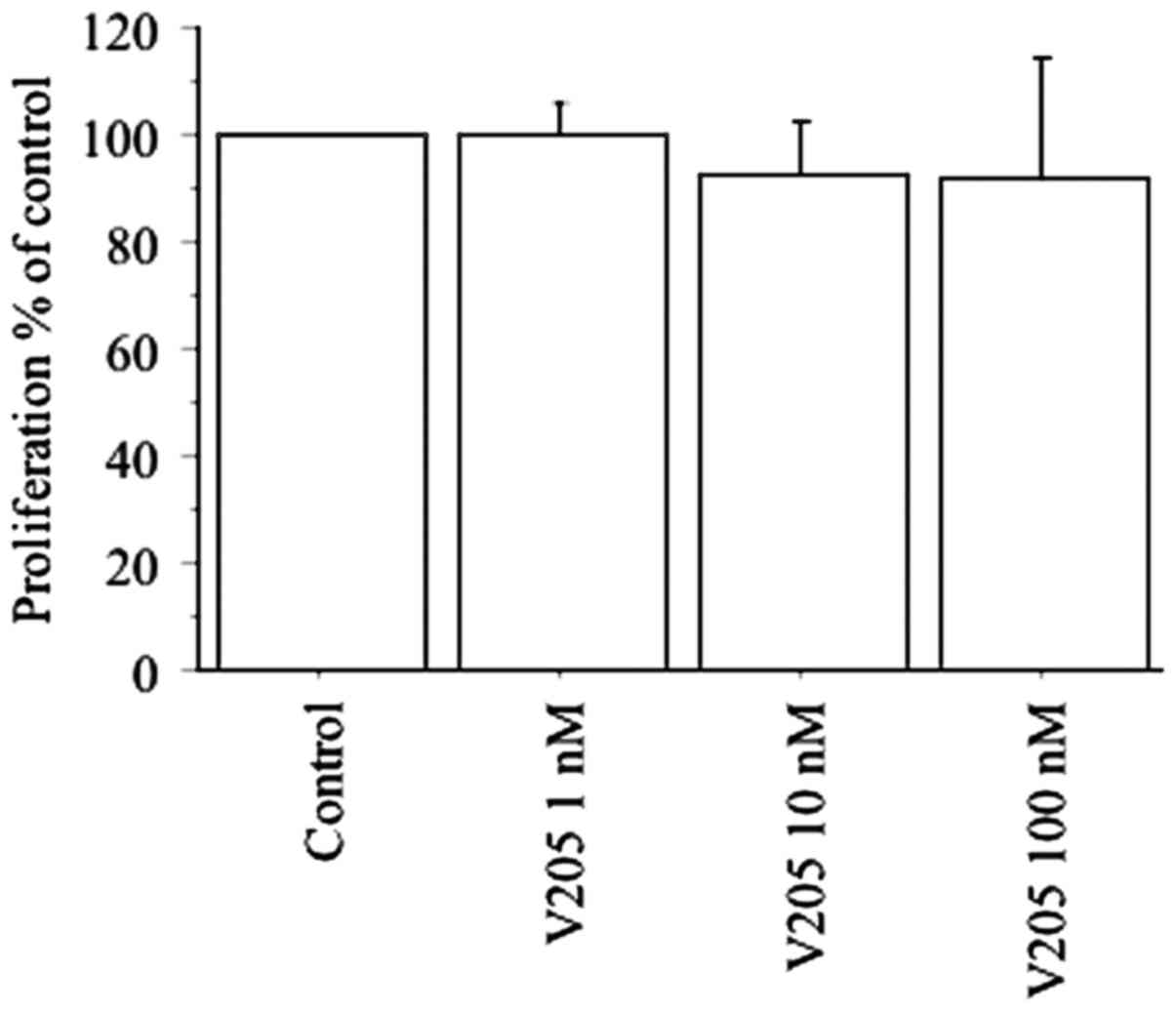
Cell viability and proliferation assay WST-1
demonstrated that V2O5 (1, 10 and 100 nM) did
not alter the viability or proliferation of the TFCs (Fig. 1). These results were confirmed by
cell counting (data not shown).
