Introduction
Osteonecrosis of femoral head (ONFH) is a
multifactorial degenerative bone disease, which may lead to the
gradual destruction and collapse of the femoral head and secondary
arthritis of the hip. Although idiopathic OFNH, steroid treatment,
alcohol consumption and trauma are considered the etiology of ONFH
(1,2), its pathogenesis remains to be
clarified and several hypotheses have been proposed, including
lipid dysfunction, increased apoptotic activity of osteocyte and
osteoblast, disorder of bone homeostasis and intravascular and
coagulation abnormalities (1,3). These
multi-hits (the cause of the lipid dysfunction, increasing
apoptotic activity of osteocyte and osteoblast, disorder of the
bone homeostasis and the intravascular and coagulation
abnormalities) result in compromised blood supply to the femoral
head and this ischemic insult of the femoral head may result in
ONFH. Therefore, the factors that induce a decrease in blood flow
and vascular deficiency resulting in failure to obtain sufficient
nutrients may be the final and of importance pathway of
osteonecrosis.
Factor V (FV) is a pivotal auxiliary factor involved
in the blood coagulation process. Following the proteolytic
activation of FV, the yield factor Va (FVa) forms the cofactor of
the prothrombinase complex binding to the FXa, which regulates the
formation of thrombin (4).
Additionally, activated protein C (APC) modulates the generation of
thrombin by inactivating the FVa. Factor V Leiden (FVL) gene
mutation is a common polymorphism in FV that results in a guanine
to adenine substitution at the nucleotide position 1691 (G1691A
polymorphism), a missense mutation FV Arg506Gln (5). As a result, a single inactivation site
of FV by activated protein C is altered, causing thrombophilia (an
increased tendency to form thrombi) and leading to intravascular
coagulation disorders. It was reported that FVL was associated with
thrombo embolic diseases such as symptomatic pulmonary embolism,
deep vein thrombosis and myocardial infarction (6,7).
Several case-control studies have been conducted to examine the
association between FVL and ONFH (8–14).
However, some studies have shown inconsistent or even contradictory
results. Explanations for this discrepancy include small sample
size, racial and ethnic differences, publication bias or
uncorrected multiple hypothesis testing.
Meta-analysis is a statistical procedure for
combining results from several studies to produce a single estimate
of the major effect, thus enhancing the precision and statistical
power (15). One of the advantages
of meta-analysis is to increase sample size, which may control the
probability of random error. Thus, meta-analysis is a useful and
rigorous method to summarize different studies that have
inconsistent results. With this as a background, we performed this
meta-analysis to assess the association of FVL with the risk of
ONFH in the published studies.
Materials and methods
Search strategies and criteria
A systematic literature search was conducted using
the following electronic databases: PubMed, Elsevier Science
Direct, Chinese National Knowledge Infrastructure (CNKI) and the
Chinese Biomedical Database (CBM) prior to December, 2012, with the
key words ‘factor V’ or ‘Leiden’ and ‘osteonecrosis’ as both
medical subject heading (MeSH) terms and text words. No limitation
on the language was applied.
The included criteria were summarized as follows: i)
the study had already been published; ii) the study provided
original data on the association of FVL and ONFH using a
case-control study design; iii) enough data were provided to
calculate the rate difference with a confidence interval (CI) and
P-value and; iv) the genotype frequencies conformed to the
Hardy-Weinberg equilibrium (HWE) among the controls. Exclusion
criteria were: i) studies that contained overlapping data; ii)
studies that were case reports and; iii) studies in which family
members had been studied because their analysis is based on linkage
consideration. An additional manual search of some relevant
journals was conducted after perusal of the bibliographies of
retrieved papers and review articles.
Data abstraction
Eligible publications were selected strictly
according to the inclusion criteria listed above and all relevant
data regarding first author’s name, year of publication, patient
demographic ethnicity, total number of cases and controls and
genotyping information were independently extracted and recorded by
two authors. Disagreements regarding extracted data were resolved
by discussion with our research team. Different ethnicities were
classified as non-Asian and Asian.
Meta-analysis methods
We examined the odds ratio (OR), i.e., the ratio of
the odds of an event occurring in a case group to the odds of that
event occurring in the control group and the respective 95%
confidence intervals (CIs) by comparing FVL with the wild
homozygotes GA + AA vs. GG. The within- and between-study variation
or heterogeneity was also assessed using the χ2
test–bases Q-statistic and I2-statistic (16,17).
