Introduction
Pancreatic cancer represents the fourth most common
cause of cancer-associated mortality in the western world (1,2). Despite
significant progress in basic and clinical research, pancreatic
cancer remains a significant therapeutic challenge to humans, with
1- and 5-year survival rates of just 20 and 6%, respectively
(3,4).
The difficult surgical approach, resistance to conventional
therapies and subsequent low survival rates all contribute to the
high frequency of occurrence of lymphatic metastases (5–7).
Currently, the use of tracer agents in the detection of lymphatic
metastases is a focus of attention, as it facilitates specification
of treatment options for the given diagnosis. However, at present,
there is no acceptable and ideal imaging modality or technique for
the accurate detection of lymphatic metastases (8,9). For
example, the use of isotope tracing is limited due to the potential
side-effects of irradiation, as well as the vague surgical
resolution provided by the blue dye (10,11).
Computed tomography and conventional magnetic resonance imaging are
not sufficiently reliable for the accurate detection of lymphatic
metastases. The limitations of these tracing methods are due to the
following two aspects: i) They possess no tumor targeting effect;
and ii) the route of administration is typically through the
lymphatic system, which is difficult for the treatment of
pancreatic cancer as the pancreas is a retroperitoneal organ
(12). Therefore, the development of
a novel lymph node tracer and imaging method is required.
Photodynamic therapy (PDT), based on the
photogeneration of highly cytotoxic singlet oxygen species and the
subsequent induction of oxidative stress that results in the death
of stained cells, is currently used in oncology (13). PDT is a minimally invasive treatment
that damages target cells by inducing cytotoxicity via the
generation of cytotoxic oxygen species. The PDT components,
comprising the photosensitizer, light and oxygen, are individually
non-toxic. However, exposure of the photosensitizer to light in the
presence of oxygen induces the generation of highly reactive
singlet oxygen (1O2) species within the tumor
tissue, which results in significant damage of the cells in
proximity to the treated area (14–18). PDT
is a widely accepted treatment strategy for numerous types of
cancerous and precancerous lesion, including those in the bladder,
brain, ovary and pancreas (19–21).
However, most attention has been directed towards the therapeutic
role of the photosensitizer, rather than its potential function as
a tracer agent.
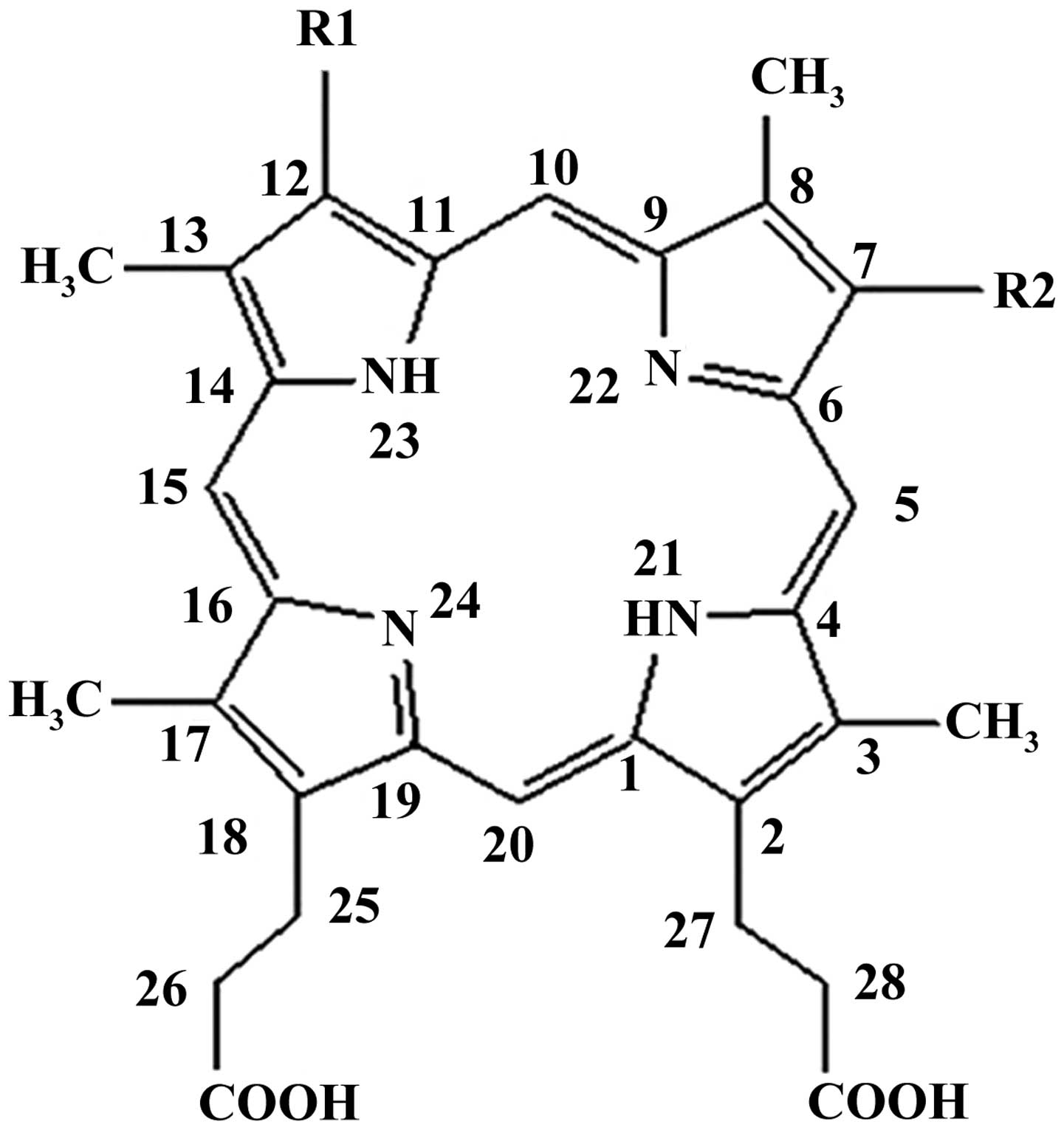
Deuteporfin, one of the novel generation of
photosensitizers, is particularly photosensitive to light with
wavelengths of 400–700 nm. Chemically, the structure of deuteporfin
is composed of four distinct sub-porphyrin derivatives:
Methoxyethy-hydroxyethyl-dipropionic, di-methoxyethyl-dipropionic,
hydroxyethy-vinyl-dipropionic and methoxyethy-vinyl-dipropionic
(Fig. 1). Compared with traditional
lymph node tracers, deuteporfin has a significant advantage in
terms of two aspects: i) Selective targeting of tumors due to high
tissue uptake and ii) that it may be administered intravenously.
