Introduction
Hepatocellular carcinoma (HCC) is one of the most
common types of malignant tumor and is the third leading cause of
cancer-related mortality worldwide (1). The global distribution of HCC is
disproportional, with the highest incidence reported in Asia and
Sub-Saharan Africa, particularly in China. HCC patients exhibit an
overall 5-year survival rate of only 5% (2). In total, ~70% of patients experience
relapse within five years of undergoing surgery and >80% of
recurrences are within the remaining liver tissue (3,4).
Patients with HCC often exhibit different outcomes, even when
identical clinicopathological features are observed; this suggests
that the development and rapid progression of HCC involves numerous
complex molecular and cellular events. Therefore, in order to
develop novel prognostic factors and improve treatment options, the
elucidation of the molecular mechanisms involved in tumor
progression and identification of the crucial markers that
discriminate between the occurrence and the various stages of HCC
is imperative (5).
The stanniocalcin 2 (STC2) protein, encoded by the
STC2 gene, is a 32-kDa extracellular matrix protein with a
signaling peptide; the protein is involved in a number of
physiological processes, including bone development, reproduction,
wound healing, angiogenesis and modulation of the inflammatory
response (6). The majority of the
current research is focused on cellular inflammation and
carcinogenesis, due to the increasing evidence demonstrating the
local actions of STCs (7). Previous
studies have reported that various cancers, including renal cell
carcinoma (8) and breast cancer
(9) have exhibited increased
expression of STC2; however, the clinical significance of STC2 in
HCC remains to be investigated. Therefore, the current study aimed
to explore the STC2 expression levels in HCC tissues and the
correlation with prognosis.
Materials and methods
Patients and tissue samples
A total of 30 fresh HCC cancerous tissues and paired
adjacent non-cancerous tissues were obtained from HCC carcinoma
patients, who had undergone hepatectomy in 2012 at the Department
of Hepatobiliary Surgery, Shandong Provincial Hospital Affiliated
to Shandong University (Jinan, China). The histological diagnosis
of HCC was confirmed by two independent pathologists, and these
paired tissue samples were utilized for the western blot analysis
of STC2 expression. The fresh tissue was surgically removed,
immediately frozen and stored in liquid nitrogen. Additionally,
paraffin-embedded, paired cancer tissue and adjacent normal tissue
samples, which had been obtained from 240 HCC patients at Shandong
Provincial Hospital Affiliated to Shandong University between 2005
and 2008, were utilized for the immunohistochemical analysis of
STC2 expression.
The follow-up results for the 240 patients enrolled
in this study were obtained according to medical records and
telephone interviews. Postoperative follow-up was performed on HCC
patients every three months during the initial two years, every six
months during the third to fifth year, and annually thereafter, for
an additional five years or until mortality. Overall survival (OS)
was defined as the time from surgery to patient mortality or the
last follow-up. Disease-free survival (DFS) was defined as the time
from surgery to disease recurrence or metastasis. The study was
approved by the Institutional Ethics Board of Shandong Provincial
Hospital Affiliated to Shandong University, and informed consent
was obtained from all participants.
Western blot analysis
Western blot analysis was performed to detect the
expression of STC2 in the 30 resected HCC specimens. Frozen HCC
specimens were ground in liquid nitrogen and harvested. Tissue
samples were lysed in RIPA lysis buffer [phosphate-buffered saline
(PBS) containing 1% Triton X-100 and 1 nM phenylmethylsulfonyl
fluoride] at 4°C for 30 min and subjected to centrifugation at
12,000 × g for 15 min. The protein concentration was quantified
using the BCA protein assay (Pierce Biotechnology Inc., Rockford,
IL, USA). Equal quantities of protein (50 μg) were loaded and
SDS-PAGE was completed on a 12% SDS-PAGE gel, which was then
transferred to nitrocellulose membrane. The membrane was incubated
for 60 min in PBS containing 0.1% Tween-20 and 5% skimmed milk to
block any nonspecific binding. This was followed by incubation at
4°C with monoclonal rabbit anti-human STC2 antibody (1:1000
dilution; Abcam, Cambridge, MA, USA). The membrane was washed three
times for 10 min in PBS with 0.1% Tween-20 and subsequently
incubated for 1 h with horseradish peroxidase-conjugated bovine
monoclonal anti-rabbit (1:5000 dilution) secondary antibody (Boster
Biological Technology Ltd., Wuhan, China) at room temperature. The
immumoreactive proteins were then detected using ECL substrate (ECL
western blotting detection system; Amersham Pharmacia Biotech,
Amersham, UK) according to the manufacturer’s instructions. GAPDH
was used as an endogenous protein for normalization. The relative
intensity of each lane was quantified by scanning densitometry
using Quantity One software (Bio-Rad, Hercules, CA, USA).