CXCL9
CXCL9 levels were not detectable in supernatants
gathered from primary thyrocyte samples, whereas the CXCL9
concentration was increased after dose-dependent induction of IFNγ
(0, 61±27, 136±34, 196±41 and 262±67 pg/ml; with IFNγ 0, 500,
1,000, 5,000 and 10,000 IU/ml, respectively; P<0.001 by ANOVA).
TNFα alone was not able to promote any impact on CXCL9 (remaining
undetectable), while the synergy of IFNγ plus TNFα elicited a
significant influence on CXCL9 release (CXCL9, 8976±1456 vs. 142±34
pg/ml with IFNγ alone, P<0.0001 by ANOVA).
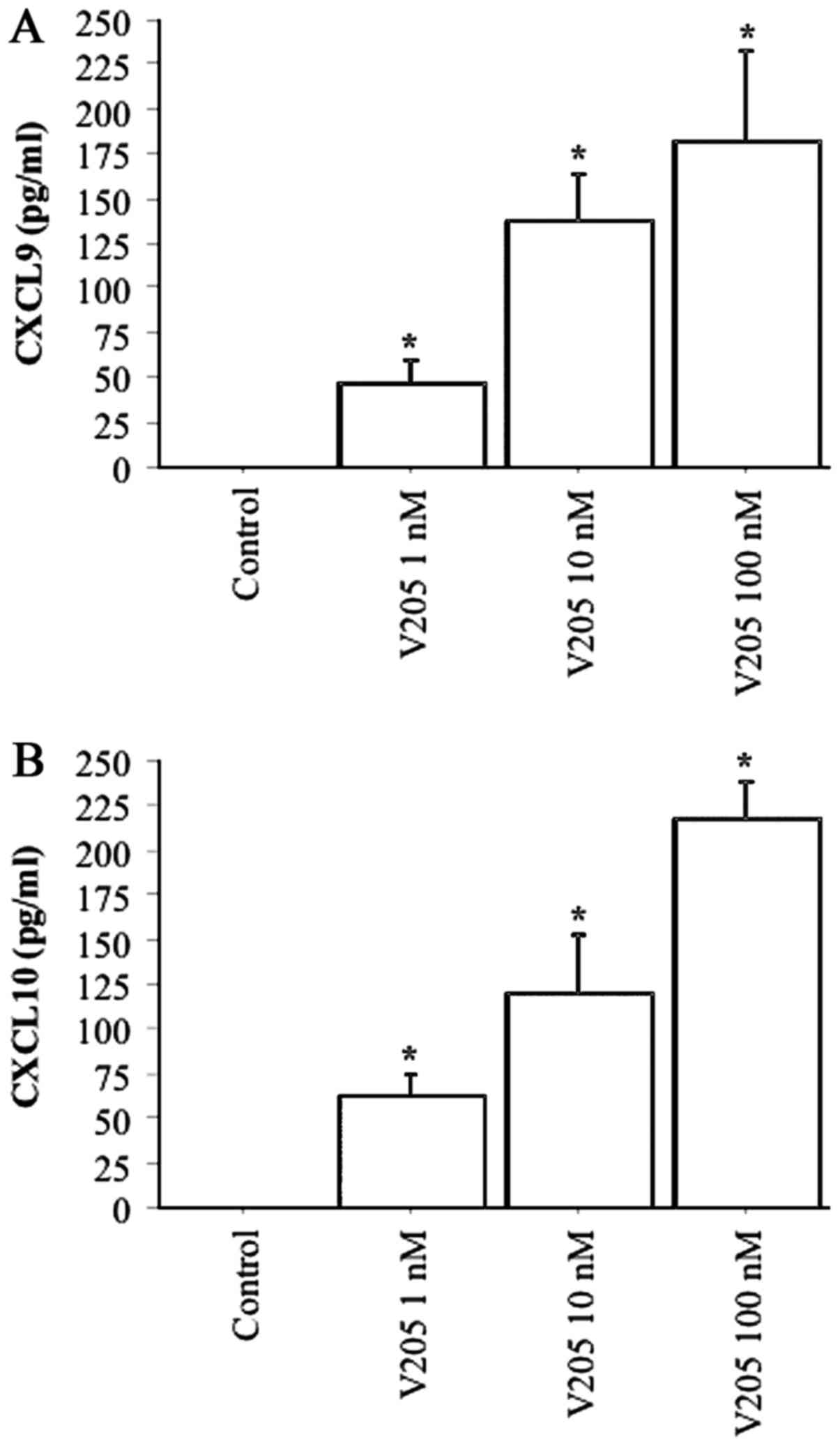
Following the treatment of thyrocytes with
V2O5 (1, 10 and 100 nM), CXCL9 secretion was
dose-dependently stimulated (ANOVA, P<0.0001) (Fig. 2A). Following the treatment of
thyrocytes with V2O5 (1, 10 and 100 nM),
together with TNFα, CXCL9 secretion was not significantly altered
with respect to V2O5 alone (data not
shown).
