Introduction
Renal cell carcinomas (RCCs) account for 2–3% of all
types of cancer worldwide and the highest incidence rate is
observed in developed countries. The disease is more common in
males, with a male to female ratio of 1.5:1, and the highest
incidence is observed between the ages of 60 and 70 years (1). Furthermore, the five-year survival
rate of RCC is 68.4% and the worldwide incidence rate increases by
2% annually (2). RCCs can
metastasize to almost every organ, including the lungs (50–60%),
liver (30–40%), bones (30–40%) and brain (5%), and ~25% of RCC
patients will already have multiple distant metastases at the time
of presentation, such as lung, lymph node, liver or bone metastases
(3). The rate of ipsilateral
adrenal metastasis from RCC ranges from 1.1 to 10% in RCC patients
and increases to 6–29% in autopsy series (4,5). By
contrast, contralateral adrenal metastases rarely occur (metastasis
rate, ~0.7%) and bilateral adrenal metastases are limited to ~20
cases reported in the literature (4). Bilateral adrenal metastases may occur
as synchronous or metachronous lesions; however, the management of
synchronous adrenal metastases is considerably more challenging. In
the majority of RCC metastasis cases, removal of the metastatic
mass contributes to the rate of survival; however, bilateral
adrenalectomy may expose the patient to novel endocrinological
complications, such as the development of iatrogenic Addison’s
disease. Therefore, minimally invasive surgical procedures and
partial adrenalectomy, in addition to radical nephrectomy, should
be the preferred treatment strategy for bilateral synchronous
adrenal metastasis from RCC. In the current case, preservation of
the right adrenal gland was considered to be more feasible due to
the size of the metastatic lesion. Therefore, right partial
adrenalectomy was preferred to left partial adrenalectomy during
the planning of the surgical procedure. Written informed consent
was obtained from the patient, and all procedures were followed in
accordance with the ethical standards of the Committee on Human
Experimentation, World Medical Association (Izmir, Turkey) and the
Declaration of Helsinki 1975, as revised in 2000.
Case report
Clinical and radiological features
In April 2014, a 50-year-old male patient was
admitted to Basmane Hospital of Sifa University (Basmane, Turkey),
presenting with right flank pain. Ultrasonography (US) revealed an
80×81×57-mm mass (Figs. 1 and
2) located in the lower pole of the
right kidney with solid-cystic components and heterogeneous
echogenicity. Computerized tomography (CT) scans identified a
primary mass in the lower pole of the right kidney measuring
86×83×66 mm and the left adrenal metastatic mass (Fig. 1), which extended to the posterior
pararenal area in the inferior region, and to the renal pelvis and
hilus in the superior region. Furthermore, the metastatic right
renal mass demonstrated marked central contrast uptake in the
arterial phase. Additionally, two metastatic masses, measuring
69×51×53 mm and 18×12×10 mm, were detected in the left (Fig. 3) and right adrenal gland (Fig. 2), respectively, with central
necrosis and peripheral contrast uptake.
Serum adrenocorticotropic hormone (ACTH; 12 pg/ml;
normal range, 9–52 pg/ml), cortisol [19 μg/dl; normal range
(morning), 7–28 μg/dl; normal range (afternoon), 2–18 μg/dl],
urinary hydroxymandelic acid (HMA; 253 mg/l; normal range, 21.7±3.2
kg/m2) and vanillylmandelic acid (VMA; 3 mg/24 h; normal
range, 2–7 mg/24 h) levels were within normal ranges; therefore,
the mass was considered to be hormonally inactive. Additionally,
biochemical tests were conducted and the results were as follows:
Glucose, 90 mg/dl; creatinine, 1.1 mg/dl; urea, 42 mg/dl; white
blood cells, 8.2×103/μl; hemoglobin, 13.9 g/dl; and
platelet count, 185,000. Mineralocorticoid and glucocorticoid
replacement therapy were administered to reduce the risk of
developing iatrogenic Addison’s disease. The patient subsequently
underwent US-guided biopsy on the renal mass, as well as right
radical nephrectomy, right partial adrenalectomy (with frozen
section examination) and left adrenalectomy. Postoperatively,
cortisol levels were within the normal range and the patient did
not exhibit adrenal insufficiency.