If a significant Q–statistic (P<0.10) indicated heterogeneity
across studies, the random-effects model was used for
meta-analysis. Otherwise, the fixed-effects model was used. The
random-effects model was used to take into account the possibility
of heterogeneity between studies, while the fixed-effects model
assumes all of the studies are estimating the same underlying
effect and considers only within-study variation. The
I2-statistic measures the degree of inconsistency in the
studies by calculating what percentage of the total variation
across studies is due to heterogeneity rather than by chance
(18). Additionally, in the
presence of (P<0.10 or I2>50%) or not, the overall
or pooled estimate of risk (OR) was obtained by using the
DerSimonian-Laird random-effects model or using the Mantel-Haenszel
fixed-effects model. The χ2 test was used for the HWE of
genotypes in the control group of each study.
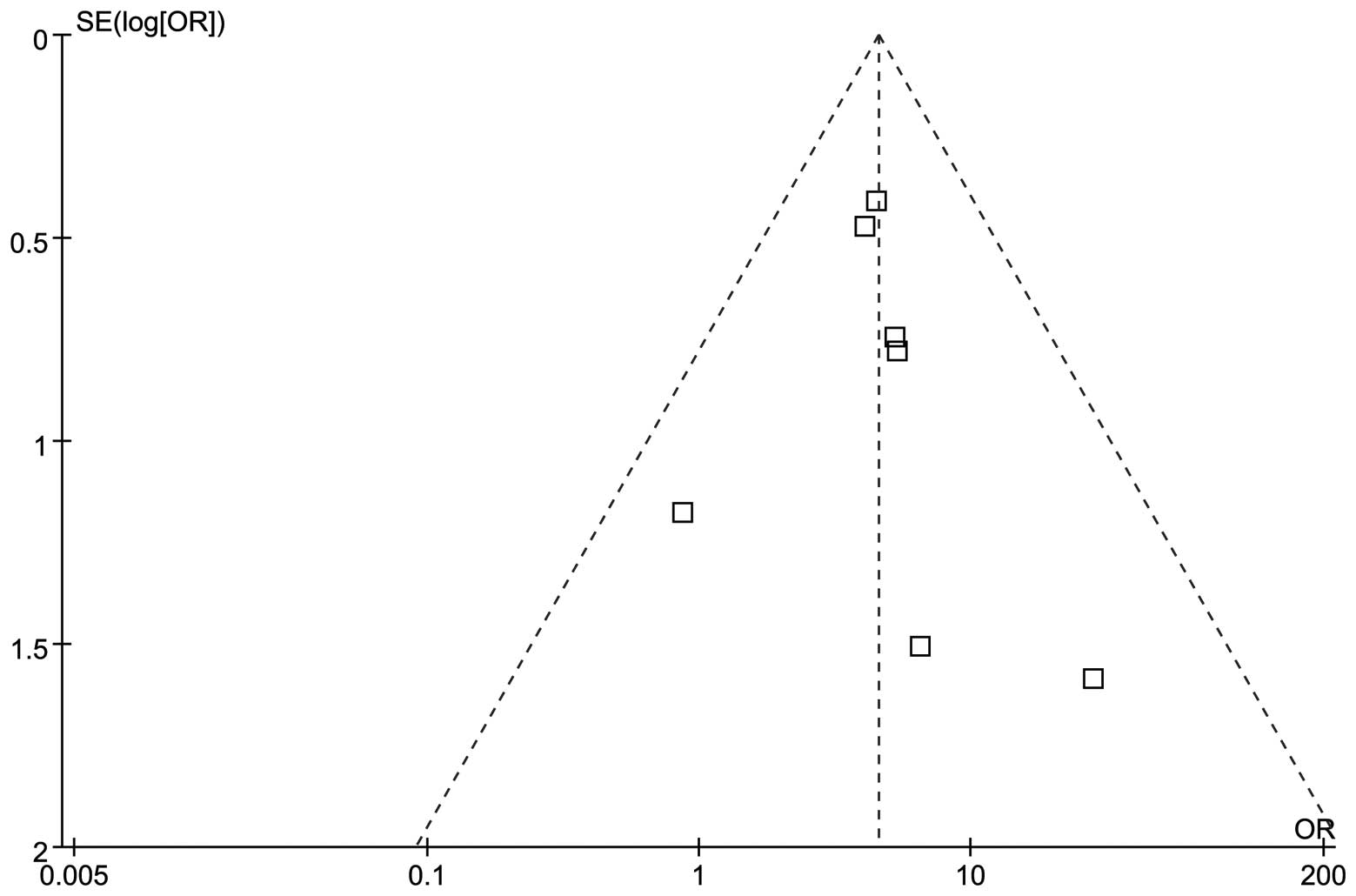
Publication bias was assessed by funnel plots, in
which the standard error of log (OR) of each study was plotted
against its log (OR). The funnel plot asymmetry, which suggests a
possible publication bias, was examined by the method of Egger’s
linear regression test (15). The
significance of the intercept was assessed by the Student’s t-test,
as previously mentioned (15).
