Introduction
Malignant melanoma predominantly occurs in the skin,
mucous membranes and the choroid. Malignant melanoma of the breast
is particularly rare. The incidence of primary melanoma of the
breast is <5% of all melanomas (1). Observation of the clinical
pathological features, immunohistochemical staining methods and
tissue tissue origin are required to identify primary malignant
melanoma of the breast, as well as other types of breast tumour.
Surgical resection is the commonly adopted treatment method for
malignant melanoma, supplemented by chemo-, radio- and
immunotherapy treatments resulting in a comprehensive treatment
strategy.
In the current study, a 26-year-old female patient
exhibiting a primary malignant melanoma of the breast is presented,
and the clinical and pathological features, diagnosis and
treatments are discussed in correlation with the literature.
Patient provided written informed consent.
Case report
A 26-year-old female was admitted to the Department
of General Surgery of Daping Hospital and Research Institute of
Surgery (Chongqing, China), due to the presence of a painless mass
in the left breast for three months. The patient indicated that the
mass had recently grown rapidly. The patient had no notable medical
history or family history of carcinoma. Clinical examination
revealed a 3×2-cm firm irregular mass in the upper inner quadrant
of the left breast. There was no change in the appearance of the
local skin, no discharge from, or retraction of, the nipple. A
small number of lymph nodes were palpated in the left axilla. The
breast magnetic resonance imaging result indicated left breast
cancer due to the presence of enlarged left axillary lymph nodes. A
chest computed tomography (CT) scan demonstrated widespread lung
and pleural nodules, indicating lung and pleural metastases. An
emission CT whole body bone scintigraphy indicated destruction to
multiple ribs, the cervical vertebrae and thoracic bone. A core