The present study aimed to exploit these features of deuteporfin
for use as a tracer agent, in order to detect lymphatic metastases
in a pancreatic cancer xenograft model. The study was approved by
the ethics committee of Fudan University, Shanghai, China.
Materials and methods
Reagents
Deuteporfin was obtained from the R&D Center of
Fudan-Zhangjiang Bio-Pharmaceutical Co. Ltd. (Shanghai, China) and
was used without further purification. Normal saline was purchased
from Shanghai Baxter Healthcare Co., Ltd., Shanghai, China.
Absolute ethanol, high glucose-Dulbecco's modified Eagle's medium
(H-DMEM), fetal bovine serum (FBS), trypsin, EDTA, formalin,
paraffin, and hematoxylin and eosin (H&E) were purchased from
Sinopharm Chemical Reagent Co., Ltd. (Shanghai, China). In
addition, deionized water was from Fudan University (Shanghai,
China), and Tris-buffered saline and phosphate-buffered saline were
prepared in our laboratory. All solvents and chemicals were of
analytical grade.
Experimental animals
Sprague-Dawley (SD) rats and BALB/C-nu/nu nude mice
were purchased from the Shanghai Laboratory Animal Co. Ltd.
(Shanghai, China). The SD rats and BALB/c-nu/nu male mice were
housed in a pathogen-free animal facility. The temperature was
maintained at 23°C with a humidity of 50–60%, and the mice were
subjected to a 10/14-h light/dark cycle. All mice were provided
with food and water 3 times a week by professional technicians. All
animal studies were in compliance with the approved animal
protocols and the guidelines of the Institutional Animal Care and
Use Committee of Fudan University. The BxPC-3 human pancreatic
cancer cell line was obtained from the Shanghai Branch of the
Chinese Academy of Science, Shanghai, China.
Cell culture
The highly lymphatic metastatic pancreatic cancer
cell line was generated from BxPC-3 cells by a continuous screening
and seeding method in vivo. Briefly, 1×107 BxPC-3
cells in 100 µl normal saline were subcutaneously injected into the
left rear footpad of male BALB/C-nu/nu nude mice (n=5; aged 6–8
weeks). Six weeks later, the mice were anesthetized by intravenous
injection with chloral hydrate and sacrificed by cervical
dislocation. The lymph nodes located in the left knee, groin, side
of the iliac artery and porta renis (depression in the kidney) were
then collected. All the conjunctive tissues were removed and the
lymph nodes were gently crushed on a 200-mesh sieve (Sinopharm
Chemical Reagent Co., Ltd.). The cells routinely cultured in H-DMEM
containing 10% FBS in an incubator at a temperature of 37°C for 2–3
days. Subsequently, cells were digested by incubation with 0.025%
trypsin/0.002% EDTA and then reinoculated into another group of
mice. This procedure was repeated 5 times (total mice, n=25), until
the BxPC-3-LN5 subline was obtained, comprising BxPC-3 cells with
an increased capacity to metastasize.
Pharmacokinetics and tissue
distribution of deuteporfin in vivo
Seventy-two SD rats were randomly divided into two
equal groups, comprising the caudal vein administration group
(n=36) and the left rear footpad administration group (n=36). The
rats were injected with 2.5 mg/ml deuteporfin either intravenously
or in the left rear footpad. At various time-points (1, 3, 6, 12,
24 and 48 h) post-injection, the rats were sacrificed by cervical
dislocation and blood samples were obtained from the aorta
abdominalis (n=6 rats per timepoint). The tissues of interest
(including the heart, liver, spleen, lung, kidney, pancreas,
popliteal lymph nodes and dorsal skin) were collected immediately,
weighed and homogenized with an adequate quantity of physiological
saline. Following centrifugation at 644 × g at 25–26°C for 5 min,
the homogenate was filtered and the filtrate was boiled, cooled and
centrifuged again (644 × g at 25–26°C for 5 min). The deuteporfin
content of each tissue of interest was determined by the
fluorometric method, using a fluorescence spectrometer (F-4500;
Hitachi High-Technologies Corp., Tokyo, Japan) at excitation and
emission wavelengths of 295 and 610 nm, respectively. The standard
curve of deuteporfin was obtained by plotting the concentration vs.
fluorescence intensity.
