Introduction
Fibroadenoma (FA) is a common disease of the breast
in females. It may occur at any age, however, the peak age of
incidence is in the second and third decade of life. The FA can be
stimulated by estrogen, progesterone, pregnancy and lactation, and
may undergo atrophy during menopause (1,2).
Furthermore, FA is a biphasic tumor composed of stromal and
epithelial components that is typically considered to be benign,
and can be effectively treated by local excision (3).
The majority FAs are clinically identifiable,
however, 25% of cases are non-palpable and, thus, require
mammography and/or ultrasonography (US) for diagnosis (4–6). FAs can
be classified as simple or complex according to specific
histological features, with the risk of malignant transformation
higher in patients with complex FA (7). Malignant transformation within FA is
unusual, reported to be 0.1–0.3% in a screened population. However,
the number of real cases appears to be even rarer; histological
diagnosis is typically unexpected following excision of a breast
lesion, with only >100 cases reported in the literature thus far
(8,9).
Classic lobular carcinoma in situ (LCIS) is a type of
lobular neoplasia and is diagnosed when >50% of the acini of a
lobular unit are distended and distorted by a dyshesive
proliferation of cells with small, and uniform nuclei (10).
The present study describes the case of a female
that had been followed up for 20 years due to the occurrence of
multiple breast lesions; in the current study, the patient
presented with lobular carcinoma in situ (LCIS) arising
within an FA. In addition, a review of the relevant literature was
conducted. As no definitive clinical or radiological criteria exist
for diagnosing carcinoma arising in an FA, the current case was
presented to increase awareness of this entity and to discuss its
management in females of different ages.
Case report
In February 2009, a 44-year-old female presented to
Beijing Hospital (Beijing, China) with lumps in the left and right
breasts. Over the past 20 years, numerous lumps were detected in
