Introduction
Recently, research on the biology of breast cancer
has made surprising progress. An attempt to understand the unique
biological characteristics of individual tumors to facilitate
treatment has been realized. At present, treatment strategy is, not
only based on the stage classification, but also on tumor biology.
The St. Gallen International Expert Consensus on the primary
therapy of early breast cancer outlines the guidelines for
endocrine and chemotherapy treatment (1). The treatment allocation mainly
consists of targeted treatments, such as endocrine therapy for
estrogen receptor (ER)-positive tumors and anti-HER2 therapy for
HER2-positive tumors. Chemotherapy is recommended for triple
negative (TN) tumors that have no targets. At present, the vital
problem is how to incorporate chemotherapy into the treatment of
hormone-sensitive patients with ER-positive and HER2-negative
tumors, as they make up the majority of the patients with primary
breast cancer. One solution is to consider the Ki-67 index when
deciding the method of treatment.
Ki-67 is present in all proliferating cells, and
there is great interest in its role as a proliferation marker
(2). The Ki-67 antibody reacts
with 395 kDa, which is a nuclear non-histone protein that is
present in all active phases of the cell cycle, except the G0 phase
(3). Moreover, Ki-67 is one of the
21 prospectively selected genes included in the Oncotype DX™ assay
used to predict the risk of recurrence and the extent of
chemotherapy benefits in women with node-negative, ER-positive
breast cancer (4,5). The proliferation biomarker Ki-67 is
considered to be a prognostic factor for breast cancer and has been
investigated in several studies (6–8).
In this study, we compared the Ki-67 index with
clinicopathological factors in 3,652 cases with early breast cancer
as well as with prognosis [disease-free survival (DFS) and overall
survival (OS)] according to the breast cancer subtypes, luminal,
HER2 and TN, at a single institute.
Patients and methods
Patients
The Ki-67 index was measured in 3,652 cases with
primary breast cancer from 1987 to 2009 in Kumamoto City Hospital,
Japan. Out of these patients, 2,638 cases were evaluated
simultaneously for ER, progesterone receptor (PgR) and HER2 from
1997, and these were analyzed as prognostic factors according to
their subtypes. The present study was approved by the ethics
committee of Kumamoto City Hospital, and informed consent was
obtained from all of the the patients. Table I shows the patient characteristics.
The age of the patients ranged from 25 to 95 years (mean 52.2), and
the mean tumor diameter was 2.2 cm (range 0.1–22). Two-thirds
(65.9%) of the patients had pathologically negative nodes. In terms
of the biological markers, the ER- and PgR-positive rates were 74.6
and 61.7%, respectively. HER2 cases of 3+ had a rate of 14.6% and
the p53 overexpression rate was 21.3%.
 | Table I.Characteristics of the 2,639 primary
breast cancer patients studied between 1997 and 2009. |
Table I.
Characteristics of the 2,639 primary
breast cancer patients studied between 1997 and 2009.
| Age (years) | |
| Mean (range) | 56.2 (25–95) |
| Tumor size (cm) | |
| Mean (range) | 2.2 (0.1–22.0) |
| Nodal status (pN)
(%) | |
| Positive | 840 (31.8) |
| Negative | 1,740 (65.9) |
| Unknown | 59 |
| Estrogen receptor
(%) | |
| Positive | 1,970 (74.6) |
| Negative | 669 (25.4) |
| Progesterone receptor
(%) | |
| Positive | 1,628 (61.7) |
| Negative | 1,011 (38.3) |
| HER2 (%) | |
| Negative | 974 (36.9) |
| 1+ | 1,085 (41.1) |
| 2+ | 193 (7.3) |
| 3+ | 387 (14.6) |
| p53 (%) | |
| Negative | 1,391 (52.7) |
| 1+ | 684 (25.9) |
| 2+ | 561 (21.3) |
| Unknown | 3 |
| Surgical operation
(%) | |
| Total
mastectomy | 1,007 (38.2) |
| Partial
mastectomy | 1,597 (60.5) |
| None performed | 35 (1.3) |
Histopathological examination
The factors investigated included the presence or
absence of lymph node metastasis, nuclear grade, ER/PgR status,
proliferation (Ki-67), HER2 and p53 overexpression. Immunostaining
for ER, PgR, p53, Ki-67 and HER2 was carried out as previously
described (9). The positive cell
rates for ER/PgR were determined by immunohistochemistry (IHC), and
a value of ≥10% was rated as positive. The proliferative activity
was determined by immunostaining for the Ki-67 antibody (Dako,
Glostrup, Denmark). The fraction of proliferating cells was based
on a count of at least 500 tumor cells. The Ki-67 values were
expressed as the percentage of positive cells in each case. p53 and
HER2 expression was evaluated by immunostaining (LSAB method) with
the mouse monoclonal anti-p53 antibody (clone DO7; Dako) and the
Hercep Test (Dako). The staining pattern of the p53 protein was
divided into three groups: 2+ (homogenous and diffuse staining), 1+
(heterogeneous or focal staining >5% of cancer cells) and
negative (focal staining <5% of cancer cells). The staining
pattern of HER2 was divided into four groups: 3+ (strong and
diffuse staining), 2+ (moderate and diffuse staining), 1+ (focal
staining >10% cancer cells) and negative.
