Introduction
Yttrium-90 (Y90) microspheres are used to treat
patients with primary hepatic and liver-dominant metastatic cancer.
The glass and resin Y90 products differ significantly in the
density of radionuclide per bead. Glass microspheres have a higher
density [2,500 Becquerel (Bq)/bead] of Y90 than resin (50 Bq/bead)
(1). The higher Y90 concentration in
glass beads allows the delivery of prescribed activity without
feeding artery occlusion, a known issue with resin microspheres.
From the time of government approval in 2002, the standard
technique for infusion of resin microspheres used sterile water
(H2O) alternating with small aliquots of contrast to
evaluate for arterial stasis prior to delivery of the entire dose
vial (2,3). While clinical outcomes have resulted in
excellent control of hepatic disease, a previous review using
H2O to inject resin microspheres identified a 20% early
stasis rate (4–6).
Delivering less than the prescribed Y90 activity has
the potential to reduce treatment efficacy or result in earlier
time to progression. Therefore, investigation of other injection
methods for resin microspheres is required. In 2013, our group
began to use 5% dextrose in water (D5W) as an
alternative to H2O (7).
The aim of the current study was to measure the
incidence of premature stasis using D5W in comparison to
H2O. We hypothesized that D5W induces stasis
less frequently than H2O in a clinical cohort of
patients with primary or secondary hepatic malignancy.
Materials and methods
Clinical setting and patients
Our Institutional Review Board approved this
retrospective study. All the procedures performed were in
accordance with the ethical standards of the Vanderbilt University
School of Medicine and with the 1964 Helsinki declaration and its
later amendments or comparable ethical standards.
We retrospectively reviewed laboratory, radiology
and nuclear pharmacy reports of all resin Y90 infusions performed
between July, 2013 and July, 2014. Consecutive patients treated
after September, 2013, were treated with D5W. A previous
data set of 128 infusions using H2O was included as well
(4). Patients in the comparison group
were treated using an identical technique, as one of the current
investigators (DBB) was involved with the previous study (4). Thus, 112 patients were treated as
follows: 78 with H2O and 34 with D5W.
Thirty-seven of the 78 H2O patients and 14 of the 34
D5W patients were male.
Patients were scheduled for treatment after clinic
assessment, including review of relevant cross-sectional imaging
(computed tomography and/or magnetic resonance imaging). Mapping
arteriography was performed as described previously (1). Criteria for treatment with Y90
microspheres included: i) Confirmed unresectable liver-dominant
disease; ii) an East Coast Oncology Group performance status of
0–2; and iii) adequate liver function (bilirubin of <1.8
mg/dl).
Patients were excluded from treatment if there was:
i) A life expectancy of <3 months, ii) side branch flow to the
gastrointestinal tract that could not be avoided or embolized, and
iii) the estimated lung dose was expected to exceed 25 Gray.
Y90 treatment
Y90 infusion was performed 7–10 days after mapping.
The dose was prescribed using the body surface area (BSA) method
and calculated as: A Gigabecquerel (GBq) =
(BSA-0.2)+Vtumor/Vliver, where A represents
prescribed activity in GBq and Vtumor and
Vliver represent the volume of the tumor and total
infused liver volume, respectively. BSA in square meters was
calculated as: 0.20247 × height in m0.725 × weight in
kg0.425.
Patients were treated with lobar therapy. In the
setting of bilobar disease, sequential infusions were performed 5–6
weeks apart.
A standard infusion protocol was followed for all
resin microsphere infusions. These infusions were performed off
label as non-colorectal metastases were treated. For the patients
with colorectal cancer metastases, infusions were off label as
intra-arterial chemotherapy was not used. Two interventional
radiologists with 5 and 19 years experience performed the infusions
(AJL, DBB). No anti-reflux devices or occlusion balloon techniques
were used. The proprietary delivery kit was used in all the cases
with the microspheres pushed into the delivery tubing with small
aliquots of H2O or D5W. After the line was
cleared, 2–3 ml of non-ionic contrast (Optiray 350-Ioversol 74%,
Mallinckrodt Pharmaceuticals, Dublin, Ireland) was injected to
evaluate for stasis. The process was repeated until the delivery
vial was clear to vision. At this point, the vial was emptied by
filling the priming line with air.