the patient's breasts, all of which were clinically diagnosed as
FAs and treated with regular follow-up once a year. One year prior
to presentation, the patient's father was diagnosed with esophageal
cancer, the patient's older sister was diagnosed with kidney cancer
and the patient herself with a benign ovarian teratoma. The
follow-up was stopped in 2008. In 2009, physical examination
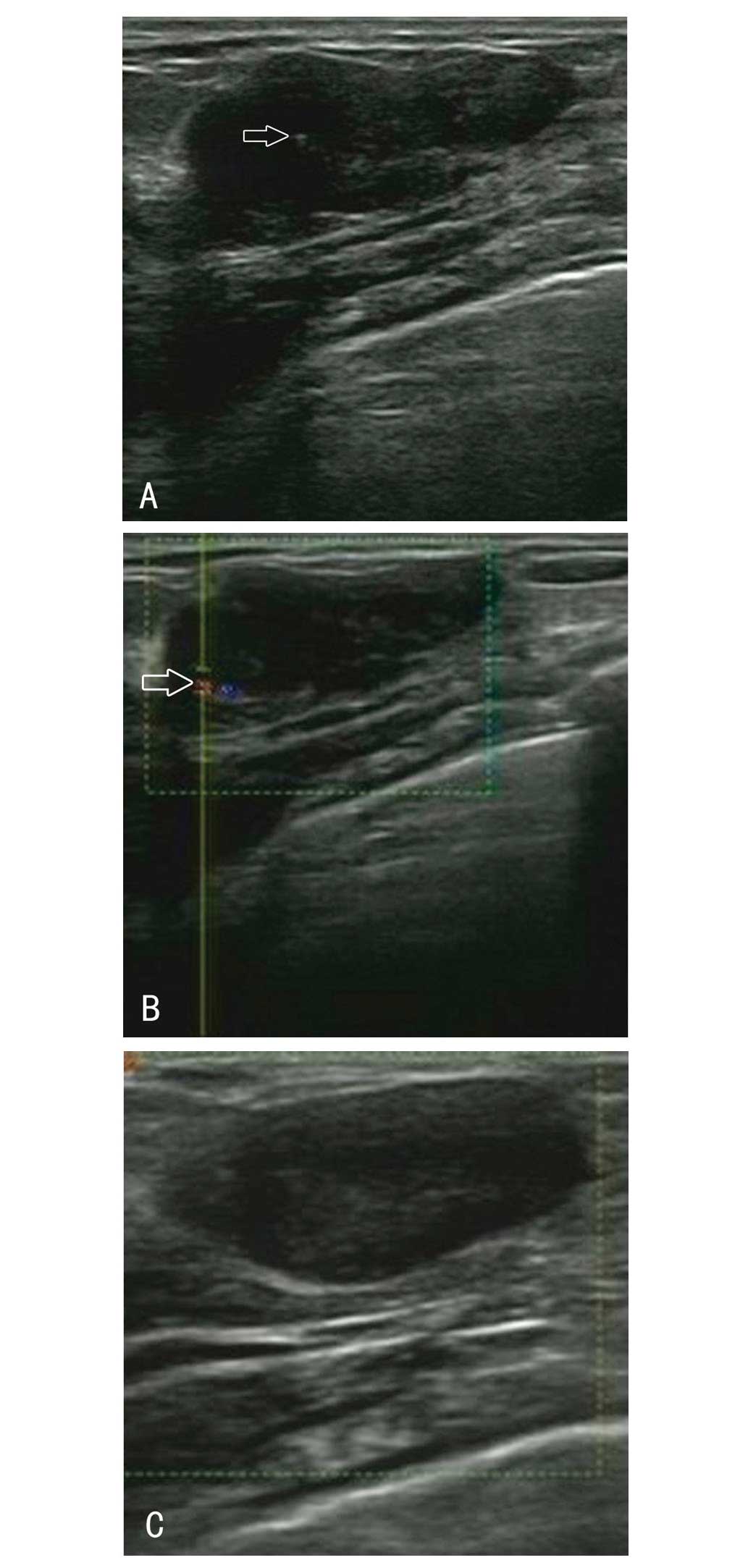
identified one enlarged lump in each breast. The largest mass in
the left breast (lump A) increased in size from 1.2×1.5
cm2 in December 2007 to 2.9×1.8 cm2 in
February 2009, as determined by US. Lump A was a lobular and
well-circumscribed heterogeneous echoic mass with a number of
hyperechoic spots. The largest mass in the right breast (lump B)
increased in size from 1.4×1.1 cm2 in December 2007 to
2.7×2.0 cm2 in February 2009. In addition, lump B was
determined to be a regular and well-circumscribed homogeneous
echoic mass. Doppler US identified a number of arterial
vascularities around lump A (Fig. 1).
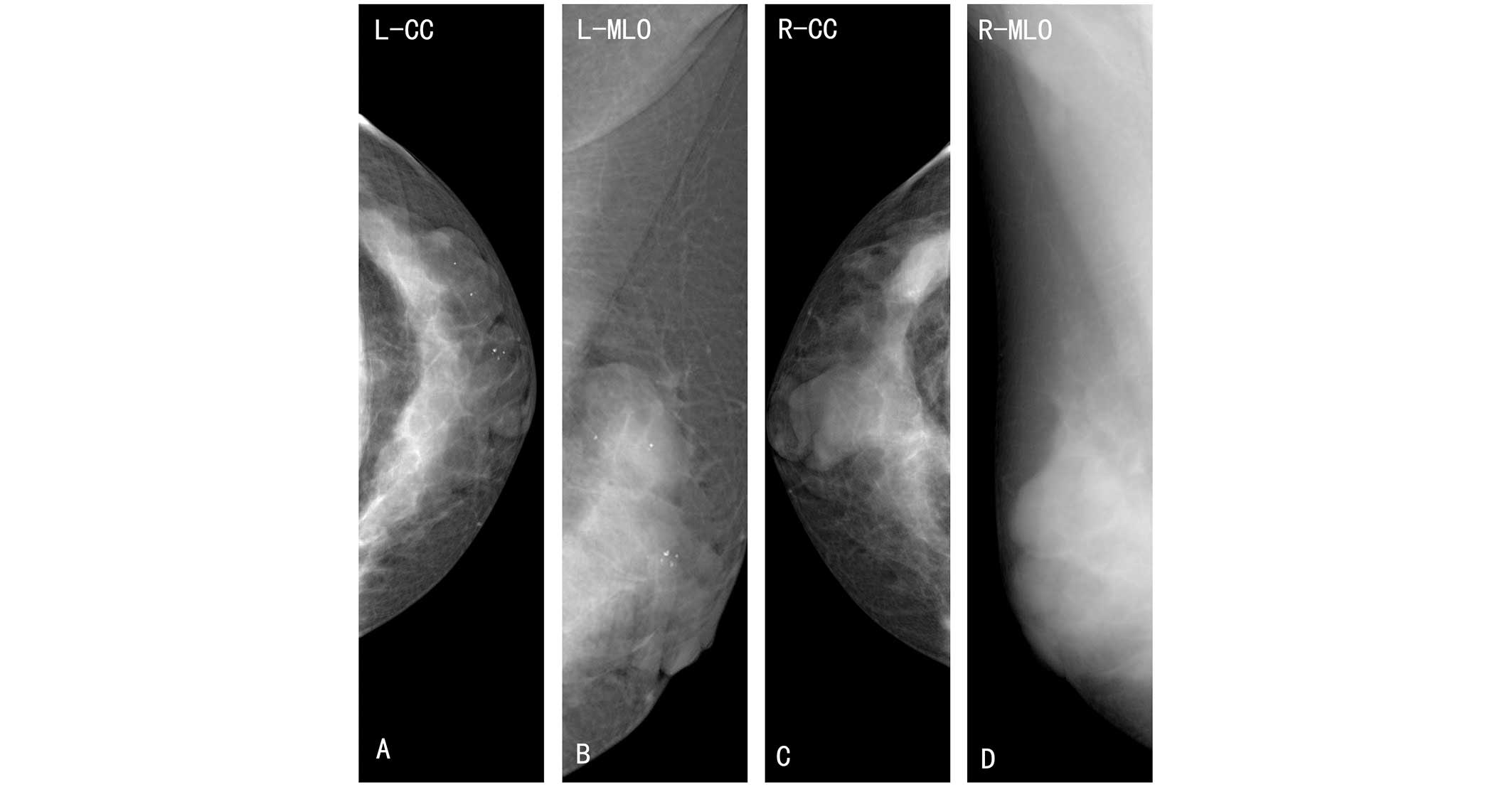
Furthermore, the mammography revealed two high-density
lobular-shaped masses in the left breast with round, scattered
calcification inside, and two high-density regularly-shaped masses
with a clear margin in the right breast (Fig. 2). Fine-needle aspiration cytology
(FNAC) determined a diagnosis of benign FA in the two lumps.
On February 13, 2009, the largest masses (lumps A
and B) were surgically excised. Lump A was histologically diagnosed
as LCIS, therefore, a mastectomy was performed on the left breast.
Subsequently, lumpectomies were performed on the remaining masses
in the right breast.
Lump A was a hard, elastic and lobular mass,
measuring 2.8×2.0×2.0 cm3 (Fig. 3). A jelly-like lesion within the mass
was observed the cut surface, measuring 5 mm in diameter and
exhibiting a well-defined boundary. Histological examination
confirmed a diagnosis of low grade LCIS within an FA (Fig. 4). Lump B comprised two discrete
lesions with an overall size of 2.6×2.5×2.0 cm3
