Introduction
Although the incidence of gastric cancer is on the
decline, it is the fifth most common malignancy and the third
leading cause of cancer-associated death worldwide, with 952,000
new cases diagnosed and 723,000 deaths occurring in 2012 (1). In China, gastric cancer ranks as the
third most common cancer overall in incidence and mortality, with
an even higher prevalence in rural areas (2). Gastric cancer patient survival
critically depends on the stage at which the malignancy is
diagnosed. The 5-year survival rate of early stage gastric cancer
patients who have undergone resection is excellent, whereas
survival is poor for patients with advanced disease (3,4). However,
most gastric cancer patients are diagnosed only after their cancer
has reached later stages, resulting in poor prognosis due to a high
rate of relapse after gastrectomy (5). Thus, identifying gastric cancer patients
at early and curable stages of the disease is essential for
decreasing gastric cancer mortality.
Several screening techniques have been developed to
facilitate detection of gastric cancer, including barium-meal
photofluorography, gastric endoscopy and the serum pepsinogen test.
Although it has been shown that these techniques are helpful for
gastric cancer screening, none of these have become a standard or
routine screening test due to the potential risks and inconvenience
associated with these procedures (6–8). For
example, the barium-meal photofluorography test requires dietary
restriction and radiation exposure, and gastric endoscopy may
result in perforation, cardiopulmonary events, aspiration pneumonia
and bleeding (9). In addition, the
serum pepsinogen and the barium-meal photofluorography tests are
commonly plagued with false-positive results in clinical practice
(9). Furthermore, the availability of
endoscopic instruments and medical expertise required for mass
screening remains limited, especially in rural areas (10). Thus, the challenge remains to develop
a convenient, non-invasive and accurate test for detecting early
stage gastric cancer.
Gene signatures or biomarkers have shown great
potential in clinical applications such as disease detection,
prognosis and targeted therapy. Peripheral blood includes immune
cells, which dynamically respond to various physiological
conditions such as lesions and cancers occurring in the body
(10). In particular, blood-derived
RNA biomarkers are emerging as potentially important tools in the
screening and early detection of various diseases. RNA-based
biomarker technology is based on the Sentinel Principle®
(11), which suggests that
information regarding the current state of health or disease of an
organism is conveyed in the blood via interactions between
circulating blood cells and the cells, tissues and organs of the
body. Blood cells therefore act as sentinels that indicate the
status of health or disease in the body. As blood samples may be
readily obtained and with little discomfort to patients, biomarkers
derived from blood RNA provide an alternative to tissue biopsies
for the diagnosis and prognosis of disease.
Over the past decade, the gene expression pattern of
blood cells as a valuable resource for biomarker identification and
pharmacogenomics has been investigated. It has been demonstrated
that RNA profiling in whole blood may be used to develop molecular
signatures of disease across a broad spectrum of pathology
(12–15). Blood mRNA expression profiles may
identify a variety of non-hematologic disorders, such as heart
failure (16), cancer (17–21),
inflammatory bowel disease (22,23) and
psychiatric disorders (24–26).
The present study aimed to identify gastric
cancer-associated expression signatures by generating and analyzing
gene expression profiles of whole blood from gastric cancer
patients and corresponding controls.
Materials and methods
Ethics
This study was approved by the Ethics Committee of
the Second Hospital of Anhui Medical University (IRB no. KY201405).
Sample acquisition for identifying gastric cancer-specific genetic
signatures was conducted between March 2014 and February 2015 at
the Second Hospital of Anhui Medical University. All 216
participants including 36 gastric cancer patients, 55 healthy
controls and 125 non-gastric carcinoma patients were enrolled and
provided written informed consent.
Study population
A total of 36 blood samples from gastric cancer
patients were obtained from 27 male and 9 female adult patients
(age range, 21–89 years; mean age, 63±10 years) and were collected
before the patients had undergone any form of treatment including
gastrectomy, radio/chemo-therapy or surgery. Patients enrolled for
gastroendoscopy donated blood before the gastroendoscopy and were
categorized after pathological examination. Healthy control samples
comprised 55 blood samples from subjects with no pathology at
gastroendoscopy (30 males and 25 females; mean age, 31±9 years). In
addition, 125 blood samples from patients with non-gastric
carcinomas (91 males and 34 females; mean age, 56±12 years) were
collected before any form of treatment and were categorized after
pathologist reports were reviewed. The non-gastric carcinomas
included 33 lung cancers, 30 liver cancers, 21 prostate cancers, 20
nasopharyngeal carcinomas, 12 breast cancers, 8 oral cancers and 1
colorectal cancer.
Blood collection, RNA isolation and
RNA quality control
Peripheral whole blood (2.5 ml) was collected in
PaxGene Blood RNA tubes (PreAnalytix GmbH, Hombrechtikon,
Switzerland). Total RNA was then isolated as described previously
(11). RNA quality was accessed using
2100 Bioanalyzer RNA 6000 Nano Chips (Agilent Technologies, Inc.,
Santa Clara, CA, USA). All the samples for microarray analysis met
the following quality criteria: RNA integrity number ≥7.0 and
28S:18S rRNA ≥1.0. RNA quantity was determined by a NanoDrop 1000
UV-Vis spectrophotometer (Thermo Fisher Scientific, Inc., Waltham,
MA, USA).