Immunohistochemistry (IHC)
Paraffin-embedded HCC or non-cancerous tissues were
assessed using immunohistochemical analysis (n=240). The slides
were immersed in EDTA (pH 8.0) and boiled for 10 min in a microwave
oven for the antigen retrieval. Following three rinses with PBS,
the endogenous peroxidase was blocked with 0.3% hydrogen peroxide
for 20 min at room temperature. The slides were incubated with the
monoclonal mouse anti-rabbit STC2 antibody (1:50 dilution; Abcam,
Cambridge, United Kingdom) in a humidified chamber at 4°C
overnight. Following additional wash with PBS for three times, the
sections were sequentially incubated with horseradish
peroxidase-conjugated secondary antibody (Abcam) at 37°C for 30 min
and subsequently washed three times with PBS. Finally,
diaminobenzidine tetrahydrochloride was used for the signal
development and PBS was used as the negative control.
The total STC2 immunostaining scores were calculated
as the product of the percentage positivity of the stained tumor
cells and the staining intensity (10). The percentage positivity was scored
as 0, <5% staining (negative); 1, ≥5 to <25% staining; 2,
≥25to <50% staining; 3, ≥50 to <75% staining; and 4, ≥75%
staining. A staining intensity score of 0, no staining; 1, mild; 2,
moderate; or 3, strong was allocated. The percentage positivity of
cells and staining intensity were determined under double-blind
conditions. The STC2 immunostaining score was calculated as the
product of the value of the percentage positivity score plus the
staining intensity score, ranging from 0 to 12. The STC2 expression
level was defined as the following: −, score of 0–3; +, score of
4–6; ++, score of 7–9; and +++, score of ≥10. Based on these STC2
expression levels, the HCC patients were divided into two groups:
negative STC2 expression (− and +) and positive STC2 expression (++
and +++).
Statistical analysis
The SPSS software, version 15.0 (SPSS, Inc.,
Chicago, IL, USA) was used for statistical analysis. The χ2 test
was used to show the differences in categorical variables. Patient
survival and the differences in patient survival were determined by
the Kaplan-Meier method and the log-rank test, respectively. A Cox
regression analysis (proportional hazard model) was performed for
the multivariate analyses of prognostic factors. P<0.05 was
considered to indicate a statistically significant difference.
