Introduction
Accounting for approximately one-quarter of all
primary osseous sarcomas, chondrosarcoma is the second most common
type of primary sarcoma of bone. Although chondrosarcoma only
occasionally originates within the lungs and bronchi, it is the
most common type of primary malignancy of the chest wall (1). Chondrosarcomas usually present with an
anterior location within the chest wall, arising from the
costochondral arches or sternum. Those tumors that arise from the
ribs occasionally manifest as intrathoracic masses with minimal
osseous involvement. Chondrosarcomas in the lungs and bronchi are
extremely rare (2). The majority of
intrathoracic chondrosarcomas manifest clinically as painless or
painful masses, and occasionally manifest as cough or chest pain.
Surgery is considered the primary treatment of chondrosarcoma,
occasionally accompanied by chemotherapy or radiation therapy
(2). The present study describes
the imaging findings of three cases of chondrosarcoma that
presented as intrathoracic masses, with the aim to recognize the
clinical and imaging features of this disease with regard to the
current literature. Patients provided written informed consent.
Case report
Case 1
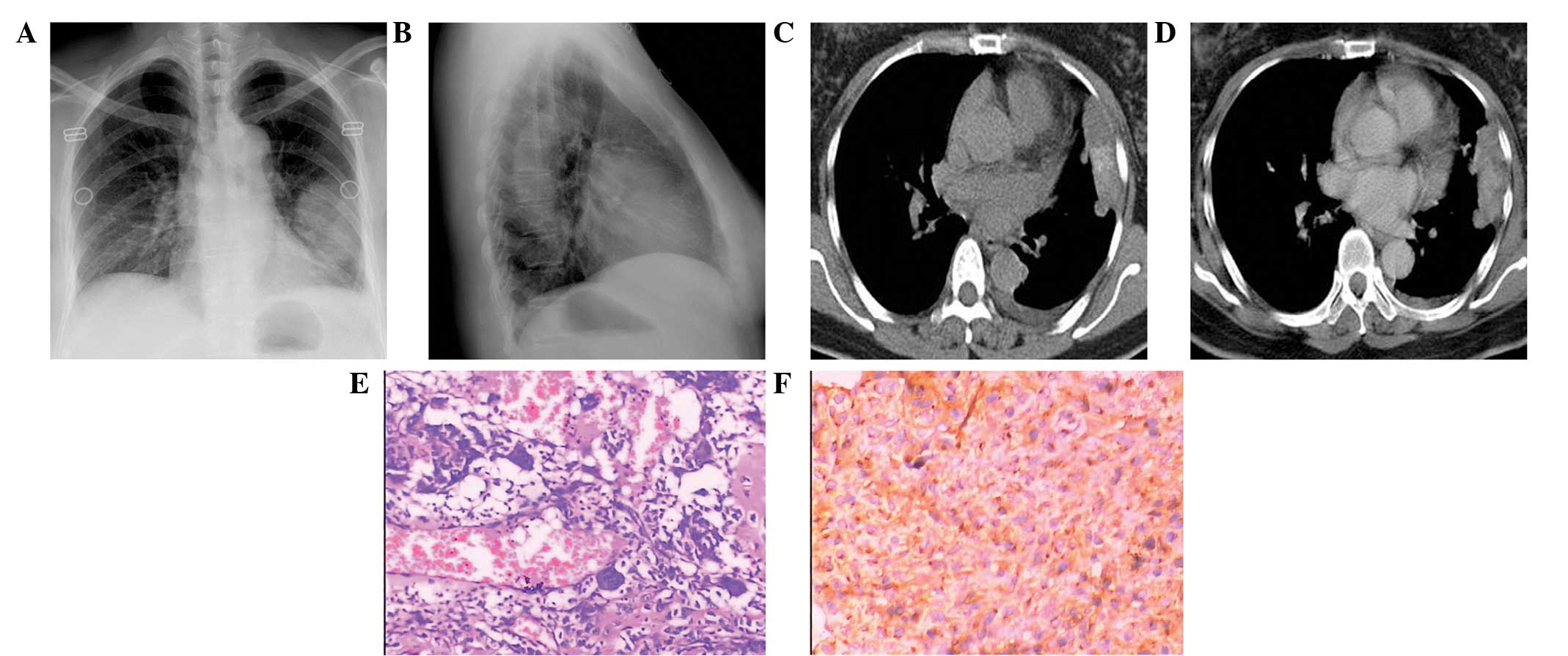
A 52-year-old female presented to the First
Affiliated Hospital of Soochow University (Suzhou, Jiangsu) with an
intermittent cough and bloody sputum that had persisted for four
months. A chest roentgenogram revealed a homogeneous, round,
well-defined shadow in the left lung (Fig. 1A and B). Computed tomography (CT)
revealed an irregular hyperdense lung mass with coarse intratumoral
calcifications in the anterior segment of the left upper lobe. Part
of the mass was closely attached to the pleura, but there was no
cartilage or bone destruction (Fig.