Microarray hybridization
Whole blood RNA from the 216 samples, including 36
gastric cancer, 55 healthy controls and 125 non-gastric carcinomas,
was analysed by microarray hybridization in accordance with the
manufacturer's protocol for Gene Profiling Array cGMP U133 P2
(Affymetrix; Thermo Fisher Scientific, Inc.). A total of 200 ng of
each RNA sample was used for cDNA synthesis (GeneChip 3′IVT PLUS
Reagent kit; Thermo Fisher Scientific, Inc.) and hybridization
using the accessory reagents of the Affymetrix microarray,
according to the manufacturer's protocols. Gene expression profiles
of RNA samples were processed using Affymetrix Expression Console
software (version 1.4.1; Affymetrix; Thermo Fisher Scientific,
Inc.) and normalized by the MAS5 normalization method (27), in which the global signal intensity
value was adjusted to 500 for each microarray to make it possible
to compare the profiling variations among microarrays (27).
Microarray data analysis
To identify candidate genes for gastric cancer,
probe sets were selected from 54,675 probe sets on the Affymetrix
Gene Profiling cGMP U133 P2 microarray, according to criteria of
reliability, repeatability and linearity. A total of 4,303 probe
sets were selected for further analysis, which presented in all the
samples with intensities ranging from 100 to 10,000. These probe
sets were also present within the MAQC list for Affymetrix U133 P2
microarray, as reported by the MAQC Consortium (28) and were repeatable within ±15% in whole
blood technical replicates (unpublished data). All microarray
procedures were performed by our laboratory at the National
Engineering Center for Biochip at Shanghai (Shanghai, China).
A total of 216 samples was divided into a training
set of 31 gastric cancer, 33 controls and 99 non-gastric carcinoma
(163 samples) and a test set of 5 gastric cancer, 22 controls and
26 non-gastric carcinoma (53 samples), which were used to generate
and to validate a predictive model of gastric cancer. The
methodology for data mining was based on the self-training logistic
regression algorithm developed and reported previously (12,29,30). The
area under the receiver-operating characteristic (ROC) curve (AUC)
was calculated to characterize the ability of each probe set to
distinguish gastric cancer from healthy controls and non-gastric
carcinomas. First, of the 4,303 probe sets, the top 60 probe sets
exhibiting the highest correlation coefficient values when compared
with gastric cancer (calculated using the CORREL function of
Microsoft Excel 2010 software) were selected as the primary probe
sets. Subsequently, another 60 probe sets (of the 4,303 probe sets)
exhibiting high correlation coefficient values with the primary 60
probe sets were selected as secondary probe sets. A total of 60
primary and 60 secondary probe sets were paired one-by-one to
achieve a data matrix containing a possible 14,280 pairs of probe
sets. The pair combinations were then generated from the 14,280
pairs and were used to calculate the ROC AUC values for each pair
combination in order to find the combination with the highest ROC
AUC.
To reduce the risk of overfitting the data in the
ROC AUC calculation, each combination was limited to 2 or 3 pairs.
As the number of 3-pair combinations from 14,280 pairs was
extremely large (4.9×1011) and would make the screening
process tedious and inefficient, the process of identifying top
combinations was accelerated using a Monte Carlo algorithm
(31). First a training fold was
generated, made up of repeated random selections of gastric cancer
samples, controls, and non-gastric cancer samples; that is, each
set in the training fold was independently generated from the total
samples and contained half of the samples of each category of
samples (18 gastric cancer; 27 healthy controls and 63 non-gastric
cancer), and this process was repeated 1,000 times to produce 1,000
randomly selected sets. Three pairs from the total 14,280 pairs
were then randomly selected and combined continuously, until a
3-pair combination repetition occurred. A total of >70,000
3-pair combinations were generated during this process. The 3-pair
combination was used as a basic unit to predict gastric cancer in
the 1,000 sample cohorts of the training fold. By comparing the ROC
AUC value of each combination for predicting gastric cancer, the
final 3-pair combination with the best ability to distinguish
gastric cancer from healthy controls and from non-gastric
carcinomas was identified. The ROC AUC values of each 3-pair
combination in diagnosing gastric cancer were calculated using
Commercial MedCalc statistical software (MedCalc Software bvba,
Ostend, Belgium), according to DeLong methodology (32).
Due to the fact that the sample size used in the
present study was small, it is possible that the genes with the
highest ROC AUC values selected for gastric cancer detection may
have derived from random chance. In order to avoid this, we
performed a 2-fold cross-validation (iterated 1,000 times). In
brief, all the samples were randomly and equally distributed into
the training fold and the test fold. A predictive model was
constructed based on selected genes and using logistic regression,
according to the performance of the model in the training fold. The
model was then used to predict the rest of the samples in the test
fold. This was repeated 1,000 times. In order to test whether the
selected genes were derived due to random chance, the model was
tested twice. The first time the model was used to predict the
sample cohort with the true cancer/control status and the second
time the model was used to predict the sample cohort with the
status randomly reassigned (null set).