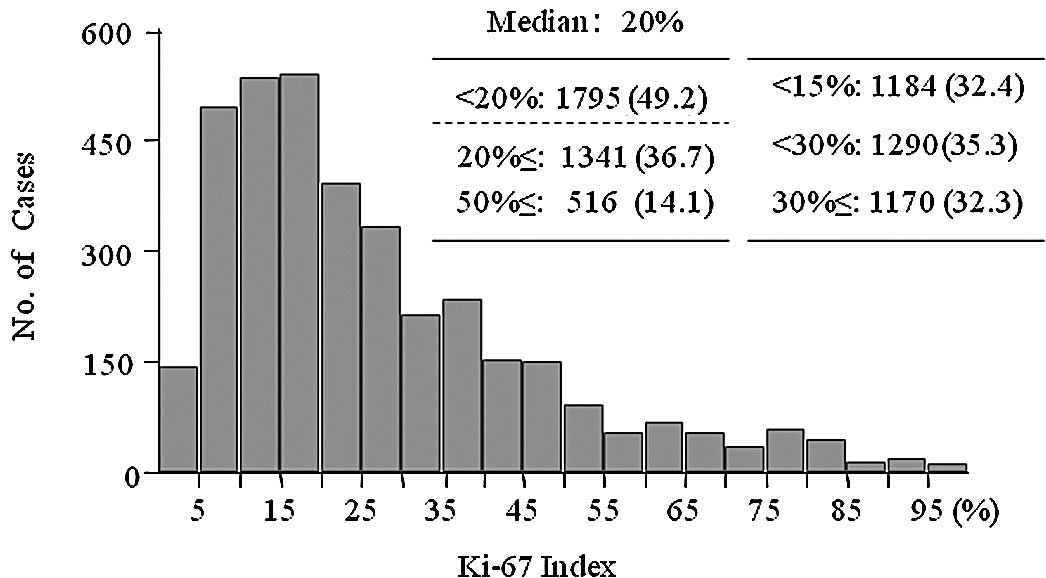
Fig. 1 shows the
distribution of the Ki-67 index for all of the patients. Many
patients had a value of 10–19% on the Ki-67 index in all of the
groups, and the median value was 20%. Therefore, the Ki-67 values
were divided into 2 or 3 groups; <20% and ≥20% (and ≥50%).
One-third of each of the groups was divided according to the St.
Gallen Consensus meeting, which recommended a cut-off value of 15
or 30%. The findings of our study revealed the cut-off point as
being 20%. Regarding the histological types and Ki-67 index, tumors
with DCIS, lobular carcinoma and mucinous carcinoma had lower
values on the Ki-67 index; the median values were 13, 14 and 17%,
respectively. Most of the cases were invasive ductal carcinomas
with a median Ki-67 index of 22% (Table II).
| Table II.Distribution of Ki-67 indices
according to histological tumor type. |
Table II.
Distribution of Ki-67 indices
according to histological tumor type.
| Histological
type | Ki-67 index
| Total |
|---|
| Median (%) | <20% | ≥20 and <50% | ≥50% |
|---|
| Non-invasive
carcinoma (DCIS) | 13 | 186 (74.1%) | 59 | 6 | 251 |
| Invasive ductal
carcinoma | 22 | 1,412 (46.5%) | 1,162 | 463 | 3,037 |
| Invasive lobular
carcinoma | 14 | 82 (71.9%) | 26 | 6 | 114 |
| Mucinous
carcinoma | 17 | 76 (61.3%) | 44 | 4 | 124 |
| Others | 28 | 39 (31.0%) | 50 | 37 | 126 |
| Total (%) | 20 | 1,795 (49.2%) | 1,341 (36.7%) | 516 (14.1%) | 3,652 |
Breast cancer subtype and adjuvant
therapy
Breast cancer is classified by gene expression
profile into subtypes consisting of two hormone receptor
(HR)-positive types (luminal A and B) and three HR-negative types
(HER2-expressing, basal-like and unclassified ‘normal-like’). IHC
surrogate panels have also been proposed to potentially identify
the molecular-based groups. In this study, HR-positive and
HER2-negative tumors were classified as luminal A type; HR-positive
and HER2-positive tumors (HER2 IHC: 3+ or 2+ and FISH amplification
ratio >2.0) as luminal B type; HR-negative and HER2-positive
tumors as HER2 disease; and HR-negative and HER2-negative tumors as
TN type.
As shown in Table
III, the distribution of cases was as follows: luminal A, 1,749
cases (66.3%); luminal B, 263 cases (10%); HER2 disease, 271 cases
(10.2%) and TN, 356 cases (13.5%). Regarding adjuvant therapy, most
of the cases with luminal type tumors received endocrine therapy.