1C). The mass was heterogeneously enhanced upon the
administration of contrast medium (Fig.
1D). The mass was completely resected using a left thoracotomy
and was easily separated from the parietal pleura. Grossly, the
resected mass was white in color and measured 5×4×4 cm, with
necrosis at the cut surface. Two small nodules could be observed on
the surface of the pleura and diaphragm. The final pathological
diagnosis was of a dedifferentiated chondrosarcoma (Fig. 1E). Immunohistochemically, the tumor
was positive for S-100 in the cartilaginous component and cluster
of differentiation (CD)99 in the sarcomatous component (Fig. 1F), but negative for smooth muscle
actin, CD34, CD117, B-cell lymphoma-2 and cytokeratin 18. The
patient received no further therapy. To date, the patient has been
followed up for three years and is alive.
Case 2
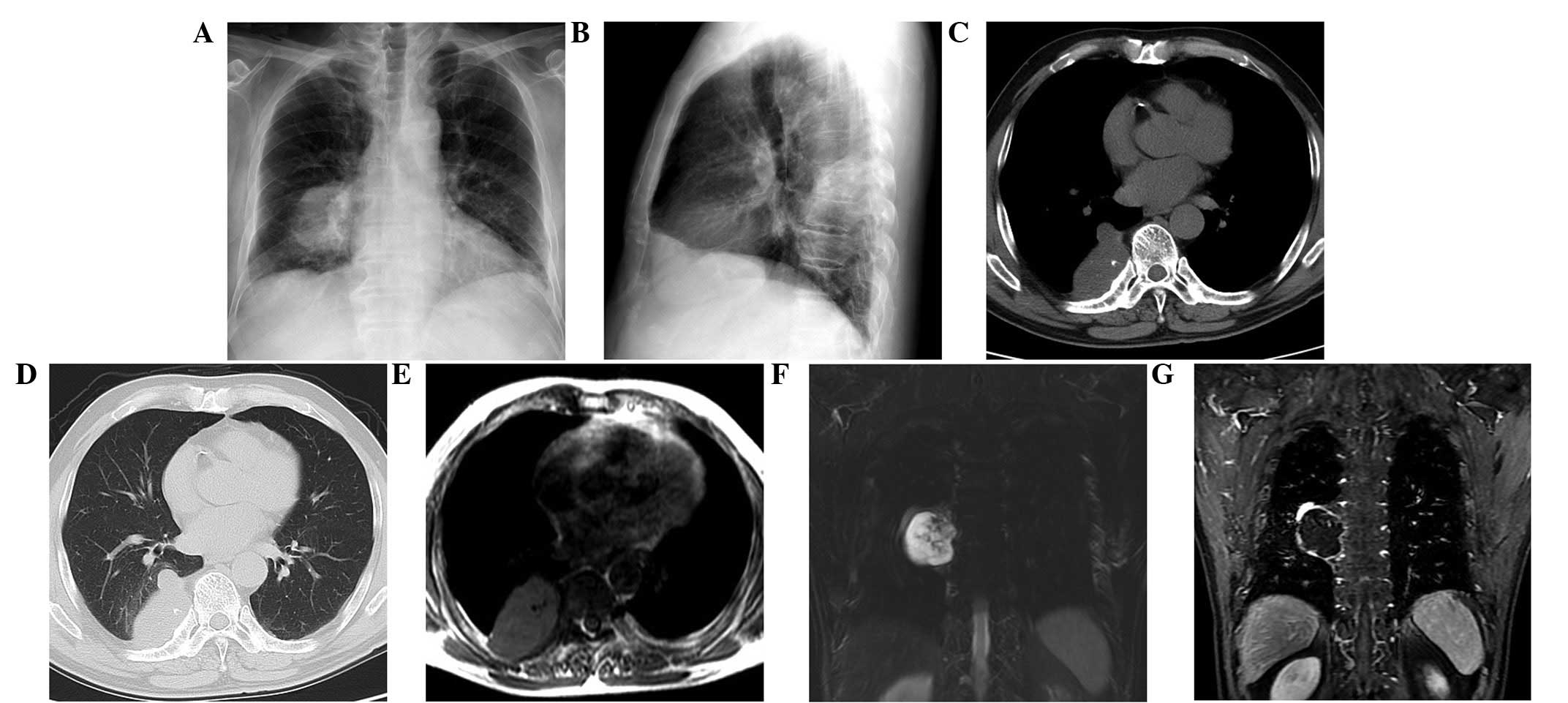
A 64-year-old male presented with a slightly
hyperdense mass with rounded boundaries on the right lower lung,
which had been incidentally diagnosed during a routine health
examination. (Fig. 2A and B). A CT
scan of the chest revealed that the mass was homogeneous and
calcified, originating from the right chest wall and protruding
into the thoracic cavity (Fig. 2C and
D). Chest magnetic resonance imaging (MRI) revealed that the
mass was slightly hypointense on the T1-weighted image (T1WI)
(Fig. 2E) and hyperintense on the
T2WI (Fig. 2F), with an enhanced
periphery following the administration of intravenous contrast
medium (Fig. 2G). The calcification
was found to be hypointense on the T1- and T2WIs. A right
thoracotomy revealed a mass on the inner surface of the right
seventh rib that did not adhere to the lung parenchyma. The mass
was completely excised and measured 3×4×4 cm. Grossly, the mass
