Introduction
Neonatal hypoxic-ischemic encephalopathy (HIE) may
result from diffuse hypoxic-ischemic brain injury (1). It is one of the most common causes of
cerebral palsy and other permanent neurological deficits in
children (2,3). Therefore, a brain computed tomography
(CT) scan is commonly used in the screening and diagnosis of HIE.
However, newborns are far more radiosensitive than adults and
suffer from potentially more serious injury. Therefore, the use of
reduced radiation doses in neonatal CT scans is an important area
of research in contemporary imaging technology (4). A 256-slice CT scanner has the fastest
rotation speed and a novel detector, which guarantees lower
radiation doses during examination (5). The aim of the present study was to
assess the overall image quality and clinical value of 256-slice
spiral CT with low radiation doses in the imaging of neonatal
brains with suspected HIE.
Patients and methods
Clinical data
From March 2011 to March 2012, 150 newborns from
Qilu Hospital (Jinan, China) were selected. There were 88 male and
62 female subjects, including 95 full-term and 55 premature cases.
The gestational age was between 28–40 weeks and the birth weight
ranged from 1,650 to 3,150 g. The newborns included 111 babies born
via natural labor, while the remaining 39 cases were delivered by
caesarean section. All parents/guardians of patients signed consent
forms and all procedures were reviewed and approved by the Ethic
Committee at the Qilu Hospital of Shandong University (Jinan,
China).
Methods
The CT scanner used in this study was a Philips
Brilliance 256-slice spiral CT (Philips Medical Systems, Amsterdam,
The Netherlands). This scanner automatically displays the CT
dose-weighted index (CTDI) and dose-length product (DLP) during
scanning.
Acquisition parameters
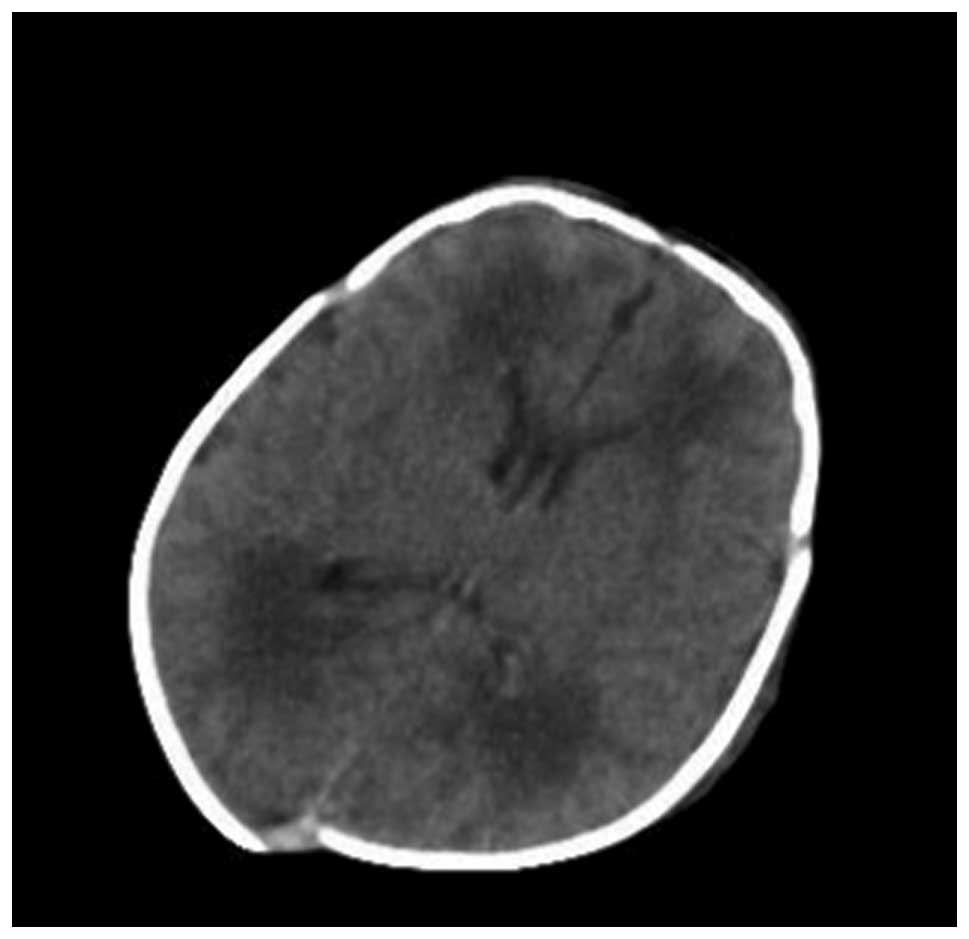
All patients were randomly divided into three groups