Results
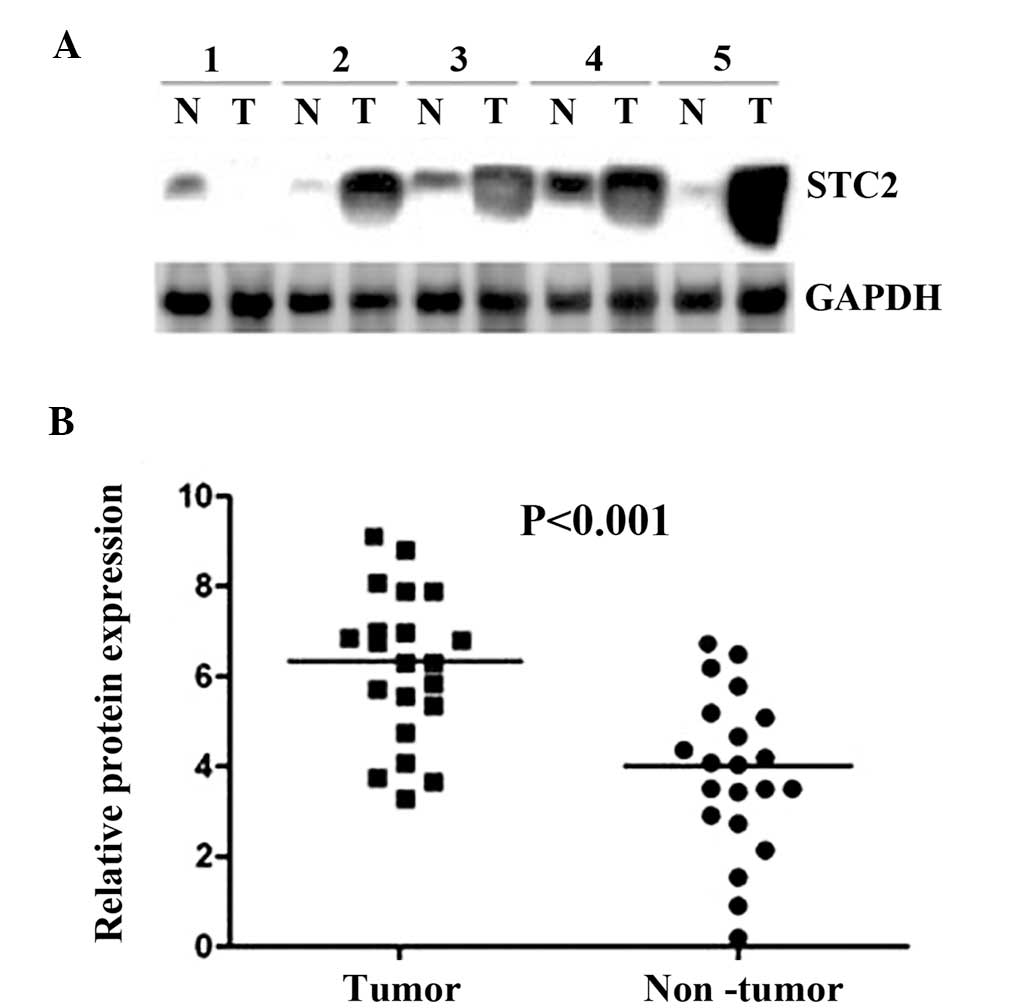
Upregulation of STC2 in HCC tissues by
western blot analysis
Initially, the expression levels of STC2 protein
were analyzed using western blot analysis on 30 HCC cancerous
tissues and the paired corresponding adjacent non-cancerous
tissues. The western blot analysis revealed that STC2 expression
was markedly increased in HCC cancerous tissues, compared with the
corresponding non-cancerous tissues (P<0.001; Fig. 1).