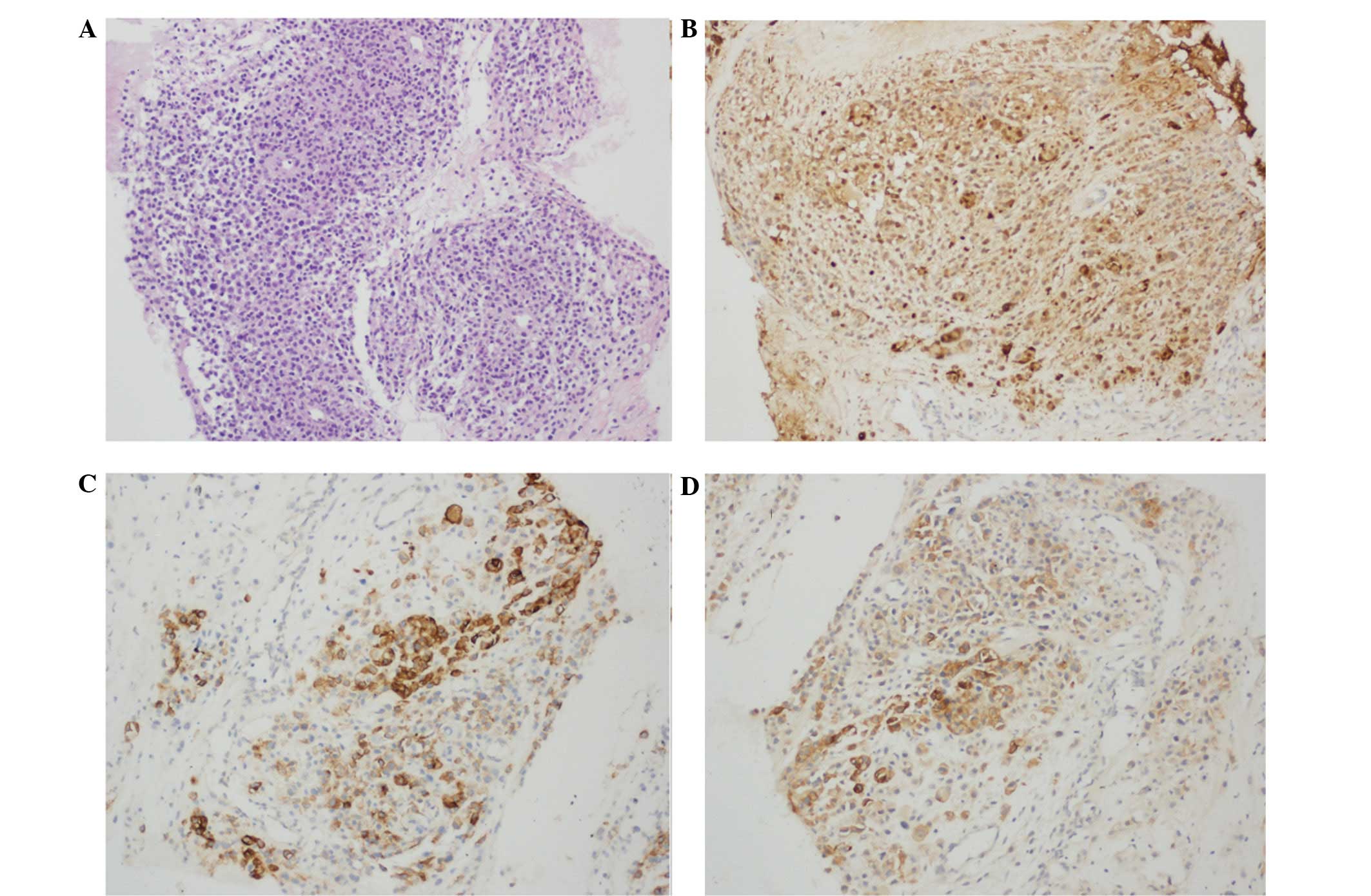
needle biopsy of the breast mass and hematoxylin and eosin staining
demonstrated that the mass tissue was comprised of a large
distribution of diffuse small cells. Those cells were round or
oval, with large nuclei and nucleoli, and abundant cytoplasm. No
significant intracellular pigmentation was observed (Fig. 1A). Immunohistochemistry demonstrated
that the tumour cells were immunopositive for S-100, HMB-45 and
melan-A (Fig. 1B–D). However. a
panel of markers that included epithelial markers, such as
cytokeratin (CK) and epithelial membrane antigen (EMA), and
mesenchymal markers, such as vimentin, smooth muscle antigen (SMA),
estrogen receptor, progesterone receptor and HER2 were negative.
The percentage of Ki-67-positive cells was 30%.
Based on the pathologic and immunohistochemical
features, a diagnosis of malignant melanoma was proposed. Careful
examination of the skin and mucous membranes failed to reveal a
malignant melanoma. Therefore this patient was diagnosed with a
primary malignant melanoma of the left breast with extensive
metastasis. The patient refused surgery and further treatment and
was automatically discharged. Two months later, the patient
succumbed as a result of widespread metastases.
Discussion
Malignant melanoma is a highly malignant tumour that
is derived from melanocytes. The incidence of malignant melanoma
has risen markedly over the last decade. It occurs anywhere on the
body, however, is commonly found in the skin, mucous membranes and
the choroid. Primary melanoma of the breast is particularly rare,
with an incidence of <5% of all malignant melanomas (1,2). The
aetiology of malignant melanoma remains unknown. It is generally
hypothesised to be associated with excessive exposure to
ultraviolet radiation from the sun. In addition, it is associated
with ethnicity, the endocrine and immune systems, chronic
stimulation and improper surgery may cause the progression of nevus
into malignant melanoma.