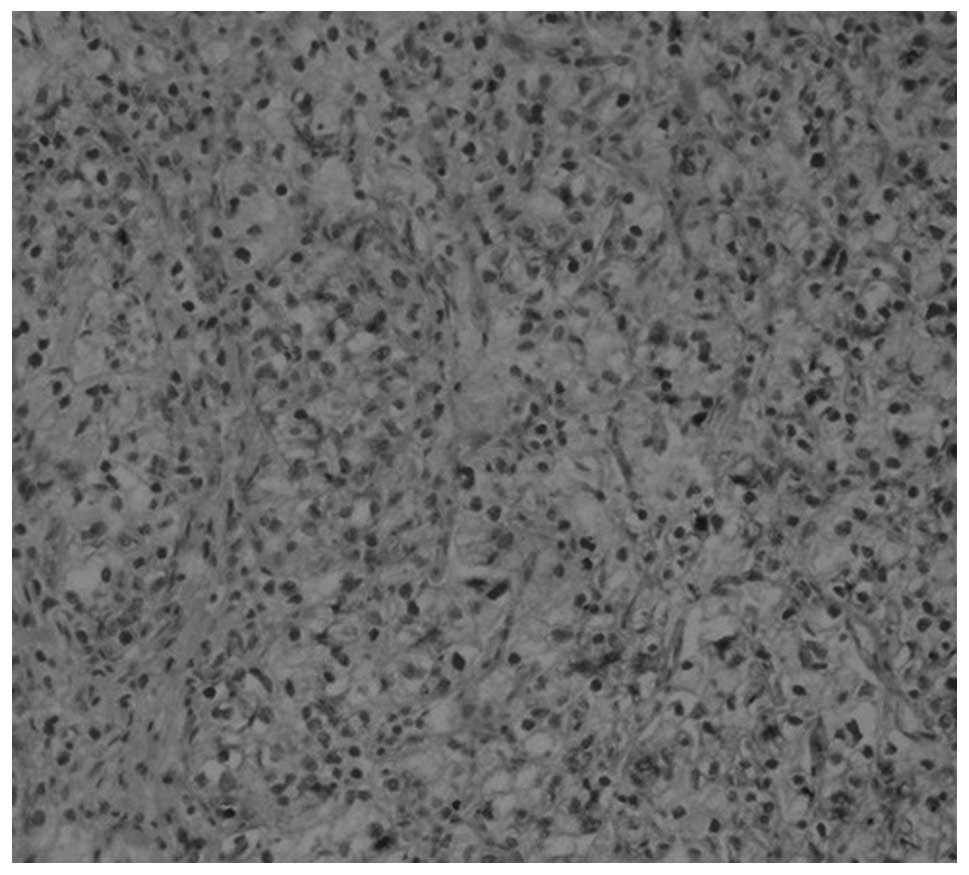
Immunohistopathological findings
The specimens obtained from the right kidney using
the US-guided biopsy technique demonstrated characteristics typical
of clear cell RCC, and high magnification examination of the right
radical nephrectomy, right partial adrenalectomy and left
adrenalectomy specimens revealed tumor cells with an alveolar
structure, clear cytoplasm and small nucleolus (hematoxylin and
eosin staining; magnification, ×200; Fig. 4). Furthermore, immunohistochemical
examination revealed positive staining for RCC and cluster of
differentiation 10 (Figs. 5 and
6). Thus, a diagnosis of bilateral
adrenal metastasis from clear cell RCC was established.