Generation of popliteal fossa
lymphatic metastasis model
The popliteal fossa (depression behind the knee
joint) lymphatic metastases model was generated as a xenograft of
the BxPC-3-LN5 human cancer cell line. Briefly, ~1×107
BxPC-3-LN5 cells in 100 µl normal saline were injected
subcutaneously into the left rear footpad of thymus-deficient
8-week-old BALB/C nude mice (n=5; weighing 18–20 g). Five weeks
later, a lymph node intumescence or swelling that was 3–5 mm in
diameter was able to be observed in the left knee. This procedure
was repeated five times (total mice, n=25). The mice were
sacrificed by cervical dislocation and the intumescent lymph nodes
were removed and fixed in 10% neutral buffered formalin. The
specimens were dehydrated in a graded series of alcohol, and
embedded in paraffin. Serial 5-µm sections were deparaffinized,
hydrated and stained with H&E in order to detect pancreatic
cancer lymphatic metastases.
Localization of deuteporfin in tumors
at inoculation site and sites of lymphatic metastases
The BALB/C-nu/nu nude mice with pancreatic cancer
metastases were intravenously injected with deuteporfin at a dose
of 2.5 mg/ml. At given time intervals (1, 2, 4, 6, 12, 24 and 48 h)
following the injection, the mice were sacrificed by cervical
dislocation. The lymph nodes in the left (metastatic side) and
right (control side) popliteal fossa, respectively, were collected
immediately. The deuteporfin content was measured according to the
aforementioned fluorescence method.
Wood's lamp observations
The difference in deuteporfin concentration between
the cancerous and normal tissues was directly observed using a
Wood's lamp (model, BS-WL1) purchased from the Sincery
International Ltd. (Shanghai, China). Briefly, the light was turned
off and the cover shade was secured prior to usage. The Wood's lamp
was placed parallel to the mice at a distance of 15–20 cm and then
tuened on. Characteristics of the mice were identified by the
appearance of different colors under the ultraviolet ray.
Statistical analysis
The number of independent replicates is listed
individually for each experiment. All data are expressed as the
mean ± standard deviation. Statistical analyses were performed with
analysis of variance using SPSS 20.0 software (IBM SPSS, Armonk,
NY, USA) and P<0.05 was considered to indicate a statistically
significant difference.
Results
Intravenous administration of
deuteporfin is advantageous over footpad administration
The efficiency of intravenous administration of
deuteporfin was compared with that of administration via the left
rear footpad. In general, the injected SD rats appeared to be
healthy throughout the experimental period and no symptoms of a
toxic reaction to light, for example partially inflamed skin or
abscesses, were observed. Furthermore, deuteporfin was observed to
be distributed in all tissues of the body following intravenous or
left rear footpad administration. However, the distribution of
deuteporfin was uneven due to differences in blood perfusion and
the tissue microenvironment.
The mean deuteporfin levels in the blood and tissues
following intravenous administration are exhibited in Table IA. It was observed that deuteporfin
levels following intravenous treatment decreased as follows:
Blood>liver>kidney>lymph
node>pancreas>skin>heart>lungs>spleen. The
time-course changes of deuteporfin levels in the blood, liver,
kidney, heart, lungs and spleen were similar, with the highest
concentration at 1 h post-injection, followed by a time-dependent
decrease. The highest expression values attained were 108.31±1.02,
75.18±3.57, 58.52±5.19, 13.01±2.10, 1.89±2.48 and 0.36±0.57 µg/l,
respectively. Notably, the normal liver exhibited a higher level of
accumulation of deuteporfin. Previously, evidence of the poor
sensitivity of cancerous liver tissue to photosensitization was
observed when compared with that of the normal liver tissue
(22). Therefore, caution must be
taken when using PDT in the treatment of hepatic disease.
 | Table I.Deuteporfin levels in blood and
tissues of Sprague-Dawley rats following intravenous
administration. |
Table I.
Deuteporfin levels in blood and
tissues of Sprague-Dawley rats following intravenous
administration.
