Introduction
Ovarian cancer accounted for ~152,000 mortalities
annually globally in 2012 (1). Among
the histological subtypes of ovarian cancer, ovarian clear cell
carcinoma occurs more frequently in the Asian region, particularly
in Japan (15–25%), compared with North America and Europe (1–12%),
and is less sensitive to platinum-based chemotherapy with poorer
prognosis, compared with serous adenocarcinoma (2–8).
Therefore, more effective treatments are urgently required.
The GOG-0218 study demonstrated that
progression-free survival (PFS) was significantly prolonged in
patients with advanced epithelial ovarian cancer who received
bevacizumab maintenance following induction therapy with
carboplatin and paclitaxel plus bevacizumab, compared with PFS in
patients who received induction therapy with carboplatin and
paclitaxel plus bevacizumab without maintenance therapy, or in
patients who received induction therapy with carboplatin and
paclitaxel without maintenance therapy (9). These data resulted in the recommendation
of the former regimen as the primary systemic therapy for patients
with ovarian cancer with stage IV in guidelines, such as the NCCN
guidelines (10). However, in that
global study, the histotype in the majority of patients was serous
carcinoma and the proportion of patients with clear cell carcinoma
was as low as 2.9%. Hence, there has been insufficient verification
of the effectiveness against ovarian clear cell carcinoma of
bevacizumab maintenance following induction therapy with
carboplatin and paclitaxel plus bevacizumab.
Furthermore, although the effectiveness of
continuous administration of bevacizumab in second-line treatment
of patients with disease progression following combination therapy,
including bevacizumab (bevacizumab beyond progression), has been
demonstrated in metastatic colorectal cancer (11), the effectiveness of bevacizumab beyond
progression has not been demonstrated in ovarian cancer.
Bevacizumab is a humanized monoclonal antibody
against vascular endothelial cell growth factor (VEGF) that reduces
abnormal blood vessels and inhibits VEGF-mediated angiogenesis in
numerous cancer types, including colorectal cancer, renal cell
carcinoma, non-small cell lung cancer, breast cancer, ovarian
cancer and glioblastoma multiforme (12,13).
Paclitaxel is a taxane-based chemotherapeutic agent that stops the
cell cycle by inhibiting tubulin depolymerization, thereby
inhibiting cell division (14). It
has been used in combination with carboplatin and bevacizumab in
the primary treatment of metastatic ovarian cancer (10). Additionally, PEGylated liposomal
doxorubicin, a formulation in which doxorubicin hydrochloride is
encapsulated in polyethylene glycolated liposomes, has been used as
monotherapy in recurrent ovarian cancer (15,16).
In the present study, a human ovarian clear cell
carcinoma xenograft model was used to investigate the antitumor
effects and mechanisms of bevacizumab maintenance following
induction treatment, including bevacizumab, and those of
bevacizumab beyond progression.
Materials and methods
Antitumor agents
Bevacizumab was manufactured by Chugai
Pharmaceutical Co., Ltd. (Tokyo, Japan) as a solution and diluted
to 5 mg/kg body weight (0.2 ml/mouse) with saline. Human
immunoglobulin G (HuIgG) was purchased from MP Biomedicals, LLC
(Santa Ana, CA, USA), and was reconstituted with water and diluted
to 5 mg/kg body weight (0.2 ml/mouse) with saline (Otsuka
Pharmaceutical Co., Ltd., Tokyo, Japan). Paclitaxel was purchased
from Wako Pure Chemical Industries, Ltd. (Osaka, Japan) and was
reconstituted with 50% ethanol-50% Cremophor EL, and immediately
prior to administration was diluted 10-fold with saline. PEGylated
liposomal doxorubicin was purchased from Janssen Pharmaceutical,
Inc. (Beerse, Belgium) as a solution and diluted to 20 mg/kg body
weight (10 ml/kg body weight) with saline.
Animals
A total of 908 female, 5-week-old BALB/c-nu/nu mice
were purchased from Charles River Laboratories Japan, Inc.
(Kanagawa, Japan) or CLEA Japan, Inc. (Tokyo, Japan). All animals
were housed in a specific pathogen-free environment under
controlled conditions (temperature, 20–26°C; humidity, 35–75%;
12/12 h light/dark cycle) and were allowed to acclimatize and
recover from shipping-associated stress for >6 days prior to the
study. Body weight of the mice at the time of randomization was
14.9–25.6 g. Chlorinated water and irradiated food were provided
ad libitum. The health of the mice was monitored by daily
observation. All animal experiments were reviewed and approved by
the Institutional Animal Care and Use Committee at Chugai
Pharmaceutical Co., Ltd. (approval no. 13-225, 15-201; Kamakura,
Japan).
Cell lines and culture conditions
A total of two human ovarian cancer cell lines were
used in the present study: SK-OV-3, which was established from the
ascites fluid of a patient with ovarian serous adenocarcinoma and
was demonstrated to be platinum-sensitive (17); and RMG-I, which was established from
the ascites fluid of a patient with ovarian clear cell carcinoma
and was immunohistochemically confirmed to be clear cell carcinoma
(18). SK-OV-3 cells were obtained
from the American Type Culture Collection (Manassas, VA, USA) and
were maintained by in vivo passage in BALB/c-nu/nu mice.
RMG-I cells were obtained from National Institute of Biomedical
Innovation (Osaka, Japan) and were maintained in Hams F-12 Nutrient
Mixture (Thermo Fisher Scientific, Inc., Waltham, MA, USA)
supplemented with 10% FBS (Bovogen Biologicals, Melbourne,
Australia). All cells were cultured at 37°C in 5%
CO2.
In vivo tumor growth inhibition
studies
Each BALB/c-nu/nu mouse was inoculated
subcutaneously into the right flank with SK-OV-3 (8-mm3
tumor block) or RMG-I (5×106 cells). After 2–5 weeks of
tumor inoculation, mice whose tumor had grown were randomly
allocated to control, bevacizumab, paclitaxel, and paclitaxel plus
bevacizumab induction treatment groups (week 1).