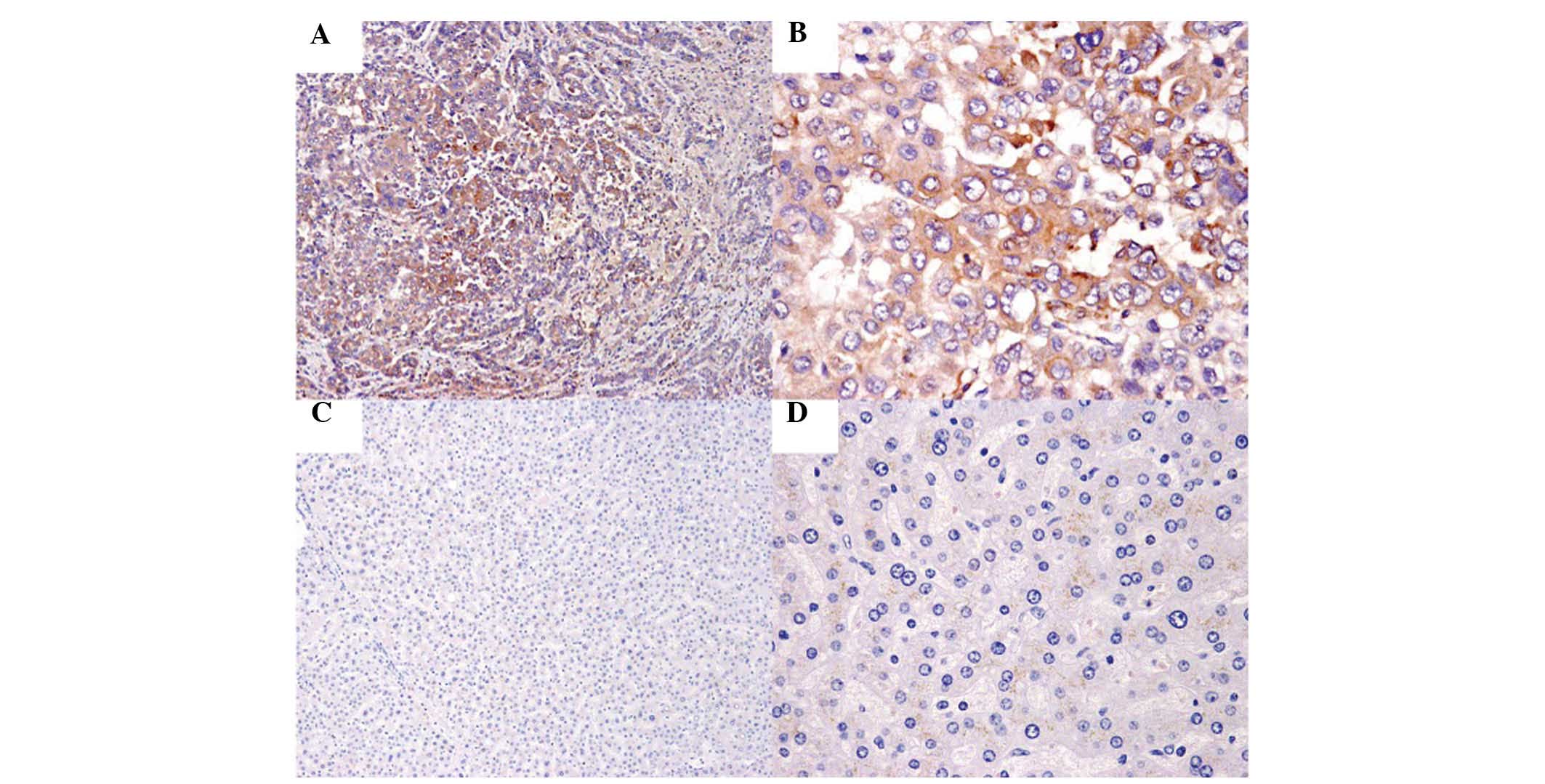
STC2 expression correlates with
clinicopathological features in HCC
The correlation between STC2 expression and
clinicopathological features in HCC was explored using IHC,
performed in 240 HCC tissue samples and the paired adjacent normal
tissue samples (Fig. 2). Among the
tissue samples, 60.83% (146/240) of HCC cancerous specimens
exhibited positive expression of STC2. However, STC2 expression was
observed to be positive only in 8.75% (21/240) paired adjacent
non-cancerous liver specimens. The associations between STC2
expression and the clinicopathological features are shown in
Table I. STC2 expression was
significantly correlated with serum α-fetoprotein (AFP) levels
(P=0.024), recurrence (P=0.011) and metastasis (P=0.025). No
statistically significant correlations were identified between the
STC2 expression and the remaining clinicopathological features.
 | Table ICorrelations of STC2 expression with
clinicopathologic features of hepatocellular carcinoma. |
Table I
Correlations of STC2 expression with
clinicopathologic features of hepatocellular carcinoma.