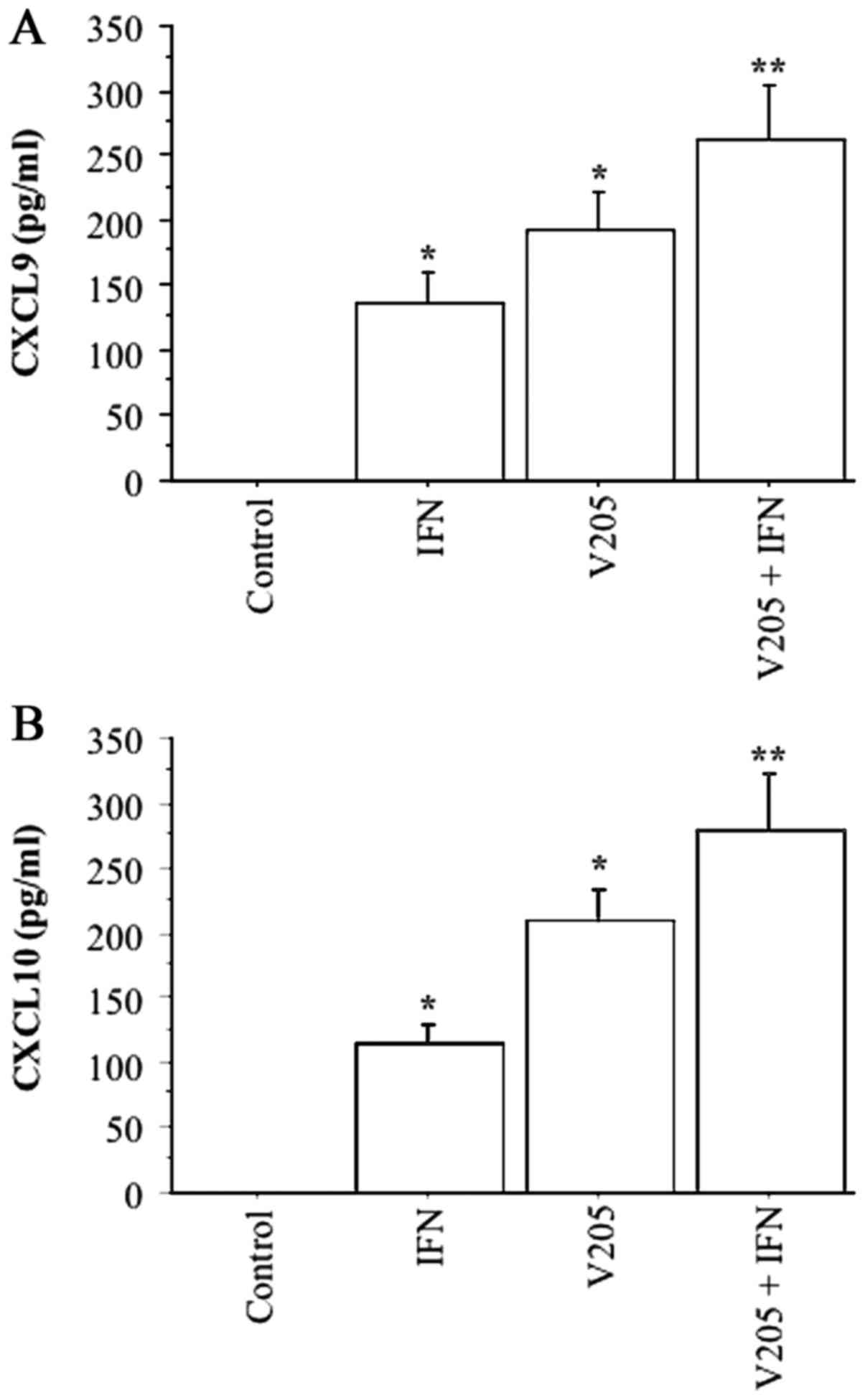
Following the treatment of thyrocytes with
V2O5 (100 nM), together with IFNγ, CXCL9
release was synergistically increased (ANOVA, P<0.0001)
(Fig. 3A).
