Introduction
Hepatocellular carcinoma (HCC) was reported to be
the sixth most common cancer and the fourth most common cause of
malignancy-associated mortality worldwide in 2018. Each year,
~841,000 new cases of HCC are diagnosed and 782,000 deaths occur
due to HCC worldwide (1). Notably,
~50% of newly diagnosed HCC cases and HCC-related deaths are
thought to occur in China, with ~466,100 newly diagnosed patients
and ~422,100 deaths occurring in China in 2015 (2). Primary liver cancer includes several
pathological types, of which HCC is the predominant form that
accounts for 75–85 % of all cases, with an incidence of 6.20 cases
per 100,000 (1,3). Compared with other types of cancer,
HCC in China carried the worst prognosis between 2003 and 2005,
with a 1-year survival rate of <50% and a 5-year-survival rate
of only 10.1% (4,5). Hepatitis B virus (HBV) infection is
the primary cause of the high incidence of HCC in China (6). Given the poor prognosis of this
disease, early HCC detection and treatment is of the utmost
importance (7). Recent advances in
genetic research have promoted a comprehensive understanding of the
role of genetic mutations in HCC, allowing for the identification
of diagnostic and prognostic HCC biomarkers (8).
Cysteine proteases are critical in promoting the
progression of various types of tumor (9). There are eight subfamilies in the
cystatin (CST) family group (Family 1, Family 2, Family 3, HRG,
Fetuins, CRP, Spp24 and CRES) (10). Cysteine proteases are inhibited by
CSTs (11) and are concentrated in
the leading edge of tumor cells, where they dissolve extracellular
matrix (ECM) proteins to promote invasion (12,13),
thus enhancing tumor progression. Several types of CST have been
discovered to possess significantly distinct expression profiles in
HCC compared with their expression in healthy tissues. CST3, CSTA
and CSTB are significantly highly expressed in HCC tissue compared
with in adjacent healthy tissue, and the expression levels of CSTA
and CSTB are strongly associated with node metastasis for HCC
(14,15). Additionally, it has been reported
that CST3 and CSTB may function as serum markers for HCC (15,16).
Therefore, further investigations into the role of CST genes in HCC
are warranted. The present study aimed to uncover the prognostic
and diagnostic values of Family 1 CSTs (CSTA and CSTB) and Family 2
CSTs (CST1, CST2, CST3, CST4, CST5, CST6, CST7 and CST8) in
patients with HCC using freely available data derived from public
genomic databases.
Materials and methods
Bioinformatics analysis of CST
genes
Database for Annotation, Visualization and
Integrated Discovery (DAVID, version 6.8; david.ncifcrf.gov/home.jsp) (17,18)
was accessed on December 17, 2018 for Kyoto Encyclopedia of Genes
and Genomes (KEGG) pathway annotation, Gene Ontology (GO)
functional annotation and enrichment analysis of CST genes. An
enrichment P<0.05 was considered to indicate a statistically
significant difference. Gene-gene interactions of CST genes were
constructed using GeneMANIA (www.genemania.org, accessed December 17, 2018)
(19,20), whereas protein-protein interactions
of CST genes were constructed using the Search Tool for the
Retrieval of Interacting Genes/Proteins (STRING; string-db.org, accessed December 17, 2018) (21,22).
Data source
The GSE14520 dataset (www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE14520,
accessed December 17, 2018), which comprises clinical data of
patients with HBV-related HCC as well as their CST gene expression
profiles, was extracted from the Gene Expression Omnibus database
(23–25). Due to multiple probe sets in
GSE14520, the expression value of each gene was regarded as the
average value corresponding to the same gene and was normalized
using the limma package of the R platform (version 3.5.1.;
www.r-project.org).
Analysis of gene association and
assessment of diagnostic value
Correlations between the CST genes were analyzed
using Pearson's correlation coefficient and were depicted using the
corrplot function of the R platform (version 3.5.1.;
www.r-project.org); P<0.05 as considered to
indicate a statistically significant difference. Differential
expression of the CST genes between healthy liver tissues and HCC
tumor tissues were statistically analyzed using Student's t-test in
SPSS software (version 22.0; IBM Corp.); P<0.05 as considered to
indicate a statistically significant difference. Receiver operating
characteristic (ROC) curve analysis was used to assess the
diagnostic value of CST genes in predicting HCC (26,27).
Survival analysis
Based on the median value of gene expression,
patients were grouped into either the low or high gene expression
group. Each CST gene was analyzed for survival using Kaplan-Meier
analysis with log-rank test, and a Cox proportional hazards
regression model was conducted to analyze the association of CST
genes with clinical parameters that were strongly associated with
OS (P<0.05). The CST genes associated with survival of patients
with HCC (adjusted P<0.05) were analyzed in combination to
explore their joint effects on survival analysis using Kaplan-Meier
analysis and log-rank test, and Cox proportional hazards regression
model. Nomograms based on biological and clinical variables were
used to construct a statistical prognostic model of overall
survival (OS) for HCC in accordance with survival analysis results
and the Cox proportional hazards regression model (28). Data processing and plot generation
were conducted in R platform (version 3.5.1.; www.r-project.org) with rms package. A scale
that was marked on both ends of the line corresponding to each
variable represented the value range of the variable, and the
length of the line segment reflected the contribution of this
factor to the outcome event.
Gene set enrichment analysis
(GSEA)
The biological pathways targeted by CST genes were
further explored with GSEA (accessed December 17, 2018) (29) using data derived from the Molecular
Signatures Database of c2 (c2.all.v6.1 symbols) and c5 (c5.all.v6.1
symbols) (30). GSEA-derived gene
enrichment sets that attained a false discovery rate (FDR) of
<0.25 and P<0.05 were determined to confer statistical
significance.