| | STC2 expression | |
|---|
| |
| |
|---|
| Clinicopathologic
variables | Cases, n | Negative | Positive | P-valuea |
|---|
| Gender | | | | 0.410 |
| Male | 198 | 80 | 118 | |
| Female | 42 | 14 | 28 | |
| Age, years | | | | 0.390 |
| ≤60 | 191 | 82 | 109 | |
| >60 | 49 | 12 | 37 | |
| Liver cirrhosis | | | | 0.520 |
| Yes | 171 | 54 | 117 | |
| No | 69 | 40 | 29 | |
| Serum AFP, μg/l | | | | 0.024 |
| ≥400 | 127 | 36 | 91 | |
| <400 | 113 | 58 | 55 | |
| Histological
differentiation | | | | 0.260 |
| Well | 67 | 31 | 36 | |
| Moderate | 71 | 11 | 60 | |
| Poor | 102 | 52 | 50 | |
| Recurrence | | | | 0.007 |
| Present | 167 | 52 | 115 | |
| Absent | 73 | 42 | 31 | |
| Metastasis | | | | 0.025 |
| Present | 162 | 53 | 109 | |
| Absent | 78 | 41 | 37 | |
Correlation between STC2 expression and
patient survival
The prognostic value of STC2 expression in HCC
patients was also evaluated between those with positive and
negative expression of STC2. Kaplan-Meier curve analysis indicated
that positive expression of STC2 was significantly correlated with
poor clinical outcome of HCC patients. HCC patients with positive
STC2 expression exhibited significantly shortened OS and DFS,
compared with those with negative STC2 expression (Fig. 3). Multivariate analysis was
conducted to investigate the impact of the STC2 expression pattern
on the clinicopathological features of HCC patients. Univariate
analysis indicated that STC2 expression was a significant
prognostic factor for OS (Table
II). Based on the multivariate analysis, STC2, metastasis and
recurrence where independent prognostic factors for OS. Therefore,
STC2 expression may be significant in predicting the OS in HCC
patients (hazard ratio, 2.39; 95% confidence interval, 1.04–5.89;
P=0.013; Table II).
| Table IIUnivariate and multivariate analysis
of overall survival in 240 hepatocellular carcinoma patients. |
Table II
Univariate and multivariate analysis
of overall survival in 240 hepatocellular carcinoma patients.
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|---|
| Variables | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| STC2 | 3.01 | 1.29–6.75 | <0.001 | 2.39 | 1.04–5.89 | 0.013 |
| Gender | 0.65 | 0.28–1.52 | 0.33 | - | - | - |
| Age | 0.81 | 0.48–1.37 | 0.44 | - | - | - |
| Tumor size | 1.19 | 0.73–2.23 | 0.51 | - | - | - |
| Histology | 1.20 | 0.66–1.56 | 0.061 | - | - | - |
| Cirrhosis | 0.78 | 0.52–1.11 | 0.22 | - | - | - |
| HBsAg | 1.32 | 0.42–2.27 | 0.74 | - | - | - |
| Serum AFP | 1.59 | 0.92–2.74 | 0.09 | - | - | - |
| Metastasis | 1.49 | 1.13–2.43 | 0.019 | 1.21 | 0.88–2.93 | 0.035 |
| Recurrence | 1.60 | 1.06–2.56 | 0.011 | 1.33 | 0.88–3.50 | 0.020 |
Discussion
Although the number of novel treatment strategies
under development for HCC is currently increasing, including
options such as molecular targeted therapy (11), gene therapy (12) and immunotherapy (13), the therapeutic outcomes remain
unsatisfactory, and the survival rate of HCC is low (14). Therefore, the identification of new
prognostic markers for the prevention and treatment of HCC is an
ongoing challenge.
Overexpression of STC2 has been demonstrated to
contribute to poor prognosis or recurrence in colorectal (15), gastric (16) and prostate (17) cancer, as well as neuroblastoma
(18) and renal cell carcinoma
(8). In ER-positive breast cancers,
however, STC2 overexpression has been found to indicate a good
prognosis (19,20). This variation between reports
suggests that the contribution of STC2 to the development of
carcinoma is likely to depend on the cancer type.