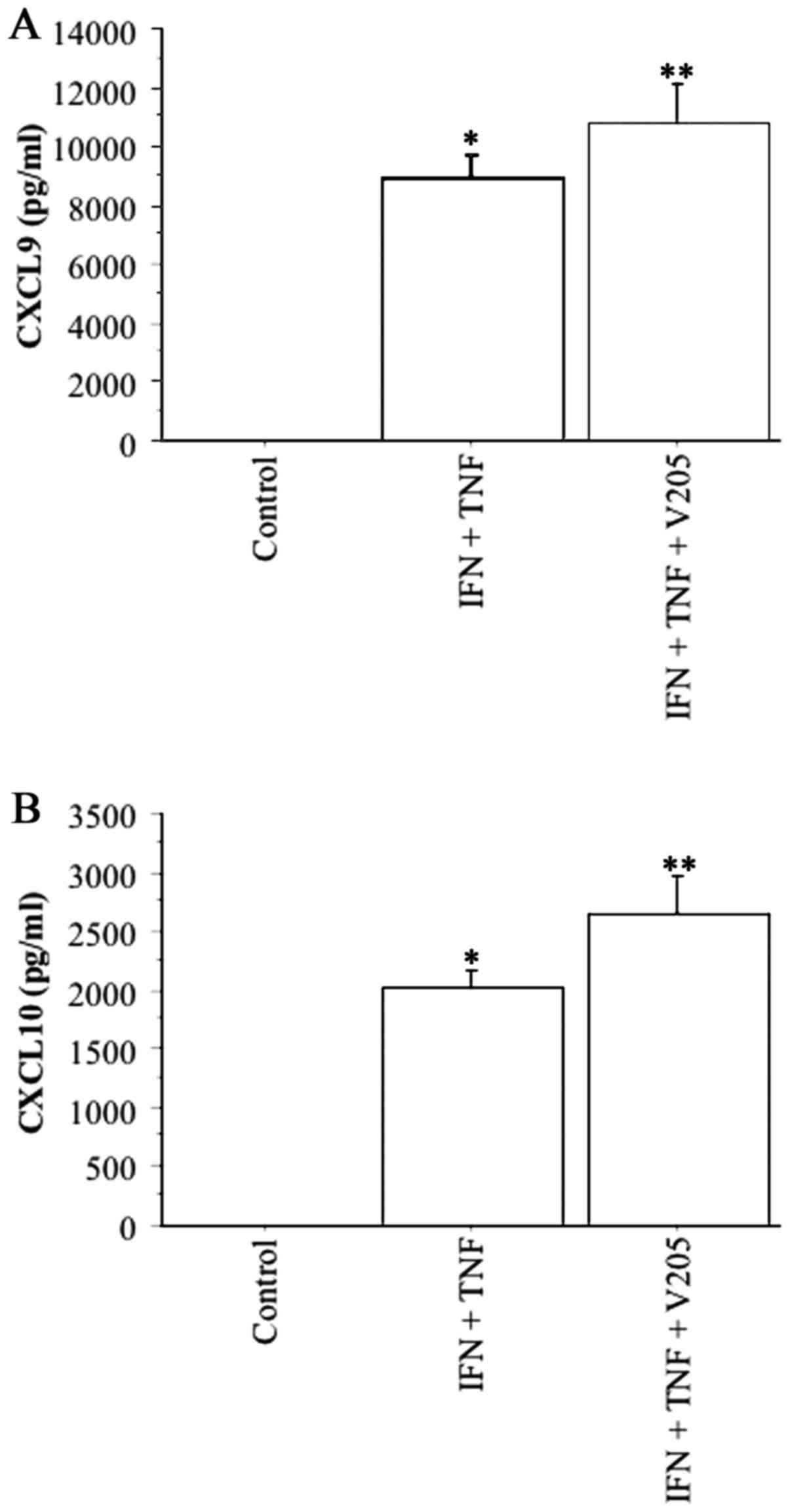
Following the treatment of thyrocytes with
V2O5 (100 nM), together with IFNγ and TNFα,
CXCL9 secretion was synergistically increased (ANOVA, P<0.0001)
(Fig. 4A).