P<0.05 was considered representative of statistically
significant publication bias.
The meta-analysis was performed using the Review
Manager software (ver.5.0, Copenhagen: The Nordic Cochrane Centre,
The Cochrane Collaboration, 2008) and Stata statistical software
(version 10) (Stata-Corp LP, College Station, TX, USA). All of the
P values were two sided and P<0.05 was considered to indicate a
statistically significant difference.
Results
Characteristics of eligible studies
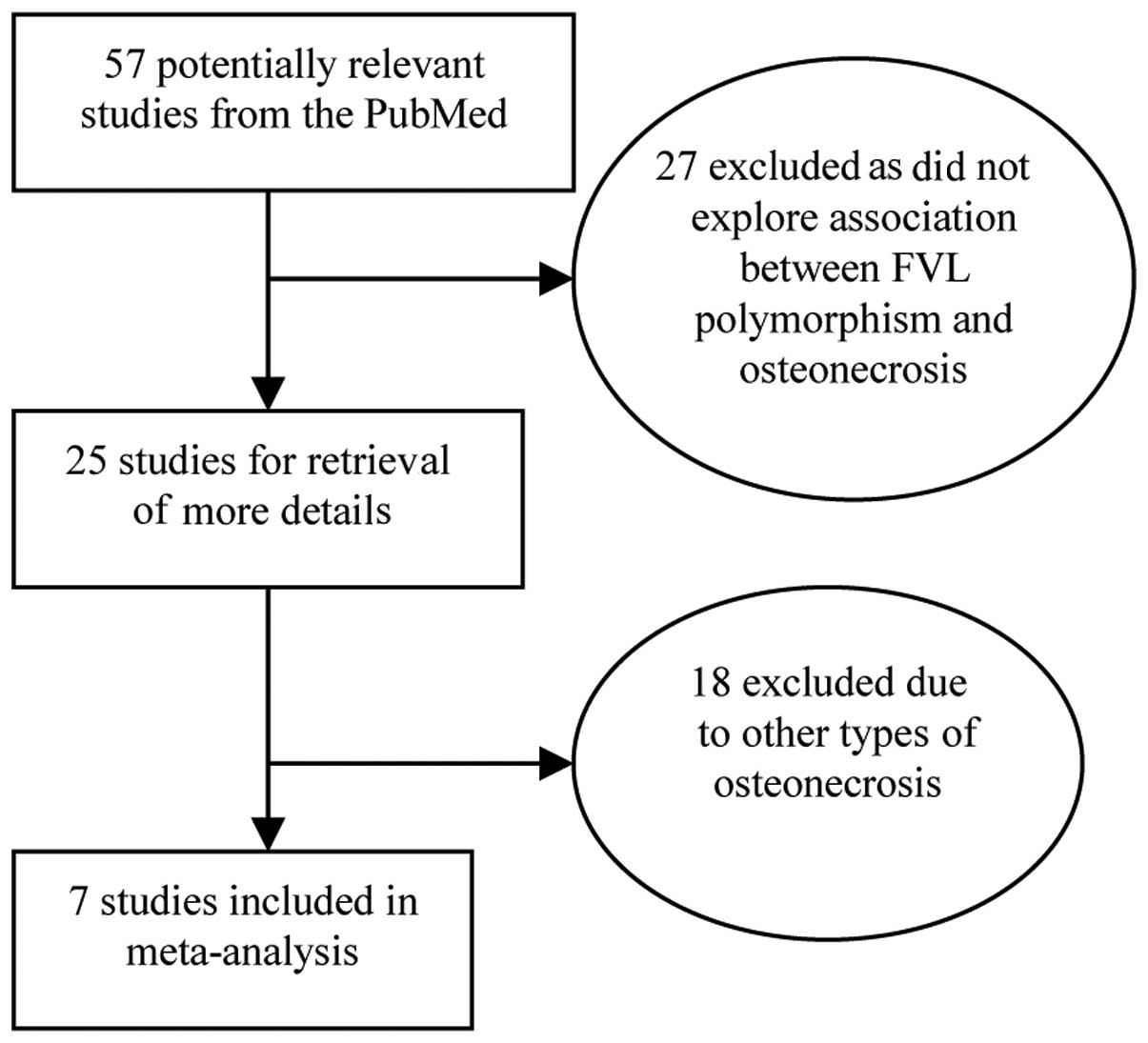
The characteristics of the 7 studies included in the
present meta-analysis are provided in Table I (8–14). We
reviewed 57 potentially relevant citations and abstracts obtained
after a search of PubMed was conducted (Fig. 1). Of these, 27 studies were excluded
as they did not survey the association between FVL polymorphism and
osteonecrosis, thus 25 studies were screened for full publication
review. Following a detailed evaluation of the remaining 25
studies, another 18 studies were deleted as they did not conform to
the definition of ONFH (Fig. 1).