Results
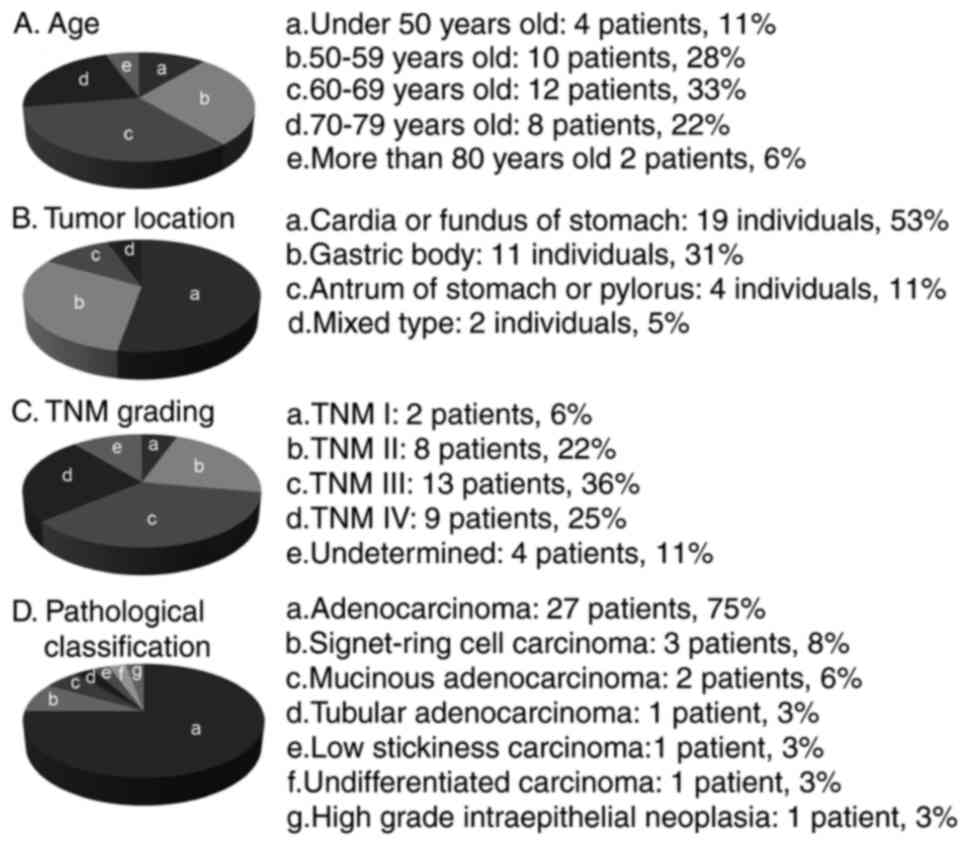
For the present study, blood samples were collected
from 216 individuals, including 36 gastric cancer patients (27
males and 9 females; mean age, 63±10 years), 55 healthy controls
(30 males and 25 females; mean age, 31±9 years) and 125 non-gastric
carcinomas (91 males and 34 females; mean age, 56±12 years). The
clinical characteristics of the gastric cancer patients are
described in Fig. 1A-D, including
age, tumor location, tumor node metastasis (TNM) status and
pathological classification.
Four candidate genes for detecting gastric cancer
were identified via a self-training logistic regression model,
including purine-rich element binding protein B (PURB),
structural maintenance of chromosomes 1A (SMC1L1), DENN/MADD
domain containing 1B (DENND1B) and programmed cell death 4
(PDCD4). Two of the genes (PURB and DENND1B)
were overexpressed (2.2- and 1.5-fold, respectively) in gastric
cancer samples when compared with healthy control samples, while
the other two genes (SMC1L1 and PDCD4) were
underexpressed (−1.6- and −1.7-fold, respectively; data not shown).
The linear fold changes in the expression of the four genes were
statistically significantly different (P<0.001) between the
gastric cancer patient samples and the healthy control samples
(data not shown). Fig. 2A and B
demonstrate, through hierarchical cluster diagrams, the performance
of each candidate gene and of the four-gene panel for gastric
cancer differentiation for a total of 216 samples (36 gastric
cancer, 55 controls and 125 non-gastric carcinomas). It was
demonstrated that the majority of the 36 gastric cancer samples
were clustered together and separated from healthy controls and
non-gastric carcinoma samples. Table
I demonstrates the performance of the four candidate genes
(PURB, SMC1L1, DENND1B and PDCD4) selected from the
microarray analysis based on 163 samples in the training set cohort
(31 gastric cancer, 33 controls and 99 non-gastric carcinoma). The
remaining 53 of the 216 samples were set aside as independent
samples for validation, as a test set cohort. The four-gene panel
had an AUC of 0.99, with 95% accuracy, 90% sensitivity, 96%
specificity for healthy controls and non-gastric carcinoma in the
training set.
 | Table I.Performance of the four-gene panel
for gastric cancer diagnosis. |
Table I.
Performance of the four-gene panel
for gastric cancer diagnosis.
|
| Training set | Test set |
|---|
|
|
|
|
|---|
| Characteristic | Gastric cancer | Healthy
controls | Non-GC
controls | Gastric
controls | Healthy
controls | Non-GC
controls |
|---|
| Positive
prediction | 28 | 0 | 5 | 5 | 0 | 3 |
| Negative
prediction | 3 | 33 | 94 | 0 | 22 | 23 |
| Sensitivity |
| 90% |
|
| 100% |
|
| Specificity |
| 96% |
|
| 94% |
|
| Accuracy |
| 95% |
|
| 94% |
|
| ROC AUC |
| 0.99 |
|
| 0.99 |
|
Mathematical predictive models built on the training
set were then used to evaluate the completely independent samples
in the test set cohort (total 53: gastric cancer, 5; controls, 22;
and non-gastric carcinoma, 26). The performance of the predictive
model for the test set had characteristics similar to that of the
training set: 0.99 of ROC AUC, 94% accuracy, 100% sensitivity, 94%
specificity for healthy controls and non-gastric carcinoma
(Table I). Three of the 26
non-gastric cancer samples, including 1 breast cancer, 1 colorectal
cancer and 1 lung cancer in the training set were predicted as
positives; the reason for these false-positive results requires
further study in larger cohorts. When results for the training set
and test set were combined, the four-gene panel had an accuracy of
95%, sensitivity of 92% and specificity of 96% for gastric cancer
diagnosis. Fig. 3A demonstrates the
performance of the four-gene panel as a box-whisker plot based on
logistic regression analysis. Fig. 3B
demonstrates the high ROC AUC value of >0.9 for gastric cancer
diagnosis.