On the other hand, most of the cases with TN and HER2 disease type
were treated with chemotherapy. One-fourth of the patients with
luminal A tumors received chemotherapy and ∼60% of those with
luminal B tumors were treated with chemotherapy. Anti-HER2 therapy
with trastuzumab has been used in Japan since receiving approval in
2008.
| Table III.Adjuvant therapy according to breast
cancer subtypes. |
Table III.
Adjuvant therapy according to breast
cancer subtypes.
| Breast cancer subtype
|
|---|
| Luminal A | Luminal B | HER2 | Triple negative |
|---|
| Endocrine therapy
(%) | | | | |
| TAM, AI | 1,538 (89.7) | 221 (83.7) | 6 (2.4) | 19 (5.6) |
| Chemotherapy (%) | | | | |
| CMF, CE(F),
Taxane | 443 (25.8) | 154 (58.3) | 197 (87.9) | 250 (73.1) |
| Trastuzumab (since
2008) | 0 | 38 (14.4) | 44 (16.2) | 0 |
| Unknown | 35 | 0 | 16 | 14 |
| Total | 1,749 | 263 | 271 | 356 |
Statistical analysis
For statistical processing, the Chi-square test and
Fisher's exact test were used for inter-group comparison (Tables IV, V and VI). Wilcoxon's (non-parametric) test was
used to compare the mean values for tumor size and age. The
Kaplan-Meier test was was used to calculate prognosis (cumulative
DFS and OS) and tested with the log-rank procedure. Cox's
proportional hazard model was used to perform univariate and
multivariate analyses of the factors related to DFS. In recurrent
cases, the relationship between disease-free interval times and
Ki-67 index was analyzed statistically using the Pearson
correlation coefficient. The median observation period was 68.5
months.
| Table IV.Ki-67 index according to breast
cancer subtypes. |
Table IV.
Ki-67 index according to breast
cancer subtypes.
| Subtype | Ki-67 index
| Total |
|---|
| Median (%) | <20% | ≥20 and
<50% | ≥50% |
|---|
| Luminal A (%) | 17 | 1,037 (59.3%) | 623 | 89 (5.10%) | 1,749 (66.3%) |
| Luminal B (%) | 29 | 72 (27.4%) | 158 | 33 (12.5%) | 263 (10.0%) |
| HER2 (%) | 40 | 22 (8.10%) | 177 | 71 (26.2%) | 271 (10.2%) |
| Triple negative
(%) | 50 | 59 (16.6%) | 114 | 183 (51.4%) | 356 (13.5%) |
| Total (%) | 22 | 1,190 (45.1%) | 1,072 | 376 | 2,639 |
| Table V.Clinicopathological factors and the
Ki-67 index in the primary breast cancer cases. |
Table V.
Clinicopathological factors and the
Ki-67 index in the primary breast cancer cases.
| Ki-67 index | <20% | 20–50% | ≥50% | P-value |
|---|
| Mean tumor size, in
cm | 1.8±1.3 | 2.4±1.9 | 2.7±2.0 | <0.0001 |
| Mean age, in
years | 58.1±13.2 | 54.8±12.4 | 54.0±12.6 | <0.0001 |
| Age, in years
(%) | | | | |
| ≤35 | 34 (31.5) | 52 | 22 | |
| ≤50 | 383 (41.9) | 392 | 139 | <0.0001 |
| ≤65 | 422 (42.9) | 414 | 147 | |
| ≥66 | 365 (55.7) | 223 | 67 | |
| No. of positive
nodes (%) | | | | |
| 0 | 887 (50.5) | 653 | 217 | |
| 1–3 | 241 (38.0) | 285 | 109 | <0.0001 |
| ≥4 | 52 (25.1) | 113 | 42 | |
| Nuclear grade
(%) | | | | |
| 1 | 756 (70.6) | 284 | 31 | |
| 2 | 396 (35.9) | 560 | 148 | <0.0001 |
| 3 | 32 (7.10) | 223 | 195 | |
| Estrogen receptor
(%) | | | | |
| Positive | 1,093 (55.4) | 763 | 116 | |
| Negative | 98 (14.6) | 310 | 261 | <0.0001 |
| Progesterone
receptor (%) | | | | |
| Positive | 943 (57.9) | 613 | 72 | |
| Negative | 247 (24.5) | 458 | 305 | <0.0001 |
| p53 (%) | | | | |
| 0 | 837 (59.5) | 458 | 111 | |
| 1+ | 310 (44.9) | 328 | 53 | <0.0001 |
| 2+ | 56 (9.90) | 295 | 213 | |
| HER2 (%) | | | | |
| 0 | 534 (53.7) | 314 | 147 | |
| 1+ | 560 (51.5) | 408 | 119 | |
| 2+ | 68 (35.1) | 97 | 29 | <0.0001 |
| 3+ | 43 (11.1) | 263 | 82 | |
| Table VI.Disease-free interval time and Ki-67
indices in recurrent cases. |
Table VI.