consisted of cyst fluid, gel-like tissue and a small quantity of
cartilage tissue. Histopathological examination indicated that the
mass was a grade 1 chondrosarcoma. Staining for S-100 and Ki-67 was
positive, but staining for smooth muscle actin, desmin, vimentin
and p53 was negative. The patient received standard radiotherapy
(total of 50 Gy; 2 Gy per fraction) during the two years of
follow-up and is alive at the time of writing.
Case 3
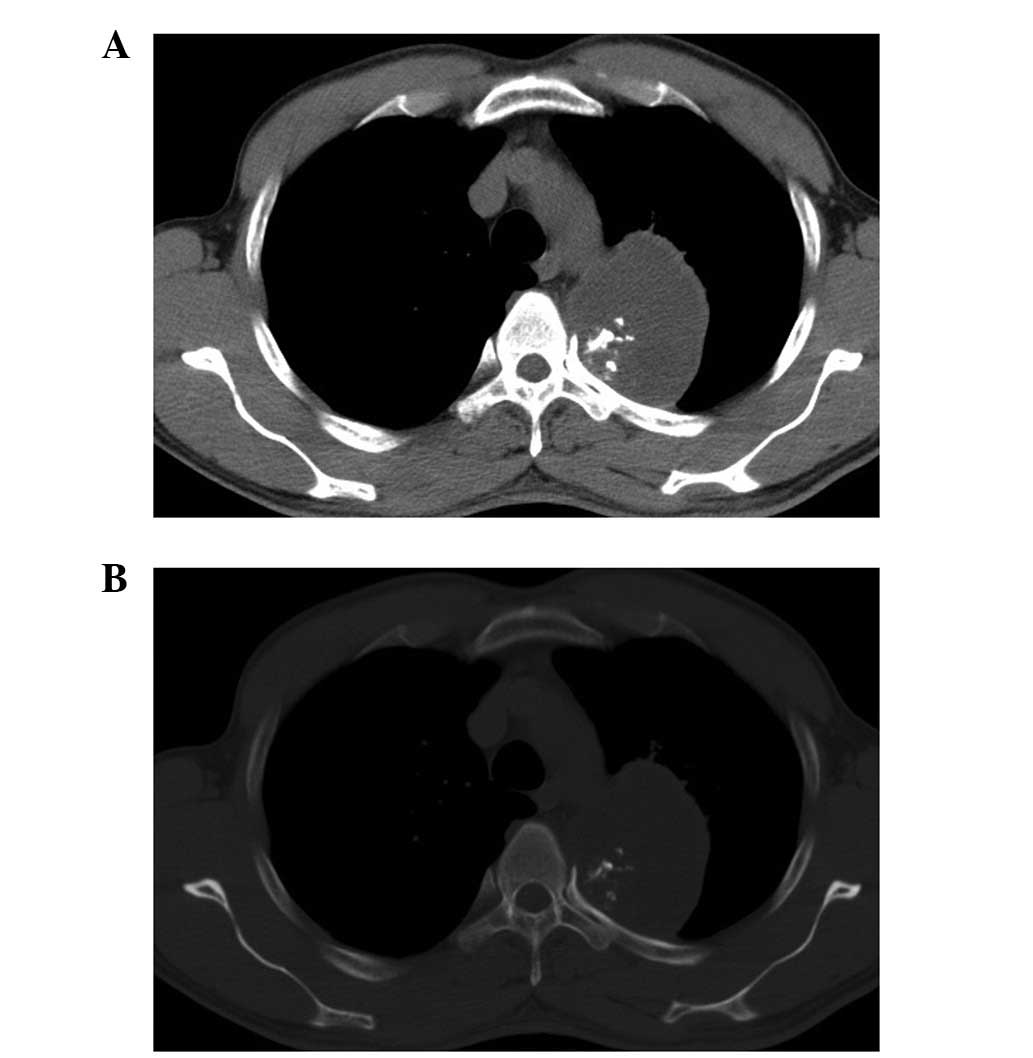
A 45-year-old male presented with a round mass on
the left lung. The mass was homogeneously hypodense (near the
density of water) and 6×5 cm in size on CT images (Fig. 3). The mass protruded into the
thoracic cavity and there was a certain amount of bony destruction
to the left fourth rib. Furthermore, the left upper lung was
compressed. A left thoracotomy was performed and the mass was found
to be adhered to the left fourth rib, with a wide base and areas of
cartilage in the basilar section. Histopathological examination
showed that the lesion was a grade 1 chondrosarcoma. The patient
received no further treatment and is alive after three years of
follow-up.
Discussion
Primary chest chondrosarcomas, including those
arising from the chest wall (bone, muscle and pleura) and lungs or
bronchi, are uncommon (3). Primary
pulmonary chondrosarcoma is extremely rare, with strict diagnositc
criteria (4,5). The majority of chondrosarcomas arising
from the chest wall appear as soft-tissue masses within the chest
wall (2). Tumors presenting as
intrathoracic masses are observed in certain cases of primary chest
wall chondrosarcoma and all cases of primary pulmonary
chondrosarcoma. The present study reported three cases of
chondrosarcoma that presented as intrathoracic masses (1). None of the cases could be diagnosed as
primary pulmonary chondrosarcoma based on the diagnostic criteria