To rule out the possibility that this four-gene
panel was due merely to chance 2-fold cross-validations were
performed, in which samples were randomly and equally divided into
training and test folds. The samples in the training folds were
used to define coefficients and thresholds for building the
predictive model based on logistic regression analysis, and the
resulting predictive model was used to make predictions of the
samples in the test folds. This process was repeated 1,000 times to
evaluate gastric cancer detection performance for the sample
cohorts using the measured gene expression data, first with the
true cancer/control status and then with the status randomly
reassigned (null set).
It was demonstrated that the distributions of the
accuracy and AUC ROC values over the 1,000 iterations resulted in 2
well-separated curves for gastric cancer, with the ‘true disease
state’ results forming a group with an accuracy and ROC AUC
>90%, whereas the ‘null-set’ with the randomly reassigned
disease status cluster had an accuracy and ROC AUC of ~50%
(Fig. 3C). There was no significant
overlap between the two clusters, from which it was concluded that
the observed performance of the 4-gene panel is unlikely to be the
result of random chance.
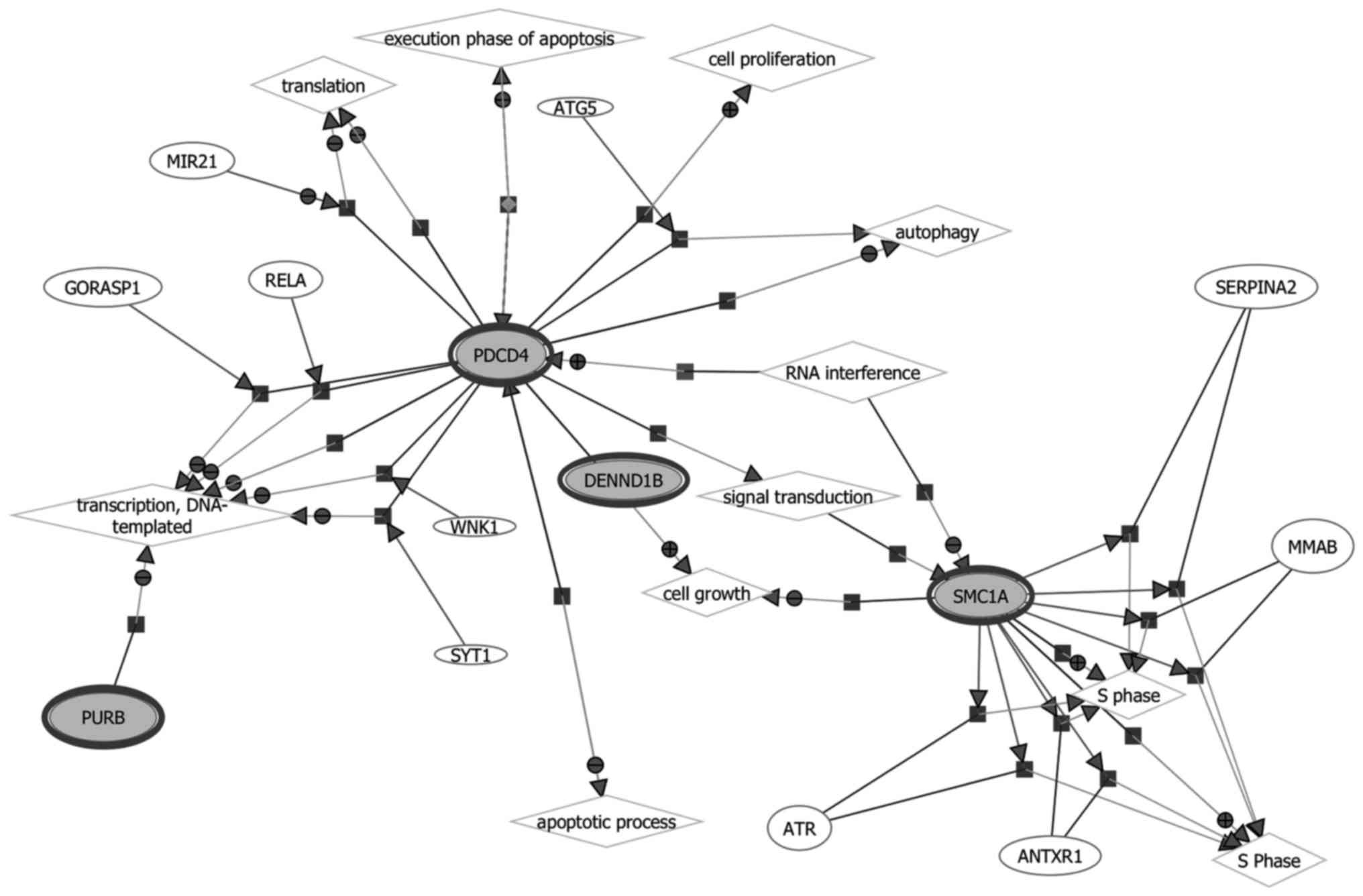
The biological functions and gene networks of the
selected 4 genes (PURB, SMC1L1, DENND1B and PDCD)
were investigated, as demonstrated in Fig. 4. Since there was an insufficient
number of genes in the gastric cancer signature to conduct pathway
analysis directly, the four genes in the blood-based gene signature
were assessed for their known protein interactions, and a
protein-protein interaction (PPI) network was constructed as
demonstrated in Fig. 5. It was
identified that 3 genes (PURB, DENND1B and PDCD) were
connected through a protein-protein network. The pathways of
PURB, DENND1B and PDCD were enriched with the
proteins in the network according to their biological functions.