The search performed in the Elsevier Science Direct, CNKI and CBM
databases did not yield any additional studies not indexed by
PubMed. A total of 7 studies were included in the current
meta-analysis.
 | Table I.Characteristics of the studies
included in the present meta-analysis. |
Table I.
Characteristics of the studies
included in the present meta-analysis.
| First author | Year | Country | Case
| Control
| Refs. |
|---|
| Wild | Leiden | Total | Wild | Leiden | Total |
|---|
| Bjorkman | 2004 | Sweden | 54 | 9 | 63 | 271 | 11 | 282 | 8 |
| Celik | 2006 | Turkey | 10 | 1 | 11 | 35 | 4 | 39 | 9 |
| Ekmekci | 2006 | Turkey | 13 | 6 | 19 | 35 | 3 | 38 | 10 |
| Glueck | 1999 | America | 55 | 4 | 59 | 40 | 0 | 40 | 11 |
| Glueck | 2008 | America | 11 | 2 | 13 | 64 | 0 | 64 | 12 |
| Glueck | 2012 | America | 221 | 23 | 244 | 102 | 2 | 104 | 13 |
| Zalavras | 2004 | Greece | 59 | 13 | 72 | 286 | 14 | 300 | 14 |
Evaluation of publication bias
Funnel plots and Egger’s test were performed to
access the publication bias of studies included in this
meta-analysis. The shape of the funnel plot was not obviously
asymmetrical in distribution for GA + AA vs. GG (Fig. 2). Furthermore, the Egger’s
regression test was used to provide statistical evidence of funnel
plot symmetry (P=0.65), which confirmed no evidence of substantial
publication bias (data not shown).
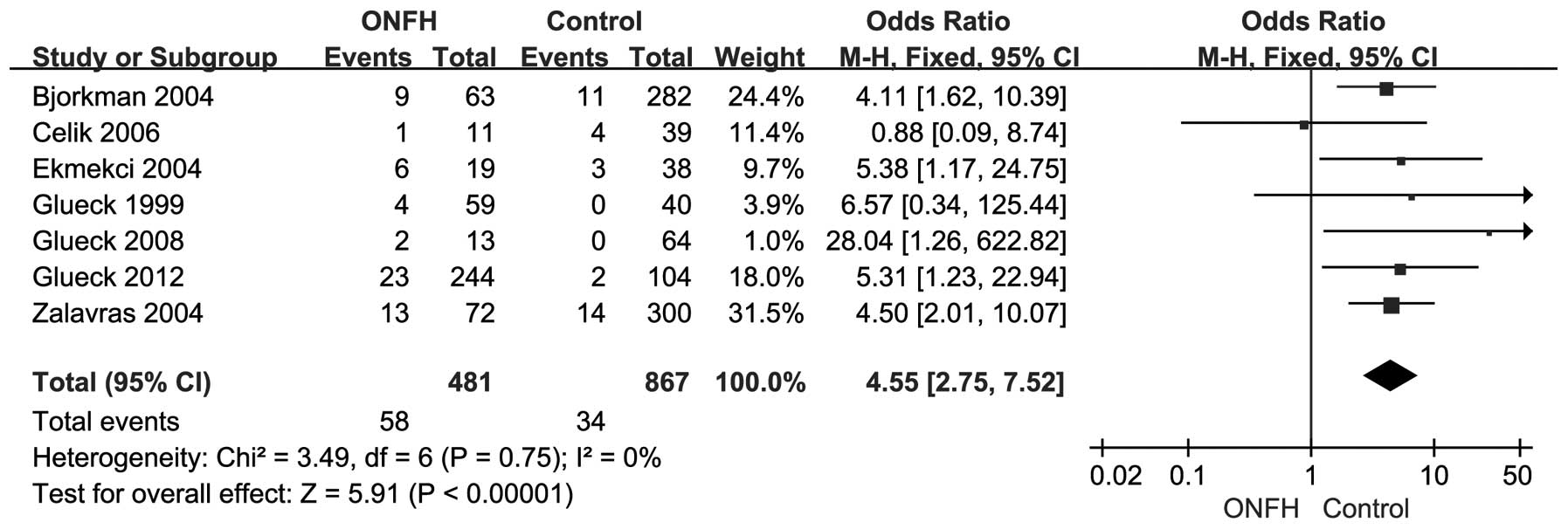
Association of FVL and ONFH
The association between FVL mutation and risk of
developing ONFH in the overall population were detected when
examining the contrast of FVL vs. wild homozygote (OR=4.55, 95% CI,
2.75–7.52, P<0.00001) and without significant between-study
heterogeneity (χ2=3.49, P=0.75, I2=0%). The
forest plot of the distribution of the ORs is shown in Fig. 3. A sensitivity analysis was
performed by changing the fixed-effects model into the
random-effects model. The results showed that there was still a
significant association when the random-effects model was used
(OR=4.47, 95% CI, 2.71–7.37, P<0.00001) although no results were
found for the forest plot of the distribution of the ORs. The
results of the fixed- and random-effects models were in agreement
with each other.
Discussion
In recent years, an increased tendency for
intravascular coagulation has been proposed as the final pathway in
the pathogenesis of osteonecrosis (19) and various environmental and genetic
risk factors lead to the interruption of the intra osseous
microcirculation supply and osteonecrosis. Intravascular thrombosis
is an effect of intravascular coagulation disorder and is
considered the cause of non-traumatic osteonecrosis (20). FVL mutation is a most common
inherited thrombophilias and causes APC resistance. An association
of APC resistance with elevated plasma levels of coagulation