As the induction treatment in the SK-OV-3 and RMG-I
xenograft models, HuIgG or bevacizumab (5 mg/kg, the maximum
effective dose; intraperitoneally injected) and paclitaxel vehicle
(5% ethanol-5% Cremophor EL-saline; intravenously injected) or
paclitaxel (40 mg/kg, the optimum dose to evaluate the combination
efficacy in the SK-OV-3 ×enograft model, intravenously injected; 80
mg/kg, the maximum tolerated dose, in the RMG-I xenograft model,
intravenously injected) were administered on weeks 1, 2 and 3.
On week 4, mice subjected to the induction treatment
were subsequently subjected to control or bevacizumab maintenance
treatment. When transitioning from a group of induction treatment
to two groups of maintenance treatment, re-randomization was
performed. As maintenance treatment, HuIgG or bevacizumab was
administered weekly until 1 week prior to the date of the last
tumor measurement (week 6, Fig. 1;
week 9, Fig. 3B) or 1 day prior to
the last tumor measurement (week 9, Fig.
3A).
 | Figure 1.Antitumor activity of BEV maintenance
following PTX plus BEV induction treatment in SK-OV-3 and RMG-I
xenograft models. (A) Mice bearing SK-OV-3 tumors were randomly
divided into four groups (n=6/group) and were treated with control
(vehicle for PTX or HuIgG for BEV), BEV, PTX or PTX+BEV on weeks 1,
2, and 3 as induction treatment, and subsequently treated weekly
with control or BEV as maintenance treatment. The control induction
group and BEV induction group were examined until week 4, as
scheduled. The dosage of PTX and BEV was 40 and 5 mg/kg,
respectively. (B) Mice bearing RMG-I tumors were randomly divided
into four groups and treated with control (vehicle for PTX or HuIgG
for BEV), BEV, PTX or PTX+BEV on weeks 1, 2, and 3 as induction
treatment, and subsequently treated weekly with control or BEV as
maintenance treatment (n=6–7). The dosage of PTX and BEV was 80 and
5 mg/kg, respectively. A total of one mouse with intraperitoneal
tumor in the BEV maintenance following BEV induction treatment
group was excluded from data analysis. Data points represent the
mean + standard deviation of tumor volume (mm3).
*P<0.05, Wilcoxon test (B) with or (A) without Holm-Bonferroni
correction. BEV, bevacizumab; PTX, paclitaxel. |
 | Figure 3.Antitumor activity of BEV maintenance
treatment vs control maintenance treatment following PTX plus
bevacizumab induction treatment in the RMG-I xenograft model. (A)
Mice bearing RMG-I tumors were randomly divided into four groups:
Control induction group (n=7); BEV induction group (n=7); PTX
induction group (n=7); and PTX+BEV induction group (n=16), and were
treated with control (vehicle for PTX or HuIgG for BEV), BEV, PTX
or PTX+BEV, respectively, on weeks 1, 2, and 3. On week 4, mice
receiving PTX+BEV induction treatments were re-randomized into a
control maintenance and a BEV maintenance group (n=8 per group).
Mice were subsequently treated weekly with control (HuIgG) or BEV
as maintenance treatment. Data points represent the mean + standard
deviation of tumor volume (mm3). *P<0.05 and
$P<0.05, Wilcoxon test with Holm-Bonferroni
correction; #P<0.05, Wilcoxon test. (B) Mice bearing
RMG-I tumors were randomly divided into two groups: PTX induction
group; and PTX+BEV induction group, and were treated with PTX or
PTX+BEV, respectively, on weeks 1, 2, and 3. From week 4, mice
receiving induction treatments were subsequently treated weekly
with BEV as maintenance treatment (n=6–7). A total of one mouse was
accidentally administered in the BEV maintenance following PTX+BEV
induction treatment group was excluded from data analysis on week
4. Data points represent the mean + standard deviation of tumor
volume (mm3). *P<0.05, Wilcoxon test. (C) Tumor
microvessels stained immunohistochemically with antibody against
CD31 on week 9. (D) The MVD in tumor tissue was determined by
calculating the ratio of CD31-positive area to the total observed
area. The dosage of PTX and BEV was 80 and 5 mg/kg, respectively.
Data represent the mean + standard deviation (n=6–7). *P<0.05,
Wilcoxon test. BEV, bevacizumab; PTX, paclitaxel; MVD, microvessel
density. |
For experiments of the second-line treatment, mice
were treated with paclitaxel plus bevacizumab induction and then
continuous bevacizumab maintenance, as aforementioned (n=110).
Tumor regrowth was defined as a consecutive increase in tumor
volume exceeding 10%/week during bevacizumab maintenance. Mice
bearing regrown tumors (with a volume of 240–720 mm3)
were randomly allocated to each of the second-line control,
bevacizumab, PEGylated liposomal doxorubicin, and PEGylated
liposomal doxorubicin plus bevacizumab treatment groups
(n=7/group). HuIgG or bevacizumab (5 mg/kg, the maximum effective
dose; intraperitoneally injected) and PEGylated liposomal
doxorubicin vehicle (saline; intravenously injected) or PEGylated
liposomal doxorubicin (20 mg/kg, the maximum tolerated dose in the
RMG-I xenograft model; intravenously injected) were administered,
weekly and once every 3 weeks, respectively, until 1 week prior to
the date of the last tumor measurement (week 15 in the second-line
control or bevacizumab treatment groups; and week 22 in the
second-line PEGylated liposomal doxorubicin or PEGylated liposomal
doxorubicin plus bevacizumab treatment groups).
Tumor volume was measured once or twice a week.