Elucidating the underlying mechanism of STC2 in HCC
is an ongoing challenge. A recent study demonstrated that the
proliferative capacity of a gastric cancer cell line was inhibited
by treatment with STC2 siRNA. Furthermore, the authors proposed
that STC2 may contribute to cancer development and poor prognosis
by controlling proliferation in gastric cancer (21). A number of reports have suggested
that cells expressing STC2 exhibit resistance to apoptosis. Ito
et al (22) reported that
STC2 expression contributes to antiapoptotic activity and survival
of ischemia nerve cells. Furthermore, STC2 was revealed to protect
cells from apoptosis in hypoxic ovarian cancer cell lines (23). Conversely, breast cancer cases
exhibiting late relapse were observed to overexpress STC2 in the
primary and recurrence sites (24).
A previous study has demonstrated that STC2 is highly expressed in
tumor vascular endothelial cells, and that this overexpression
correlates with postoperative recurrences (25). These observations indicate that STC2
expression in cancer samples may contribute to the development of
carcinoma through the host vascular endothelial cells, as well as
cancer cells.
In the current study, the STC2 protein levels in HCC
and tumor-adjacent non-cancerous tissues were evaluated using
western blot analysis and IHC. These analyses indicated that STC2
was highly expressed in HCC compared with the corresponding
non-cancerous tissues. Furthermore, positive expression of STC2 in
HCC was observed to correlate with certain aggressive
clinicopathological characteristics, including AFP levels,
recurrence and metastasis in the 240 paraffin-embedded paired
tissue specimens. The results from the current study also imply
that positive STC2 expression was associated with poor prognosis;
STC2 positive expression correlated with OS and DFS in the 240 HCC
patients. Notably, STC2 was observed to be an independent
prognostic factor in these HCC patients.
In summary, the current study reports the
differential expression of STC2 in HCC and the possible use of STC2
as a novel prognostic marker in HCC. The present findings
demonstrate that the high expression of STC2 in HCC tissue is
associated with poor prognosis in HCC patients. Further studies are
required to explore and elucidate the underlying mechanisms of STC2
in HCC. STC2 expression may present a useful prognostic marker in
HCC patients.
Acknowledgements
This study was supported by the Natural Science
Foundation of Shandong Province, China (grant no. ZR2012HM079).
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108.
2005.
|
|
2
|
Forner A, Llovet JM and Bruix J:
Hepatocellular carcinoma. Lancet. 379:1245–1255. 2012.
|
|
3
|
Sherman M: Recurrence of hepatocellular
carcinoma. N Engl J Med. 359:2045–2047. 2008.
|
|
4
|
Thorgeirsson SS and Grisham JW: Molecular
pathogenesis of human hepatocellular carcinoma. Nat Genet.
31:339–346. 2002.
|
|
5
|
Tsai CL, Koong AC, Hsu FM, et al:
Biomarker studies on radiotherapy to hepatocellular carcinoma.
Oncology. 84:64–68. 2013.
|
|
6
|
Jellinek DA, Chang AC, Larsen MR, et al:
Stanniocalcin 1 and 2 are secreted as phosphoproteins from human
fibrosarcoma cells. Biochem J. 350:453–461. 2000.
|
|
7
|
Yeung BH, Law AY and Wong CK: Evolution
and roles of stanniocalcin. Mol Cell Endocrinol. 349:272–280.
2012.
|
|
8
|
Meyer HA, Tölle A, Jung M, et al:
Identification of stanniocalcin 2 as prognostic marker in renal
cell carcinoma. Eur Urol. 55:669–678. 2009.
|
|
9
|
Esseghir S, Kennedy A, Seedhar P, et al:
Identification of NTN4, TRA1, and STC2 as prognostic markers in
breast cancer in a screen for signal sequence encoding proteins.