markers has been identified, suggesting that this phenotype
represented an in vivo hypercoagulable state (21). However, inconsistent results were
observed when FVL was investigated in ONFH patients. Considered
individually, some studies in our meta-analysis did not reveal a
statistically significant association with ONFH (Table I and Fig. 3), possibly due to small sample size
and therefore limited statistical power of these individual
studies. The largest sample size among the included studies was
372, while the smallest was only 50. However, most studies
concluded that the FVL polymorphism was a risk factor for ONFH.
Therefore, our meta-analysis draws a conclusion that FVL has an
effect on ONFH patients.
Based on the results obtained, we established an
association between FVL mutation and ONFH, with a cumulative OR of
4.55. Therefore, the carriers of FVL mutation had a 4-fold risk of
ONFH when compared with non-carriers. Inclusion and exclusion
criteria are a crucial component of a meta-analysis and may affect
the results. We were relatively conservative in selecting studies,
which likely underestimated the alrealy identified association.
Several articles investigating FVL met our criteria, but they were
excluded as they could not provide sufficient information for
calculating the ORs of the FVL mutation and be extracted (22–24).
Consequently, the studies that were included in this meta-analysis
strengthened the association between FVL mutation and ONFH.
Of note, the disproportionately large study by
Zalavras et al (14) showed
a strong association (OR=4.5) and it contributed 31.5% of the
FVL-positive ONFH cases to our meta-analysis. Nevertheless, the
relatively small study by Celik et al (9) showed no association (OR=0.88). One
possible reason for the insignificant effect of the present study
was the limited sample size. Additionally, the main population
included in the meta-analysis was non-Asian. Two studies in which
the study subjects included an Asian population and conformed to
the included criteria were deleted as they observed no FVL mutation
in cases or controls. Chang et al (22) suggested that the FVL mutation is not
a genetic risk factor for ONFH in Asians, or at least in the Korean
population, which was in agreement with findings by Sun et
al (24). The results obtained
by these authors were consistent with previous reports, which
demonstrated the absence of FVL mutation in the Chinese and Korean
populations (25,26). A previous study also showed that
Factor V Leiden allele was present in ∼5% of Caucasian individuals
(Europeans, Jews, Israeli Arabs and Indians) (27). The reasons for the same polymorphism
having different associations influenced by different ethnic
populations or studies may be explained by various factors.