Statistical analysis
Statistical data processing was conducted using SPSS
(version 22.0; IBM Corp.) and R (version 3.5.1.; www.r-project.org). The relative risk of patients with
HCC based on CST gene expression was expressed in terms of 95%
confidence intervals (CIs) and hazard ratios (HRs). Univariate
survival analysis of the CST genes and clinical parameters was
performed using Kaplan-Meier analysis with log-rank test. CST genes
and patient clinical parameters that were strongly correlated with
OS (P<0.05) were further subjected to a multivariate Cox
proportional hazards regression model. Pearson's correlation
coefficient was used to assess the relationship between
co-expressed CST genes. P<0.05 was considered to indicate a
statistically significant difference. FDR control of GSEA was
achieved using the Benjamini-Hochberg procedure and adjusted for
multiple testing (31–33).
Results
Bioinformatics analysis of CST
genes
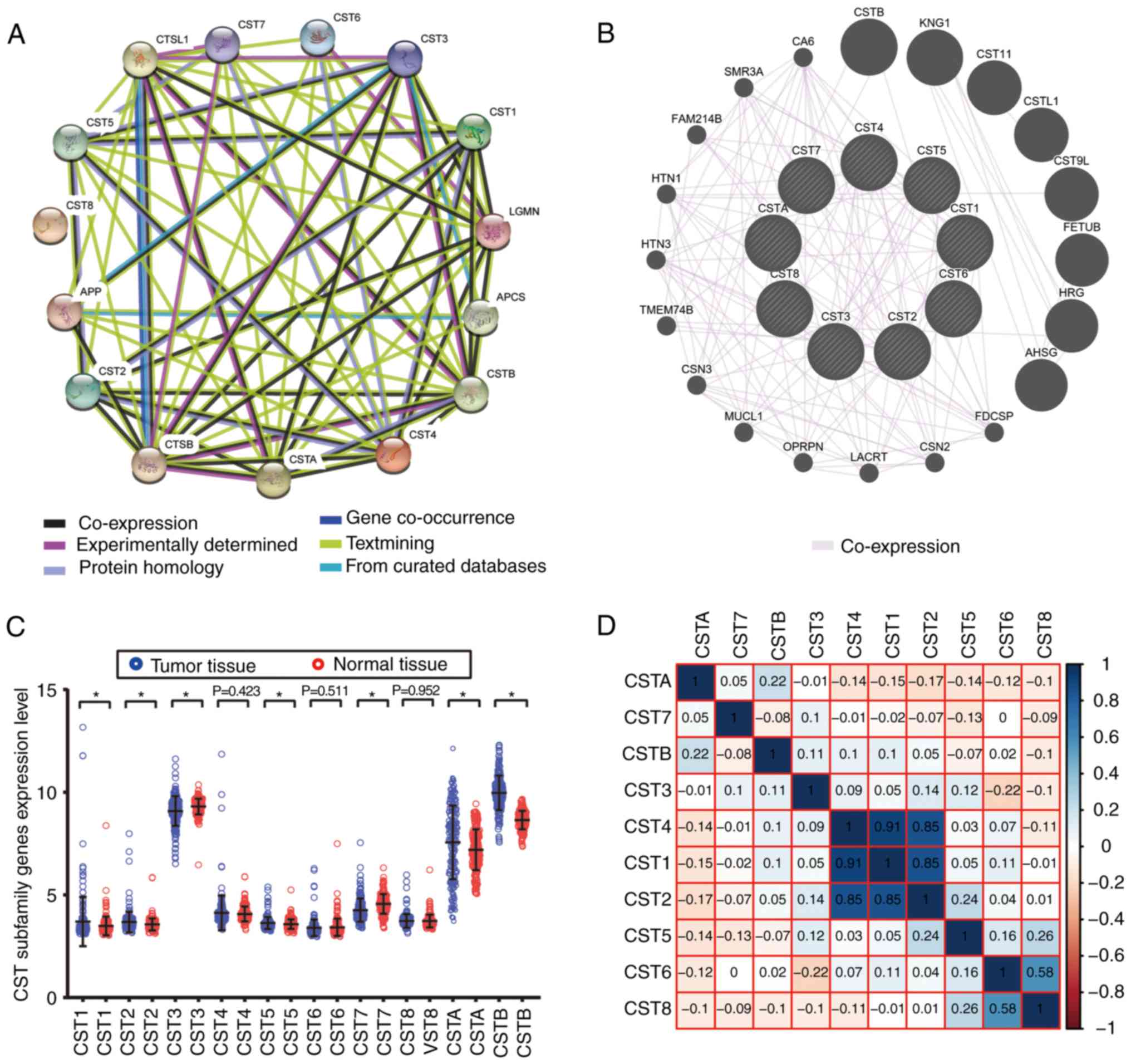
Biological functions (biological processes, cellular
components and molecular functions) of CST1, CST2, CST3, CST4,
CST5, CST6, CST7, CST8, CSTA and CSTB were subjected to a GO
analysis using DAVID. Each of these genes was markedly enriched in
‘extracellular space’, ‘cysteine-type endopeptidase inhibitor
activity’ and ‘protease binding’ (Fig.
1). KEGG pathway analysis using DAVID suggested that CST1,
CST2, CST3, CST4 and CST5 were involved in ‘salivary secretion’
(Fig. 1). CST1, CST2, CST4, CSTA
and CSTB genes and proteins had significant co-expression
relationships (Fig. 2B) and strong
protein homology (Fig. 2A) with
each other.
Data source
The present study derived its data only from the
Affymetrix HT Human Genome U133A Array of GSE14520 in order to
avoid a batch effect. The majority of subjects in this cohort had
HBV-related HCC, whereas the remainder of non-HBV-related cases and
those with no survival data were eliminated. This resulted in data
from 204 adjacent healthy liver tissues and 212 HBV-related HCC
tumor tissues. Data regarding patient prognosis were available for
all patients.