Malignant melanoma of the breast has four
predominant manifestations: i) Primary malignant melanoma of the
breast skin; ii) malignant melanoma metastasis to the breast; iii)
in-transit metastases to breast tissue and skin; and iv) primary
malignant melanoma of the breast gland (1). The diagnosis of primary malignant
melanoma of the breast is highly dependent on pathological
morphology, immunohistochemistry and electron microscopy, amongst
other diagnostic techniques, and the following should be noted
during diagnosis: i) Pleomorphism of tumour cells and nuclear
atypia; ii) scattered intracellular pigment granules (although
there are 6–10% of malignant melanomas exhibiting little or no
pigment, which are termed amelanotic melanoma) (3); iii) immunohistochemistry results
demonstrating positive expression of the proteins S-100, HMB-45 and
melan-A (4); iv) electron
microscopy identifying melanosome and former melanosome (5); v) the edge of the tumour tissue and
normal breast tissue does not exhibit a transition; and vi)
exclusion of tumour metastases and tumor invasion from neighboring
sites. The diagnosis of malignant melanoma is occasionally
particularly complex and, therefore, requires the use of
immunohistochemical staining for its identification. Positive
expression of S-100 is an exceptionally sensitive indicator for
malignant melanoma, however, it is also expressed in 50% of breast
cancer cases. Therefore it must be observed in combination with a
positive expression of HMB-45 and melan-A for the diagnosis of
primary melanoma of the breast. Whereas other indicators, such as
CK, vimentin and SMA, demonstrate a negative expression and signal
the presentation of other types of tumours. Furthermore, Ki-67
staining may be used to distinguish between benign and malignant
tumours (6,7).
In the present study, the first symptom that was
noted by the patient was the tumour in the left breast. Based on
the clinical examination, histopathological features and results
from immunohistochemical staining, the patient was diagnosed with a
primary malignant melanoma of the breast.
The treatment of primary malignant melanoma of the
breast is the same as that for other malignant melanoma located
elsewhere on the body. The primary treatment method is surgical
resection, with an appropriate combination of chemo-, radio-,
immuno- and targeted therapy (1,8). Wide
local excision is the predominant surgical approach. It is
generally hypothesised that a cutting edge of 2 cm ensures the
reliability of the surgery. A mastectomy does not improve the
patient’s prognosis, and a comprehensive axillary lymph node
dissection is required when preoperative axillary lymph node
metastasis is identified and confirmed. A sentinel lymph node
biopsy reduces the requirement for an unnecessary lymph node
dissection (9,10).
The role of adjuvant chemo- or radiotherapy, either
singularly or in combination, remains unknown with regard to their
efficacy in malignant melanoma. Chemotherapy is commonly used for
pre- and postoperative adjuvant therapy and for those who are not
suitable for, or refuse, surgery or for those patients who exhibit
widespread metastases. The chemotherapy programme is usually with a
dacarbazine-based treatment plan, however, the effective rate is
only 7–13% (11). Other commonly
used agents include temozolomide, cisplatin and taxol; multi-agent
chemotherapy may improve the treatment outcome. Adjuvant
radiotherapy may be performed when removal of the lesion is not
possible, there are positive margins, the lymph node size is >3
cm, the number of lymph nodes involved exceeds four or when there
is local recurrence or distant metastases. Although adjuvant
radiotherapy decreases the local regional failure from 30 to 10%,
the survival rate of patients remains unknown (12,13).
Malignant melanoma is an immunogenic tumour and
adjuvant immunotherapy is associated with high-risk tumours.
Interferon, interleukin-2 and other biological response modifiers
for malignant melanoma have a moderate effect. It is reported that
immunotherapy in combination with chemotherapy may improve the
efficiency of patient treatment, however, the long-term effects
require further investigation (14–16).
In recent years, numerous novel biological and
molecular targeted therapies have been adopted for the treatment of
malignant melanoma. Clinical studies have identified that
ipilimumab (a monoclonal antibody that blocks cytotoxic T
lymphocyte-associated antigen 4) and vemurafenib (oncogenic
BRAF-inhibitor agent) improve the overall response rate, and
prolong the progression-free survival and overall survival for
advanced malignant melanoma patients. However, the specific
efficacy is currently being investigated and evaluated (17–19).
In conclusion, primary malignant melanoma of the
breast is a particularly rare type of tumour and the prognosis is
somewhat poor. The diagnosis depends on histopathological
assessment and immunohistochemical staining combined with a
detailed clinical history and careful physical examination. Early
diagnosis, correct surgical resection and comprehensive adjuvant
therapy are significant factors for improving the patient survival
rate.
Acknowledgements
The present study was supported by the Natural
Science Foundation of Chongqing (project no. CSTC, 2011BB5032).