according to the radiation dose, as follows: standard dose group
(Fig. 1) with 120 Kv, 250 mAsec;
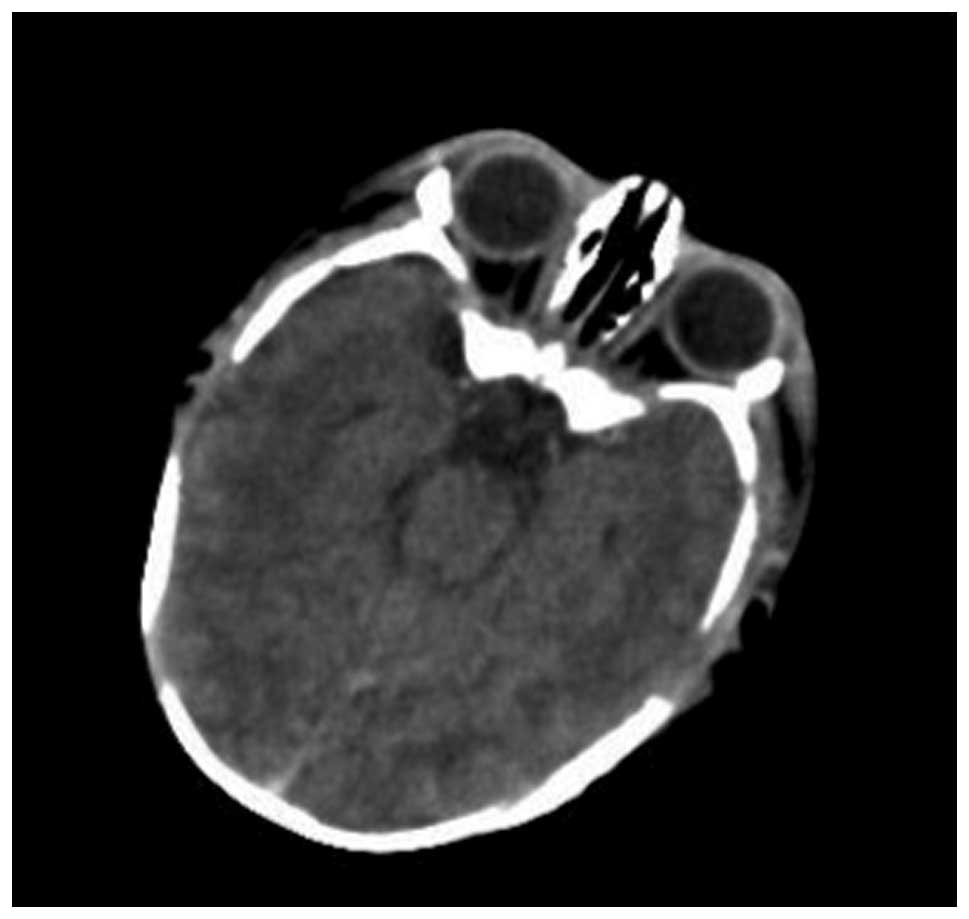
low dose group 1 (Fig. 2) with 120
Kv, 150 mAsec and low dose group 2 (Fig. 3) with 120 Kv, 50 mAsec. The slice
thickness was 5 mm and the interlayer spacing was 5 mm. The newborn
was placed in a supine position and a full brain scan was
performed.
The CTDI and DLP were recorded from the scanner
display. Since the DLP is related to the scanning range, the CTDI
and DLP of the standard dose and low dose CT at the same scan
length were also recorded. The CT values in the left basal ganglia
were also measured by drawing the region of interest (ROI).
Image quality assessment
The images were blindly assessed by two experienced
physicians. The evaluation criteria were as follows: score 3, no
image artifacts, sharp edges of the skull, good contrast between
the gray and white matter, clear ventricle edge and clear lesions;
score 2, some image artifacts and a lower signal-to-noise ratio,
but the reduced image quality did not affect the overall diagnosis;
and score 1, images had a greater amount of noise and the lesions
were not clearly delineated, potentially making an accurate
diagnosis challenging and complicated.
Statistical analysis
The CTDI, DLP, signal noise and image quality were
compared among the three groups. Data are presented as mean ±
standard deviation (SD). SPSS 13.0 software (SPSS Inc., Chicago,
IL, USA) was used to perform statistical analyses. P<0.05 was
considered to indicate a statistically significant difference.
Results
Image quality rating
The image quality scores in the standard dose group,
low dose group 1 and low dose group 2 were 2.55±0.29, 2.25±0.41 and
2.05±0.74, respectively. There was no statistical difference in the
image quality rating among the three groups (P>0.05).