Discussion
A routine ipsilateral adrenalectomy is not
recommended in cases of radical nephrectomy (6), as there is no difference in the
overall survival rate between undergoing surgery and not undergoing
surgery. Only 3/2,065 patients who underwent concurrent ipsilateral
adrenalectomy exhibited direct invasion of the adrenal gland by RCC
or RCC metastasis. Even in the presence of suspicious adrenal
lesions detected by imaging techniques, only 13% of these lesions
are cancerous (7). Furthermore, in
a retrospective study by Kobayashi et al (8), no statistically significant difference
was identified in terms of cancer-specific survival (CSS) between
patients that underwent ipsilateral simultaneous adrenalectomy and
patients that underwent adrenal-sparing radical nephrectomy due to
RCC. Ipsilateral adrenalectomy does not appear to provide any
survival benefits, however, it is currently recommended when upper
pole tumors are present, metastases are detected by CT and/or
magnetic resonance imaging (MRI), or a renal mass measuring >8
cm is identified (9). Various risk
factors have been described for the development of adrenal
metastasis, including large renal masses, upper pole tumors, tumors
arising from the left kidney and multifocal tumors; however, it
must be considered that small lower pole tumors may subsequently
develop ipsilateral and contralateral adrenal metastases. These
adrenal metastases may occur by tumor spread via the vessel in
Gerota’s fascia, the lymphatic vessels, arterial embolism or
retrograde venous embolism (10,11).
In addition, the risk of developing metastasis is lower in the
right adrenal gland compared with the left adrenal gland (12). However, the present case possessed
none of the abovementioned risk factors and the burden of
metastasis was higher in the right adrenal gland compared with left
side. In a systematic review of 11,736 patients conducted by Su
et al (13), the role of
ipsilateral adrenalectomy was evaluated in radical nephrectomy and
a novel use for adrenalectomy was proposed. The rate of ipsilateral
involvement in RCC was 4.5%; however, upper pole tumors were not
associated with a higher incidence of ipsilateral adrenal
metastases, and adrenal involvement from RCC was rare, even in
advanced tumors. Furthermore, synchronous adrenalectomy did not
appear to offer any survival benefit, even for high-risk patients.
Therefore, Su et al (13)
proposed that adrenalectomy should be performed, in addition to
radical nephrectomy, when an ipsilateral adrenal mass is detected
in the preoperative period.
Although adrenal-sparing radical nephrectomy is a
standard surgical procedure, it should not be the preferred method
in the presence of suspicious adrenal lesions detected by imaging
methods; in this case, adrenalectomy is recommended. A number of
cases of RCC with ipsilateral metastasis are considered to be
associated with the underdiagnosis of metastasis in the adrenal
tissue. In such cases, intraoperative frozen section examination
may be of benefit in the decision to perform adrenalectomy
(14). Adrenal metastases are
common, however, benign adrenal adenomas account for 70% of adrenal
masses detected in cancer patients (15). Radiological studies may facilitate
preoperative diagnosis; however, they cannot definitively determine
whether an adrenal tumor in an RCC patient is a primary adrenal
neoplasm, an adrenal cortical adenoma or a metastatic lesion
(3). Therefore, a hormonal
examination is recommended for RCC patients with adrenal lesions
detected that have been detected using CT, MRI or positron-emission
tomography/CT (16). This hormonal
examination is useful in the differentiation of primary carcinomas
of the adrenal gland from other hormonally active tumors. In the
present case, the hormonal examination demonstrated that ACTH,
cortisol, HMA and VMA levels were within the normal ranges.
The surgical treatment options of for adrenal
metastases are similar to those for localized disease (10). Efforts to improve survival are more
effective in patients with low metastatic tumor load, good
performance status and in those that developed adrenal metastasis
late following nephrectomy. Previous studies have demonstrated the
long-term survival and palliative benefits of metastasectomy in
selected patients (9,10). However, in the current patient,
bilateral adrenal metastases were detected synchronously in the
early period following nephrectomy. Furthermore, the surgical
removal of metastatic foci of RCC in the lungs and bones provides
survival benefit (10), and various
studies have demonstrated a survival benefit even in the presence
of multiple metastatic foci. For example, Alt et al
(10) identified that
metastasectomy provided a survival benefit in patients with RCC and
multiple metastatic lesions (9).