Clin Cancer Res. 13:3164–3173. 2007.
|
|
10
|
Almeida M, Muñoz J, Nunes S and
Fonseca-Moutinho J: Cyclooxygenase-2 immunoexpression in breast
cancer: progesterone receptor influence. Cancer Epidemiol.
35:e81–e84. 2011.
|
|
11
|
Tazi el M, Essadi I, M’rabti H, Touyar A
and Errihani PH: Systemic treatment and targeted therapy in
patients with advanced hepatocellular carcinoma. N Am J Med Sci.
3:167–175. 2011.
|
|
12
|
Qu L, Wang Y, Gong L, et al: Suicide gene
therapy for hepatocellular carcinoma cells by survivin
promoter-driven expression of the herpes simplex virus thymidine
kinase gene. Oncol Rep. 29:1435–1440. 2013.
|
|
13
|
Tada F, Abe M, Hirooka M, et al: Phase
I/II study of immunotherapy using tumor antigen-pulsed dendritic
cells in patients with hepatocellular carcinoma. Int J Oncol.
41:1601–1609. 2012.
|
|
14
|
Xie B, Zhou J, Yuan L, et al: Epigenetic
silencing of Klotho expression correlates with poor prognosis of
human hepatocellular carcinoma. Hum Pathol. 44:795–801. 2013.
|
|
15
|
Ieta K, Tanaka F, Yokobori T, et al:
Clinicopathological significance of stanniocalcin 2 gene expression
in colorectal cancer. Int J Cancer. 125:926–931. 2009.
|
|
16
|
Yokobori T, Mimori K, Ishii H, et al:
Clinical significance of stanniocalcin 2 as a prognostic marker in
gastric cancer. Ann Surg Oncol. 17:2601–2607. 2010.
|
|
17
|
Tamura K, Furihata M, Chung SY, et al:
Stanniocalcin 2 overexpression in castration-resistant prostate
cancer and aggressive prostate cancer. Cancer Sci. 100:914–919.
2009.
|
|
18
|
Volland S, Kugler W, Schweigerer L,
Wilting J and Becker J: Stanniocalcin 2 promotes invasion and is
associated with metastatic stages in neuroblastoma. Int J Cancer.
125:2049–2057. 2009.
|
|
19
|
Bouras T, Southey MC, Chang AC, et al:
Stanniocalcin 2 is an estrogen-responsive gene coexpressed with the
estrogen receptor in human breast cancer. Cancer Res. 62:1289–1295.
2002.
|
|
20
|
Esseghir S, Kennedy A, Seedhar P, et al:
Identification of NTN4, TRA1, and STC2 as prognostic markers in
breast cancer in a screen for signal sequence encoding proteins.
Clin Cancer Res. 13:3164–3173. 2007.
|
|
21
|
Arigami T, Uenosono Y, Ishigami S,
Yanagita S, Hagihara T, Haraguchi N, Matsushita D, Hirahara T, et
al: Clinical significance of stanniocalcin 2 expression as a
predictor of tumor progression in gastric cancer. Oncol Rep.
30:2838–2844. 2013.
|
|
22
|
Ito D, Walker JR, Thompson CS, et al:
Characterization of stanniocalcin 2, a novel target of the
mammalian unfolded protein response with cytoprotective properties.
Mol Cell Biol. 24:9456–9469. 2004.
|
|
23
|
Law AY and Wong CK: Stanniocalcin-2 is a
HIF-1 target gene that promotes cell proliferation in hypoxia. Exp
Cell Res. 316:466–476. 2010.
|
|
24
|
Joensuu K, Heikkilä P and Andersson LC:
Tumor dormancy: elevated expression of stanniocalcins in late
relapsing breast cancer. Cancer Lett. 265:76–83. 2008.
|
|
25
|
Buckanovich RJ, Sasaroli D,
O’Brien-Jenkins A, Botbyl J, Hammond R, Katsaros D, Sandaltzopoulos
R, Liotta LA, Gimotty PA and Coukos G: Tumor vascular proteins as
biomarkers in ovarian cancer. J Clin Oncol. 25:852–861. 2007.
|