(Fig. 3). Each cut surface was
well-circumscribed, solid and greyish in color. Histological
examination confirmed the diagnosis of FA.
Postoperatively, the patient received endocrine
therapy with tamoxifen, as the LCIS was determined to be ER and PR
positive. Clinic visits, including US, occurred every six months,
and mammographies were performed every two years. After a five-year
follow-up, no local recurrence or contralateral breast cancer were
observed. Written informed consent was obtained from the patient
for publication of this case report and any accompanying images.
The study was approved by the ethics committee of Beijing
Hospital.
Discussion
FA is a common type of benign breast lesion with a
reported incidence rate of 7–13% in female individuals. FA has been
reported from adolescence to the middle of the second decade of
life in breast disease clinics and occurs asymptomatically in 25%
of all patients. Furthermore, 13–20% of patients exhibit multiple
FAs (4–6,11).
According to its clinicopathological presentation, FA can be
divided into simple and complex FA. Complex FA is characterized by
cysts, sclerosing adenosis, epithelial calcification or papillary
apocrine change (1,11,12).
A carcinoma arising within an FA is uncommon, with
an incidence rate of 0.1–0.3% in a screened population (10). However, the actual number of cases is
even rarer, with only >100 cases reported in the worldwide
literature thus far. Therefore, histological diagnosis is typically
unexpected (1,8,9,13,14). The
mean age of patients with carcinoma in FA has been reported as
42–44 years, ~20 years subsequent to the peak age of occurrence of
FA (15,16). Two-thirds of carcinomas within FA are
lobular, and one-third are ductal or mixed ductal and lobular, with
the frequency of LCIS and ductal carcinoma in situ almost
equal (2,15). Carcinoma is diagnosed as arising
within FA if: i) The carcinoma is entirely encased within the FA;
or ii) if the carcinoma is only focally involved with the adjacent
breast tissue (3). The case presented
in the present study met the first criterion.