Analysis of gene association and
assessment of diagnostic value
CST gene co-expression in HCC neoplastic tissues was
analyzed using the Pearson correlation coefficient. CST1, CST2 and
CST4 were closely associated with each other in GSE14520 (Fig. 2D). Furthermore, CST1, CST2, CST5,
CSTA and CSTB expression levels were markedly increased in HCC
tumor tissue in the GSE14520 dataset, whereas CST3 and CST7
expression levels were markedly decreased in HCC tumor tissue
(Fig. 2C). There was no significant
difference in the expression of CST4, CST6 and CST8 between HCC
tumor tissues and healthy liver tissues.
ROC analysis of CST genes revealed that the
expression levels of CST7 and CSTB had significant diagnostic
values in differentiating between healthy and malignant hepatic
tissues. The area under the ROC curves of CST7 and CSTB were 0.702
(95% CI: 0.651-0.753; Fig. 3G) and
0.919 (95% CI: 0.891-0.948; Fig.
3J), respectively. The other CST genes did not exhibit
significant diagnostic values.
 | Figure 3.ROC curve analysis of the ability of
CST genes to discriminate between hepatocellular carcinoma and
adjacent healthy tissues in the GSE14520 dataset. ROC curves for
(A) CST1, (B) CST2, (C) CST3, (D) CST4, (E) CST5, (F) CST6, (G)
CST7, (H) CST8, (I) CSTA and (J) CSTB. AUC, area under the curve;
CST, cystatin; ROC, receiver operating characteristic. |
Survival analysis
In GSE14520, patients with an advanced Barcelona
Clinic Liver Cancer (BCLC) stage (34), larger tumor volume (diameter, >5
cm), higher serum α-fetoprotein (AFP; >300 ng/ml) and cirrhosis
were at high risk of death due to HBV-related HCC (Table SI). Cirrhotic patients, males and
those with advanced BCLC stages were also more at risk of
recurrence of HBV-related HCC (Table
SI). No other clinical parameters were revealed to impact
recurrence-free survival (RFS) or OS.
The results of survival analyses of the CST genes
are presented in Figs. 4A-J,
5A-J and Table I. Low expression levels of CST6
(adjusted P=0.009; adjusted HR=1.651; 95% CI: 1.136-2.398; Table I; Fig.
4F) and high expression levels of CST7 (adjusted P=0.048;
adjusted HR=0.688; 95% CI: 0.475-0.966; Table I; Fig.
4G) were strongly associated with the increased RFS of patients
with HBV-related HCC, adjusted for sex, BCLC stage and cirrhosis.
Low expression levels of CST6 (adjusted P=0.036; adjusted HR=1.618;
95% CI: 1.033-2.533; Table I;
Fig. 5F) and high expression levels
of CST7 (adjusted P=0.014; adjusted HR=0.559; 95% CI: 0.351-0.891;
Table I; Fig. 5G) were also strongly associated with
the increased OS of patients with HBV-related HCC, adjusted for
tumor size, AFP, BCLC stage and cirrhosis.
 | Table I.Prognostic values of CST gene
expression in patients with hepatitis B virus-related
hepatocellular carcinoma from the GSE14520 dataset. |
Table I.
Prognostic values of CST gene
expression in patients with hepatitis B virus-related
hepatocellular carcinoma from the GSE14520 dataset.
|
|
| RFS | OS |
|
|
|
|
|
| Gene
expression | Patients
(n=212) | No. of events | MRT (months) | Crude HR (95%
CI) | Crude P-value | Adjusted HR (95%
CI) | Adjusted
P-valuea | No. of events | MST (months) | Crude HR (95%
CI) | Crude P-value | Adjusted HR (95%
CI) | Adjusted
P-valueb |
| CST1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 57 | 46 | 1 |
| 1 |
| 42 | NA | 1 |
| 1 |
|
|
High | 106 | 59 | 40 | 0.964
(0.670-1.388) | 0.846 | 0.900
(0.624-1.299) | 0.575 | 40 | NA | 0.878
(0.569-1.354) | 0.555 | 0.931
(0.602-1.44) | 0.748 |
| CST2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 62 | 35 | 1 |
| 1 |
| 44 | NA | 1 |
| 1 |
|
|
High | 106 | 54 | 53 | 0.811
(0.563-1.169) | 0.261 | 0.739
(0.511-1.068) | 0.108 | 38 | NA | 0.813
(0.527-1.256) | 0.351 | 0.768
(0.492-1.198) | 0.244 |
| CST3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 57 | 43 | 1 |
| 1 |
| 42 | NA | 1 |
| 1 |
|
|
High | 106 | 59 | 46 | 1.043
(0.725-1.501) | 0.821 | 0.940
(0.647-1.365) | 0.746 | 40 | NA | 0.979
(0.635-1.509) | 0.923 | 0.803
(0.513-1.259) | 0.339 |
| CST4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 52 | 51 | 1 |
| 1 |
| 35 | NA | 1 |
| 1 |
|
|
High | 106 | 64 | 40 | 1.278
(0.886-1.843) | 0.19 | 1.186
(0.821-1.713) | 0.365 | 47 | 60 | 1.325
(0.855-2.054) | 0.208 | 1.230
(0.791-1.913) | 0.357 |
| CST5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 57 | 46 | 1 |
| 1 |
| 41 | NA | 1 |
| 1 |
|
|
High | 106 | 59 | 45 | 1.041
(0.723-1.498) | 0.83 | 1.066
(0.738-1.539 | 0.735 | 41 | NA | 1.032
(0.699-1.591) | 0.888 | 1.074
(0.693-1.664) | 0.75 |
| CST6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 55 | 57 | 1 |
| 1 |
| 35 | NA | 1 |