Tumor volume was estimated from the equation: Tumor volume =
ab2/2, where a and b are tumor length and width,
respectively. Individuals that succumbed due to accidental
administration or individuals whose tumor self-destructed were
excluded. The experimental protocol mandated that tumor volume
measurement in both the second-line control group and the
second-line bevacizumab group was to end whenever tumor
self-destruction or blister breakage was observed in three or more
mice in the second-line control or second-line bevacizumab groups.
When tumor measurement was terminated by blister breakage, tumor
samples were collected within 4 days from a site that was less
affected by blister breakage.
Immunohistochemistry and
quantification of microvessel density (MVD) in tumor tissues
Immunohistochemical analyses of CD31 was conducted
using a Rat Horseradish Peroxidase (HRP)-Polymer 1-Step (Mouse
adsorbed) system (cat. no. BRR4016; Biocare Medical, LLC, Pacheco,
CA, USA) according to the manufacturers protocols. Subsequently,
5-µm thick sections from optimal cutting temperature
compound-embedded freshly frozen tissues were fixed in 4%
paraformaldehyde at 4°C for 10 min. The endogenous peroxidase
activity and endogenous non-specific background were blocked with
0.3% hydrogen peroxide at room temperature for 30 min and Rodent
Block M (undiluted; cat. no. RBM961, Biocare Medical, LLC) at room
temperature for 30 min. The tissue sections were incubated at 4°C
overnight with rat anti-mouse CD31 monoclonal antibody (clone MEC
13.3; 1:500; cat. no. 553370, BD Biosciences; Becton-Dickinson and
Company, Franklin Lakes, NJ, USA) as the primary antibody.
Subsequently, the sections were incubated at room temperature with
the Rat HRP-Polymer 1-Step (Mouse adsorbed; undiluted) for 30 min.
Staining was conducted at room temperature using
3,3-diaminobenzidine solution (DAB+, Liquid, 2-component system;
cat. no. K3468; Agilent Technologies, Inc., Santa Clara, CA, USA)
for 5 min. All sections were counterstained at room temperature
with hematoxylin for 2 sec. Tumor samples from freshly frozen
tissues were collected on weeks 6, 9, 16 and 22. MVD (%) was
calculated from the ratio of the CD31-positive staining area to the
total observation area in the viable region. A total of 3–6
fields/section were analyzed at a magnification of ×100 with a
light microscope (ECLIPSE Ni; Nikon Corporation, Tokyo, Japan),
excluding necrotic areas. Positive-staining areas were calculated
using imaging analysis software (WinROOF Version 6.3.1; Mitani
Corporation, Fukui, Japan).
Human angiogenesis array and human
insulin like growth factor binding protein-3 (IGFBP-3) ELISA
assay
Tumor tissues collected from xenografts and stored
at −80°C were homogenized with Cell Lysis buffer (Cell Signaling
Technology, Inc., Danvers, MA, USA) with Complete Protease
Inhibitor Cocktail Tablets and Complete Phosphatase Inhibitor
Cocktail Tablets (both from Roche Diagnostics, Basel, Switzerland).
The homogenate was centrifuged at 9,100 × g at 4°C for 20 min. The
resultant supernatant was used for the assays as cell lysates.
Protein concentration of the cell lysates was quantified using a
Direct Detect spectrometer (Merck KGaA, Darmstadt, Germany). Human
Angiogenesis Array and Human IGFBP-3 ELISA (both from R&D
Systems, Inc., Minneapolis, MN, USA) were performed using the cell
lysates. ImageQuant 400 (GE Healthcare Life Sciences, Little
Chalfont, UK) was used for detection of the Human Angiogenesis
Array.
Statistical analysis
Data were presented as mean + standard deviation,
and analyzed with the Wilcoxon test. For comparison between the two
groups, P<0.05 was considered to indicate a statistically
significant difference. For multiple comparison, the P-values were
corrected by the Holm-Bonferroni method (19). All statistical analyses were conducted
using JMP software (SAS Institute, Inc., Cary, NC, USA).
Results
Antitumor activity of bevacizumab
maintenance treatment following paclitaxel plus bevacizumab
induction treatment
Firstly, the efficacy of bevacizumab treatment in
the induction and maintenance phases in the human ovarian serous
carcinoma cell line SK-OV-3 ×enograft model and in the human
ovarian clear cell carcinoma cell line RMG-I xenograft model was
evaluated. In the SK-OV-3 ×enograft model, tumor volume in the
bevacizumab maintenance following paclitaxel plus bevacizumab
induction treatment group on week 6 was significantly reduced,
compared with the control maintenance following paclitaxel
induction treatment group (Fig. 1A).
A similar effect was observed in the RMG-I xenograft model, with
the tumor volume in the bevacizumab maintenance following
paclitaxel plus bevacizumab induction group on week 6 being
significantly reduced, compared with the control maintenance
following paclitaxel induction group (Fig. 1B), indicating that the addition of
bevacizumab during and following paclitaxel induction was notable
in ovarian serous and clear cell carcinoma models.
Anti-angiogenic activity of
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment in the RMG-I xenograft model
To estimate the angiogenesis inhibitory activity,
the MVD in RMG-I tumor tissues was evaluated from specimens
obtained on week 6. The MVD on week 6 was significantly lower in
the bevacizumab maintenance treatment following bevacizumab
induction treatment group and in the control maintenance treatment
following paclitaxel induction treatment group, compared with the
control maintenance following control induction treatment group
(Fig. 2). Additionally, the MVD on
week 6 was significantly lower in the bevacizumab maintenance
following paclitaxel plus bevacizumab induction group, compared
with the three aforementioned treatment groups.