| A, Following
intravenous administration of deuteporfin |
|
|
|
|
|
|
|
|
|
|---|
|
|---|
|
| Concentration of
deuteporfin, µg/1 |
|---|
|
|
|
|---|
| Time, h | Blood | Heart | Liver | Spleen | Lung | Kidney | Pancreas | Lymph nodes | Skin |
|---|
| 1 |
108.31±1.02 |
13.01±2.10 |
75.18±3.57 |
0.36±0.57 |
1.89±2.48 |
58.52±5.19 |
30.14±2.56 |
28.95±7.18 |
26.87±0.51 |
| 3 |
103.00±1.14 |
6.76±4.11 |
60.47±6.21 |
0.33±0.52 |
1.18±0.46 |
35.47±11.83 |
25.89±2.29 |
22.87±4.42 |
28.08±6.37 |
| 6 |
37.67±0.55 |
6.15±1.96 |
60.93±7.01 |
0.06±0.11 |
1.19±1.55 |
31.34±13.15 |
30.38±4.05 |
25.89±5.82 |
32.24±4.95 |
| 12 |
30.00±0.27 |
4.95±0.83 |
50.11±4.5 |
0.02±0.05 |
0.86±0.23 |
44.43±9.34 |
31.60±2.85 |
24.78±7.26 |
23.74±1.50 |
| 24 |
26.5±0.51 |
3.16±0.33 |
47.19±10.89 |
0.03±0.07 |
0.85±1.29 |
52.80±11.28 |
30.97±0.86 |
16.57±2.19 |
25.76±5.04 |
| 48 |
24.18±0.07 |
3.03±0.25 |
35.29±7.05 |
0.02±0.06 |
0.81±0.69 |
42.51±7.09 |
31.95±7.93 |
22.47±1.72 |
30.86±8.29 |
|
| B, Following left
rear footpad administration of deuteporfin |
|
|
|
|
|
|
|
|
|
|
|
| Concentration of
deuteporfin, µg/1 |
|
|
|
| Time, h | Blood | Heart | Liver | Spleen | Lung | Kidney | Pancreas | Lymph nodes | Skin |
|
| 1 |
38.29±1.86 |
8.37±2.83 |
64.62±13.96 |
1.11±1.42 |
2.93±0.88 |
39.64±16.26 |
36.45±4.29 |
16.50±1.17 |
30.57±2.64 |
| 3 |
73.26±2.87 |
6.46±1.44 |
66.81±3.01 |
0.60±0.17 |
2.52±1.63 |
82.25±15.60 |
31.88±1.29 |
71.75±15.68 |
29.75±1.09 |
| 6 |
35.42±5.78 |
5.61±4.35 |
48.52±3.58 |
0.60±0.11 |
1.10±0.84 |
46.47±13.39 |
30.08±1.95 |
32.11±3.60 |
30.88±1.85 |
| 12 |
30.21±4.23 |
4.28±3.54 |
44.90±10.44 |
0.49±0.58 |
1.36±1.01 |
42.44±8.73 |
31.18±4.67 |
24.39±16.11 |
33.87±6.23 |
| 24 |
20.28±3.65 |
4.63±3.50 |
37.07±5.64 |
0.28±0.31 |
0.99±1.08 |
36.06±6.84 |
21.00±9.09 |
18.05±3.59 |
24.96±2.50 |
| 48 |
19.43±2.51 |
4.25±0.95 |
39.20±6.55 |
0.27±0.42 |
0.03±0.05 |
27.95±9.82 |
30.00±8.73 |
21.86±3.08 |
27.69±2.23 |
The mean levels of deuteporfin in the blood and
tissues following left rear footpad administration are displayed in
Table IB. In comparison to the
intravenous administration group, the entry rates of deuteporfin
into the tissues were markedly slower. For example, deuteporfin
levels in the liver, kidney, lymph node and blood were demonstrated
to reach a peak level at 3 h post-injection, and reached levels of
66.81±3.01, 82.25±15.60, 71.75±15.68 and 73.26±2.87 µg/l,
respectively. However, the deuteporfin levels in the heart, spleen,
lungs and pancreas peaked at 1 h post-injection and were
subsequently eliminated with time. Additionally, the spleen and
lungs exhibited their removal or resisting effects to deuteporfin,
as the highest deuteporfin concentrations observed were only
1.11±1.42 and 2.93±0.88 µg/l, respectively. As for the skin, a
higher level of deuteporfin (30.57 µg/l) was observed at 1 h
post-injection and the peak concentration was detected at 12 h
post-injection. It is notable that, following footpad
administration, deuteporfin may directly enter the popliteal lymph
nodes along the lymphatic vessels.