| 1 |
|
|
High | 106 | 66 | 28 | 1.499
(1.037-2.166) | 0.031 | 1.651
(1.136-2.398) | 0.009 | 47 | 60 | 1.459
(0.942-2.260) | 0.091 | 1.618
(1.033-2.533) | 0.036 |
| CST7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 63 | 27 | 1 |
| 1 |
| 49 | 60 | 1 |
| 1 |
|
|
High | 106 | 53 | 53 | 0.695
(0.482-1.003) | 0.052 | 0.688
(0.475-0.966) | 0.048 | 33 |
| 0.579
(0.372-0.901) | 0.016 | 0.559
(0.351-0.891) | 0.014 |
| CST8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 56 | 51 | 1 |
| 1 |
| 37 | NA | 1 |
| 1 |
|
|
High | 106 | 60 | 30 | 1.139
(0.791-1.641) | 0.483 | 1.106
(0.764-1.602) | 0.592 | 45 | NA | 1.290
(0.835-1.994) | 0.251 | 1.382
(0.883-2.164) | 0.157 |
| CSTA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 59 | 46 | 1 |
| 1 |
| 38 | NA | 1 |
| 1 |
|
|
High | 106 | 57 | 40 | 1.026
(0.713-1.477) | 0.889 | 1.173
(0.811-1.696) | 0.397 | 44 | NA | 1.266
(0.820-1.955) | 0.288 | 1.473
(0.943-2.299) | 0.088 |
| CSTB |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low | 106 | 54 | 51 | 1 |
| 1 |
| 34 | NA | 1 |
| 1 |
|
|
High | 106 | 62 | 36 | 1.311
(0.910-1.889) | 0.147 | 1.164
(0.803-1.698) | 0.423 | 48 | 53 | 1.734
(1.115-2.694) | 0.014 | 1.468
(0.935-2.307) | 0.096 |
The results of CST gene survival analysis indicated
that the expression levels of CST6 and CST7 may be significantly
associated with the recurrence and mortality of patients with
HBV-related HCC. The combined impact of CST6 and CST7 on OS and RFS
of patients with HBV-related HCC was then further analyzed.
Patients were divided into four groups according to CST6 and CST7
expression: Group A, high CST6 and low CST7 expression; Group B,
low CST6 and low CST7 expression; Group C, high CST6 and high CST7
expression; Group D, low CST6 and high CST7 expression. Patients
who had low CST6 expression and high CST7 expression had a
decreased risk of recurrence (adjusted P=0.003; adjusted HR=0.431;
95% CI: 0.264-0.754; Table II;
Fig. 6A) and mortality (adjusted
P=0.001; adjusted HR=0.315; 95% CI: 0.115-0.641; Table III; Fig. 6B) in HBV-related HCC. In addition,
the nomogram indicated that both CST6 and CST7 may make a
contribution to the prognosis of HCC (Fig. 6C).
 | Figure 6.Combined effect of CST6 and CST7 on
the overall survival and recurrence-free survival of patients, and
nomogram for predicting 1-, 2- and 3-year events. (A)
Recurrence-free survival curves for the combined effect of CST6 and
CST7; (B) overall survival curves for the combined effect of CST6
and CST7. Group A, high CST6 and low CST7 expression; Group B, low
CST6 and low CST7 expression; Group C, high CST6 and high CST7
expression; Group D, low CST6 and high CST7 expression. (C)
Nomogram for predicting 1-, 2- and 3-year events (death) that
combine clinical data with CST6 and CST7 expression. AFP,
α-fetoprotein; BCLC, Barcelona Center Liver Cancer; CST,
cystatin. |
| Table II.Joint effects analysis of CST6 and
CST7 expression in the recurrence-free survival of patients with
hepatocellular carcinoma. |
Table II.
Joint effects analysis of CST6 and
CST7 expression in the recurrence-free survival of patients with
hepatocellular carcinoma.
| Group | CST6 | CST7 | Patients | No. of events | MRT (months) | Crude HR (95%
CI) | Crude P-value | Adjusted HR (95%
CI) | Adjusted
P-valuea |
|---|
| A | High | Low | 53 | 34 | 22 | 1 | – | 1 | – |
| B | Low | Low | 53 | 29 | 42 | 0.788
(0.480-1.294) | 0.48 | 0.753
(0.458-1.237) | 0.263 |
| C | High | High | 53 | 32 | 36 | 0.815
(0.503-1.322 | 0.408 | 0.880
(0.541-1.4330) | 0.608 |
| D | Low | High | 53 | 21 | NA | 0.452
(0.262-0.779) | 0.004 | 0.431
(0.264-0.754) | 0.003 |
| Table III.Joint effects analysis of CST6 and
CST7 expression in the overall survival of patients with
hepatocellular carcinoma. |
Table III.
Joint effects analysis of CST6 and
CST7 expression in the overall survival of patients with
hepatocellular carcinoma.
| Group | CST6 | CST7 | Patients | No. of events | MST (months) | Crude HR (95%
CI) | Crude P-value | Adjusted HR (95%
CI) | Adjusted
P-valuea |
|---|
| A | High | Low | 53 | 26 | 61 | 1 | – | 1 | – |
| B | Low | Low | 53 | 23 | NA | 0.849
(0.484-1.488) | 0.567 | 0.785
(0.447-1.739) | 0.399 |
| C | High | High | 53 | 21 | NA | 0.723
(0.407-1.286) | 0.27 | 0.721
(0.396-1.310) | 0.283 |
| D | Low | High | 53 | 12 | NA | 0.367
(0.185-0.728) | 0.004 | 0.315
(0.115-0.641) | 0.001 |
GSEA
A CST genome-wide RNA sequencing dataset was used
for GSEA in order to uncover the potential biological mechanisms of
CST6 and CST7 in HCC. The genome expression profile in GSE14520 was
categorized based on CST6 and CST7 median gene expression values.