Comparison of antitumor activity of
bevacizumab maintenance treatment vs. control maintenance treatment
following paclitaxel plus bevacizumab induction treatment in the
RMG-I xengoraft model
Subsequently, the effect of bevacizumab treatment in
the maintenance phase in the RMG-I xenograft with a longer
treatment duration than in Fig. 1B
was evaluated. The tumor volume in the bevacizumab maintenance
treatment group following paclitaxel plus bevacizumab induction
treatment was significantly reduced on week 9, compared with the
tumor volume in the control maintenance groups following the same
induction treatment of paclitaxel induction treatment. In the
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment group, the tumor volume was
significantly reduced on week 4 (start date of maintenance
treatment), compared with week 1 (start date of induction
treatment), and the tumor volume was significantly reduced on week
9, compared with week 4, indicating that the tumors in this group
continued to significantly regress not only during induction
treatment, but also during bevacizumab maintenance treatment
(Fig. 3A).
Comparison of antitumor activity of
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment vs. bevacizumab maintenance
treatment following paclitaxel induction treatment in the RMG-I
xenograft model
Subsequently, the effect of bevacizumab treatment in
the induction phase in the RMG-I xenograft with bevacizumab
maintenance treatment was evaluated. Tumor volume in the
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment group was significantly reduced,
compared with the bevacizumab maintenance following paclitaxel
induction treatment group on week 9, indicating the potency of
bevacizumab induction treatment (Fig.
3B).
Comparison of anti-angiogenic activity
of bevacizumab maintenance treatment vs. control maintenance
treatment following paclitaxel plus bevacizumab induction treatment
in the RMG-I xenograft model
The MVD in RMG-I tumor tissues on week 9 in the
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment group was significantly lower,
compared with the control maintenance following paclitaxel plus
bevacizumab induction treatment group (Fig. 3C and D).
Antitumor activity of second-line
PEGylated liposomal doxorubicin plus bevacizumab treatment
following paclitaxel plus bevacizumab induction treatment and
bevacizumab maintenance treatment in the RMG-I xenograft model
Although the tumors regressed during the 4 weeks of
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment, when the maintenance treatment was
continued further, tumor regrowth was observed in 61/110
individuals at week 12 (data not shown). To investigate the
efficacy of second-line treatment and the usefulness of continuous
bevacizumab treatment following progression, at week 12, mice whose
tumors had regrown were selected and re-randomized into four groups
for the second-line treatments. In the preliminary experiments, the
sensitivity of treatment-naive RMG-I tumors to PEGylated liposomal
doxorubicin and gemcitabine was tested among the second-line
chemotherapeutics used in the treatment of patients with ovarian
cancer, and it was determined that RMG-I was sensitive only to
PEGylated liposomal doxorubicin (data not shown); therefore, this
drug was selected for further experiments. PEGylated liposomal
doxorubicin monotherapy was also efficacious in tumors that regrew
during bevacizumab maintenance, and no significant tumor growth was
observed from the initiation of treatment (weeks 22 vs. 13 in the
second-line PEGylated liposomal doxorubicin treatment group;
Fig. 4). Notably, the tumors in the
second-line PEGylated liposomal doxorubicin plus bevacizumab
treatment group regressed significantly from their volume at the
initiation of this treatment (week 22 vs. 13). The tumor volume in
the second-line PEGylated liposomal doxorubicin plus bevacizumab
treatment group at week 22 was significantly reduced, compared with
the tumor volume in the second-line PEGylated liposomal doxorubicin
treatment group.
 | Figure 4.Antitumor activity of 2L PLD plus BEV
treatment following PTX plus BEV induction treatment and BEV
maintenance treatment in the RMG-I xenograft model. Mice bearing
RMG-I tumors were randomly divided into a control induction group
(n=6) and a PTX+BEV induction and BEV maintenance group (n=110) and
treated with control (vehicle for PTX plus HuIgG) or PTX+BEV on
weeks 1, 2, and 3 as first-line induction treatment, and
subsequently treated weekly with BEV as maintenance treatment. The
control induction group was examined until week 4, as scheduled. On
week 12, mice treated with BEV maintenance and whose tumors had
regrown were selected and re-randomized into four groups
(n=7/group): 2L control group; BEV group; PLD group; and PLD+BEV
group. At re-randomization, 82 mice were excluded, including
individuals whose tumor did not regrow or those that were excluded
to reduce the variability in tumor volume, body weight and growth
rate. Plots of the PTX+BEV induction and BEV maintenance group were
based on 28 individuals selected on week 12. Mice were subsequently
treated with PLD once every 3 weeks and/or BEV weekly as the 2L
treatment. The dosage of PLD, BEV and PTX was 20, 5 and 80 mg/kg,
respectively. The following individuals receiving 2L treatment were
excluded from data analysis: 1 mouse with tumor self-destruction in
the 2L BEV group on week 13; 1 mouse with tumor blister breakage in
the 2L BEV group on week 14; 1 mouse that was accidentally
administered in the 2L PLD group on week 19; 1 mouse with tumor
self-destruction in the 2L PLD group on week 19; and 1 mouse that
was accidentally administered in the 2L PLD+BEV group on week 13.
Data points represent the mean + standard deviation of tumor volume
(mm3). *P<0.05, Wilcoxon test. PLD, PEGylated
liposomal doxorubicin; BEV, bevacizumab; PTX, paclitaxel; 2L,
second line. |
Anti-angiogenic activity of
second-line PEGylated liposomal doxorubicin plus bevacizumab
treatment following paclitaxel plus bevacizumab induction treatment
and bevacizumab maintenance treatment in the RMG-I xenograft
model
The investigation of MVD comparing second-line
control treatment and second-line bevacizumab treatment was
terminated at week 16 due to the tumor blister breaking in 3/7 mice
in the control group (the number pre-specified in the study
protocol). MVD in the second-line bevacizumab treatment group was
significantly lower, compared with the second-line control
treatment group, on week 16, 4 days after the tumor blister
breakage was observed (Fig. 5).
Furthermore, MVD in the second-line PEGylated liposomal doxorubicin
plus bevacizumab treatment group on week 22 was significantly
lower, compared with in the second-line bevacizumab treatment group
on week 16 and in the second-line PEGylated liposomal doxorubicin
treatment group on week 22, indicating that the MVD suppression
effect of the second-line bevacizumab was enhanced by the
combination with the second-line PEGylated liposomal
doxorubicin.