Disease-free interval time and Ki-67
indices in recurrent cases.
| Ki-67 index | Disease-free
survival
| Total (n=307) |
|---|
| ≤2 years | ≤5 years | ≤10 years | >10 years |
|---|
| <20% | 22 (35.4) | 21 | 13 | 6 (9.7) | 62 |
| 20–50% | 58 (53.3) | 59 | 13 | 5 (3.0) | 165 |
| ≥50% | 60 (76.9) | 17 | 1 | 0 (0.0) | 78 |
Results
Ki-67 index and breast cancer
subtype(s)
As shown in Table
IV, the median Ki-67 index of tumors with luminal A was 17% and
that of tumors with luminal B was 29%; the median Ki-67 index for
tumors with HER2 was 40% and that for TN tumors was 50%. There was
a significant difference among these values. Approximately 60% of
the luminal A type tumors had lower proliferation (Ki-67 <20%),
while more than half of the TN type tumors had higher proliferation
(Ki-67 ≥50%).
Ki-67 index and clinicopathological
factors
Table V shows the
relationship between the Ki-67 index and the clinicopathological
factors in primary breast cancer. A higher Ki-67 index
significantly correlated with larger tumors, younger age, positive
lymph nodes, a higher nuclear grade, negative ER/PgR, p53
overexpression and positive HER2. Older patients (≥65 years) had
tumors with lower proliferation; however, there was no difference
in the Ki-67 index values of the tumors in patients between 36–50
and 50–65 years of age.
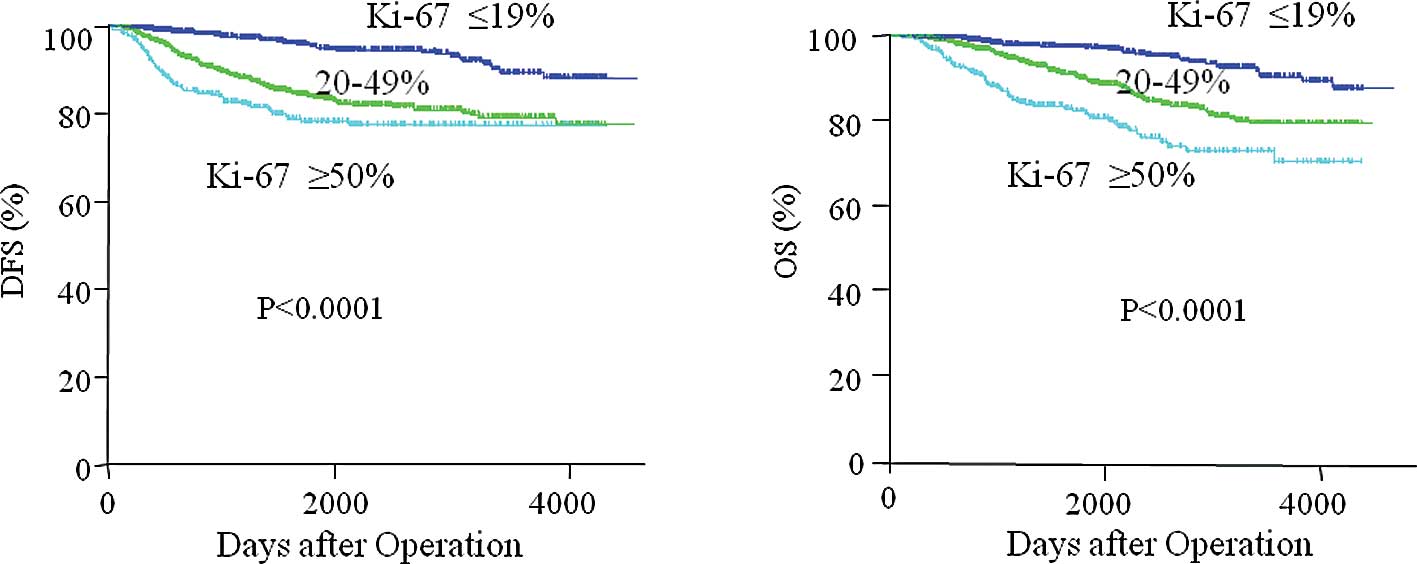
Ki-67 index and prognosis
Fig. 2 depicts the
relationship between the Ki-67 index and prognosis (Fig. 2A, DFS and 2B, OS). Patients with a
higher Ki-67 index had significantly lower DFS and OS rates than
those with a lower index. Moreover, patients with a Ki-67 index
≥20% had a similar DFS as those with an index of ≥50% 10 years
after the operation. This indicates that the dichotomized data
(<20 vs. ≥20%) was appropriate for the evaluation of DFS.