GSEA results of the c2 reference gene set are shown in Table SII, in which increased CST7
expression was associated with tumor evasion and tolerogenicity,
cancer progenitors, liver cancer late recurrence, liver cancer
progression and several liver cancer subclasses (Fig. 7A-I). The enrichment results of c5
are shown in Table SIII; high CST7
expression was revealed to also be involved in positive regulation
of the tumor necrosis factor subfamily cytokine production,
positive regulation of NF-κB transcription factor and positive
regulation of G1-S transition of mitotic cell cycle
(Fig. 7J-L). Conversely, the GSEA
results of CST6 did not exhibit a significant association between
CST6 and biological pathways relevant to HCC.
Discussion
It has been reported that cysteine proteases are
involved in the progression of several types of tumor (9). Destruction and remodeling of the ECM
is an essential process in tumor progression (35), which can be promoted by cysteine
proteases (36), particularly
cathepsin B, a representative cysteine protease that serves a key
role in tumor cell invasion (37–39).
However, biological functions of cysteine proteases are inhibited
by CSTs (11). Therefore, CSTs may
also be associated with tumor progression. Notably, CSTs have been
reported to be associated with the progression of various types of
cancer, including bladder cancer (40), breast cancer (41,42),
esophageal cancer (43), ovarian
cancer (44) and prostate cancer
(45). The results of GSEA in the
present study indicated that CST7 was significantly enriched in
liver cancer progression. Co-expression analysis of the CST genes
in GSE14520 using Pearson's correlation coefficient revealed that
CST1, CST2 and CST4 are closely associated with each other,
verifying the results of GeneMANIA and STRING.
CST7 expression was markedly decreased in HCC tissue
samples, whereas CSTB was highly expressed in HCC tumor tissue. ROC
analysis indicated that CST7 and CSTB exhibit significant
diagnostic values and may serve as potential diagnostic biomarkers.
The diagnostic value of CST genes has been reported in previous
studies. Having higher expression in HCC compared with in adjacent
healthy tissues, the diagnostic value of CSTB for HCC was reported
in previous research, and the present investigation provided
validation for this (14,16,46).
In addition to HCC, the diagnostic value of CSTB has been reported
in other tumor types. For example, compared with in normal bladder
tissue, CSTB immunohistochemical staining is more intense in
bladder cancer tissue (40). CSTB
has also been demonstrated to be a diagnostic biomarker of ovarian
clear cell carcinoma, due to its high expression in tumor cells
based on the results of immunohistochemical analysis, reverse
transcription-PCR and western blot analysis (47).
The survival analysis of CST genes indicated that
CST6 and CST7 may be strongly associated with the OS and RFS of
patients with HBV-related HCC. The combined effects survival
analysis indicated that the risks of mortality and recurrence in
patients with HBV-related HCC were lowest in those with increased
expression of CST7 and attenuated expression of CST6. Therefore,
CST7 and CST6 may function as prognostic biomarkers for HCC. The
prognostic value of CST genes has been reported across several
malignancies. It has been reported that overexpression of CST6
promotes pancreatic cancer growth (48). The function of CST6 was revealed to
be similar in the present study, where the survival analysis
results indicated that high CST6 expression was associated with
poor survival of patients with HCC. However, CST6 has also been
reported to act as a human tumor suppressor gene in previous
reports (45,49–54).
Therefore, these findings indicated that CST6 may exert distinct
effects in different types of cancer. The similar role of CST6 in
the liver and pancreas may be a result of the liver and pancreas
stemming from a common progenitor at the embryo stage (55). The fact that the molecular mechanism
of CST6 serves different roles in various types of cancer still
requires further exploration. Although no significant association
was detected between CSTB and the prognosis of patients with HCC,
differences have been reported in the expression of CSTB between
tumor tissues and adjacent healthy tissues (16,46,56).
In addition, the prognostic value of CSTB has been demonstrated in
several other tumors. For example, high CSTB expression is
associated with a more favorable prognosis in lung cancer (57). A similar scenario of CSTB
functioning as a prognostic biomarker has been reported in gastric
cancer, where it restrains tumor development by suppressing
proliferation and migration of neoplastic cells (58). The present study did not determine a
prognostic value of CST3 in HCC; however, CST3 has been
demonstrated to act as a tumor suppresser that restrains tumor cell
invasion in previous studies (56,59). A
recent study reported that the rate of glomerular filtration of
creatinine and CST3 may serve as potential predictors of OS in HCC
(60). By reviewing these studies,
the different roles of CST genes in numerous types of cancer can be
identified. The present results corresponded with the results of
previous studies. Although in the same subfamily, the expression
levels and biological functions of each CST gene are not the same
as those of others, even in different types of cancer. CST genes
may also function as oncogenes; however, further studies are needed
to validate the present findings.
The GSEA conducted in the present study revealed
that CST7 was enriched in tumor evasion and tolerogenicity, cancer
progenitors, liver cancer late recurrence, liver cancer
progression, several liver cancer subclasses, tumor necrosis factor
subfamily cytokine production, regulation of NF-κB transcription
factor and regulation of G1-S transition of the mitotic
cell cycle. These results suggested that CST7 may be closely
associated with liver cancer. However, the association between CST
genes and HCC requires further validation in future studies. In
addition, although GSEA of CST6 indicated that CST6 was not
involved in any pathway or molecular mechanism associated with
cancer, the effects of CST6 on different types of cancer have been
confirmed by previous studies (45,49–54).
One limitation of the present study was that the
sample size was insufficient, which could affect the validity of
the results. Secondly, the clinical data obtained from the GSE14520
dataset are not complete, barring the opportunity to carry out a
more comprehensive survival analysis using multivariate Cox
proportional hazards regression model. In order to better evaluate
the association between CST subfamily members and HCC prognosis,
likely HCC risk factors, including the presence of a tumor capsule
and vascular invasion, Child-Pugh score and alcohol intake, should
be taken into consideration. Thirdly, the current investigation
only explored the relationship between CST gene mRNA expression and
HCC prognosis and did not explore the effects of CST protein levels
on HCC prognosis. Finally, further studies are warranted to
determine the effects of Family 3 and Family 4 CSTs on HCC.