Stasis
Stasis was defined as a lack of antegrade arterial
flow leading to procedure cessation prior to delivering the final
air purge of the vial. Post-infusion assessment of residual
activity was measured using a Ludlum Model 3 Survey Meter (Ludlum
Measurements, Inc., Sweetwater, TX, USA).
Statistical analysis
The primary outcome variable was the incidence of
stasis. The stasis incidents between H2O and
D5W cases were compared using a z-test, with α=0.05.
Secondary measures included differences in prescribed activity and
the percentage of prescribed activity that was delivered between
the H2O and D5W groups. The secondary
variables were evaluated using t-tests.
Results
A total of 112 patients were treated: 78 with
H2O and 34 with D5W. Thirty-seven of the 78
H2O patients and 14 of the 34 D5W patients
were male. The group underwent 190 infusions: 137 were performed
with H2O and 53 with D5W. Infusions and
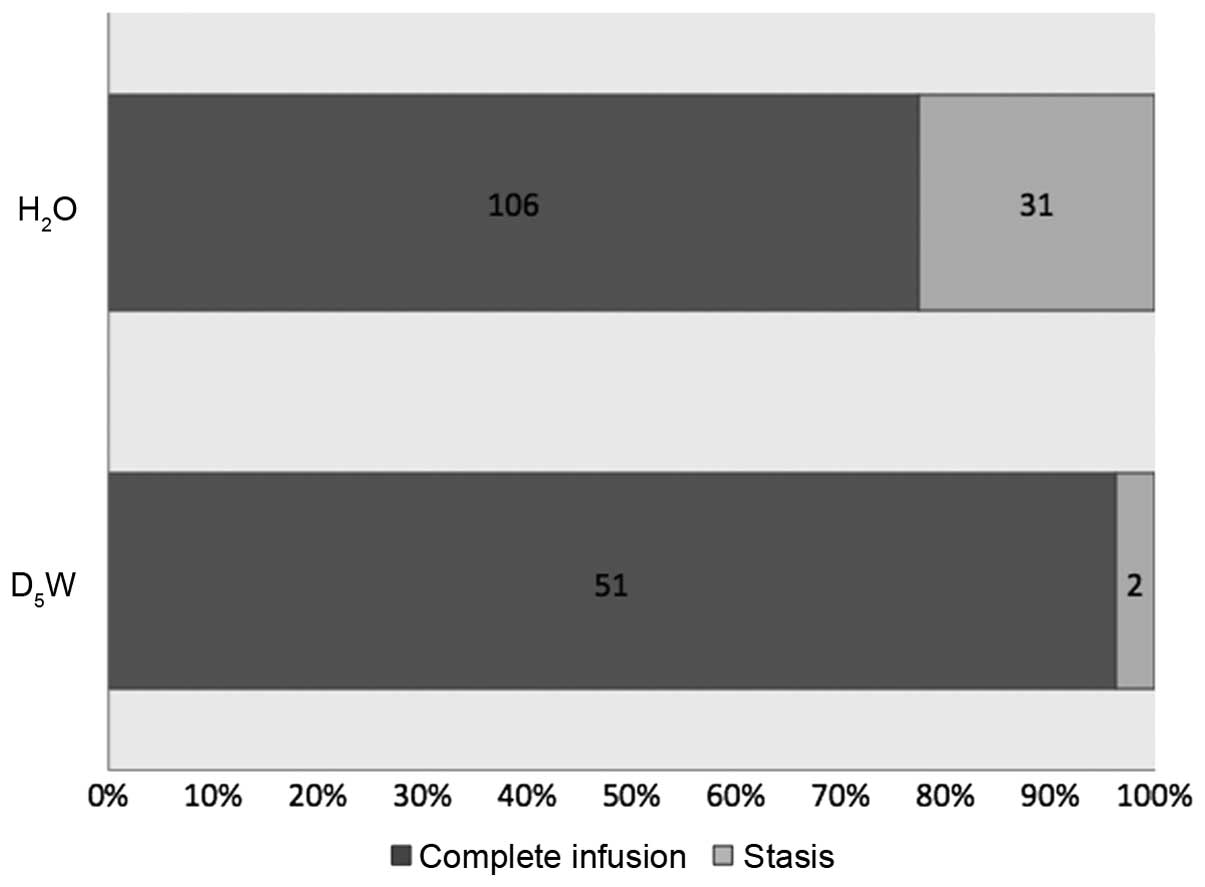
stasis events broken down by tumor type are shown in Table I. Thirty-one of the 137 (23%)
H2O infusions developed stasis compared to 2 of the 53
infusions (4%) with D5W (z=3.1, p=1.1E-3) (Fig. 1). The H2O group had a
significantly lower prescribed dose than that of the D5W
cohort [0.75 vs 1.04 millicuries (mCi), respectively; t=5.0,
p=1.1E-6] as demonstrated in Fig. 2A.