IGFBP-3 expression level in the RMG-I
xenograft model
To investigate the mechanism of the further MVD
reduction observed in the combination treatment, expression levels
of human angiogenesis factors in RMG-I tumor tissue were evaluated
by a human angiogenesis array on samples obtained on weeks 16 and
22. Among the 55 angiogenesis-associated proteins on the array,
only IGFBP-3 expression was affected, which was lower in the
second-line PEGylated liposomal doxorubicin plus bevacizumab
treatment group, compared with the second-line control, bevacizumab
or PEGylated liposomal doxorubicin treatment groups (Fig. 6A). This tendency was confirmed with a
quantitative ELISA assay of IGFBP-3 to be statistically significant
(Fig. 6B). No reduced level in
IGFBP-3 expression was observed in the second-line bevacizumab
treatment or the second-line PEGylated liposomal doxorubicin
treatment groups, compared with the IGFBP-3 expression in the
second-line control group.
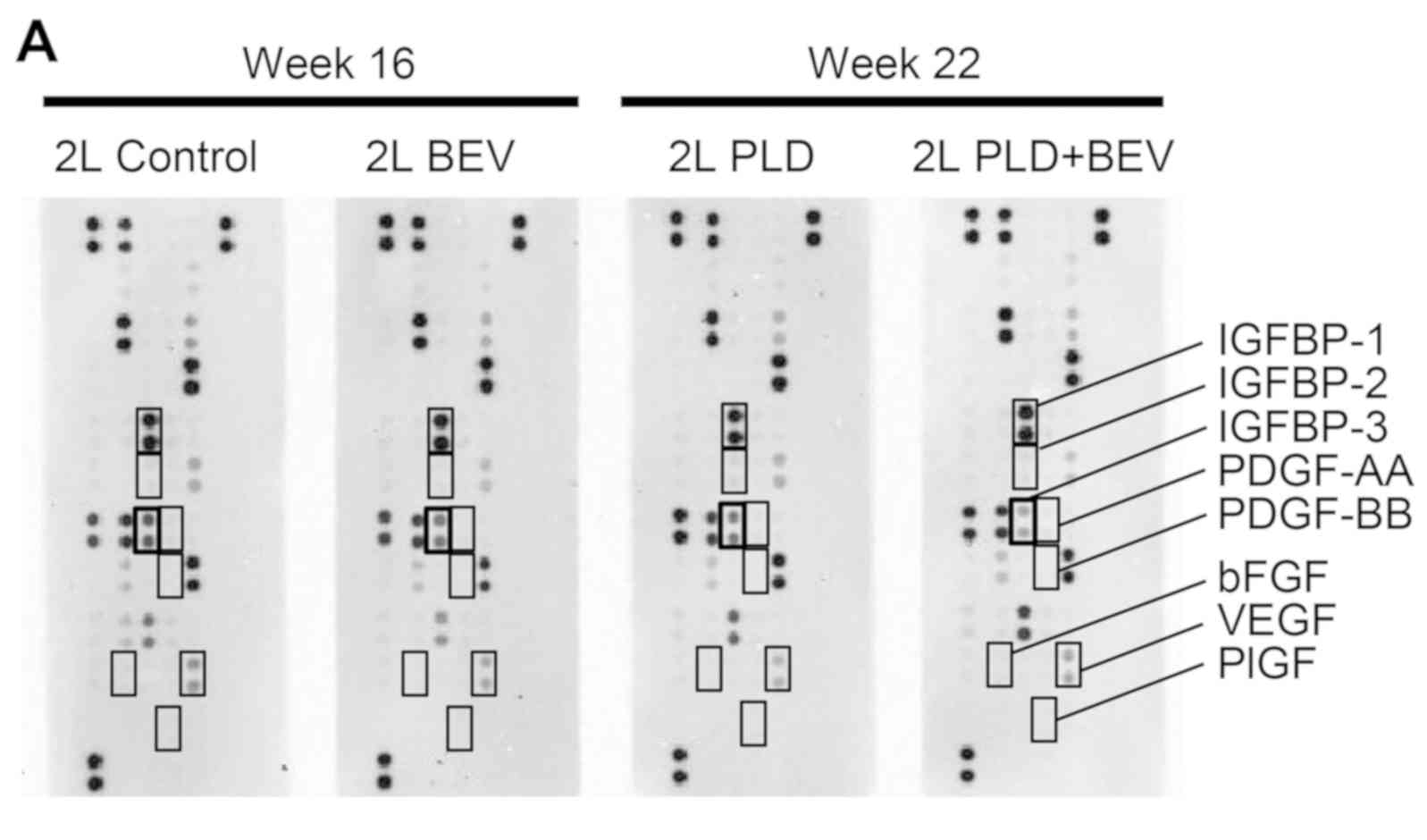 | Figure 6.IGFBP-3 expression level in RMG-I
xenografts treated with 2L PLD plus BEV following PTX plus BEV
induction treatment and BEV maintenance treatment. (A) Expression
levels of human angiogenesis factors in RMG-I tumor tissues were
evaluated by human angiogenesis array on weeks 16 and 22. (B)
IGFBP-3 expression level was determined by human ELISA assay on
weeks 16 and 22. The dosage of PLD, BEV and PTX was 20, 5 and 80
mg/kg, respectively. Data represent the mean + standard deviation
(n=5–7). *P<0.05, Wilcoxon test with Holm-Bonferroni correction.