Although there are several limitations to the
present study, to the best of our knowledge, this is the first to
discover the clinical significance of CST6 and CST7 in the
prognosis of patients with HBV-related HCC. In addition, our result
verified the findings of previous reports and suggested that CSTB
may act as a diagnostic biomarker for HCC. Furthermore, CST7 was
discovered to be enriched in several tumor-related signaling
pathways and biological processes, including tumor evasion and
tolerogenicity, cancer progenitors, liver cancer late recurrence,
liver cancer progression, several liver cancer subclasses, tumor
necrosis factor subfamily cytokine production, regulation of NF-κB
transcription factor and regulation of G1-S transition
of the mitotic cell cycle. The prospective molecular mechanisms
underlying the effects of CST7 gene expression on patients with
HBV-related HCC were determined using GSEA.
In conclusion, the gene expression levels of CST1,
CST2, CST5, CSTA and CSTB were significantly increased in HCC
tissue, whereas CST3 and CST7 were overexpressed in normal tissue
compared with in HCC tissue. Notably, the present study revealed
that CST7 and CSTB may serve as diagnostic markers for HCC, and
survival analysis of CST genes indicated that CST6 and CST7
expression levels may be closely associated with the OS and RFS of
patients with HCC. However, this investigation requires further
validation using a sufficient sample size spread across multiple
geographical regions.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This study was supported in part by the National
Natural Science Foundation of China (grant nos. 81560535, 81802874,
81072321, 30760243, 30460143 and 30560133), the Natural Science
Foundation of Guangxi Province of China (grant no. 2017JJB140189y),
the 2009 Program for New Century Excellent Talents in University
(NCET), Guangxi Natural Sciences Foundation (grant no. GuiKeGong
1104003A-7) and the Guangxi Health Ministry Medicine Grant (Key
Scientific Research Grant; grant no. Z201018). The present study
was also partly supported by the Scientific Research Fund of the
Health and Family Planning Commission of Guangxi Zhuang Autonomous
Region (grant no. Z2016318), the Key Laboratory of High Incidence
Tumor Prevention & Treatment (Guangxi Medical University),
Ministry of Education (grant no. GKE2018-01), the Basic Ability
Improvement Project for Middle-aged and Young Teachers in Colleges
and Universities in Guangxi (grant no. 2018KY0110), the Innovation
Project of Guangxi Graduate Education (grant no. JGY2018037) the
2018 Innovation Project of Guangxi Graduate Education (grant no.
YCBZ2018036), and the Research Institute of Innovative Think-tank
at Guangxi Medical University (the gene-environment interaction in
hepatocarcinogenesis in Guangxi HCCs and its translational
applications in the HCC prevention). The authors would also like to
acknowledge the support provided by the National Key Clinical
Specialty Programs (General Surgery & Oncology) and the Key
Laboratory of Early Prevention & Treatment for Regional
High-Incidence-Tumor (Guangxi Medical University), Ministry of
Education, China. This work was also supported in part by the
Natural Science Foundation of Guangxi Province of China (grant no.
2018GXNSFBA138013), the Key Laboratory of High-Incidence-Tumor
Prevention & Treatment (Guangxi Medical University) and the
Guangxi Key R & D Program (grant no. GKEAB18221019).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XZ and TP conceived and designed the study. XW, KH,
XL, CY, TY, JL, CH, GZ, HS, WQ, QH, ZL, JH, YG, XY and TP acquired
the data and performed data analyses. XZ wrote the manuscript, and
TP guided and supervised the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declared that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Njei B, Rotman Y, Ditah I and Lim JK:
Emerging trends in hepatocellular carcinoma incidence and
mortality. Hepatology. 61:191–199. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zeng H, Zheng R, Guo Y, Zhang S, Zou X,
Wang N, Zhang L, Tang J, Chen J, Wei K, et al: Cancer survival in
China, 2003-2005: A population-based study. Int J Cancer.
136:1921–1930. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Altekruse SF, McGlynn KA and Reichman ME:
Hepatocellular carcinoma incidence, mortality, and survival trends
in the United States from 1975 to 2005. J Clin Oncol. 27:1485–1491.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Volk ML and Marrero JA: Early detection of
liver cancer: Diagnosis and management. Curr Gastroenterol Rep.
10:60–66. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sawyers CL: The cancer biomarker problem.
Nature. 452:548–552. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gora J and Latajka R: Involvement of
cysteine proteases in cancer. Curr Med Chem. 22:944–957. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ochieng J and Chaudhuri G: Cystatin
superfamily. J Health Care Poor Underserved. 21 (Suppl 1):S51–S70.
2010. View Article : Google Scholar
|
|
11
|
Turk V, Stoka V and Turk D: Cystatins:
Biochemical and structural properties, and medical relevance. Front
Biosci. 13:5406–5420. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sinha AA, Gleason DF, Deleon OF, Wilson MJ
and Sloane BF: Localization of a biotinylated cathepsin B
oligonucleotide probe in human prostate including invasive cells
and invasive edges by in situ hybridization. Anat Rec. 235:233–240.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Visscher DW, Sloane BF, Sameni M, Babiarz
JW, Jacobson J and Crissman JD: Clinicopathologic significance of
cathepsin B immunostaining in transitional neoplasia. Mod Pathol.