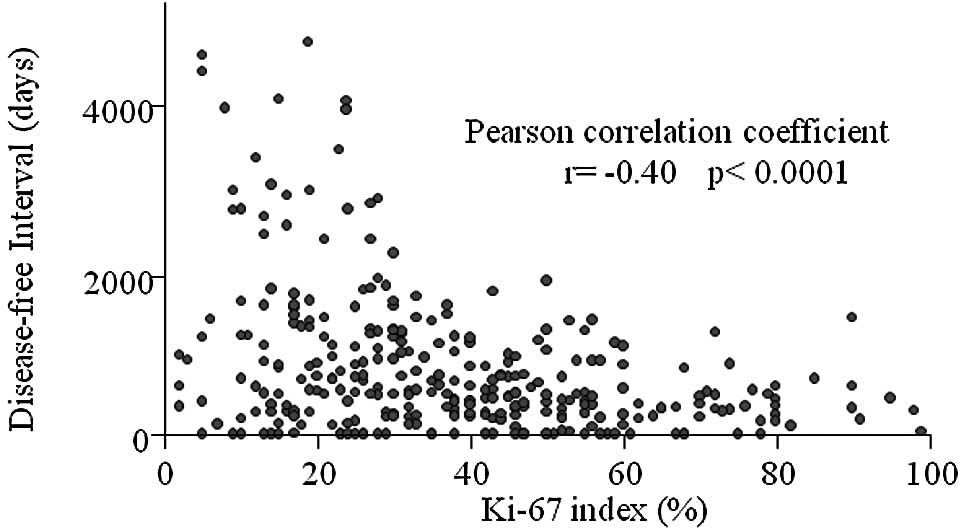
Regarding the disease-free interval times in
recurrent cases (Fig. 3), these
cases were inversely associated with Ki-67 using Pearson
correlation coefficient (P<0.0001). Moreover, most of the
patients with a Ki-67 index of ≥50% had recurrence within 2 years
after the operation. On the other hand, ∼10% of the patients with a
Ki-67 index of <20% had recurrences over 10 years. There was a
significant difference in the recurrence time after the operation
among the Ki-67 index groups (Table
VI).
Univariate and multivariate analyses were performed
to identify the prognostic factors for DFS (Table VII). The significant factors
included tumor size, lymph node status, p53, HER2, hormone
dependency and Ki-67 in the univariate analysis. Multivariate
analysis revealed that tumor size, lymph node status, Ki-67 index
and hormone dependency were significant factors for DFS. When
evaluating the significant factors for DFS as a function of lymph
node metastasis, tumor size and Ki-67 index were independent
factors in both groups. Adjuvant treatments were not significant
factors in this series (data not shown).
| Table VII.Univariate and multivariate analysis
of the factors for disease-free survival according to nodal status
in breast cancer. |
Table VII.
Univariate and multivariate analysis
of the factors for disease-free survival according to nodal status
in breast cancer.
| Factor | Category | Univariate analysis
| Multivariate
analysis (P-value)
|
|---|
| P-value | HR (95% CI) | All cases | n0 | n+ |
|---|
| Tumor size
(cm) | <2 vs. ≥2 | <0.0001 | 3.92
(3.05–5.03) | <0.00010 | 0.0004 | 0.0001 |
| Nodal status | + vs. − | <0.0001 | 5.12
(4.0–6.560) | <0.00010 | | |
| Nuclear grade | 3 vs. 1, 2 | 0.0050 | 1.52
(1.13–2.03) | 0.04200 | 0.4700 | 0.0600 |
| Ki-67 | ≥20% vs. ≤19% | <0.0001 | 3.48
(2.62–4.61) | 0.00003 | 0.0070 | 0.0005 |
| HER2 | + vs. − | <0.0001 | 1.99
(1.56–2.53) | 0.14000 | 0.3400 | 0.2400 |
| p53 | 2+ vs. −, + | <0.0001 | 2.50
(1.98–3.16) | 0.03000 | 0.8500 | 0.0200 |
| Hormone
dependency | + vs. − | <0.0001 | 0.43
(0.34–0.54) | 0.00030 | 0.2700 | 0.0005 |
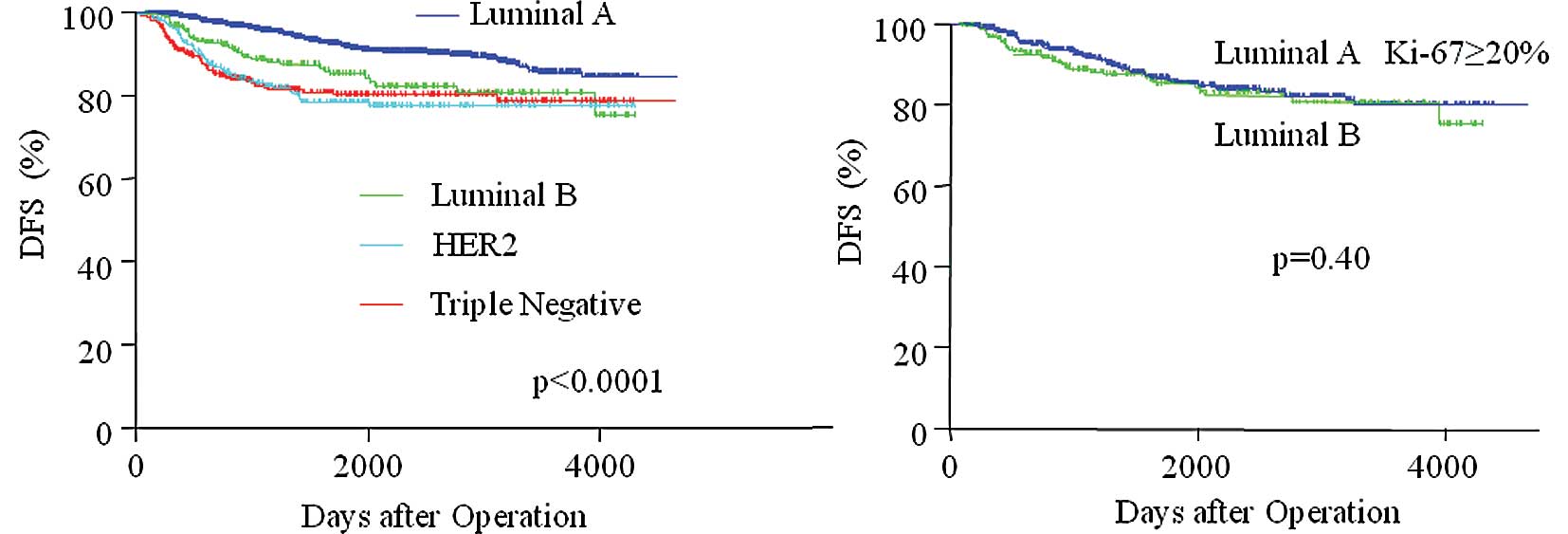
Breast cancer subtypes and prognosis
In terms of DFS after operation according to breast
cancer subtypes (Fig. 4A and
Table VIII), patients with luminal
A type tumors had more favorable DFS than patients in the other
subtype groups (P<0.0001). There were no significant differences
among types luminal B, HER2 and TN.
| Table VIII.Log-rank test; P-value between
subtypes. |
Table VIII.
Log-rank test; P-value between