2L, second line; PLD, PEGylated liposomal doxorubicin; BEV,
bevacizumab; PTX, paclitaxel. IGFBP-3, insulin like growth factor
binding protein-3; PDGF, platelet derived growth factor; bFGF,
basic fibroblast growth factor; VEGF, vascular endothelial cell
growth factor; PlGF, placental growth factor. |
Discussion
The present study was conducted to address the
following two clinical questions regarding continuous treatment
with bevacizumab in ovarian cancer. The first question arises from
the study reported by Burger et al (GOG-0218) (9) concerning the efficacy of bevacizumab
maintenance following induction therapy with carboplatin and
paclitaxel plus bevacizumab in ovarian clear cell carcinoma. The
second question concerns the efficacy and mechanisms of bevacizumab
beyond progression, which is continuous treatment with bevacizumab
in combination with a second-line chemotherapeutic agent for
patients who have disease progression after first-line chemotherapy
plus bevacizumab combination therapy followed by maintenance with
bevacizumab (11). Therefore,
experiments were conducted using mouse xenograft models inoculated
with the human ovarian clear cell carcinoma cell line RMG-I and the
ovarian serous adenocarcinoma cell line SK-OV-3.
With respect to the first question, it was
demonstrated that the regimens with bevacizumab maintenance
treatment following induction treatments, including bevacizumab,
exhibited an increased antitumor effect, compared with the regimens
without bevacizumab, during the induction and maintenance phases in
the SK-OV-3 and RMG-I xenograft models (Fig. 1). These results demonstrated that the
regimens with bevacizumab treatment throughout the induction and
maintenance phases result in an increased antitumor effect,
compared with regimens without bevacizumab, not only in ovarian
serous carcinoma model, but also in the ovarian clear cell
carcinoma model.
Notably, compared with the control maintenance
treatment following control induction treatment group on week 6,
the MVD was significantly lower, not only with the bevacizumab
maintenance treatment following bevacizumab induction treatment
group, but also with the control maintenance treatment following
paclitaxel induction treatment group (Fig. 2). Additionally, the MVD with
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment group was even more significantly
lower. Paclitaxel has been reported to exhibit anti-angiogenic
activity through inhibition of proliferation, chemotaxis,
chemo-invasion, alignment and cord formation of vascular
endothelial cells (20,21). Although the precise mechanisms of
paclitaxel-induced anti-angiogenic activity have not yet been
elucidated, the combination effect of paclitaxel and bevacizumab
demonstrated in the present study indicates that these two agents
act to reduce MVD via different underlying mechanisms, and this
stronger MVD reduction is considered to contribute, at least in
part, to superior antitumor activity of this treatment regimen.
Subsequently, the efficacy of continuous treatment
with bevacizumab in the induction and maintenance phases in the
clear cell carcinoma model was investigated. As expected, an
increased antitumor activity was observed in the bevacizumab
maintenance following paclitaxel plus bevacizumab treatment group,
compared with the groups without bevacizumab maintenance (Fig. 3A). In additional experiments,
increased antitumor activity was observed with bevacizumab
maintenance treatment following paclitaxel plus bevacizumab
induction treatment, compared with bevacizumab maintenance
treatment following paclitaxel induction treatment (Fig. 3B). These data indicated that
bevacizumab treatment was notable not only during the induction
phase in combination with paclitaxel, but also during the
maintenance phase in the ovarian clear cell carcinoma model. The
MVD following bevacizumab maintenance treatment following
paclitaxel plus bevacizumab induction treatment was significantly
lower at week 9, compared with the MVD following paclitaxel plus
bevacizumab induction treatment without maintenance treatment
(Fig. 3C and D). Collectively, this
data indicated that continuous presence of bevacizumab is required
to maintain the tumor microvessel density at a low level, and the
addition of paclitaxel during induction further augments the
reduction of these vessels.
With respect to the second question, since the
efficacy and mechanism of bevacizumab beyond progression has not
been demonstrated in ovarian cancer, to investigate its potency in
a non-clinical model, mice whose tumors exhibited regrowth during
bevacizumab maintenance were selected and PEGylated liposomal
doxorubicin was used as a second-line partner of bevacizumab in the
RMG-I xenograft model. Second-line PEGylated liposomal doxorubicin
plus bevacizumab exhibited a significantly increased antitumor
activity, compared with second-line PEGylated liposomal doxorubicin
alone, even when bevacizumab monotherapy itself had no apparent
effect on tumor growth (Fig. 4).
This result raises two possibilities. Firstly,
continuous inhibition of VEGF-A by bevacizumab was still required
to reduce angiogenesis, but reduction of angiogenesis alone was
insufficient to control tumor growth at this stage, unlike in the
treatment naive stage in this model, but it was efficacious when
combined with PEGylated liposomal doxorubicin. The other
possibility is that RMG-I had acquired resistance to bevacizumab by
VEGF-A-independent angiogenesis, which was blocked by PEGylated
liposomal doxorubicin to produce the combination effect. We
previously reported that the latter mechanism was observed with
capecitabine in a human colon cancer cell xenograft model after
acquired resistance to bevacizumab (22).
To investigate the mechanism of action of
second-line bevacizumab with PEGylated liposomal doxorubicin, MVD
in RMG-I tumors was analyzed. Compared with control in the
second-line treatment, bevacizumab kept MVD significantly lower,
which indicated that tumor angiogenesis remained dependent on
VEGF-A and that resistance to bevacizumab had not been acquired, at
least in terms of angiogenesis in this model. Notably, the
bevacizumab-induced decrease in MVD was significantly enhanced by
PEGylated liposomal doxorubicin (Fig.
5), indicating that this drug may also have additional
VEGF-A-independent suppressive effects on angiogenesis.