Similarly, according to data from the Mayo Clinic, complete
resection of the metastatic foci provided 4.8 years CSS, whereas
incomplete resection was associated with a significant reduction in
survival to 1.3 years (11). In
metastatic RCC, leaving metastatic foci untreated resulted in a
significantly worse prognosis. Instead, surgical removal is the
only known effective treatment in patients with solitary adrenal
metastasis, resulting in ≥5 years survival in 29–35% of patients
(17). In addition, Plawner
(18) demonstrated that the
five-year survival rate of patients who underwent surgery for
metachronous solitary RCC metastases to the contralateral adrenal
gland was lower than that for patients with synchronous adrenal
metastases (20 and 40%, respectively). The prognosis for RCC
patients with adrenal metastases was dependent on the time between
the detection of the adrenal metastasis and nephrectomy, and was
improved for patients who developed the metastasis late rather than
early following nephrectomy. Metastasectomy (adrenalectomy) is
particularly recommended to achieve a longer survival period
(17). In a previous study of four
patients, Chkhotua et al (19) identified that the mean cancer
specific survival time to the development of adrenal metastasis
following surgery was 83.3 months; three patients underwent
adrenalectomy and one patient underwent bilateral adrenalectomy,
and the authors reported a survival period of 19–63 months. The
shortest survival period was achieved in the patient exhibiting
bilateral metachronous adrenal metastasis. In the current study,
the presence of a bilateral adrenal metastasis was considered to be
a poor prognostic factor and the resulting adrenal insufficiency
was considered to be an additional reason for the development of
comorbidity. Therefore, adrenal-sparing surgical procedures are of
particular importance in cases of bilateral adrenal metastasis.
In a previous study, the median survival period for
patients with adrenal involvement but no systemic involvement was
11.7 years, however, survival decreased to 16 months in the
presence of systemic involvement and to six months following
bilateral adrenalectomy (13). The
presence of metastatic lesions in both of the adrenal glands
(bilateral adrenal metastasis) is regarded as widespread disease
(12). Although bilateral
adrenalectomy with radical nephrectomy is recommended to decrease
tumor load in RCC patients with metastasis to the adrenal glands,
patients who underwent this surgical procedure exhibited a poor
prognosis. Sparing the right adrenal gland is more straightforward
than sparing the left adrenal gland, due to its anatomical position
and the low risk of metastasis (12). In the present patient, partial
surgery was performed in an attempt to spare the right adrenal
gland due to its low tumor load. Parallel to the literature, the
right adrenal gland was affected to a lesser extent, despite the
primary RCC being located in the right adrenal gland. However,
controversial reports exist in the literature, for example,
Moudouni et al (20)
identified that adrenal involvement was a weak prognostic factor in
predicting the prognosis of operated RCC. Furthermore, metachronous
metastasis of RCC to periadrenal tissue has been described in the
literature; however, additional studies are required to develop an
adrenal-sparing approach for the treatment of periadrenal tissue
metastases (21).
Antonelli et al (22) compared lung metastases (LM) from RCC
with atypical metastases (AM) from RCC (including, bone, liver and
adrenal) in terms of CSS. The study evaluated 1,800 RCC patients,
comparing 37 patients who underwent lung metastasectomy with 57
patients who underwent atypical metastasectomy. CSS from
metastasectomy was affected by the synchronicity in the diagnosis
of metastasis and primary tumor, as well as by the simultaneous
presence of other metastases; however, the type of metastasis (AM
vs. LM) did not affect the CSS. Notably, metastasectomy in AM was
as effective as in LM. The present study emphasizes the importance
of RCC metastasectomy regardless of the metastatic location; even
in the presence of bilateral adrenal metastasis, adrenal-sparing
surgery with the guidance of frozen section examination may provide
significant benefits in CSS.