Deuteporfin may be used as a tracer to
detect lymphatic metastases in a pancreatic cancer xenograft
model
Regional lymphatic metastases from pancreatic cancer
is considered to be relevant to tumor spread and progress (23). Therefore, a reliable lymphatic
metastases model of pancreatic cancer that effectively mimics human
pancreatic cancer and may be used to test the efficacy of
therapeutic strategies, including resection and tracing, is
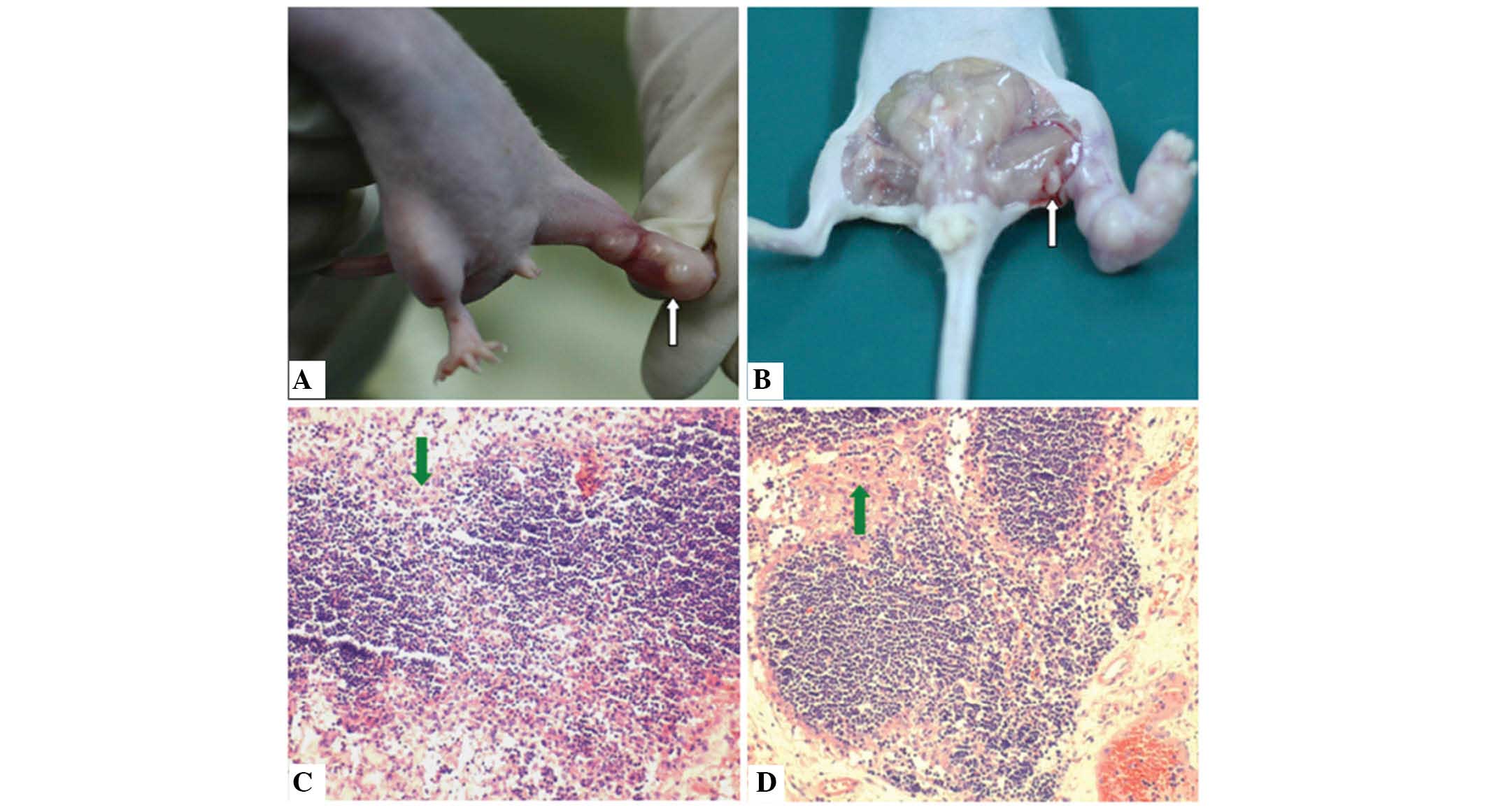
urgently required (24–26). Xenografts of the BxPC-3-LN5 pancreatic
cancer cell line with lymphatic metastases were generated in
athymic nude mice. Tumors developed at the site of direct
implantation of BxPC-3-LN5 cells in all the animals (Fig. 2A). The incidence of lymphatic
metastases was 100% and the metastatic growth of tumor cells was
observed in all cases. Swelling of the popliteal fossa lymph node
was also observed 5 weeks following implantation on the metastatic
side, but not on the control side (Fig.
2B). Immunohistochemical evaluation revealed an aggressive
invasion of cancer cells in the lymph nodes. Initially, cancer
cells were able to enter the marginal sinus and form isolated tumor
cells or small groups of metastatic niduses (Fig. 2C). Subsequently, tumor cells
accumulated to form large metastatic niduses. Certain tumor cells
were also able to infiltrate the intermediate sinuses and
proliferate, diffuse toward medullary sinuses and invade the whole
lymph node (Fig. 2D).