Among the angiogenesis-associated proteins that were
tested, IGFBP-3 was the only one where the expression was
determined to be lower when bevacizumab was combined with PEGylated
liposomal doxorubicin. Additionally, no changes in the expression
levels of IGFBP-1 or IGFBP-2, which belong to the same protein
family as IGFBP-3, or other angiogenic factors, including basic
fibroblast growth factor, placental growth factor, platelet derived
growth factor (PDGF)-AA and PDGF-BB, were observed (Fig. 6A). Granata et al (23) demonstrated that IGFBP-3 induces
angiogenesis in an in vitro assay of capillary-like structure
formation and in a quantitative in vivo analysis of
neovascularization in Matrigel plugs. Although PEGylated liposomal
doxorubicin alone and bevacizumab alone did not affect human
IGFBP-3 expression, PEGylated liposomal doxorubicin plus
bevacizumab treatment resulted in levels of human IGFBP-3 being
significantly lower, compared with levels following PEGylated
liposomal doxorubicin alone or bevacizumab alone treatment
(Fig. 6B).
It was reported that IGFBP-3 secretion is stimulated
by VEGF, and IGFBP-3 and VEGF secretions are induced by hypoxia
inducible factor (HIF)-1α (24,25).
Accordingly, in the present model, although IGFBP-3 production by
VEGF is considered to be inhibited by treatment with bevacizumab
alone, IGFBP-3 production via HIF-1α derived from hypoxia may be
enhanced and act to cancel out any change of IGFPB-3. However,
doxorubicin is reported to inhibit the activation of HIF-1α
(26); therefore, when PEGylated
liposomal doxorubicin and bevacizumab are combined, simultaneous
inhibition of VEGF and HIF-1α may result in a decrease in the
production of IGFBP-3. In addition to the blockade of VEGF by
bevacizumab, the decrease in IGFBP-3 by PEGylated liposomal
doxorubicin plus bevacizumab may contribute to the continuous and
enhanced suppression of MVD and may be the mechanism through which
bevacizumab beyond progression acts in the present model.
It is not probable that the disease progression
observed in the present study is resistance to bevacizumab due to
increased IGFBP-3 expression, since there was no difference in
level of IGFBP-3 expression between the second-line control group
and the second-line bevacizumab group. The precise mechanism by
which the PEGylated liposomal doxorubicin plus bevacizumab
combination reduces the IGFBP-3 level and its general contribution
to tumor angiogenesis remains to be elucidated. Although one of the
proposed modes of action of bevacizumab is to increase the
intra-tumor concentration of co-administered chemotherapeutics
(27), the present study confirmed
that this was not the case since there was no difference in
apoptosis, number of cells in the M phase or Ki-67 levels, due to
bevacizumab induction, maintenance or second-line treatment (data
not shown).
In conclusion, the present study demonstrated that
bevacizumab maintenance treatment following paclitaxel plus
bevacizumab induction treatment produced antitumor activity
superior to that with no bevacizumab treatment as induction or
maintenance in ovarian clear cell carcinoma. Additionally, it
indicated that second-line PEGylated liposomal doxorubicin plus
bevacizumab treatment following paclitaxel plus bevacizumab
induction and bevacizumab maintenance treatment had antitumor
activity superior to that with second-line PEGylated liposomal
doxorubicin alone following the same induction and maintenance
treatments. Bevacizumab treatment throughout induction, maintenance
and the second-line combination phase resulted in a continuous
reduction of MVD, which indicates that it is the primary mechanism
underlying the superior efficacy in the first-line induction,
maintenance and second-line treatments that include bevacizumab.
Further studies are required to elucidate the efficacy and the
mechanism of action of the continuation of bevacizumab as a
maintenance therapy following induction treatment including
bevacizumab, and as a bevacizumab beyond progression, in ovarian
cancer.
Acknowledgements
The authors would like to thank Dr Kaori
Fujimoto-Ouchi for her advice on experimental design, and Ms.
Masako Miyazaki and Ms. Hiromi Sawamura for their excellent
technical assistance (Product Research Department, Chugai
Pharmaceutical Co., Ltd. Kamakura, Japan).
Funding
No funding was received.
Availability of data and materials
The datasets analyzed during the study are available
from the corresponding author on reasonable request.
Authors contributions
NI designed and performed the experiments, analyzed
the data, and drafted the manuscript. KYo and MK produced the
slides, performed the pathological diagnosis, and analyzed the
data. MY collected the data. MS performed data interpretation and
revised the manuscript. KYa provided the study concept and design.
All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
All animal experiments were reviewed and approved by
the Institutional Animal Care and Use Committee at Chugai
Pharmaceutical Co., Ltd. (approval no. 13-225, 15-201).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chan JK, Teoh D, Hu JM, Shin JY, Osann K
and Kapp DS: Do clear cell ovarian carcinomas have poorer prognosis
compared to other epithelial cell types? A study of 1411 clear cell
ovarian cancers. Gynecol Oncol. 109:370–376. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sugiyama T, Kamura T, Kigawa J, Terakawa
N, Kikuchi Y, Kita T, Suzuki M, Sato I and Taguchi K: Clinical
characteristics of clear cell carcinoma of the ovary: A distinct
histologic type with poor prognosis and resistance to
platinum-based chemotherapy. Cancer. 88:2584–2589. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Itamochi H, Kigawa J and Terakawa N:
Mechanisms of chemoresistance and poor prognosis in ovarian clear
cell carcinoma. Cancer Sci. 99:653–658. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mackay HJ, Brady MF, Oza AM, Reuss A,
Pujade-Lauraine E, Swart AM, Siddiqui N, Colombo N, Bookman MA,
Pfisterer J and Du Bois A; Gynecologic Cancer InterGroup, :
Prognostic relevance of uncommon ovarian histology in women with
stage III/IV epithelial ovarian cancer. Int J Gynecol Cancer.
20:945–952. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Piccart MJ, Bertelsen K, James K, Cassidy
J, Mangioni C, Simonsen E, Stuart G, Kaye S, Vergote I, Blom R, et
al: Randomized intergroup trial of cisplatin-paclitaxel versus
cisplatin-cyclophosphamide in women with advanced epithelial
ovarian cancer: Three-year results. J Natl Cancer Inst. 92:699–708.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vasey PA, Jayson GC, Gordon A, Gabra H,
Coleman R, Atkinson R, Parkin D, Paul J, Hay A and Kaye SB;
Scottish Gynaecological Cancer Trials Group, : Phase III randomized
trial of docetaxel-carboplatin versus paclitaxel-carboplatin as
first-line chemotherapy for ovarian carcinoma. J Natl Cancer Inst.