Finally, the H2O group had a significantly lower
percentage delivery of the prescribed dose compared to
D5W, as seen in Fig. 2B
(92.7 vs. 101.5%, respectively; t=3.8, p=2.2E-4). Over 97% of
completed infusions with H2O and D5W achieved
>90% delivery of prescribed activity while none of the infusions
with early stasis reached 90% delivery (Table II). No patients in either group
developed gastrointestinal signs/symptoms of ulceration.
 | Table I.Breakdown of infusion regimens and
stasis events by tumor type. |
Table I.
Breakdown of infusion regimens and
stasis events by tumor type.
| Variables | H2O
patient | H2O
infusions | Stasis events | Stasis (%) | D5W
patients | D5W
infusions | Stasis events | Stasis (%) |
|---|
| Total | 78 | 137 | 31 | 22.6 | 34 | 53 | 2 | 3.8 |
| Uveal melanoma | 43 | 78 | 12 | 15.4 | 0 | 0 | N/A | N/A |
| Neuroendocrine | 5 | 9 | 6 | 67 | 14 | 23 | 0 | 0 |
| Colorectal
carcinoma | 14 | 22 | 9 | 40.9 | 8 | 11 | 1 | 9.1 |
| Breast
carcinoma | 3 | 7 | 1 | 14.3 | 3 | 4 | 0 | 0 |
| Hepatocellular
carcinoma | 5 | 7 | 1 | 14.3 | 0 | 0 | N/A | N/A |
|
Cholangio-carcinoma | 2 | 4 | 0 | 0 | 3 | 4 | 1 | 25 |
| Other | 6 | 10 | 2 | 20 | 6 | 11 | 0 | 0 |
| Table II.Percent delivery of resin Y90 with
and without early stasis. |
Table II.
Percent delivery of resin Y90 with
and without early stasis.
| Delivery percentage
(%) | Early stasis
(%) | No stasis (%) |
|---|
| <50 | 12/33 (36) | 0/157 (0) |
| 50–75 | 10/33 (30) | 0/157 (0) |
| 76–90 | 11/33 (33) | 4/157 (3) |
| 90–100 | 0/33 (0) | 153/157 (97) |
Discussion
Delivery of resin Y90 microspheres with
D5W rather than H2O significantly reduces the
rates of early arterial stasis. Improved delivery was achieved
despite the D5W group being prescribed significantly
greater activity, which could have actually increased the risk of
stasis. We also achieved more complete delivery of resin Y90
microspheres with D5W compared to H2O. In all
the stasis events using either D5W or H2O,
administered activity was ≥10% less than the prescribed activity.
Although both glass and resin microsphere have been used to
palliate patients with common metastatic tumors such as colorectal
and breast cancer, the efficacy of glass microspheres was
significantly decreased with the increasing tumor burden (5,8,9). The number of microspheres in a 3 GBq
resin vial can be ≤80-fold greater than the same activity of glass
spheres based on the time from calibration (1). Potentially, resin Y90 can better saturate
larger tumors and improve outcomes given the greater number of
microspheres with preferential clustering in the viable,
hypervascular portion of target masses (10). However, the theoretical benefit of more
complete tumor coverage has been incompletely realized as
incomplete delivery of the prescribed activity potentially
decreases efficacy or the result in earlier time to
progression.