The detection of adrenal metastases, the choice of
surgical technique, the perioperative decision process and the
challenges in postoperative follow-up produce a clinical picture
that is difficult to manage. In the previous study by Antonelli
et al (22), long-term use
of mineralocorticoid and glucocorticoid replacement therapy must
have been considered prior to surgery to prevent the possible
development of iatrogenic Addison’s disease. Partial adrenalectomy
is an ideal treatment strategy, as sparing a section of the adrenal
tissue may prevent the occurrence of other comorbid conditions.
When intraoperative examination of the frozen sections of the mass
and adrenal tissue determine that partial adrenalectomy is not
possible, adrenalectomy must be performed. Metastatic lesions in
RCC often occur between the cortex and the medulla, however, they
can occur at any site within the organ (15). Sparing 10% of the adrenal gland is
sufficient for the maintenance of adrenal gland function;
therefore, bilateral metastatic spread to both of the adrenal
glands rarely causes adrenal insufficiency (23,24).
For bilateral metastatic patients, an alternative treatment
strategy to bilateral adrenalectomy is partial adrenalectomy, which
can be performed in suitable patients to avoid the side effects of
steroid replacement therapy, such as gastritis, hypertension and
hypokalemia (4,25). In clinical practice, metastasis to
the adrenal glands accounts for <1% of patients with primary
Addison’s disease (23), however,
iatrogenic Addison’s disease occurs relatively more frequently with
adrenalectomy. Alkan et al (21) recommended robotic surgical
approaches in the treatment of adrenal metastases due to lower rate
of complications, mortality and morbidity rates, as well as a
shorter length of hospital stay and increased patient comfort in
the postoperative period (21).
In conclusion, bilateral adrenal metastasis from
operated RCC poses a complicated oncological problem, as the
optimal diagnostic and treatment strategies of this condition are
yet to be thoroughly defined. However, it is of particular
importance to detect the hormonal activity of the metastatic
adrenal masses and, due to the survival benefits, metastasectomy is
important in the treatment of bilateral adrenal metastasis of RCC.
If adrenalectomy is required, minimally invasive surgical
procedures, such as laparoscopic/robotic procedures, should be
preferred and partial adrenalectomy should remain the preferred
type of surgery. In cases where adrenalectomy is inevitable, the
decision must be based on intra-operative biopsies and frozen
section examination. This is due to the necessity of life-long
mineralocorticoid and glucocorticoid replacement therapy in
patients with iatrogenic Addison’s disease, as well as the lack of
adrenal tissue possibly resulting in endocrinological disease,
additional to the previous oncological disease.
Abbreviations:
|
RCC
|
renal cell carcinoma
|
|
US
|
ultrasound
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
ACTH
|
adrenocorticotropic hormone
|
|
HMA
|
hydroxymandelic acid
|
|
VMA
|
vanillyl mandelic acid
|
|
CSS
|
cancer-specific survival
|
References
|
1
|
Ljungberg B, Bensalah K, Bex A, et al;
European Association of Urology. Guidelines on renal cell
carcinoma. http://www.guideline.gov/content.aspx?id=45321.
Accessed February 2, 2014
|
|
2
|
Horner MJ, Ries LAG, Krapcho M, et al;
National Cancer Institute. SEER cancer statistics review,
1975–2006. http://seer.cancer.gov/csr/1975_2006.
Accessed February 2, 2014
|
|
3
|
Lau WK, Zincke H, Lohse CM, et al:
Contralateral adrenal metastasis of renal cell carcinoma:
treatment, outcome and a review. BJU Int. 91:775–779. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Koutalellis GE, Felekouras E, Evangelou C,
et al: Renal cell carcinoma with bilateral synchronous adrenal
gland metastases: a case report. Cases J. 2:72982009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Siemer S, Lehmann J, Kamradt J, et al:
Adrenal metastases in 1635 patients with renal cell carcinoma:
outcome and indication for adrenalectomy. J Urol. 171:2155–2159.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kuczyk M, Münch T, Machtens S, et al: The
need for routine adrenalectomy during surgical treatment for renal
cell cancer: the Hannover experience. BJU Int. 89:517–522. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lane BR, Tiong HY, Campbell SC, et al:
Management of the adrenal gland during partial nephrectomy. J Urol
Jun. 181:2430–2436. 2009. View Article : Google Scholar
|
|
8
|
Kobayashi T, Nakamura E, Yamamoto S, et
al: Low incidence of ipsilateral adrenal involvement and
recurrences in patients with renal cell carcinoma undergoing
radical nephrectomy: a retrospective analysis of 393 patients.