96:1682–1691. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Köbel M, Kalloger SE, Huntsman DG, Santos
JL, Swenerton KD, Seidman JD and Gilks CB; Cheryl Brown Ovarian
Cancer Outcomes Unit of the British Columbia Cancer Agency,
Vancouver BC, : Differences in tumor type in low-stage versus
high-stage ovarian carcinomas. Int J Gynecol Pathol. 29:203–211.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Burger RA, Brady MF, Bookman MA, Fleming
GF, Monk BJ, Huang H, Mannel RS, Homesley HD, Fowler J, Greer BE,
et al Gynecologic Oncology Group, : Incorporation of bevacizumab in
the primary treatment of ovarian cancer. N Engl J Med.
365:2473–2483. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Morgan RJ Jr, Armstrong DK, Alvarez RD,
Bakkum-Gamez JN, Behbakht K, Chen LM, Copeland L, Crispens MA, De
Rosa M, Dorigo O, et al: Ovarian Cancer, Version 1.2016, NCCN
Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw.
14:1134–1163. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Masi G, Salvatore L, Boni L, Loupakis F,
Cremolini C, Fornaro L, Schirripa M, Cupini S, Barbara C, Safina V,
et al BEBYP Study Investigators, : Continuation or reintroduction
of bevacizumab beyond progression to first-line therapy in
metastatic colorectal cancer: Final results of the randomized BEBYP
trial. Ann Oncol. 26:724–730. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Presta LG, Chen H, O'Connor SJ, Chisholm
V, Meng YG, Krummen L, Winkler M and Ferrara N: Humanization of an
anti-vascular endothelial growth factor monoclonal antibody for the
therapy of solid tumors and other disorders. Cancer Res.
57:4593–4599. 1997.PubMed/NCBI
|
|
13
|
Braghiroli MI, Sabbaga J and Hoff PM:
Bevacizumab: Overview of the literature. Expert Rev Anticancer
Ther. 12:567–580. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Crossin KL and Carney DH: Evidence that
microtubule depolymerization early in the cell cycle is sufficient
to initiate DNA synthesis. Cell. 23:61–71. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gabizon AA: Pegylated liposomal
doxorubicin: Metamorphosis of an old drug into a new form of
chemotherapy. Cancer Invest. 19:424–436. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pérez-López ME, Curiel T, Gómez JG and
Jorge M: Role of pegylated liposomal doxorubicin (Caelyx) in the
treatment of relapsing ovarian cancer. Anticancer Drugs.
18:611–617. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fogh J, Wright WC and Loveless JD: Absence
of HeLa cell contamination in 169 cell lines derived from human
tumors. J Natl Cancer Inst. 58:209–214. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nozawa S, Tsukazaki K, Sakayori M, Jeng CH
and Iizuka R: Establishment of a human ovarian clear cell carcinoma
cell line (RMG-I) and its single cell cloning - with special
reference to the stem cell of the tumor. Hum Cell. 1:426–435.
1988.PubMed/NCBI
|
|
19
|
Holm S: A simple sequentially rejective
multiple test procedure. Scand J Stat. 6:65–70. 1979.
|
|
20
|
Belotti D, Vergani V, Drudis T, Borsotti
P, Pitelli MR, Viale G, Giavazzi R and Taraboletti G: The
microtubule-affecting drug paclitaxel has antiangiogenic activity.
Clin Cancer Res. 2:1843–1849. 1996.PubMed/NCBI
|
|
21
|
Naumova E, Ubezio P, Garofalo A, Borsotti
P, Cassis L, Riccardi E, Scanziani E, Eccles SA, Bani MR and
Giavazzi R: The vascular targeting property of paclitaxel is
enhanced by SU6668, a receptor tyrosine kinase inhibitor, causing
apoptosis of endothelial cells and inhibition of angiogenesis. Clin
Cancer Res. 12:1839–1849. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Iwai T, Sugimoto M, Harada S, Yorozu K,
Kurasawa M and Yamamoto K: Continuous administration of bevacizumab
plus capecitabine, even after acquired resistance to bevacizumab,
restored anti-angiogenic and antitumor effect in a human colorectal
cancer xenograft model. Oncol Rep. 36:626–632. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Granata R, Trovato L, Lupia E, Sala G,
Settanni F, Camussi G, Ghidoni R and Ghigo E: Insulin-like growth
factor binding protein-3 induces angiogenesis through IGF-I- and
SphK1-dependent mechanisms. J Thromb Haemost. 5:835–845. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Slomiany MG and Rosenzweig SA: Autocrine
effects of IGF-I-induced VEGF and IGFBP-3 secretion in retinal
pigment epithelial cell line ARPE-19. Am J Physiol Cell Physiol.
287:C746–C753. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Slomiany MG and Rosenzweig SA:
IGF-1-induced VEGF and IGFBP-3 secretion correlates with increased
HIF-1 alpha expression and activity in retinal pigment epithelial
cell line D407. Invest Ophthalmol Vis Sci. 45:2838–2847. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Duyndam MC, van Berkel MP, Dorsman JC,
Rockx DA, Pinedo HM and Boven E: Cisplatin and doxorubicin repress
vascular endothelial growth factor expression and differentially
down-regulate hypoxia-inducible factor I activity in human ovarian
cancer cells. Biochem Pharmacol. 74:191–201. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yanagisawa M, Yorozu K, Kurasawa M, Nakano
K, Furugaki K, Yamashita Y, Mori K and Fujimoto-Ouchi K:
Bevacizumab improves the delivery and efficacy of paclitaxel.
Anticancer Drugs. 21:687–694. 2010.PubMed/NCBI
|
