FA is typically considered to be a type of benign
lesion and requires careful observation. However, data regarding
whether FA is a risk factor for carcinoma is inconsistent (17). A number of studies have provided
evidence of the association between the excised FA and carcinoma.
The relative risk of developing breast cancer following surgically
excised FA appears to depend on the histological characteristics of
FA and the state of the breast parenchyma (18,19).
Dupont et al (18) identified
that patients with benign proliferative disease in the parenchyma
adjacent to the FA had a relative risk of developing carcinoma of
3.88 (95% CI, 2.1–7.3) and patients with complex FA had a relative
risk of 3.10 (95% CI, 1.9–5.1). This risk remained elevated for
decades after diagnosis. By contrast, two-thirds of the patients
with simple FA and with no family history of breast cancer did not
exhibit an increased risk of carcinoma. However, the aforementioned
studies do not explain the association between non-excised FA and
the occurrence of carcinoma.
Reports of malignant breast neoplasms are common in
the literature; however, few studies exist regarding benign breast
neoplasms. Therefore, management of FA, in particular the
management of multiple FAs, is often a dilemma for surgeons. FA is
considered to be an aberration of normal breast development
(20) and the majority that occur in
younger females may resolve or reduce in size without intervention
(6,21). Although malignancy in FA is rare it
may be difficult to predict malignant transformation in an FA, as
the clinical and radiological signs may be masked (2,22). There
is a general consensus that the management of FA depends on the age
of the patient, the nature of the lesion, the family history of
breast or ovary carcinoma, or any data of proliferative changes in
the breasts from previous biopsies (6,21). For
example, previous studies have proposed a conservative therapeutic
strategy for FA in patients younger than a certain age. However,
the threshold ages proposed or conservative treatment are
inconsistent, and have been reported as 25, 35 and 45 years
(23–26).
At the breast clinic of Beijing Hospital (Ministry
of Health, Beijing, China), >20,000 patients are examined each
year. Over 75% of biopsies of benign breast lesions are diagnosed
as FA. At the breast clinic of Beijing Hospital, the majority of
lesions can be diagnosed by performing the following triple
assessment: i) A clinical examination; ii) FNAC or core needle
biopsy; and iii) imaging methods, for example US and/or mammography
(if the patient is >35 years of age or a malignant diagnosis is
suspected) or magnetic resonance imaging. If all the results are
consistent with simple FA, two different treatment approaches are
recommended, dependent on whether the patient is younger or older
than the cut-off age of 35 years. For females aged <35 years,
expectant management with a protocol of follow-up every six months
is recommended in order to detect any changes in the lesion. If the
lesion increases in size, dissection is immediately performed.
However, if the lesion is regressive, follow up should be continued
until the regression is complete. If the lesion does not completely
regress, or stabilizes by the age of 35 years, a lumpectomy is
suggested. For females aged >35 years, surgery is recommended
when the lesion is stable or increases in size after a 6- to
12-month follow-up period. Additionally, excision is recommended
for any complex FA. For patients with a family history of breast
and/or ovarian cancer, surgery is more actively advised.
Furthermore, the recommendations for the treatment of multiple FAs
is the same as that for single FA, and dissection is advised for
any lesions with an unclear diagnosis. Patients have the right to
refuse surgery.
In conclusion, the present case was presented to
increase awareness of this entity and to discuss its management in
females of different ages.
Glossary
Abbreviations
Abbreviations:
|
FA
|
fibroadenoma
|
|
LCIS
|
lobular carcinoma in situ
|
|
DCIS
|
ductal carcinoma in situ
|
|
US
|
ultrasonography
|
|
FNAC
|
fine-needle aspiration cytology
|
References
|
1
|
Kuijper A, Mommers EC, van der Wall E and
van Diest PJ: Histopathology of the fibroadenomas of the breast. Am
J Clin Pathol. 115:736–742. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kuijper A, Preisler-Adams SS, Rahusen FD,
et al: Multiple fibroadenomas harboring carcinoma in situ in a
woman with a family history of breast/ovarian cancer. J Clin
Pathol. 55:795–797. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Azzopardi JG Ahmed and Mills RR: Problems
in breast pathologyMajor Problems in Pathology. Bennington JC: WB
Saunders Company Ltd; Edinburgh: pp. 325–328. 1979
|
|
4
|
Drukker BH: Breast disease: a primer on
diagnosis and management. Int J Fertil Womens Med. 42:278–287.