Firstly, the polymorphism plays a different role in different
ethnicities in different genetic backgrounds, as indicated above.
There are also a number of other factors that may affect
thrombosis, such as the damage of vascular endothelial cells,
changes of blood flow and drugs. Additionally, the potential
contribution of differences in patient demographic parameters, such
as age, gender and disease severity that may lead to varying
results should be considered, although this data was not available
for the present meta-analysis.
In addition, FVL can be co-inherited with other
genetic risk factors to increase the susceptibility to thrombosis
in the individual patient population (28). A number of the studies included in
this meta-analysis considered multiple genetic risk factors.
5,10-Methylenetetrahydrofolate reductase (MTHFR) is an enzyme that
plays a role in the re-methylation of homo-cysteine and the C667T
polymorphism is involved in the elevated plasma total homocysteine
level (29). Furthermore, it has
been proven that coinheritance of MTHFR and FVL was likely to
increase the risk of venous thromboembolism (30). Another such polymorphism is the
prothrombin gene G20210A mutation, which is associated with a
20–50% increase in prothrombin plasma levels (31). In addition to the FVL polymorphism,
two studies (9,11) investigated the MTHFR C667T
polymorphism and five studies (8–10,13,14)
investigated the prothrombin gene G20210A mutation association with
ONFH. However, results of most studies indicated a negative
conclusion, which reported that MTHFR C667T polymorphism and
prothrombin gene G20210A mutation were not risk factors in ONFH.
However, a limited sample size may have been used and therefore a
lower power to detect the true association. Therefore, larger
studies are necessary to determine whether these polymorphisms and
mutations serve as risk factors for ONFH.
Nevertheless, there were limitations to this
meta-analysis. Firstly, the sample size of studies included was
relatively small and more studies containing a large sample size
are required. Secondly, most control groups were not uniformly
defined. Case and control groups were not age- and gender-matched,
which might increase the selection bias. Thirdly, we focused mainly
on English and Chinese studies, thus, language bias may also be a
relevant factor. Fourthly, the meta-analysis remains a
retrospective investigation that is subject to the methodological
deficiencies of the included studies. Additionally, no publication
bias was detected, indicating that the total pooled OR might be
unbiased.
In conclusion, the present meta-analysis has
demonstrated the association between FVL polymorphism and ONFH
susceptibility. However, to reach a definitive conclusion, large
sample studies including different ethnic groups with age- and
gender-matched groups and multiple gene polymorphism detection
should be considered. Additional investigations focusing on the
gene-gene and gene-environment interaction in the process of
pathogenesis should also be conducted.
References
|
1
|
Malizos KN, Karantanas AH, Varitimidis SE,
Dailiana ZH, Bargiotas K and Maris T: Osteonecrosis of the femoral
head: etiology, imaging and treatment. Eur J Radiol. 63:16–28.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jones LC and Hungerford DS: Osteonecrosis:
etiology, diagnosis, and treatment. Curr Opin Rheumatol.
16:443–449. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lafforgue P: Pathophysiology and natural
history of avascular necrosis of bone. Joint Bone Spine.
73:500–507. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rosing J and Tans G: Coagulation factor V:
an old star shines again. Thromb Haemost. 78:427–433.
1997.PubMed/NCBI
|
|
5
|
Bertina RM, Koeleman BPC, Koster T, et al:
Mutation in blood coagulation factor V associated with resistance
to activated protein C. Nature. 369:64–67. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dentali F, Ageno W, Bozzato S, et al: Role
of factor V Leiden or G20210A prothrombin mutation in patients with
symptomatic pulmonary embolism and deep vein thrombosis: a
meta-analysis of the literature. J Thromb Haemost. 10:732–737.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dowaidar M and Settin A: Risk of
myocardial infarction related to factor V Leiden mutation: a
meta-analysis. Genet Test Mol Biomarkers. 14:493–498. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bjorkman A, Svensson PJ, Hillarp A,
Burtscher IM, Runow A and Benoni G: Factor V leiden and prothrombin
gene mutation: risk factors for osteonecrosis of the femoral head
in adults. Clin Orthop Relat Res. 452:168–172. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Celik A, Tekis D, Saglam F, et al:
Association of corticosteroids and factor V, prothrombin, and MTHFR
gene mutations with avascular osteonecrosis in renal allograft
recipients. Transplant Proc. 38:512–516. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ekmekci Y, Keven K, Akar N, et al:
Thrombophilia and avascular necrosis of femoral head in kidney
allograft recipients. Nephrol Dial Transplant. 21:3555–3558. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Glueck CJ, Fontaine RN, Gruppo R, et al:
The plasminogen activator inhibitor-1 gene, hypofibrinolysis, and
osteonecrosis. Clin Orthop Relat Res. 366:133–146. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Glueck CJ, Freiberg RA, Boppana S and Wang
P: Thrombophilia, hypofibrinolysis, the eNOS T-786C polymorphism,
and multifocal osteonecrosis. J Bone Joint Surg Am. 90:2220–2229.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Glueck CJ, Freiberg RA, Boriel G, et al:
The role of the factor V Leiden mutation in osteonecrosis of the
hip. Clin Appl Thromb Hemost. June 12–2012.(Epub ahead of
print).