CXCL10
CXCL10 was not detectable in the supernatants from
primary thyrocyte cultures in basal condition. IFNγ induced CXCL10
secretion dose-dependently (0, 45±22, 111±35, 213±27, 254±64 pg/ml,
with IFNγ 0, 500, 1,000, 5,000 and 10,000 IU/ml; respectively;
P<0.001 by ANOVA). TNFα only was not able in this case to carry
out any impact on CXCL10, while the synergy of IFNγ plus TNFα
elicited a significant influence on CXCL10 secretion (2,011±154 vs.
108±26 pg/ml with IFNγ alone; P<0.0001, by ANOVA).
Following treatment of thyrocytes with
V2O5 (1, 10 and 100 nM) CXCL10 secretion was
stimulated dose-dependently (P<0.0001 by ANOVA) (Fig. 2B). Following treatment of thyrocytes
with V2O5 (1, 10 and 100 nM), together with
TNFα, CXCL10 secretion was not significantly changed with respect
to V2O5 alone (data not shown).
Following treatment of thyrocytes with
V2O5 (100 nM), together with IFNγ, CXCL10
release was synergistically increased (P<0.0001 by ANOVA)
(Fig. 3B).
Following treatment of thyrocytes with
V2O5 (100 nM), together with IFNγ plus TNFα,
CXCL10 secretion was synergistically increased (P<0.0001 by
ANOVA) (Fig. 4B).
Discussion
The results of the present study demonstrated that
V2O5 can promote IFNγ-dependent chemokine
secretion by TFCs, without altering the viability and proliferation
of the cells. Moreover, as expected (14), our study confirmed that IFNγ and
TNFα stimulated the secretion of C-X-C chemokines, CXCL9 and
CXCL10, evaluated by ELISA, which is an accepted and commonly
published method to dose chemokine levels in supernatants. Notably,
V2O5 was able to synergize with IFNγ and
TNFα, further increasing chemokine secretion. These results, on the
whole, are in agreement with the view that
V2O5 is able to induce and perpetuate an
inflammatory disorder in the thyroid evolving from a predominant
T-helper (Th)1 immune response (15).
In fact, IFNγ-inducible C-X-C chemokines can be
secreted by several types of mammalian cells, such as fibroblasts,
thyrocytes, islet cells, colon epithelial cells, endothelial cells,
and others (12–19). However, in basal condition such cell
types do not produce these chemokines, that are secreted after the
stimulation with IFNγ (alone or in combination with TNFα), a
cytokine that is produced by Th1-activated lymphocytes in several
autoimmune diseases, for example in the thyroid in Graves' disease,
or in autoimmune thyroiditis. This process has been hypothesized to
be involved in the initiation and/or the perpetuation in several
autoimmune disorders (12–21), and it can be applied also to the
thyroid.
Our results agree with those of other researches in
different cell types. V2O5 exposure is a
cause of occupational bronchitis, and a study evaluated gene
expression profiles in human lung fibroblasts (in cultures) after
exposure in vitro to V2O5 in order to
identify genes that may play a role in the bronchial inflammation,
repair and fibrosis in the pathogenesis of bronchitis.
Approximately 12 genes were overexpressed following exposure to
V2O5, including chemokines (CXCL9, CXCL10 and
interleukin-8) (22). In a second
study, it was shown that fibroblasts respond to vanadium oxidative
stress by producing IFNβ and activating STAT-1, that led to
increased CXCL10 levels (23),
playing a role in the innate immune response.