Noise
The signal noise levels of the ROI in the standard
dose group, low dose group 1 and low dose group 2 were 1.78±0.42,
1.95±0.35 and 2.36±0.49 HU, respectively. The measured noise levels
of the groups were significantly different (P<0.05; Table I).
 | Table IParameters and results of computed
tomography (CT) scanning. |
Table I
Parameters and results of computed
tomography (CT) scanning.
| Group | kV | mAsec | CTDI (mGy.cm) | DLP (mGy) | Signal noise
(HU) | Image quality (mean ±
SD) |
|---|
| Standard dose | 120 | 250 | 30.4 | 311.6 | 1.78±0.42 | 2.55±0.29 |
| Low dose group 1 | 120 | 150 | 24.8 | 109.7 | 1.95±0.35 | 2.25±0.41 |
| Low dose group 2 | 120 | 50 | 6.2 | 60.2 | 2.36±0.49 | 2.05±0.74 |
Radiation dose
In the standard dose group, low dose group 1, and
low dose group 2, the DLPs were 311.6, 109.7 and 60.2 mGy
respectively. The DLP in low dose group 1 was 35.2% of the DLP in
the standard dose group, and the DLP in low dose group 2 was 19.3%
of the DLP in the standard dose group. A reduction in the radiation
dose resulted in a decline in the DLP value. However, this did not
affect the image quality. Although the image noise was relatively
high in low dose group 2 (Fig. 3),
intracranial structures and lesions were clearly delineated. The
window and level settings may be adjusted to generate a diagnostic
image.
Discussion
Low dose CT scanning is currently used in a variety
of clinical applications. The successful application of low dose CT
scanning requires a good natural contrast between the skull, brain
tissue and the ventricular system. In the present study, we reduced
the radiation dose in multi-slice spiral CT scanning of the newborn
brain without compromising the image quality. The appropriate dose
ensures that the image has adequate contrast between normal brain
structures and lesions in order to make a correct clinical
diagnosis.
Multidetector CT (MDCT) achieves a larger volume of
data acquisition, which broadens the applications of CT and
improves the diagnostic level. 256-Slice CT scanning adopts
conventional technology for the processing of high-speed data, but
reduces the electronic noise in the image chain (6). This improves the signal-to-noise
ratio and may ultimately reduce the X-ray dose. It also improves
the image quality to a certain extent, by compensating for a
reduction in image quality due to the increased noise, which may
reduce the radiation damage to patients. Consequently, 256-slice
spiral CT may be used in the study of newborns with suspected HIE.
The results of the current study demonstrated that there was no
diagnostic difference in the image quality between low dose and
conventional dose CT scanning (P>0.05).
The higher the applied X-ray dose used during a CT
scan, the greater the likelihood of radiation damage. A previous
study demonstrated that after receiving the same radiation dose,
the risk of brain tumors and leukemia in children is much higher
compared with that in adults, and younger children have a greater
risk (7). Due to the specificity
of neonatal physiology, children are likely to be exposed to larger
doses and potentially develop more radiation damage than adults
under the same scanning conditions. Therefore, the parameters of CT
examination for children and newborns should be adjusted
accordingly. Also, a smaller field of view and collimator should be
used (8). Reducing the radiation
dose in CT scanning is the main goal in protecting the neonatal
brain. In the present study, the DLP in the lowest dose group was
~80% lower than that in the standard dose group (60.2 vs. 311.6
mGy). The CT images were all of diagnostic quality and the newborn
brain was protected. In summary, a 256-slice CT scan using a lower
radiation dose may be used to safely screen the neonatal brain
without a reduction in the overall image quality.
References
|
1
|
McKinney AM, Teksam M, Felice R, et al:
Diffusion-weighted imaging in the setting of diffuse cortical
laminar necrosis and hypoxic-ischemic encephalopathy. AJNR Am J
Neuroradiol. 25:1659–1665. 2004.PubMed/NCBI
|
|
2
|
Fee SC, Malee K, Deddish R, et al: Severe
acidosis and subsequent neurologic status. Am J Obstet Gynecol.
162:802–806. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ferrari F, Todeschini A, Guidotti I, et
al: General movements in full-term infants with perinatal asphyxia
are related to Basal Ganglia and thalamic lesions. J Pediatr.
158:904–911. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Berrington de González A, Mahesh M, Kim
KP, et al: Projected cancer risks from computed tomographic scans
performed in the United States in 2007. Arch Int Med.
169:2071–2077. 2009.PubMed/NCBI
|
|
5
|
Mori S, Endo M, Nishizawa K, et al:
Comparison of patient doses in 256-slice CT and 16-slice CT
scanners. Br J Radiol. 79:56–61. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Endo M, Mori S, Tsunoo T and Miyazaki H:
Magnitude and effects of x-ray scatter in a 256-slice CT scanner.
Med Phys. 33:3359–3368. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pearce MS, Salotti JA, Little MP, et al:
Radiation exposure from CT scans in childhood and subsequent risk
of leukaemia and brain tumours: a retrospective cohort study.
Lancet. 380:499–505. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Strauss KJ, Goske MJ, Kaste SC, et al:
Image gently: ten steps you can take to optimize image quality and
lower CT dose for pediatric patients. AJR Am J Roentgenol.
94:868–873. 2010. View Article : Google Scholar : PubMed/NCBI
|