|
|
14
|
Zalavras CG, Vartholomatos G, Dokou E and
Malizos KN: Genetic background of osteonecrosis: associated with
thrombophilic mutations? Clin Orthop Relat Res. 251–255.
2004.PubMed/NCBI
|
|
15
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cochran WG: The combination of estimates
from different experiments. Biometrics. 10:101–129. 1954.
View Article : Google Scholar
|
|
17
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jones JP Jr: Intravascular coagulation and
osteonecrosis. Clin Orthop Relat Res. 277:41–53. 1992.PubMed/NCBI
|
|
20
|
Jones JP Jr: Coagulopathies and
osteonecrosis. Acta Orthop Belg. 65(Suppl 1): 5–8. 1999.
|
|
21
|
Lowe GD, Rumley A, Woodward M, Reid E and
Rumley J: Activated protein C resistance and the FV: R506Q mutation
in a random population sample-associations with cardiovascular risk
factors and coagulation variables. Thromb Haemost. 81:918–924.
1999.PubMed/NCBI
|
|
22
|
Chang JD, Hur M, Lee SS, Yoo JH and Lee
KM: Genetic background of nontraumatic osteonecrosis of the femoral
head in the Korean population. Clin Orthop Relat Res.
466:1041–1046. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kechli AM, Wilimas JA, Pui CH, Park VM,
Tonkel S and Deitcher SR: Factor V Leiden and other hypercoagulable
state mutations are not associated with osteonecrosis during or
after treatment for pediatric malignancy. J Pediatr. 134:310–314.
1999. View Article : Google Scholar
|
|
24
|
Sun W, Li ZR, Shi ZC, et al: Hematological
changes and related gene mutation of post-severe acute respiratory
syndrome patients with osteonecrosis. Zhonghua Yi Xue Za Zhi.
86:442–445. 2006.(In Chinese).
|
|
25
|
Jun ZJ, Ping T, Lei Y, Li L, Ming SY and
Jing W: Prevalence of factor V Leiden and prothrombin G20210A
mutations in Chinese patients with deep venous thrombosis and
pulmonary embolism. Clin Lab Haematol. 28:111–116. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim YW, Yoon KY, Park S, Shim YS, Cho HI
and Park SS: Absence of factor V Leiden mutation in Koreans. Thromb
Res. 86:181–182. 1997.PubMed/NCBI
|
|
27
|
De Stefano V, Chiusolo P, Paciaroni K and
Leone G: Epidemiology of factor V Leiden: clinical implications.
Semin Thromb Hemost. 24:367–379. 1998.PubMed/NCBI
|
|
28
|
Rosendorff A and Dorfman DM: Activated
protein C resistance and factor V Leiden: a review. Arch Pathol Lab
Med. 131:866–871. 2007.PubMed/NCBI
|
|
29
|
Frosst P, Blom HJ, Milos R, et al: A
candidate genetic risk factor for vascular disease: a common
mutation in methylenetetrahydrofolate reductase. Nat Genet.
10:111–113. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Eldibany MM and Caprini JA:
Hyperhomocysteinemia and thrombosis: an overview. Arch Pathol Lab
Med. 131:872–884. 2007.PubMed/NCBI
|
|
31
|
Rosendaal FR, Doggen CJ, Zivelin A, et al:
Geographic distribution of the 20210 G to A prothrombin variant.
Thromb Haemost. 79:706–708. 1998.PubMed/NCBI
|