References
|
1
|
Kurul S, Taş F, Büyükbabani N, et al:
Different manifestations of malignant melanoma in the breast: a
report of 12 cases and a review of the literature. Jpn J Clin
Oncol. 35:202–206. 2005.
|
|
2
|
Alzaraa A and Sharma N: Primary cutaneous
melanoma of the breast: A case report. Cases J. 1:2122008.
|
|
3
|
Duggal R and Srinivasan R: Primary
amelanotic melanoma of the cervix: case report with review of
literature. J Gynecol Oncol. 21:199–202. 2010.
|
|
4
|
Bonetti F, Pea M, Martignoni G, et al:
False-positive immunostaining of normal epithelia and carcinomas
with ascites fluid preparations of antimelanoma monoclonal antibody
HMB45. Am J Clin Pathol. 95:454–459. 1991.
|
|
5
|
Taatjes DJ, Arendash-Durand B, von
Turkovich M and Trainer TD: HMB-45 antibody demonstrates melanosome
specificity by immunoelectron microscopy. Arch Pathol Lab Med.
117:264–268. 1993.
|
|
6
|
Ohsie SJ, Sarantopoulos GP, Cochran AJ and
Binder SW: Immunohistochemical characteristics of melanoma. J Cutan
Pathol. 35:433–444. 2008.
|
|
7
|
Lee AH: Use of immunohistochemistry in the
diagnosis of problematic breast lesions. J Clin Pathol. 66:471–477.
2013.
|
|
8
|
Davar D, Tarhini AA and Kirkwood JM:
Adjuvant therapy for melanoma. Cancer J. 18:192–202. 2012.
|
|
9
|
Biswas A, Goyal S, Jain A, et al: Primary
amelanotic melanoma of the breast: combating a rare cancer. Breast
Cancer. 21:236–240. 2014.
|
|
10
|
Thompson JF, McCarthy WH, Bosch CM, et al:
Sentinel lymph node status as an indicator of the presence of
metastatic melanoma in regional lymph nodes. Melanoma Res.
5:255–260. 1995.
|
|
11
|
Avril MF, Aamdal S, Grob JJ, et al:
Fotemustine compared with dacarbazine in patients with disseminated
malignant melanoma: a phase III study. J Clin Oncol. 22:1118–11125.
2004.
|
|
12
|
Lee RJ, Gibbs JF, Proulx GM, et al: Nodal
basin recurrence following lymph node dissection for melanoma:
implications for adjuvant radiotherapy. Int J Radiat Oncol Biol
Phys. 46:467–474. 2000.
|
|
13
|
Calabro A, Singletary SE and Balch CM:
Patterns of relapse in 1001 consecutive patients with melanoma
nodal metastases. Arch Surg. 124:1051–1055. 1989.
|
|
14
|
Thompson JF, Scolyer RA and Kefford RF:
Cutaneous melanoma. Lancet. 365:687–701. 2005.
|
|
15
|
Verma S, Quirt I, McCready D, et al:
Systematic review of systemic adjuvant therapy for patients at high
risk for recurrent melanoma. Cancer. 106:1431–1442. 2006.
|
|
16
|
Hauschild A, Weichenthal M, Rass K, et al:
Efficacy of low-dose interferon α2a 18 versus 60 months of
treatment in patients with primary melanoma of >= 1.5 mm tumor
thickness: results of a randomized phase III DeCOG trial. J Clin
Oncol. 28:841–846. 2010.
|
|
17
|
Chapman PB, Hauschild A, Robert C, et al;
BRIM-3 Study Group. Improved survival with vemurafenib in melanoma
with BRAF V600E mutation. N Engl J Med. 364:2507–2516. 2011.
|
|
18
|
Ribas A, Hersey P, Middleton MR, et al:
New challenges in endpoints for drug development in advanced
melanoma. Clin Cancer Res. 18:336–41. 2012.
|
|
19
|
Spagnolo F and Queirolo P: Upcoming
strategies for the treatment of metastatic melanoma. Arch Dermatol
Res. 304:177–184. 2012.
|