subtypes.
| Luminal A vs.
B | P=0.0003 |
| Luminal A vs.
HER2 | P<0.0001 |
| Luminal A vs.
Triple negative | P<0.0001 |
| Luminal B vs.
HER2 | P=0.1500 |
| Luminal B vs.
Triple negative | P=0.1400 |
| HER2 vs. Triple
negative | P=0.9700 |
Table IX shows the
multivariate analysis of factors for DFS according to breast cancer
subtypes. Tumor size and lymph node status were significant factors
in all subtypes. However, Ki-67 index was identified as a
significant factor only in luminal A type. As shown in Fig. 4B, there was no difference in DFS
between luminal A types with Ki-67 >20% and luminal B types.
Thus, the Ki-67 index was a significant prognostic factor only in
luminal A type, and Ki-67 may distinguish the patients with poor
DFS from luminal A type patients with favorable DFS.
| Table IX.Multivariate analysis of the factors
for disease-free survival according to breast cancer subtypes. |
Table IX.
Multivariate analysis of the factors
for disease-free survival according to breast cancer subtypes.
| Factor
(category) | Multivariate
analysis (P-value)
|
|---|
| Luminal A | Luminal B | HER2 | Triple
negative |
|---|
| Tumor size (<2
cm vs. ≥2 cm) | <0.0001 | 0.035 | 0.0070 | 0.0009 |
| Nodal status (+ vs.
−) | <0.0001 | 0.002 | <0.0001 | <0.0001 |
| Ki-67 (<20% vs.
≥20%) | <0.0001 | 0.190 | 0.8700 | 0.2800 |
| p53 (−,1+ vs.
2+) | 0.0700 | 0.580 | 0.3700 | 0.1000 |
| Nuclear grade (1, 2
vs. /3) | 0.5300 | 0.950 | 0.4700 | 0.0010 |
Discussion
This study included more than 3,500 cases of breast
cancer at a single institute and evaluated the clinical
significance of the Ki-67 index as a prognostic marker in relation
to breast cancer subtypes. Moreover, the relationships between the
Ki-67 index and the clinicopathological factors that reflect
prognosis were investigated.
The Ki-67 index ranged widely from 1 to 99%, and
most of the tumors of the primary breast cancer patients showed a
peak of 10–19% with a median of 20%. Regarding the Ki-67 index and
clinicopathological factors, a higher Ki-67 index (≥20%)
significantly correlated with a higher grade of malignancy, such as
negative ER/PgR, higher grade, p53 overexpression and positive
HER2. Wiesner et al (10)
reported that a Ki-67 proliferation index ≥20% was found to be
associated with all of the prognostic factors that were tested (ER,
PgR, HER2 and nuclear grade). They stated that for routine clinical
purposes, grading appeared to add only limited information about
the prognosis in comparison to Ki-67 expression. These data suggest
that patients with a higher Ki-67 index have a poorer
prognosis.