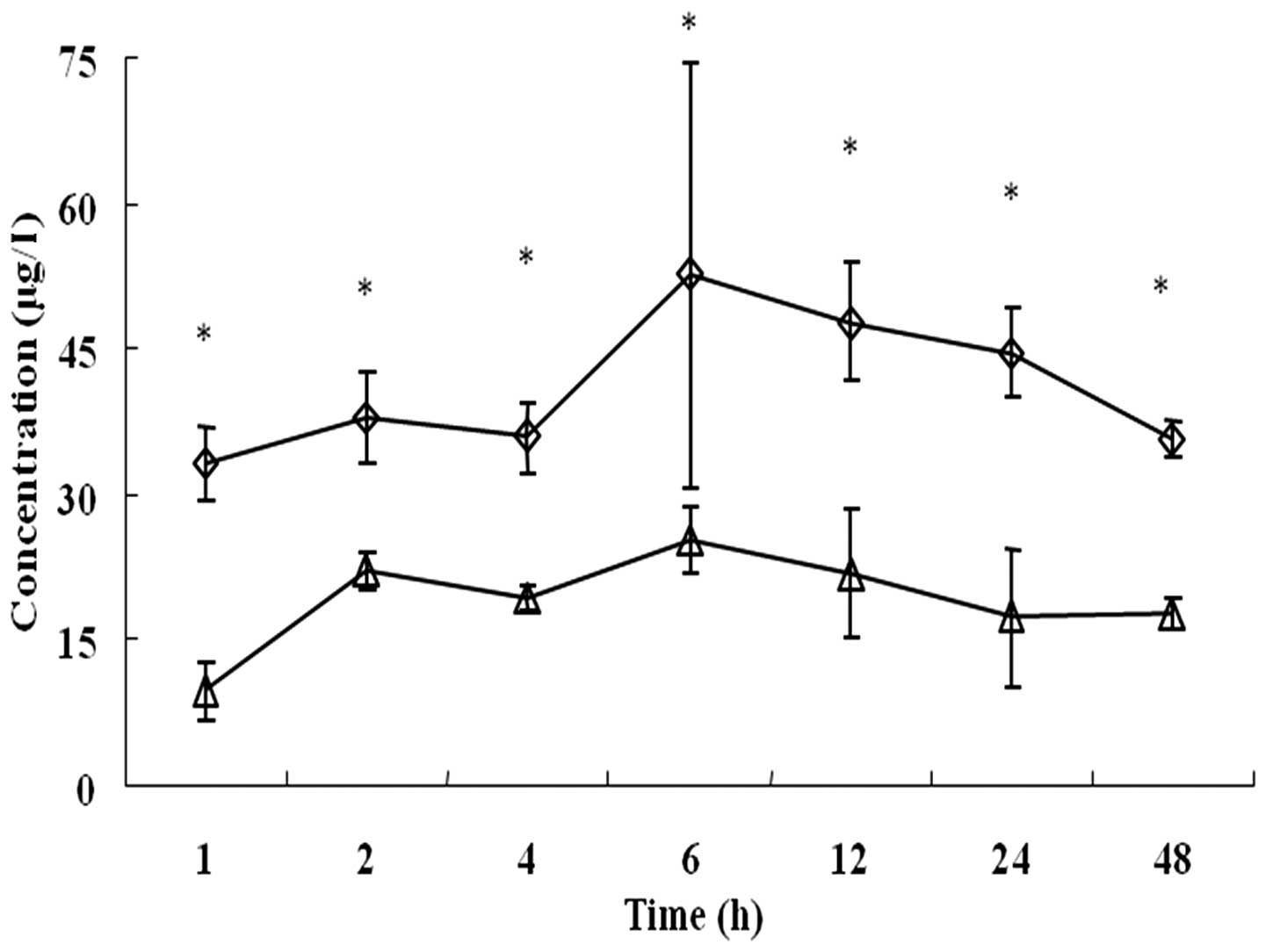
Based on this lymphatic metastases model of
pancreatic cancer, the extent of accumulation of deuteporfin in the
bilateral popliteal fossa lymph nodes, following intravenous
administration, was determined. As shown in Fig. 3, the two popliteal fossa lymph nodes
exhibited similar metabolic kinetic trends, and deuteporfin
accumulated with the highest concentration at 6 h following
administration. However, the deuteporfin concentration in the lymph
nodes was ~2–3 times higher on the metastatic side than that of the
control side (P<0.05). Furthermore, the concentration of
deuteporfin reached 33.10±3.81 µg/l at 1 h and 52.59±21.91 µg/l at
6 h, respectively, on the metastatic side; while the concentration
of deuteporfin on the control side was 9.72±2.95 µg/l at 1 h and
25.13±3.43 µg/l at 6 h, respectively. The deuteporfin concentation
peaked at 24 h on the metastatic and control sides. Subsequently,
the concentration of deuteporfin in the bilateral popliteal fossa
lymph nodes gradually decreased and reached 17.64±1.56 and
35.58±1.95 µg/l at 48 h post-injection, respectively. A previous
study reported that pancreatic cancer cells are selective to the
uptake of photosensitizers, and that the ratio of uptake of
deuteporfin between pancreatic cancer cells and normal tissues is
3:1 (27). Furthermore, the
selectivity of cancer tissues for the photosensitizer is likely
explained by their characteristic abnormal physiology, including
poor lymphatic drainage, leaky vasculature, lower pH environment,
higher level of receptors for low-density lipoproteins and abnormal
stromal composition (19,28,29). In
the present study, the concentration of deuteporfin in the
bilateral popliteal fossa lymph nodes of normal nude mice was also
evaluated, and reached 28.19±1.7l and 26.16±1.5 µg/l, respectively,
24 h post-injection. This result indicated that the selectivity of
cancer tissue to deuteporfin led to a significant decrease in the
deuteporfin concentration in the corresponding normal tissue
(P=0.002). The increased difference in drug concentration between
the cancerous and normal tissues was directly observed through the
application of the Wood's lamp (Fig.
4).
Discussion
PDT, through the use of an intravenously
administered photosensitizer, has been used as an anti-vascular and
anti-tumor therapeutic strategy for several decades (30). Furthermore, the development of lymph
node-specific PDT has generated notable interest. Kilarski et
al (31) reported that anti-lymph
node PDT allows the control of lymphatic ablation and regeneration
by alteration of the light fluence and photosensitizer dose. Other
potential therapeutic uses of lymph node-specific PDT include the
inhibition of the spread of lymph node-trafficking parasites or
pathogens, as well as slowing the clearance of locally delivered
drugs (32,33). However, the application of a
photosensitizer as a tracing agent for the detection of lymphatic
metastases of pancreatic cancer has not previously been reported or
fully explored, to the best of our knowledge.