Although there is a known 21% incidence of early
stasis with H2O, the etiology remains largely
unexplained (4). In vivo use of
H2O can result in intravascular hemolysis (11). The Food and Drug Administration
reported 10 hemolysis cases in 1999, following dilution of 25%
albumin to 5% using H2O for plasmapheresis (11). The hypotonicity of the resulting
infusion resulted in acute renal failure in five patients and death
in one patient. Red blood cells lyse in hypotonic solutions such as
those created with H2O (12). The release of intracellular contents
following hemolysis expends endothelial nitric oxide, which
increases the vasomotor tone (13–15). The end
result of these events could include increased vascular spasm
resulting in early stasis or in situ thrombosis, which is
seen in other entities associated with hemolysis such as paroxysmal
nocturnal hemoglobinuria or esophageal dysmotility (16,17).
Previous research evaluated other potential risk
factors contributing to early arterial stasis without finding a
significant correlation (4).
Considerations included relative tumor vascularity at
cross-sectional imaging and previous intra-arterial therapy.
However, neither of these factors affected stasis rates. Notably,
the main limiting factor in the majority of stasis events with
resin microspheres is use of H2O. Tumors that appear
hypovascular on computed tomography or magnetic resonance imaging
are frequently hypervascular at angiography (18). We also perform chemoembolization using
techniques associated with maximal long-term arterial patency
(19). The findings of Chao et
al, support the limitations of H2O (20). They described a reduction in early
stasis from 15% with H2O to 4.5% with dilute contrast
[Chao et al (20) presented at
the 2014 Society of Interventional Radiology Annual Scientific
Meeting]. Direct comparisons of D5W and dilute contrast
have not been reported. While dilute contrast allows real-time
monitoring of vascular patency and possible reflux into non-target
arteries, we did not have any gastrointestinal toxicities using
D5W with intermittent contrast injection in our
group.
There are several important limitations to this
study. First, our data are retrospective and include a variety of
tumor types. However, as patients were treated consecutively with
each delivery vehicle, the potential for selection bias is unlikely
to have altered results in either direction. Furthermore, previous
findings have has not shown any difference in stasis based on
treatment/tumor history (4). Second,
our sample size reflects that of a single approach to prescribing
and infusing resin Y90. A multi-center study is necessary to
substantiate these findings. Finally, the impact of early stasis on
efficacy remains uncertain, and should be explored in future
studies.
In summary, D5W performs superiorly to
H2O to deliver resin microspheres with lower rates of
early arterial stasis and greater delivered activity. Future
research may evaluate differences between D5W and dilute
contrast. Based on our findings, practitioners should eliminate use
of H2O when performing resin microsphere infusion.
Acknowledgements
The authors would like to acknowledge Marni L.
Gardner, DPh and Jeffrey A. Clanton, MS, DPh, BCNP for their
assistance in dose preparation and patient care.
Glossary
Abbreviations
Abbreviations:
|
Y90
|
Yttrium-90
|
|
Bq
|
Becquerel
|
|
H2O
|
water
|
|
D5W
|
5% dextrose in water
|
|
BSA
|
body surface area
|
|
Vtumor
|
volume tumor
|
|
Vliver
|
volume liver
|
References
|
1
|
Lewandowski RJ, Sato KT, Atassi B, Ryu RK,
Nemcek AA Jr, Kulik L, Geschwind JF, Murthy R, Rilling W, Liu D, et
al: Radioembolization with 90Y microspheres: Angiographic and
technical considerations. Cardiovasc Intervent Radiol. 30:571–592.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Murthy R, Xiong H, Nunez R, Cohen AC,
Barron B, Szklaruk J, Madoff DC, Gupta S, Wallace MJ, Ahrar K, et
al: Yttrium 90 resin microspheres for the treatment of unresectable
colorectal hepatic metastases after failure of multiple
chemotherapy regimens: Preliminary results. J Vasc Interv Radiol.