The present analysis confirmed that Ki-67 expression
is a prognostic factor for both OS and DFS, irrespective of the
lymph nodal status. Although many studies have investigated the
possible use of Ki-67 as a prognostic marker for breast cancer, the
optimal cut-off point and scoring protocol have not yet been
standardized. The present data included 3,652 tumors, which showed
a median Ki-67 value of 20%. The median Ki-67 values were different
among the subtypes; the Ki-67 index of luminal A type tumors was
low (17%) and that of TN tumors was high (50%). Therefore, the
constant cut-off point is crucial when considering the prognosis
for breast cancer patients of all subtypes. Moreover, many studies
have adopted a cut-off point of 20% (10–13).
A prognostic significance of the Ki-67 index in each
subtype was investigated. The Ki-67 index significantly correlated
with DFS only in luminal A type tumors, and a multivariate analysis
revealed that the Ki-67 index was a significant factor in this type
of tumor. Moreover, approximately 40% of luminal A type tumors had
a higher Ki-67 index (≥20%) and showed the same DFS rate as luminal
B type tumors. The luminal A type group should be treated more
frequently with chemotherapy, as tumors with a higher Ki-67 index
frequently respond better to chemotherapy (14–16).
Cheang et al (17)
suggested that the most appropriate Ki-67 index cut-off point to
distinguish luminal B from luminal A tumors was 13.25% in a similar
manner using a gene expression profile. Hormone-sensitive breast
cancers with higher Ki-67 levels (>13.25%) were assigned to the
luminal B group and were associated with a worse prognosis compared
to tumors with lower Ki-67 levels (<13.25%). There were 625
luminal A, 263 luminal B and 55 luminal/HER2+ tumors
that were node-negative at the time of diagnosis, and these cases
were not treated with systemic therapy. This method using Ki-67 may
be suitable for the diagnosis and treatment in practical clinical
settings.
Regarding Ki-67 as a predictive factor, most of the
studies outlining the importance of Ki-67 to predict the clinical
and/or pathological response to chemotherapy in early or locally
advanced breast cancer, found that a higher Ki-67 was associated
with a more favorable response. We previously reported that there
was no pathological responder in cases with Ki-67 <25% (16).
Topoisomerase II α (topo IIα) may become a
predictive tool with which to identify candidates who may benefit
from anthracycline (18).
Furthermore, a topo IIα gene amplification is rarely detected in
HER2-negative tumors. However, hyperproliferation was found to lead
to topo IIα protein over-expression independently of topo IIα gene
status (19).
In terms of the efficacy of docetaxel,
Penault-Llorca et al (11)
reported that a higher Ki-67 (≥20%) was a candidate biomarker for
predicting the docetaxel efficacy in ER-positive breast cancer.
Notably, the predictors of tumor progression during neoadjuvant
chemotherapy included a high Ki-67 score (median score, 60% for
progressive disease vs. 30% for response/stable disease) (20). On the other hand, no significant
relationship between the Ki-67 score and response to treatment has
been reported for neoadjuvant endocrine treatment (21,22).
However, Dowsett et al (23) indicated that measurements of Ki-67
level after short-term endocrine treatment may improve the
prediction of recurrence-free survival. These findings suggest that
the Ki-67 index is an important marker, not only at baseline, but
also throughout the course of treatment.
In conclusion, the Ki-67 index had a wide
distribution of 1–99% in primary breast cancer, and the median was
20% in 3,652 cases. A higher Ki-67 index (≥20%) correlated
significantly with young age, large tumors, positive lymph nodes,
negative ER/PgR, p53 overexpression and positive HER2. A higher
Ki-67 index correlated with a poorer prognosis and early recurrence
(<2 years). On the other hand, a lower Ki-67 index correlated
with a favorable prognosis and late recurrence (>10 years).
Thus, proliferative activity determined by Ki-67 may reflect the
aggressive behavior of breast cancer and predict the time of
recurrence and the appropriate therapy. It is therefore important
to take the Ki-67 index into consideration in the treatment and
follow-up of breast cancer patients.
Acknowledgements
We would like to express our gratitude
to the staff at the Department of Clinical Pathology, Kumamoto City
Hospital, for the technical assistance and for collecting cancer
tissue.
References
|
1.
|
Goldhirsch A, Ingle JN, Gelber RD, Coates
AS, Thürlimann B and Senn HJ: panel members:. Thresholds for
therapies: highlights of the St Gallen International Expert
Consensus on the primary therapy of early breast cancer 2009. Ann
Oncol. 20:1319–1329. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Gerdes J, Schwab U, Lemke H and Stein H:
Production of a mouse monoclonal antibody reactive with a human
nuclear antigen associated with cell proliferation. Int J Cancer.
31:13–20. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Cattoretti G, Becker MH, Key G, Duchrow M,
Schlüter C, Galle J and Gerdes J: Monoclonal antibodies against
recombinant parts of the Ki-67 antigen (MIB 1 and MIB 3) detect
proliferating cells in microwave-processed formalin-fixed paraffin
sections. J Pathol. 168:357–363. 1982. View Article : Google Scholar
|
|
4.
|
Paik S, Shak S, Tang G, et al: A multigene
assay to predict recurrence of tamoxifen-treated, node-negative
breast cancer. N Engl J Med. 351:2817–2826. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Paik S, Tang G, Shak S, et al: Gene
expression and benefit of chemotherapy in women with node-negative,
estrogen receptor-positive breast cancer. J Clin Oncol.