(4). However, they were considered
to be primary intrathoracic chondrosarcoma due to the absence of a
clinical history and other lesions.
The natural history of primary intrathoracic
chondrosarcoma is similar to that of skeletal chondrosarcoma.
Chondrosarcomas usually occur in individuals >30 years old, with
a male predominance (1). Patients
may be symptom-free during the initial phase when the
chondrosarcoma grows slowly. The most common symptoms of
intrathoracic chondrosarcoma include a non-productive cough, chest
pain, dyspnoea and hemoptysis (5–8). The
tumors are often locally invasive and have a high rate of
recurrence (5,9).
The imaging features of primary intrathoracic
chondrosarcoma resemble those of skeletal chondrosarcoma. CT
imaging of primary intrathoracic chondrosarcoma often reveals a
large soft-tissue mass with heterogeneous calcification and
occasional destruction of the adjacent bone (5,6,8,10–12).
Intratumoral calcification is one of the characteristic imaging
findings of chondrosarcoma and may be an important indicator for
diagnosis (13). The MRI features
of chondrosarcoma show as isointense on the T1WI and hyperintense
on the T2WI (12,13). However, in the present case,
calcification was revealed as hypointense on the T1- and T2WIs.
Atelectasis or obstructive inflammation may present when the
bronchus is obstructed by the mass. Pleural effusion may be
performed if the pleura is involved (14). Significant invasion to the pulmonary
arteries has been reported (15).
Atypical imaging features are found in certain cases and may
mislead the diagnosis. Intratumoral necrosis or cystic degeneration
has also been found in certain cases (6,14).
Parker et al (12) reported
a case of primary pulmonary chondrosarcoma with CT and MRI features
mimicking a bronchogenic cyst.