SMC1L1 by contrast was not found to be connected in the
protein network, and the reason for this is unknown. Table II presents the closely associated
network canonical pathways using hypergeometric distribution
analysis.
| Table II.Closely associated canonical pathways
using a hypergeometric distribution analysis. |
Table II.
Closely associated canonical pathways
using a hypergeometric distribution analysis.
| Canonical
pathway | Genes in
category | Percent in the
observed list | Percent in the
genome | Fold of
over-representation | Odds ratio | P-value |
|---|
| RNA transport | 10 | 0.20 | 0.03 | 7.93 | 10.33 |
3.28×10−7 |
| Mismatch
repair | 5 | 0.10 | 0.00 | 26.04 | 36.63 |
9.89×10−7 |
| DNA
replication | 5 | 0.10 | 0.01 | 16.64 | 21.22 |
1.02×10−5 |
| Nucleotide excision
repair | 5 | 0.10 | 0.01 | 13.61 | 16.84 |
2.80×10−5 |
| Homologous
recombination | 4 | 0.08 | 0.00 | 17.11 | 21.47 |
7.58×10−5 |
| Ribosome | 6 | 0.12 | 0.02 | 7.90 | 9.41 |
9.63×10−5 |
| Shigellosis | 4 | 0.08 | 0.01 | 7.85 | 8.99 |
1.58×10−3 |
| Neurotrophin
signaling pathway | 5 | 0.10 | 0.02 | 4.72 | 5.31 |
3.90×10−3 |
| mRNA surveillance
pathway | 4 | 0.08 | 0.01 | 5.77 | 6.46 |
4.86×10−3 |
| Wnt signaling
pathway | 5 | 0.10 | 0.03 | 3.99 | 4.45 |
7.87×10−3 |
| Oocyte meiosis | 4 | 0.08 | 0.02 | 4.28 | 4.70 |
1.38×10−2 |
| Circadian
rhythm | 2 | 0.04 | 0.00 | 10.89 | 12.34 |
1.42×10−2 |
| Spliceosome | 4 | 0.08 | 0.02 | 3.77 | 4.12 |
2.09×10−2 |
| Ribosome biogenesis
in eukaryotes | 3 | 0.06 | 0.01 | 4.49 | 4.86 |
2.87×10−2 |
Discussion
It is well recognized that a minimally invasive,
accurate diagnostic test would be of major importance in reducing
mortality from gastric cancer. Efforts have been made to identify
biomarkers that may be of clinical use in detecting early stage
gastric cancer, including high throughput genetic, epigenetic,
transcriptomic and proteomic technologies (33,34). Other
investigators have studied circulating tumor cells in late-stage
gastric cancer (35). By contrast,
this study aimed to identify a tumor-independent gene expression
biological signature for gastric cancer in peripheral blood, a
potential ‘liquid biopsy’. Such a blood-based signature, if
clinically verified, may potentially provide an objective,
non-invasive, tissue-independent test for the detection of early
gastric cancer.
The expression signature of peripheral blood cells
that the present study has identified in gastric cancer patients
may be a result of the interaction between peripheral blood cells
and gastric cancer lesions. This hypothesis is supported by a
previous study by Sakai et al (36), who reported that the peripheral blood
cells of hepatocellular carcinoma patients shared common gene
expression alterations with tumor-infiltrating mononuclear
inflammatory cells, providing clues to the source of gene
expression alteration in peripheral blood cells of gastric cancer
patients.
Although the gastric cancer samples used in the
present study were limited in number, the prediction performance
was evaluated by distributing the samples into traditional training
and test sets. To reduce any possible bias that may occur due to
the limited number of gastric cancer samples (for example, a single
data point skewing the results, particularly for samples in the
test set), the samples were randomly distributed using a random
sampling process with fixed proportions in the training set (28/33)
and in the test set (5/33). The four-gene panel was used to predict
outcomes across the two sample sets (the training and test sets)
via random sampling and cross-validation for 1,000 iterations. The
prediction performances of the four-gene panel were consistent
throughout the 1,000-times cross-validation process, suggesting
high reliability and reproducibility of prediction results, despite
the small number of gastric cancer samples in the test set.
The blood-based four-gene signature identified in
the present study may be the first reported, and comprised the
genes PURB, SMC1L1, DENND1B and PDCD4. The four-gene
panel was obtained by analyzing blood cell expression profiles from
36 gastric cancer patients, 55 healthy controls and 125 patients
with non-gastric carcinomas. The logistic regression scores of
gastric cancer, healthy controls and non-gastric cancer carcinoma
samples in the training set (31 gastric cancers, 33 controls and 99
non-gastric carcinomas) and the test set (5 gastric cancers, 22
controls and 26 non-gastric carcinomas) were analyzed. The logistic
regression scores for each sample were calculated through a
self-trained logistic regression model. The samples were predicted
as gastric cancer if their logistic regression scores were ≥0. The
four-gene panel showed high performance in discriminating gastric
cancer from healthy controls and from non-gastric carcinomas with
an accuracy of 95% and ROC AUC value of 0.99 (95% confidence
interval) by combining the results of the training and test
sets.