1997.PubMed/NCBI
|
|
5
|
Foster ME, Garrahan N and Williams S:
Fibroadenoma of the breast: a clinical and pathological study. J R
Coll Surg Edinb. 33:16–19. 1988.PubMed/NCBI
|
|
6
|
Greenberg R, Skornick Y and Kaplan O:
Management of breast fibroadenomas. J Gen Intern Med. 13:640–645.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Buzanowski-Konakry K, Harrison EG Jr and
Payne WS: Lobular carcinoma arising in fibroadenomas of the breast.
Cancer. 35:450–456. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Iyengar KR, Peh SC, Yip CH and
Vijayananthan A: Infiltrating duct carcinoma within a fibroadenoma.
Indian J Cancer. 46:244–246. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abe H, Hanasawa K, Naitoh H, et al:
Invasive ductal carcinoma within a fibroadenoma of the breast. Int
J Clin Oncol. 9:334–338. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lakhani SR, Ellis LO, Schnitt SJ, et al:
WHO classification of tumours of the breastLobular neoplasia.
Lakhani SR, Schnitt SJ, Malley FO, van de Vijver MJ, Simpson PT and
Palacios J: IARC Press; Lyon: pp. 77–80. 2012
|
|
11
|
Dixon JM and Mansel RE: ABC of breast
diseases. Congenital problems and aberrations of normal breast
development and involution. BMJ. 309:797–800. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tissier F, De Roquancourt A, Astier B,
Espie M, Clot P, Marty M and Janin A: Carcinoma arising within
mammary fibroadenomas. A study of six patients. Ann Pathol.
20:110–114. 2000.PubMed/NCBI
|
|
13
|
Sklair-Levy M, Sella T, Alweiss T, Craciun
I, Libson E and Mally B: Incidence and management of complex
fibroadenomas. AJR Am J Roentgenol. 190:214–218. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Netto D, Satchidanand SK and Gaeta JF:
Carcinomas arising in fibroadenomas: a report of two cases and a
review of literature. J Surg Oncol. 13:367–372. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Diaz NM, Palmer JO and McDivitt RW:
Carcinoma arising within fibroadenomas of the breast. A
clinicopathologic study of 105 patients. Am J Clin Pathol.
95:614–622. 1991.PubMed/NCBI
|
|
16
|
Pick PW and Iossifides IA: Occurrence of
breast carcinoma within a fibroadenoma. A review. Arch Pathol Lab
Med. 108:590–594. 1984.PubMed/NCBI
|
|
17
|
Dent DM and Cant PJ: Fibroadenoma. World J
Surg. 13:706–710. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dupont WD, Page DL, Parl FF, Vnencak-Jones
CL, Plummer WD Jr, Rados MS and Schuyler PA: Long-term risk of
breast cancer in women with fibroadenoma. N Engl J Med. 331:10–15.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
McDivitt RW, Stevens JA, Lee NC, Wingo PA,
Rubin GL and Gersell D: Histologic types of benign breast disease
and the risk for breast cancer. The Cancer and Steroid Hormone
Study Group. Cancer. 69:1408–1414. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hughes LE, Mansel RE and Webster DJ:
Aberrations of normal development and involution (ANDI): a new
perspective on pathogenesis and nomenclature of benign breast
disorders. Lancet. 2:1316–1319. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Carty NJ, Carter C, Rubin C, Ravichandran
D, Royle GT and Taylor I: Management of fibroadenoma of the breast.
Ann R Coll Surg Engl. 77:127–130. 1995.PubMed/NCBI
|
|
22
|
Goldman RL and Friedman NB: Carcinoma of
the breast arising in fibroadenoma, with emphasis on lobular
carcinoma. A clinicopathologic study. Cancer. 23:544–550. 1969.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cant PJ, Madden MV, Close PM, Learmonth
GM, Hacking EA and Dent DM: Case for conservative management of
selected fibro-adenomas of the breast. Br J Surg. 74:857–859. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sainsbury JR, Nicholson S, Needham GK,
Wadehra V and Farndon JR: Natural history of the benign breast
lump. Br J Surg. 75:1080–1082. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wilkinson S, Anderson TJ, Rifkind E,
Chetty U and Forrest AP: Fibroadenoma of the breast: a follow-up of
conservative management. Br J Surg. 76:390–391. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Dixon JM, Dobie V, Lamb J, Walsh JS and
Chetty U: Assessment of the acceptability of conservative
management of fibroadenoma of the breast. Br J Surg. 83:264–265.
1996. View Article : Google Scholar : PubMed/NCBI
|