16:937–945. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stuart JE, Tan B, Myerson RJ,
Garcia-Ramirez J, Goddu SM, Pilgram TK and Brown DB: Salvage
radioembolization of liver-dominant metastases with a resin-based
microsphere: Initial outcomes. J Vasc Interv Radiol. 19:1427–1433.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Piana PM, Bar V, Doyle L, Anne R, Sato T,
Eschelman DJ, McCann JW, Gonsalves CF and Brown DB: Early arterial
stasis during resin-based yttrium-90 radioembolization: Incidence
and preliminary outcomes. HPB Oxf. 16:336–341. 2014. View Article : Google Scholar
|
|
5
|
Saxena A, Meteling B, Kapoor J, Golani S,
Morris DL and Bester L: Is yttrium-90 radioembolization a viable
treatment option for unresectable, chemorefractory colorectal
cancer liver metastases? A large single-center experience of 302
patients. Ann Surg Oncol. 22:794–802. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
van Hazel GA, Heinemann V, Sharma NK,
Findlay MP, Ricke J, Peeters M, Perez D, Robinson BA, Strickland
AH, Ferguson T, et al: SIRFLOX: Randomized phase III trial
comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus
mFOLFOX6 (plus or minus bevacizumab) plus selective internal
radiation therapy in patients with metastatic colorectal cancer. J
Clin Oncol. 34:1723–1731. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Food and Drug Administration, . Available
at. http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/PMAApprovals/ucm431264.htmAccessed
on June 15, 2016.
|
|
8
|
Gordon AC, Gradishar WJ, Kaklamani VG,
Thuluvath AJ, Ryu RK, Sato KT, Gates VL, Salem R and Lewandowski
RJ: Yttrium-90 radioembolization stops progression of targeted
breast cancer liver metastases after failed chemotherapy. J Vasc
Interv Radiol. 25:1523–1532, 1532. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lewandowski RJ, Memon K, Mulcahy MF,
Hickey R, Marshall K, Williams M, Salzig K, Gates VL, Atassi B,
Vouche M, et al: Twelve-year experience of radioembolization for
colorectal hepatic metastases in 214 patients: Survival by era and
chemotherapy. Eur J Nucl Med Mol Imaging. 41:1861–1869. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kennedy AS, Nutting C, Coldwell D, Gaiser
J and Drachenberg C: Pathologic response and microdosimetry of
(90)Y microspheres in man: Review of four explanted whole livers.
Int J Radiat Oncol Biol Phys. 60:1552–1563. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pierce LR, Gaines A, Finlayson JS,
Varricchio F and Epstein JS: Hemolysis and acute renal failure due
to the administration of albumin diluted in sterile water.
Transfusion. 39:110–111. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ramaswamykanive H and Greaves J:
Intravenous infusion of sterile water for the treatment of
hypernatraemia. Anaesth Intensive Care. 42:258–262. 2014.PubMed/NCBI
|
|
13
|
Liao JC, Hein TW, Vaughn MW, Huang KT and
Kuo L: Intravascular flow decreases erythrocyte consumption of
nitric oxide. Proc Natl Acad Sci USA. 96:8757–8761. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Vaughn MW, Huang KT, Kuo L and Liao JC:
Erythrocytes possess an intrinsic barrier to nitric oxide
consumption. J Biol Chem. 275:2342–2348. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rother RP, Bell L, Hillmen P and Gladwin
MT: The clinical sequelae of intravascular hemolysis and
extracellular plasma hemoglobin: A novel mechanism of human
disease. JAMA. 293:1653–1662. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Clark DA, Butler SA, Braren V, Hartmann RC
and Jenkins DE Jr: The kidneys in paroxysmal nocturnal
hemoglobinuria. Blood. 57:83–89. 1981.PubMed/NCBI
|
|
17
|
Hirsch DP, Holloway RH, Tytgat GN and
Boeckxstaens GE: Involvement of nitric oxide in human transient
lower esophageal sphincter relaxations and esophageal primary
peristalsis. Gastroenterology. 115:1374–1380. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sato KT, Omary RA, Takehana C, Ibrahim S,
Lewandowski RJ, Ryu RK and Salem R: The role of tumor vascularity
in predicting survival after yttrium-90 radioembolization for liver
metastases. J Vasc Interv Radiol. 20:1564–1569. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Geschwind JF, Ramsey DE, Cleffken B, van
der Wal BC, Kobeiter H, Juluru K, Hartnell GG and Choti MA:
Transcatheter arterial chemoembolization of liver tumors: Effects
of embolization protocol on injectable volume of chemotherapy and
subsequent arterial patency. Cardiovasc Intervent Radiol.
26:111–117. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chao C, Dagli M, Mondschein J,
Stavropoulos W, Sudheendra D, Nadolski G, et al: Effect of
substituting 50% issue for sterile water as the delivery medium for
SIR-SPHERES: Improved dose delivery and decreased incidence of
stasis. J Vasc Interv Radiol. 2:S892014. View Article : Google Scholar
|