7:76–81. 1994.PubMed/NCBI
|
|
14
|
Lin YY, Chen ZW, Lin ZP, Lin LB, Yang XM,
Xu LY and Xie Q: Tissue levels of stefin A and stefin B in
hepatocellular carcinoma. Anat Rec (Hoboken). 299:428–438. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zinkin NT, Grall F, Bhaskar K, Otu HH,
Spentzos D, Kalmowitz B, Wells M, Guerrero M, Asara JM, Libermann
TA and Afdhal NH: Serum proteomics and biomarkers in hepatocellular
carcinoma and chronic liver disease. Clin Cancer Res. 14:470–477.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lee MJ, Yu GR, Park SH, Cho BH, Ahn JS,
Park HJ, Song EY and Kim DG: Identification of cystatin B as a
potential serum marker in hepatocellular carcinoma. Clin Cancer
Res. 14:1080–1089. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dennis G Jr, Sherman BT, Hosack DA, Yang
J, Gao W, Lane HC and Lempicki RA: DAVID: Database for annotation,
visualization, and integrated discovery. Genome Biol. 4:P32003.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Huang DW, Sherman BT, Tan Q, Kir J, Liu D,
Bryant D, Guo Y, Stephens R, Baseler MW, Lane HC and Lempicki RA:
DAVID bioinformatics resources: Expanded annotation database and
novel algorithms to better extract biology from large gene lists.
Nucleic Acids Res 35 (Web Server issue). W169–W175. 2007.
View Article : Google Scholar
|
|
19
|
Warde-Farley D, Donaldson SL, Comes O,
Zuberi K, Badrawi R, Chao P, Franz M, Grouios C, Kazi F, Lopes CT,
et al: The GeneMANIA prediction server: Biological network
integration for gene prioritization and predicting gene function.
Nucleic Acids Res 38 (Web Server issue). W214–W220. 2010.
View Article : Google Scholar
|
|
20
|
Montojo J, Zuberi K, Rodriguez H, Bader GD
and Morris Q: GeneMANIA: Fast gene network construction and
function prediction for Cytoscape. F1000Res. 3:1532014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
von Mering C, Huynen M, Jaeggi D, Schmidt
S, Bork P and Snel B: STRING: A database of predicted functional
associations between proteins. Nucleic Acids Res. 31:258–261. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Szklarczyk D, Morris JH, Cook H, Kuhn M,
Wyder S, Simonovic M, Santos A, Doncheva NT, Roth A, Bork P, et al:
The STRING database in 2017: Quality-controlled protein-protein
association networks, made broadly accessible. Nucleic Acids Res.
45:D362–D368. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cancer Genome Atlas Research Network.
Electronic address, . simplewheeler@bcm.edu; Cancer
Genome AtlasResearch Network: Comprehensive and integrative genomic
characterization of hepatocellular carcinoma. Cell.
169:1327–1341.e23. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liao X, Liu X, Yang C, Wang X, Yu T, Han
C, Huang K, Zhu G, Su H, Qin W, et al: Distinct diagnostic and
prognostic values of minichromosome maintenance gene expression in
patients with hepatocellular carcinoma. J Cancer. 9:2357–2373.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Roessler S, Long EL, Budhu A, Chen Y, Zhao
X, Ji J, Walker R, Jia HL, Ye QH, Qin LX, et al: Integrative
genomic identification of genes on 8p associated with
hepatocellular carcinoma progression and patient survival.
Gastroenterology. 142:957–966e12. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hoo ZH, Candlish J and Teare D: What is an
ROC curve? Emerg Med J. 34:357–359. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ma H, Bandos AI, Rockette HE and Gur D: On
use of partial area under the ROC curve for evaluation of
diagnostic performance. Stat Med. 32:3449–3458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Balachandran VP, Gonen M, Smith JJ and
DeMatteo RP: Nomograms in oncology: More than meets the eye. Lancet
Oncol. 16:e173–e180. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Subramanian A, Tamayo P, Mootha VK,
Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub
TR, Lander ES and Mesirov JP: Gene set enrichment analysis: A
knowledge-based approach for interpreting genome-wide expression
profiles. Proc Natl Acad Sci USA. 102:15545–15550. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Liberzon A, Birger C, Thorvaldsdóttir H,
Ghandi M, Mesirov JP and Tamayo P: The molecular signatures
database (MSigDB) hallmark gene set collection. Cell Syst.
1:417–425. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
François O, Martins H, Caye K and
Schoville SD: Controlling false discoveries in genome scans for
selection. Mol Ecol. 25:454–469. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Glickman ME, Rao SR and Schultz MR: False
discovery rate control is a recommended alternative to
Bonferroni-type adjustments in health studies. J Clin Epidemiol.
67:850–857. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Reiner A, Yekutieli D and Benjamini Y:
Identifying differentially expressed genes using false discovery
rate controlling procedures. Bioinformatics. 19:368–375. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Llovet JM, Brú C and Bruix J: Prognosis of
hepatocellular carcinoma: The BCLC staging classification. Semin
Liver Dis. 19:329–338. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Liotta LA, Rao CN and Barsky SH: Tumor
invasion and the extracellular matrix. Lab Invest. 49:636–649.
1983.PubMed/NCBI
|
|
36
|
Cudic M and Fields GB: Extracellular
proteases as targets for drug development. Curr Protein Pept Sci.
10:297–307. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yan S, Sameni M and Sloane BF: Cathepsin B
and human tumor progression. Biol Chem. 379:113–123.
1998.PubMed/NCBI
|
|
38
|
Mirković B, Markelc B, Butinar M, Mitrović
A, Sosič I, Gobec S, Vasiljeva O, Turk B, Čemažar M, Serša G and
Kos J: Nitroxoline impairs tumor progression in vitro and in vivo
by regulating cathepsin B activity. Oncotarget. 6:19027–19042.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Aggarwal N and Sloane BF: Cathepsin B:
Multiple roles in cancer. Proteomics Clin Appl. 8:427–437. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Feldman AS, Banyard J, Wu CL, McDougal WS
and Zetter BR: Cystatin B as a tissue and urinary biomarker of
bladder cancer recurrence and disease progression. Clin Cancer Res.