There have been no previous reports associating
PURB, SMC1L1 and DENND1B with gastric cancer.
However, the involvement of PDCD4 in gastric cancer has been
extensively examined. PDCD4 is associated with tumor cell
promotion, progression and metastasis and is regarded as a tumor
suppressor and a potential molecular target for the diagnosis and
treatment of certain tumors. It has been demonstrated that
PDCD4 expression in human digestive tract cancers such as
gastric, colorectal and pancreatic cancers was significantly
downregulated compared with PDCD4 expression in normal
digestive tract tissues (37–39). In addition, the degree of PDCD4
downregulation was associated with the degree of differentiation of
hepatocellular and gastric cancer cells (36,37).
The PPI network contained 75 genes closely
associated with PURB, DENND1B and PDCD, which may be
enriched to 14 canonical pathways. Hypergeometric distribution
analysis against canonical pathways demonstrated that these genes
are closely associated with pathways involved in RNA transport,
replication and repair, oocyte meiosis and Wnt signaling. Through
the closely associated genes presented in the PPI network, the four
gastric cancer-specific genes found in this study were directly or
indirectly involved in important biological tumorigenic processes
such as regulation of cell growth and death, DNA replication and
mismatch repair (Table II).
Although SMC1L1, DENND1B and PURB have
not been directly associated with gastric cancer, these genes
exhibit biological relevance in other types of carcinoma, including
colorectal, cervical, pancreatic and renal cancer. SMC1L1 is
represented in cell cycle and oocyte meiosis pathways, which are
responsible for the structural maintenance of chromosome 1A and
provide nucleotide binding sites. SMC1L1 has not yet been
associated with gastric cancer; however, this gene is reportedly
associated with biological processes involved in cervical and
colorectal cancer. It has been reported that SMC1L1
expression is upregulated in cervical cancer relative to normal
cervical tissue (40). The
SMC1L1 protein was also identified in gastric tissue and
acts as a CDX2-binding protein, and CDX2 is regarded
as a tumor suppressor for colorectal cancer (41). The expression of SMC1L1 for the
S phase checkpoint protein was upregulated by treatment with
ferulic acid (FA), whereas FA served a protective role in the
development of colon cancer (42).
With respect to the DENND1B (DENN/MADD domain
containing 1B), its single nucleotide polymorphisms have been
significantly associated with risk for pancreatic cancer (43) and have been associated with
genetically inherited renal cancer (44). PURB is responsible for encoding
functionally cooperative proteins in the Pur family. It has been
reported that the deletion of PURB in patients with acute
myelogenous leukemia was significantly higher (>5-fold higher)
than statistically expected (45).
In conclusion, the four-gene panel identified from
peripheral blood was able to differentiate gastric cancer from
healthy controls and non-gastric carcinomas, and shows biological
plausibility in cancer pathogenesis. The biological signature
identified in this study differed from conventional tumor-derived
cancer biomarkers. The candidate four-gene signature identified in
the present study likely reflects subtle alterations in blood gene
expression, serving as a systemic response to disease and possibly
acting to maintain homeostasis or mediating disease pathology.
Although the findings of the present study require
further validation using larger cohorts, this study suggests the
possibility of detecting gastric cancer using gene expression
profiles derived from blood. As a non-invasive, blood-based test,
the gene signature may be of benefit to healthcare providers to
help assess the requirement for increased monitoring of patients,
or to suggest the requirement for further, more invasive and
expensive procedures to confirm gastric cancer in an individual
patient. The results of this study and other research demonstrate
the potential for mining the dynamic genome to identify multiple
disease signatures using quantitative RNA expression analysis of a
single blood sample.
Acknowledgements
The authors would like to thank Mr. Wang Min who
performed the Affymetrix studies, and Mr. Guangdong Duan, who
helped analyze the gene pathways. Ms Isolde Prince helped with the
editing of the manuscript.
Competing interests
Dr Choong-Chin Liew is Chair and Founder and Ma Jun
is employed by Golden Health Diagnostics Inc., China, who funded
this research.
References
|
1
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E386. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Zeng H, Zhang S and He J:
Annual report on status of cancer in China, 2011. Chin J Cancer
Res. 27:2–12. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Park JM, Ryu WS, Kim JH, Park SS, Kim SJ,
Kim CS and Mok YJ: Prognostic factors for advanced gastric cancer:
Stage-stratified analysis of patients who underwent curative
resection. Cancer Res Treat. 38:13–18. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Canyilmaz E, Soydemir G, Serdar L, Uslu
GH, Sahbaz A, Colak F, Kandaz M, Bahat Z and Yoney A: Evaluation of
prognostic factors and survival results in gastric carcinoma:
Single center experience from Northeast Turkey. Int J Clin Exp Med.