Urology. 62:40–45. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gill IS, McClennan BL, Kerbl K, et al:
Adrenal involvement from renal cell carcinoma: predictive value of
computerized tomography. J Urol. 152:1082–1085. 1994.PubMed/NCBI
|
|
10
|
Alt AL, Boorjian SA, Lohse CM, et al:
Survival after complete surgical resection of multiple metastases
from renal cell carcinoma. Cancer. 117:2873–2882. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Karam JA and Wood CG: The role of surgery
in advanced renal cell carcinoma: cytoreductive nephrectomy and
metastasectomy. Hematol Oncol Clin North Am. 25:753–764. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yu CC, Huang JK, Tzeng WS, et al:
Simultaneous bilateral adrenal metastases from renal cell
carcinoma. Surgical implications and review of the literature. Eur
Urol. 22:335–338. 1992.PubMed/NCBI
|
|
13
|
Su JR, Zhu DJ, Liang W and Xie WL:
Investigation on the indication of ipsilateral adrenalectomy in
radical nephrectomy: a meta-analysis. Chin Med J (Engl).
125:3885–3890. 2012.
|
|
14
|
Tsui KH, Shvarts O, Smith RB, et al:
Prognostic indicators for renal cell carcinoma: a multivariate
analysis of 643 patients using the revised 1997 TNM staging
criteria. J Urol. 163:1090–1095. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vespasiani G, Porena M, Virgili G, et al:
Renal cell carcinoma with synchronous adrenal metastases. Acta Urol
Belg. 58:197–203. 1990.PubMed/NCBI
|
|
16
|
Sancho JJ, Triponez F, Montet X and
Sitges-Serra A: Surgical management of adrenal metastases.
Langenbecks Arch Surg. 397:179–194. 2012. View Article : Google Scholar
|
|
17
|
Kessler OJ, Mukamel E, Weinstein R, et al:
Metachronous renal cell carcinoma metastasis to the contralateral
adrenal gland. Urology. 51:539–543. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Plawner J: Results of surgical treatment
of kidney cancer with solitary metastasis to contralateral adrenal.
Urology. 37:233–236. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chkhotua A, Managadze L and Pertia A:
Metastasis of renal cell carcinoma to contralateral adrenal gland:
case report and review of the literature. Georgian Med News.
212:12–18. 2012.PubMed/NCBI
|
|
20
|
Moudouni SM, En-Nia I, Rioux-Leclercq N,
et al: Solitary contralateral adrenal metastasis after nephrectomy
for renal cell carcinoma. Urol Int. 68:295–298. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Alkan E, Ozkanli O and Balbay D:
Metachronous periadrenal fatty tissue metastasis from contralateral
renal cell carcinoma. Case Rep Urol. 2013:2060782013.PubMed/NCBI
|
|
22
|
Antonelli A, Arrighi N, Corti S, et al:
Surgical treatment of atypical metastasis from renal cell carcinoma
(RCC). BJU Int. 110:E559–E563. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Selli C, Carini M, Barbanti G, et al:
Simultaneous bilateral adrenal involvement by renal cell carcinoma:
experience with 3 cases. J Urol. 137:480–482. 1987.PubMed/NCBI
|
|
24
|
Rosenthal FD, Davies MK and Burden AC:
Malignant disease presenting as Addison’s disease. Br Med J.
1:1591–1592. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Schomer NS and Mohler JL: Partial
adrenalectomy for renal cell carcinoma with bilateral adrenal
metastases. J Urol. 153:1196–1198. 1995. View Article : Google Scholar : PubMed/NCBI
|