Importantly, vanadium was able to increase chemokine
secretion in a dose range, from 1 to 100 nM. It was observed that
normal blood levels of vanadium range from 0.45 to 18.4 nM, and
that 100 nM is a dose that may mimic an abnormally high exposure
(24).
The mechanisms by which V2O5
induces lung cancer have been investigated in mice in numerous
studies. Experts agree that in vivo and in vitro
research suggests that cancers are induced by secondary mechanisms
(probably not genotoxic effects) (25).
Thus, we hypothesized that, also for the thyroid,
the induction and perpetuation of an inflammatory reaction into
this gland, and the variety of involved candidate genes could
predispose to the appearance of thyroid cancer (as recently
demonstrated for the association of papillary thyroid cancer and
autoimmune thyroiditis), and could be at the basis of
V2O5-induced effects after occupational and
environmental exposure.
In conclusion, the present study showed that
V2O5 is able to induce the secretion of Th1
chemokines into the thyroid, synergistically increasing the effect
of important Th1 cytokines such as IFNγ and TNFα, leading to the
induction and perpetuation of an inflammatory reaction in the
thyroid. Further studies are necessary to investigate the mechanism
of action by which chemokines are secreted, and to evaluate thyroid
function, and nodules, in subjects occupationally exposed, or
living in polluted areas.
Acknowledgements
Not applicable.
References
|
1
|
‘Occupational Safety and Health Guidelines
for Vanadium Pentoxide’. Occupational Safety and Health
Administration. https://www.osha.gov/SLTC/healthguidelines/vanadiumpentoxidedust/recognition.htmlRetrieved
29 January 2009.
|
|
2
|
Sax NI: Dangerous Properties of Industrial
Materials. 6th. Van Nostrand Reinhold Company; New York: pp.
2717–2720. 1984
|
|
3
|
Ress NB, Chou BJ, Renne RA, Dill JA,
Miller RA, Roycroft JH, Hailey JR, Haseman JK and Bucher JR:
Carcinogenicity of inhaled vanadium pentoxide in F344/N rats and
B6C3F1 mice. Toxicol Sci. 74:287–296. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wörle-Knirsch JM, Kern K, Schleh C,
Adelhelm C, Feldmann C and Krug HF: Nanoparticulate vanadium oxide
potentiated vanadium toxicity in human lung cells. Environ Sci
Technol. 41:331–336. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Scibior A, Zaporowska H and Ostrowski J:
Selected haematological and biochemical parameters of blood in rats
after subchronic administration of vanadium and/or magnesium in
drinking water. Arch Environ Contam Toxicol. 51:287–295. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
González-Villalva A, Fortoul TI,
Avila-Costa MR, Piñón-Zarate G, Rodriguez-Laraa V, Martínez-Levy G,
Rojas-Lemus M, Bizarro-Nevarez P, Díaz-Bech P, Mussali-Galante P,
et al: Thrombocytosis induced in mice after subacute and subchronic
V2O5 inhalation. Toxicol Ind Health. 22:113–116. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kobayashi K, Himeno S, Satoh M, Kuroda J,
Shibata N, Seko Y and Hasegawa T: Pentavalent vanadium induces
hepatic metallothionein through interleukin-6-dependent and
-independent mechanisms. Toxicology. 228:162–170. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Soazo M and Garcia GB: Vanadium exposure
through lactation produces behavioral alterations and CNS myelin
deficit in neonatal rats. Neurotoxicol Teratol. 29:503–510. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Barceloux DG and Barceloux D: Vanadium. J
Toxicol Clin Toxicol. 37:265–278. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Malandrino P, Russo M, Ronchi A, Minoia C,
Cataldo D, Regalbuto C, Giordano C, Attard M, Squatrito S,
Trimarchi F, et al: Increased thyroid cancer incidence in a
basaltic volcanic area is associated with non-anthropogenic
pollution and biocontamination. Endocrine. 53:471–479. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ferrari SM, Fallahi P, Antonelli A and
Benvenga S: Environmental issues in thyroid diseases. Front