7:2656–2666. 2014.PubMed/NCBI
|
|
5
|
Hundahl SA, Phillips JL and Menck HR: The
National Cancer Data Base Report on poor survival of U.S. gastric
carcinoma patients treated with gastrectomy: Fifth Edition American
Joint Committee on Cancer staging, proximal disease, and the
‘different disease’ hypothesis. Cancer. 88:921–932. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Leung WK, Wu MS, Kakugawa Y, Kim JJ, Yeoh
KG, Goh KL, Wu KC, Wu DC, Sollano J, Kachintorn U, et al: Screening
for gastric cancer in Asia: Current evidence and practice. Lancet
Oncol. 9:279–287. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hamashima C, Shibuya D, Yamazaki H, Inoue
K, Fukao A, Saito H and Sobue T: The Japanese guidelines for
gastric cancer screening. Jpn J Clin Oncol. 38:259–267. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tashiro A, Sano M, Kinameri K, Fujita K
and Takeuchi Y: Comparing mass screening techniques for gastric
cancer in Japan. World J Gastroenterol. 12:4873–4874.
2006.PubMed/NCBI
|
|
9
|
Leja M, You W, Camargo MC and Saito H:
Implementation of gastric cancer screening-the global experience.
Best Pract Res Clin Gastroenterol. 28:1093–1106. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Park JY, Karsa L and Herrero R: Prevention
strategies for gastric cancer: A global perspective. Clin Endosc.
47:478–489. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liew CC: Method for the detection of gene
transcripts in blood and uses there of U.S. Patent Application No.
2002000268730. 1999.
|
|
12
|
Liew CC, Ma J, Tang HC, Zheng R and
Dempsey AA: Peripheral blood transcriptome dynamically reflects
system wide biology: A potential diagnostic tool. J Lab Clin Med.
147:126–132. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Burczynski ME: Transcriptional profiling
of peripheral blood in oncologySurrogate tissue analysis: Genomic,
proteomic and metabolomic approaches. Burczynski ME and Rockett JC:
(edition). Taylor and Francis; Boca Raton: pp. 47–63. 2006
|
|
14
|
Liew CC and Dzau VJ: Molecular genetics
and genomics of heart failure. Nat Rev Genet. 5:811–825. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ponnampalam SN, Kamaluddin NR, Zakaria Z,
Matheneswaran V, Ganesan D, Haspani MS, Ryten M and Hardy JA: A
blood-based gene expression and signaling pathway analysis to
differentiate between high and low grade gliomas. Oncol Rep.
37:10–22. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vanburen P, Ma J, Chao S, Mueller E,
Schneider DJ and Liew CC: Blood gene expression signatures
associate with heart failure outcomes. Physiol Genomics.
43:392–397. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Marshall KW, Mohr S, Khettabi FE, Nossova
N, Chao S, Bao W, Ma J, Li XJ and Liew CC: Blood-based biomarker
panel for stratifying current risk for colorectal cancer. Int J
Cancer. 126:1177–1186. 2010.PubMed/NCBI
|
|
18
|
Osman I, Bajorin DF, Sun TT, Zhong H,
Douglas D, Scattergood J, Zheng R, Han M, Marshall KW and Liew CC:
Novel blood biomarkers of human urinary bladder cancer. Clin Cancer
Res. 12:3374–3380. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Liong ML, Lim CR, Yang H, Chao S, Bong CW,
Leong WS, Das PK, Loh CS, Lau BE, Yu CG, et al: Blood-based
biomarkers of aggressive prostate cancer. PLoS One. 7:e458022012.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Twine NC, Stover JA, Marshall B, Dukart G,
Hidalgo M, Stadler W, Logan T, Dutcher J, Hudes G, Dorner AJ, et
al: Disease-associated expression profiles in peripheral blood
mononuclear cells from patients with advanced renal cell carcinoma.
Cancer Res. 63:6069–6075. 2003.PubMed/NCBI
|
|
21
|
Baine MJ, Chakraborty S, Smith LM, Mallya
K, Sasson AR, Brand RE and Batra SK: Transcriptional profiling of
peripheral blood mononuclear cells in pancreatic cancer patients
identifies novel genes with potential diagnostic utility. PLoS One.
6:e170142011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Burakoff R, Chao S, Perencevich M, Ying J,
Friedman S, Makrauer F, Odze R, Khurana H and Liew CC: Blood-based
biomarkers can differentiate ulcerative colitis from Crohn's
disease and noninflammatory diarrhea. Inflamm Bowel Dis.