Deuteporfin, one of the latest generation of
photosensitizers, is characterized by clear and relatively pure
chemical constituents, and has been demonstrated to possess good
photodynamic anti-tumor activity (34); however, its role as a photosensitizer
has not previously been studied. The present study aimed to
elucidate the preclinical pharmacokinetic characteristics of
deuteporfin, as well as using it in the detection of lymphatic
metastases in a pancreatic cancer xenograft model. Similarly to
previous reports (34), deuteporfin
was rapidly eliminated throughout the mouse model, which suggested
that it may be a promising drug with few side effects.
The current study was divided into two sections. The
first section aimed to identify an appropriate route of
administration for deuteporfin. The biodistribution and
pharmacokinetics of deuteporfin in SD rats, following
administration via separate routes, were therefore investigated. In
the second section, a lymphatic metastatic pancreatic cancer
xenograft model was established, and the biodistribution of
deuteporfin in cancerous and normal lymph nodes was subsequently
compared. It was demonstrated that the concentration of deuteporfin
in the metastatic lymph nodes was highest 6 h following
administration, and was ~2–3 times higher than that in the normal
lymph nodes.
Following intravenous administration, only 1.89±2.48
and 0.36±0.57 µg/l of deuteporfin were detected in the lungs and
spleen, respectively, 1 h post-injection. These low values may be a
result of specific removal or resistance mechanisms of these organs
to xenenthesis (the introduction of a novel drug in the organ).
Notably, the metabolic and retention effects of deuteporfin in the
lymph nodes, skin and pancreas stabilized, and deuteporfin reached
relatively stable levels in these organs at 48 h post-injection.
These characteristics of deuteporfin distribution indicate that it
may be helpful in the detection of lymphatic metastases and in the
treatment of pancreatic cancer.
By contrast, the lymph node deuteporfin
concentration in the footpad administration group was significantly
higher than that in the intravenous administration group
(P<0.05). However, the administration of deuteporfin in the left
rear footpad is limited in a clinical setting due to the
inconvenience of the required operation, particularly for
intraperitoneal organs, including the pancreas. In addition, the
longer distribution-equilibrium time of deuteporfin in tissues
associated with footpad administration may prolong the lucifugal or
light-repelling time of the patients. Taken together, these results
indicated that intravenous administration was the most appropriate
method for deuteporfin, compared with administration via the left
rear footpad.
Deuteporfin appeared to be selectively enriched in
cancerous pancreatic lymph nodes, and it was therefore hypothesized
that deuteporfin may be a potential tracer agent for the detection
of lymphatic metastases.
To the best of our knowledge, the present study was
the first to explore the potential use of deuteporfin as a tracer
for identifying the lymphatic metastases of pancreatic cancer. Two
administration routes were compared, and intravenous administration
was found to be more practical than the local lymphatic route for
human pancreatic cancer treatment, with the advantages of ease of
administration and more rapid metabolism. The application of
deuteporfin in the BxPC-3-LN5 human pancreatic cancer xenograft
model, clearly exhibited the potential of deuteporfin as a tracer
agent in the lymphatic metastases model of a pancreatic cancer cell
line.
Acknowledgements
The present study was financially supported by the
Shanghai Municipal Health Bureau (no. 2010Y081), the Shanghai
Medical College of Fudan University (no. 10L-10) and the National
Science Foundation of China (no. 81201896).
References
|
1
|
Saleem A, Jackson A, Mukherjee S, Stones
N, Crosby T, Tait D and Price PACORRN UK Pancreatic Radiotherapy
Group: Radiotherapy in the management of unresectable locally
advanced pancreatic cancer: A survey of the current UK practice of
clinical oncologists. Clin Oncol (R Coll Radiol). 22:257–260. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hidalgo M: Pancreatic cancer. N Engl J
Med. 362:1605–1617. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Braat H, Bruno M, Kuipers EJ and
Peppelenbosch MP: Pancreatic cancer: Promise for personalized
medicine. Cancer Lett. 318:1–8. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chan A, Diamandis EP and Blasutig IM:
Strategies for discovering novel pancreatic cancer biomarkers. J
Proteomics. 81:126–134. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
McAllaster JD and Cohen MS: Role of the
lymphatics in cancer metastasis and chemotherapy applications. Adv
Drug Deliv Rev. 63:867–875. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang F, Jin C, Subedi S, Lee CL, Wang Q,
Jiang Y, Li J, Di Y and Fu D: Emerging inorganic nanomaterials for
pancreatic cancer diagnosis and treatment. Cancer Treat Rev.