Primary intrathoracic chondrosarcomas are usually
indistinguishable using imaging methods. Primary intrathoracic
chondrosarcomas should be differentiated from calcified pulmonary
lesions, including pulmonary hamartoma (PH), primary lung cancer
and other intrathoracic sarcomas (3,13). PH
is the most benign lung tumor, with a relatively small size
(diameter of ≤4 cm on chest radiograph or ≤2.5 cm on CT). The
finding of fat and calcification together is diagnostic, as the
tumor is composed of fat, epithelial tissue, fibrous tissue and
cartilage. Furthermore, an air cleft on the side or the inside is
characteristic of pulmonary hypertension. It is necessary to
regularly follow-up hamartoma-like lesions, as chondrosarcoma may
develop from persistent hamartomas (16). Primary lung cancer may present with
calcification of various patterns as a result of a secretary
function of the carcinoma, chemotherapy or hypercalcemia. Although
calcification within lung cancer is rare, it is difficult to
differentiate intrathoracic chondrosarcoma from primary lung cancer
when intratumoral calcification is found. Primary intrathoracic
chondrosarcomas are difficult to differentiate from other sarcomas,
including Ewing’s sarcoma, primitive neuroectodermal tumors and
osteosarcomas, if the diagnosis depends only on the imaging
technique. An accurate diagnosis is possible by combining the
imaging findings with the clinical presentation. For example,
Ewing’s sarcoma and osteosarcoma often occur in young individuals
<30 years old; however, chondrosarcomas occur in adults >30
years old.
In conclusion, primary intrathoracic chondrosarcoma
is a rare, malignant tumor that originates from the chest and may
involve the chest wall, lungs or bronchi. Radiologically, primary
intrathoracic chondrosarcomas usually occur as large masses with
intratumoral calcification. Although histological analysis is
always required for a definite diagnosis, imaging is important for
analyzing the tumor. It may also be useful to pay careful attention
to the imaging features of the tumor and its clinical
manifestations for the diagnosis.
Acknowledgements
The present study was supported by a grant from the
National Natural Science Foundation of China (grant no.
31271066).
References
|
1
|
Gladish GW, Sabloff BM, Munden RF, et al:
Primary thoracic sarcomas. Radiographics. 22:621–637. 2002.
|
|
2
|
Foran P, Colleran G, Madewell J and
O’Sullivan PJ: Imaging of thoracic sarcomas of the chest wall,
pleura, and lung. Semin Ultrasound CT MR. 32:365–376. 2011.
|
|
3
|
Khan AN, Al-Jahdali HH, Allen CM, et al:
The calcified lung nodule: What does it mean? Ann Thorac Med.
5:67–79. 2010.
|
|
4
|
Zhan ZL: Primary chondrosarcoma of the
lung. Zhonghua Zhong Liu Za Zhi. 14:447–448. 1992.(In Chinese).
|
|
5
|
Shah ND and Diwanji SR: Primary
chondrosarcoma of the lung with cutaneous and skeletal metastases.
Singapore Med J. 48:e196–e199. 2007.
|
|
6
|
Yellin A, Schwartz L, Hersho E and
Lieberman Y: Chondrosarcoma of the bronchus. Chest. 84:224–226.
1983.
|
|
7
|
Kalhor N, Suster S and Moran CA: Primary
pulmonary chondrosarcomas: a clinicopathologic study of 4 cases.
Hum Pathol. 42:1629–1634. 2011.
|
|
8
|
Karapolat S: Lung images: chondrosarcoma
on the chest wall. Lung. 187:141–142. 2009.
|
|
9
|
Kurotaki H, Tateoka H, Takeuchi M, et al:
Primary mesenchymal chondrosarcoma of the lung. A case report with
immunohistochemical and ultrastructural studies. Acta Pathol Jpn.
42:364–371. 1992.
|
|
10
|
Huang HY, Hsieh MJ, Chen WJ, et al:
Primary mesenchymal chondrosarcoma of the lung. Ann Thorac Surg.
73:1960–1962. 2002.
|
|
11
|
Rees GM: Primary chondrosarcoma of lung.
Thorax. 25:366–371. 1970.
|
|
12
|
Parker LA, Molina PL, Bignault AG and
Fidler ME: Primary pulmonary chondrosarcoma mimicking bronchogenic
cyst on CT and MRI. Clin Imaging. 20:181–183. 1996.
|
|
13
|
O’Sullivan P, O’Dwyer H, Flint J, Munk PL
and Muller NL: Malignant chest wall neoplasms of bone and
cartilage: a pictorial review of CT and MR findings. Br J Radiol.
80:678–684. 2007.
|
|
14
|
Boueiz A, Abougergi MS, Noujeim C, et al:
Primary dedifferentiated chondrosarcoma of the lung. South Med J.
102:861–863. 2009.
|
|
15
|
Sun CC, Kroll M and Miller JE: Primary
chondrosarcoma of the lung. Cancer. 50:1864–1866. 1982.
|
|
16
|
Jazy FK, Cormier WJ, Panke TW, Shehata WM
and Amongero FJ: Primary chondrosarcoma of the lung. A report of
two cases. Clin Oncol. 10:273–279. 1984.
|