17:1719–1725. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Burakoff R, Hande S, Ma J, Banks PA,
Friedman S, Makrauer F and Liew CC: Differential regulation of
peripheral leukocyte genes in patients with active Crohn's disease
and Crohn's disease in remission. J Clin Gastroenterol. 44:120–126.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tsuang MT, Nossova N, Yager T, Tsuang MM,
Guo SC, Shyu KG, Glatt SJ and Liew CC: Assessing the validity of
blood-based gene expression profiles for the classification of
schizophrenia and bipolar disorder: A preliminary report. Am J Med
Genet B Neuropsychiatr Genet. 133B:1–5. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Glatt SJ, Everall IP, Kremen WS, Corbeil
J, Sásik R, Khanlou N, Han M, Liew CC and Tsuang MT: Comparative
gene expression analysis of blood and brain provides concurrent
validation of SELENBP1 up-regulation in schizophrenia. Proc Natl
Acad Sci USA. 102:15533–15538. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Glatt SJ, Stone WS, Nossova N, Liew CC,
Seidman LJ and Tsuang MT: Similarities and differences in
peripheral blood gene-expression signatures of individuals with
schizophrenia and their first-degree biological relatives. Am J Med
Genet B Neuropsychiatr Genet. 156B:869–887. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Irizarry RA, Bolstad BM, Collin F, Cope
LM, Hobbs B and Speedet TP: Summaries of Affymetrix GeneChip probe
level data. Nucleic Acids Res. 31:e152003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
MAQC Consortium, . Shi L, Reid LH, Jones
WD, Shippy R, Warrington JA, Baker SC, Collins PJ, de Longueville
F, Kawasaki ES, et al: The MicroArray quality control (MAQC)
project shows inter- and intraplatform reproducibility of gene
expression measurements. Nat Biotechnol. 24:1151–1161. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Han M, Liew CT, Zhang HW, Chao S, Zheng R,
Yip KT, Song ZY, Li HM, Geng XP, Zhu LX, et al: Novel, blood-based
five-gene panel biomarker set for the detection of colorectal
cancer. Clin Cancer Res. 14:455–460. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Burakoff R, Pabby V, Onyewadume L, Odze R,
Adackapara C, Wang W, Friedman S, Hamilton M, Korzenik J, Levine J,
et al: Blood-based biomarkers used to predict disease activity in
Crohn's disease and ulcerative colitis. Inflamm Bowel. Dis.
21:1132–1140. 2015.
|
|
31
|
Chao S, Cheng C and Liew CC: Mining the
dynamic genome: A method for identifying multiple disease
signatures using quantitative RNA expression analysis of a single
blood sample. Microarrays (Bassel). 4:671–689. 2015. View Article : Google Scholar
|
|
32
|
DeLong ER, DeLong DM and Clarke-Pearson
DL: Comparing the areas under two or more correlated receiver
operating characteristic curves: A nonparametric approach.
Biometrics. 44:837–845. 1988. View
Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang Z, Dou M, Yao X, Tang H, Li Z and
Zhao X: Potential biomarkers in diagnosis of human gastric cancer.
Cancer Invest. 34:115–122. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kalnina Z, Meistere I, Kikuste I, Tolmanis
I, Zayakin P and Line A: Emerging blood-based biomarkers for
detection of gastric cancer. World J Gastroenterol. 21:11636–11653.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Matsumura N, Zembutsu H, Yamaguchi K,
Sasaki K, Tsuruma T, Nishidate T, Denno R and Hirata K:
Identification of novel molecular markers for detection of gastric
cancer cells in the peripheral blood circulation using genome-wide
microarray analysis. Exp Ther Med. 2:705–713. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sakai Y, Honda M, Fujinaga H, Tatsumi I,
Mizukoshi E, Nakamoto Y and Kaneko K: Common transcriptional
signature of tumor-infiltrating mononuclear inflammatory cells and
peripheral blood mononuclear cells in hepatocellular carcinoma
patients. Cancer Res. 68:10267–10279. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tu H, Sun H, Lin Y, Ding J, Nan K, Li Z,
Shen Q and Wei Y: Oxidative stress upregulates PDCD4 expression in
patients with gastric cancer via miR-21. Curr Pharm Des.
20:1917–1923. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ma G, Zhang H, Dog M, Zheng X, Ozaki I,
Matsuhashi S and Guo K: Downregulation of programmed cell death 4
(PDCD4) in tumorigenesis and progression of human digestive tract
cancers. Tumour Biol. 34:3879–3885. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yu H, Zeng J, Liang X, Wang W, Zhou Y, Sun
Y, Liu S, Li W, Chen C and Jia J: Helicobacter pylori promotes
epithelial-mesenchymal transition in gastric cancer by
downregulating programmed cell death protein 4 (PDCD4). PLoS One.
9:e1053062014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Narayan G, Bourdon V, Chaganti S,
Arias-Pulido H, Nandula SV, Rao PH, Gissmann L, Dürst M, Schneider
A, Pothuri B, et al: Gene dosage alterations revealed by cDNA
microarray analysis in cervical cancer: Identification of candidate
amplified and overexpressed genes. Genes Chromosomes Cancer.
46:373–384. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Jeong MS, Hwang EY, Kim HT, Yoo M and Jang
SB: Purification of caudal-related homeodomain transcription factor
and its binding characterization. J Microbiol Biotechnol.
19:1557–1564. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Janicke B, Hegardt C, Krogh M, Onning G,
Akesson B, Cirenajwis HM and Oredsson SM: The antiproliferative
effect of dietary fiber phenolic compounds ferulic acid and
p-coumaric acid on the cell cycle of Caco-2 cells. Nutr Cancer.
63:611–622. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cotterchio M, Lowcock E, Bider-Canfield Z,
Lemire M, Greenwood C, Gallinger S, Gallinger S and Hudson T:
Association between variants in atopy-related immunologic candidate
genes and pancreatic cancer risk. PLoS One. 10:e01252732015.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Nookala RK, Langemeyer L, Pacitto A,
Ochoa-Montaño B, Donaldson JC, Blaszczyk BK, Chirgadze DY, Barr FA,
Bazan JF and Blundell TL: Crystal structure of folliculin reveals a
hidDENN function in genetically inherited renal cancer. Open Biol.
2:1200712012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lezon-Geyda K, Najfeld V and Johnson EM:
Deletions of PURA, at 5q31, and PURB, at 7p13, in myelodysplastic
syndrome and progression to acute myelogenous leukemia. Leukemia.
15:954–962. 2001. View Article : Google Scholar : PubMed/NCBI
|