Endocrinol. 8:502017. View Article : Google Scholar
|
|
12
|
García-López MA, Sancho D, Sánchez-Madrid
F and Marazuela M: Thyrocytes from autoimmune thyroid disorders
produce the chemokines IP-10 and Mig and attract CXCR3+
lymphocytes. J Clin Endocrinol Metab. 86:5008–5016. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Antonelli A, Ferri C, Fallahi P, Ferrari
SM, Frascerra S, Sebastiani M, Franzoni F, Galetta F and Ferrannini
E: High values of CXCL10 serum levels in patients with hepatitis C
associated mixed cryoglobulinemia in presence or absence of
autoimmune thyroiditis. Cytokine. 42:137–143. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Antonelli A, Ferrari SM, Fallahi P,
Frascerra S, Santini E, Franceschini SS and Ferrannini E: Monokine
induced by interferon gamma (IFNgamma) (CXCL9) and IFNgamma
inducible T-cell alpha-chemoattractant (CXCL11) involvement in
Graves' disease and ophthalmopathy: Modulation by peroxisome
proliferator-activated receptor-gamma agonists. J Clin Endocrinol
Metab. 94:1803–1809. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Antonelli A, Rotondi M, Fallahi P,
Romagnani P, Ferrari SM, Buonamano A, Ferrannini E and Serio M:
High levels of circulating CXC chemokine ligand 10 are associated
with chronic autoimmune thyroiditis and hypothyroidism. J Clin
Endocrinol Metab. 89:5496–5499. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Antonelli A, Ferrari SM, Frascerra S,
Pupilli C, Mancusi C, Metelli MR, Orlando C, Ferrannini E and
Fallahi P: CXCL9 and CXCL11 chemokines modulation by peroxisome
proliferator-activated receptor-alpha agonists secretion in Graves'
and normal thyrocytes. J Clin Endocrinol Metab. 95:E413–E420. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kemp EH, Metcalfe RA, Smith KA, Woodroofe
MN, Watson PF and Weetman AP: Detection and localization of
chemokine gene expression in autoimmune thyroid disease. Clin
Endocrinol. 59:207–213. 2003. View Article : Google Scholar
|
|
18
|
Antonelli A, Ferrari SM, Corrado A,
Ferrannini E and Fallahi P: CXCR3, CXCL10 and type 1 diabetes.
Cytokine Growth Factor Rev. 25:57–65. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Antonelli A, Ferrari SM, Giuggioli D,
Ferrannini E, Ferri C and Fallahi P: Chemokine (C-X-C motif) ligand
(CXCL)10 in autoimmune diseases. Autoimmun Rev. 13:272–280. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fallahi P, Ferrari SM, Ruffilli I, Elia G,
Biricotti M, Vita R, Benvenga S and Antonelli A: The association of
other autoimmune diseases in patients with autoimmune thyroiditis:
Review of the literature and report of a large series of patients.
Autoimmun Rev. 15:1125–1128. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Antonelli A, Fallahi P, Delle Sedie A,
Ferrari SM, Maccheroni M, Bombardieri S, Riente L and Ferrannini E:
High values of Th1 (CXCL10) and Th2 (CCL2) chemokines in patients
with psoriatic arthtritis. Clin Exp Rheumatol. 27:22–27.
2009.PubMed/NCBI
|
|
22
|
Ingram JL, Antao-Menezes A, Turpin EA,
Wallace DG, Mangum JB, Pluta LJ, Thomas RS and Bonner JC: Genomic
analysis of human lung fibroblasts exposed to vanadium pentoxide to
identify candidate genes for occupational bronchitis. Respir Res.
8:342007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Antao-Menezes A, Turpin EA, Bost PC,
Ryman-Rasmussen JP and Bonner JC: STAT-1 signaling in human lung
fibroblasts is induced by vanadium pentoxide through an IFN-beta
autocrine loop. J Immunol. 180:4200–4207. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sabbioni E, Kuèera J, Pietra R and
Vesterberg O: A critical review on normal concentrations of
vanadium in human blood, serum, and urine. Sci Total Environ.
188:49–58. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Assem FL and Levy LS: A review of current
toxicological concerns on vanadium pentoxide and other vanadium
compounds: Gaps in knowledge and directions for future research. J
Toxicol Environ Health B Crit Rev. 12:289–306. 2009. View Article : Google Scholar : PubMed/NCBI
|