24:3726–3734. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
De Azambuja E, Cardoso F, de Castro G Jr,
et al: Ki-67 as prognostic marker in early breast cancer: a
meta-analysis of published studies involving 12,155 patients. Br J
Cancer. 96:1504–1513. 2007.PubMed/NCBI
|
|
7.
|
Yerushalmi R, Woods R, Ravdin PM, Hayes MM
and Gelmon KA: Ki67 in breast cancer: prognostic and predictive
potential. Lancet Oncol. 11:174–183. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Urruticoechea A, Smith IE and Dowsett M:
Proliferation marker Ki-67 in early breast cancer. J Clin Oncol.
23:7212–7220. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Kai K, Nishimura R, Arima N, Miyayama H
and Iwase H: p53 expression status is a significant molecular
marker in predicting the time to endocrine therapy failure in
recurrent breast cancer: a cohort study. Int J Clin Oncol.
11:426–433. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Wiesner FG, Magener A, Fasching PA, et al:
Ki-67 as a prognostic molecular marker in routine clinical use in
breast cancer patients. Breast. 18:135–141. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Penault-Llorca F, Andre F, Sagan C, et al:
Ki67 expression and docetaxel efficacy in patients with estrogen
receptor-positive breast cancer. J Clin Oncol. 27:2809–2815. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Clahsen PC, van de Velde CJ, Duval C, et
al: The utility of mitotic index, estrogen receptor and Ki-67
measurements in the creation of novel prognostic indices for
node-negative breast cancer. Eur J Surg Oncol. 25:356–363. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Weikel W, Brumm C, Wilkens C, Beck T and
Knapstein PG: Growth fractions (Ki-67) in primary breast cancers,
with particular reference to node-negative tumors. Cancer Detect
Prev. 19:446–450. 1995.PubMed/NCBI
|
|
14.
|
Petit T, Wilt M, Velten M, et al:
Comparative value of tumour grade, hormonal receptors, Ki-67, HER2
and topoisomerase II alpha status as predictive markers in breast
cancer patients treated with neoadjuvant anthracycline based
chemotherapy. Eur J Cancer. 40:205–211. 2004. View Article : Google Scholar
|
|
15.
|
Mauriac L, MacGrogan G, Avril A, et al:
Neoadjuvant chemotherapy for operable breast carcinoma larger than
3 cm: a unicentre randomized trial with a 124-month median
follow-up. Institut Bergonie Bordeaux Groupe Sein (IBBGS). Ann
Oncol. 10:47–52. 1999. View Article : Google Scholar
|
|
16.
|
Nishimura R, Osako T, Okumura Y, Hayashi M
and Arima N: Clinical significance of Ki-67 in neoadjuvant
chemotherapy for primary breast cancer as a predictor for
chemosensitivity and for prognosis. Breast Cancer. Sept.
4–2009.(E-pub ahead of print).
|
|
17.
|
Cheang MCU, Chia SK, Voduc D, et al: Ki67
index, HER2 status, and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009. View Article : Google Scholar
|
|
18.
|
Di Leo A, Biganzoli L, Claudino W, Licitra
S, Pestrin M and Larsimont D: Topoisomerase II alpha as a marker
predicting anthracyclines' activity in early breast cancer
patients: ready for the primetime? Eur J Cancer. 44:2791–2798.
2008.
|
|
19.
|
Durbecq V, Desmed C, Paesmans M, et al:
Correlation between topoisomerase-II alpha gene amplification and
protein expression in HER-2 amplified breast cancer. Int J Oncol.
25:1473–1479. 2004.PubMed/NCBI
|
|
20.
|
Caudle AS, Gonzalez-Angulo AM, Hunt KK, et
al: Predictors of tumor progression during neoadjuvant chemotherapy
in breast cancer. J Clin Oncol. 28:1821–1828. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Chang J, Powles TJ, Allred DC, et al:
Prediction of clinical outcome from primary tamoxifen by expression
of biologic markers in breast cancer patients. Clin Cancer Res.
6:616–621. 2000.PubMed/NCBI
|
|
22.
|
Makris A, Powles TJ, Allred DC, et al:
Changes in hormone receptors and proliferation markers in tamoxifen
treated breast cancer patients and the relationship with response.
Breast Cancer Res Treat. 48:11–20. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Dowsett M, Smith IE, Ebbs SR, Dixon JM,
Skene A, A'Hern R, Salter J, Detre S, Hills M and Walsh G; IMPACT
Trialists Group: Prognostic value of Ki67 expression after
short-term presurgical endocrine therapy for primary breast cancer.
J Natl Cancer Inst. 99:167–170. 2007. View Article : Google Scholar
|