38:566–579. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Russell M and Anzai Y: Ultrasmall
superparamagnetic iron oxide enhanced MR imaging for lymph node
metastases. Radiography. 13:e73–e84. 2007. View Article : Google Scholar
|
|
9
|
Abdollahi A, Jangjoo A, Dabbagh Kakhki VR,
Rasoul Zakavi S, Memar B, Naser Forghani M, Mehrabibahar M and
Sadeghi R: Factors affecting sentinel lymph node detection failure
in breast cancer patients using intradermal injection of the
tracer. Rev Esp Med Nucl. 29:73–77. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Varghese P, Mostafa A, Abdel-Rahman AT,
Akberali S, Gattuso J, Canizales A, Wells CA and Carpenter R:
Methylene blue dye versus combined dye-radioactive tracer technique
for sentinel lymph node localization in early breast cancer. Eur J
Surg Oncol. 33:147–152. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ogasawara Y, Yoshitomi S, Sato S and
Doihara H: Clinical significance of preoperative lymphoscintigraphy
for sentinel lymph node biopsy in breast cancer. J Surg Res.
148:191–196. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Noh YW, Kong SH, Choi DY, et al:
Near-infrared emitting polymer nanogels for efficient sentinel
lymph node mapping. ACS Nano. 6:7820–7831. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Agostinis P, Berg K, Cengel KA, Foster TH,
Girotti AW, Gollnick SO, Hahn SM, Hamblin MR, Juzeniene A, Kessel
D, et al: Photodynamic therapy of cancer: An update. CA Cancer J
Clin. 61:250–281. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dolmans DE, Fukumura D and Jain RK:
Photodynamic therapy for cancer. Nat Rev Cancer. 3:380–387. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lovell JF, Liu TW, Chen J and Zheng G:
Activatable photosensitizers for imaging and therapy. Chem Rev.
110:2839–2857. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Issa MC and Manela-Azulay M: Photodynamic
therapy: A review of the literature and image documentation. An
Bras Dermatol. 85:501–511. 2010.(In English, Portuguese).
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nishioka NS: Drug, light, and oxygen: A
dynamic combination in the clinic. Gastroenterology. 114:604–606.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fan BG and Andrén-Sandberg A: Photodynamic
therapy for pancreatic cancer. Pancreas. 34:385–389. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Brown SB, Brown EA and Walker I: The
present and future role of photodynamic therapy in cancer
treatment. Lancet Oncol. 5:497–508. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Celli JP, Spring BQ, Rizvi I, Evans CL,
Samkoe KS, Verma S, Pogue BW and Hasan T: Imaging and photodynamic
therapy: Mechanisms, monitoring, and optimization. Chem Rev.
110:2795–2838. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Abd-Elgaliel WR, Cruz-Monserrate Z, Wang
H, Logsdon CD and Tung CH: Pancreatic cancer-associated Cathepsin E
as a drug activator. J Control Release. 167:221–227. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Anand S, Ortel BJ, Pereira SP, Hasan T and
Maytin EV: Biomodulatory approaches to photodynamic therapy for
solid tumors. Cancer Lett. 326:8–16. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pawlik TM, Gleisner AL, Cameron JL, et al:
Prognostic relevance of lymph node ratio following
pancreaticoduodenectomy for pancreatic cancer. Surgery.
141:610–618. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ni X, Yang J and Li M: Imaging-guided
curative surgical resection of pancreatic cancer in a xenograft
mouse model. Cancer Lett. 324:179–185. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fidler IJ: Rationale and methods for the
use of nude mice to study the biology and therapy of human cancer
metastasis. Cancer Metastasis Rev. 5:29–49. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tamada Y, Aoki D, Nozawa S and Irimura T:
Model for paraaortic lymph node metastasis produced by orthotopic
implantation of ovarian carcinoma cells in athymic nude mice. Eur J
Cancer. 40:158–163. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Schroder T, Chen IW, Sperling M, Bell RH
Jr, Brackett K and Joffe SN: Hematoporphyrin derivative uptake and
photodynamic therapy in pancreatic carcinoma. J Surg Oncol. 38:4–9.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Barrett AJ, Kennedy JC, Jones RA, Nadeau P
and Pottier RH: The effect of tissue and cellular pH on the
selective biodistribution of porphyrin-type photochemotherapeutic
agents: A volumetric titration study. J Photochem Photobiol B.
6:309–323. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dougherty TJ, Gomer CJ, Henderson BW, Jori
G, Kessel D, Korbelik M, Moan J and Peng Q: Photodynamic therapy. J
Natl Cancer Inst. 90:889–905. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Alexiades-Armenakas M: Laser-mediated
photodynamic therapy. Clin Dermatol. 24:16–25. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kilarski WW, Muchowicz A, Wachowska M,
Mężyk-Kopeć R, Golab J, Swartz MA and Nowak-Sliwinska P:
Optimization and regeneration kinetics of lymphatic-specific
photodynamic therapy in the mouse dermis. Angiogenesis. 17:347–357.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Taylor MJ, Hoerauf A and Bockarie M:
Lymphatic filariasis and onchocerciasis. Lancet. 376:1175–1185.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Padera TP, Kadambi A, di Tomaso E,
Carreira CM, Brown EB, Boucher Y, Choi NC, Mathisen D, Wain J, Mark
EJ, et al: Lymphatic metastasis in the absence of functional
intratumor lymphatics. Science. 296:1883–1886. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wang R, Hao H, Wang G, Xie H, Xu M, Wang
W, He H and Li X: Pharmacokinetics, tissue distribution and
excretion of a new photodynamic drug deuxemether. J Photochem
Photobiol B. 90:179–186. 2008. View Article : Google Scholar : PubMed/NCBI
|