15:1024–1031. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Leto G, Incorvaia L, Flandina C, Ancona C,
Fulfaro F, Crescimanno M, Sepporta MV and Badalamenti G: Clinical
impact of cystatin C/cathepsin L and follistatin/activin A systems
in breast cancer progression: A preliminary report. Cancer Invest.
34:415–423. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ai L, Kim WJ, Kim TY, Fields CR, Massoll
NA, Robertson KD and Brown KD: Epigenetic silencing of the tumor
suppressor cystatin M occurs during breast cancer progression.
Cancer Res. 66:7899–7909. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Shiba D, Terayama M, Yamada K, Hagiwara T,
Oyama C, Tamura-Nakano M, Igari T, Yokoi C, Soma D, Nohara K, et
al: Clinicopathological significance of cystatin A expression in
progression of esophageal squamous cell carcinoma. Medicine
(Baltimore). 97:e03572018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Wang X, Gui L, Zhang Y, Zhang J, Shi J and
Xu G: Cystatin B is a progression marker of human epithelial
ovarian tumors mediated by the TGF-β signaling pathway. Int J
Oncol. 44:1099–1106. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Pulukuri SM, Gorantla B, Knost JA and Rao
JS: Frequent loss of cystatin E/M expression implicated in the
progression of prostate cancer. Oncogene. 28:2829–2838. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Unić A, Derek L, Duvnjak M, Patrlj L,
Rakić M, Kujundžić M, Renjić V, Štoković N, Dinjar P, Jukic A and
Grgurević I: Diagnostic specificity and sensitivity of PIVKAII,
GP3, CSTB, SCCA1 and HGF for the diagnosis of hepatocellular
carcinoma in patients with alcoholic liver cirrhosis. Ann Clin
Biochem. 55:355–362. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Takaya A, Peng WX, Ishino K, Kudo M,
Yamamoto T, Wada R, Takeshita T and Naito Z: Cystatin B as a
potential diagnostic biomarker in ovarian clear cell carcinoma. Int
J Oncol. 46:1573–1581. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Li Q, Zheng ZC, Ni CJ, Jin WX, Jin YX,
Chen Y, Zhang XH, Chen ED and Cai YF: Correlation of cystatin E/M
with clinicopathological features and prognosis in triple-negative
breast cancer. Ann Clin Lab Sci. 48:40–44. 2018.PubMed/NCBI
|
|
49
|
Soh H, Venkatesan N, Veena MS,
Ravichandran S, Zinabadi A, Basak SK, Parvatiyar K, Srivastava M,
Liang LJ, Gjertson DW, et al: Cystatin E/M suppresses tumor cell
growth through cytoplasmic retention of NF-κB. Mol Cell Biol.
36:1776–1792. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Shridhar R, Zhang J, Song J, Booth BA,
Kevil CG, Sotiropoulou G, Sloane BF and Keppler D: Cystatin M
suppresses the malignant phenotype of human MDA-MB-435S cells.
Oncogene. 23:2206–2215. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kioulafa M, Balkouranidou I, Sotiropoulou
G, Kaklamanis L, Mavroudis D, Georgoulias V and Lianidou ES:
Methylation of cystatin M promoter is associated with unfavorable
prognosis in operable breast cancer. Int J Cancer. 125:2887–2892.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Chen X, Cao X, Dong W, Xia M, Luo S, Fan Q
and Xie J: Cystatin M expression is reduced in gastric carcinoma
and is associated with promoter hypermethylation. Biochem Biophys
Res Commun. 391:1070–1074. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Qiu J, Ai L, Ramachandran C, Yao B,
Gopalakrishnan S, Fields CR, Delmas AL, Dyer LM, Melnick SJ,
Yachnis AT, et al: Invasion suppressor cystatin E/M (CST6):
High-level cell type-specific expression in normal brain and
epigenetic silencing in gliomas. Lab Invest. 88:910–925. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Veena MS, Lee G, Keppler D, Mendonca MS,
Redpath JL, Stanbridge EJ, Wilczynski SP and Srivatsan ES:
Inactivation of the cystatin E/M tumor suppressor gene in cervical
cancer. Genes Chromosomes Cancer. 47:740–754. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
McCarthy DJ, Chen Y and Smyth GK:
Differential expression analysis of multifactor RNA-Seq experiments
with respect to biological variation. Nucleic Acids Res.
40:4288–4297. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Ji NY, Kang YH, Park MY, Lee CI, Kim MK,
Kim DG, Kim JW and Song EY: Development of a fluorescent
microsphere immunoassay for cystatin B (CSTB) in serum of patients
with hepatocellular carcinoma. Clin Chem Lab Med. 49:151–155. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Ma Y, Chen Y and Petersen I: Expression
and epigenetic regulation of cystatin B in lung cancer and
colorectal cancer. Pathol Res Pract. 213:1568–1574. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Zhang J, Shi Z, Huang J and Zou X: CSTB
downregulation promotes cell proliferation and migration and
suppresses apoptosis in gastric cancer SGC-7901 cell line. Oncol
Res. 24:487–494. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Coulibaly S, Schwihla H, Abrahamson M,
Albini A, Cerni C, Clark JL, Ng KM, Katunuma N, Schlappack O,
Glössl J and Mach L: Modulation of invasive properties of murine
squamous carcinoma cells by heterologous expression of cathepsin B
and cystatin C. Int J Cancer. 83:526–531. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Tamai Y, Iwasa M, Kawasaki Y, Yoshizawa N,
Ogura S, Sugimoto R, Eguchi A, Yamamoto N, Sugimoto K, Hasegawa H
and Takei Y: Ratio between estimated glomerular filtration rates of
creatinine and cystatin C predicts overall survival in patients
with hepatocellular carcinoma. Hepatol Res. 49:153–163. 2019.
View Article : Google Scholar : PubMed/NCBI
|