Article
Computed tomography angiography manifestations of collateral circulations in Budd-Chiari syndrome
- Authors:
- Shi‑Feng Cai
- Yong‑Hao Gai
- Qing‑Wei Liu
-
View Affiliations / Copyright
Affiliations:
Department of Radiology, Provincial Hospital Affiliated to Shandong University, Jinan, Shandong 250021, P.R. China, Department of Ultrasound, Provincial Hospital Affiliated to Shandong University, Jinan, Shandong 250021, P.R. China
-
Pages:
399-404
|
Published online on:
December 10, 2014
https://doi.org/10.3892/etm.2014.2125
- Expand metrics +
Metrics:
Total
Views: 0
(Spandidos Publications: | PMC Statistics:
)
Metrics:
Total PDF Downloads: 0
(Spandidos Publications: | PMC Statistics:
)
This article is mentioned in:
Abstract
The aim of this study was to assess the computed tomography angiography (CTA) manifestations of collateral circulations in patients with Budd‑Chiari syndrome (BCS). Eighty patients with BCS were examined by CT scan. Using the CTA images of the relevant blood vessels, including the affected hepatic veins (HVs) and inferior venae cavae (IVCs), the collateral circulations were reconstructed. In addition to obstructed HVs and IVCs, collateral circulations were found in each of the patients. The collateral circulations were classified as intrahepatic, extrahepatic and portosystemic pathways. Intrahepatic collateral pathways were further classified as the following six types: HV‑accessory HV (n=51, 63.8%), HV‑HV (n=6, 7.5%), HV‑accessory HV plus HV (n=6, 7.5%), IVC‑HV/accessory HV‑HV‑right atrium (n=5, 6.3%), HV‑umbilical vein (n=4, 5.0%) and HV‑inferior phrenic vein (n=8, 10.0%). Extrahepatic collateral pathways included IVC‑lumbar‑ascending lumbar‑hemiazygos/azygos vein (n=80, 100.0%), IVC‑left renal‑ascending lumbar‑hemiazygos vein (n=75, 93.8%), IVC‑left renal‑inferior phrenic vein (n=49, 61.3%), IVC‑renal ‑peri‑renal ‑superficial epigastric vein (n=26, 32.5%) and superficial epigastric vein (n=12, 15.0%) types. The CTA characteristics of each type of collateral circulation were demonstrated. In conclusion, the present study revealed that CTA is able to show the intra- and extrahepatic collateral circulations of patients with BCS, which may be useful for therapeutic planning.
View Figures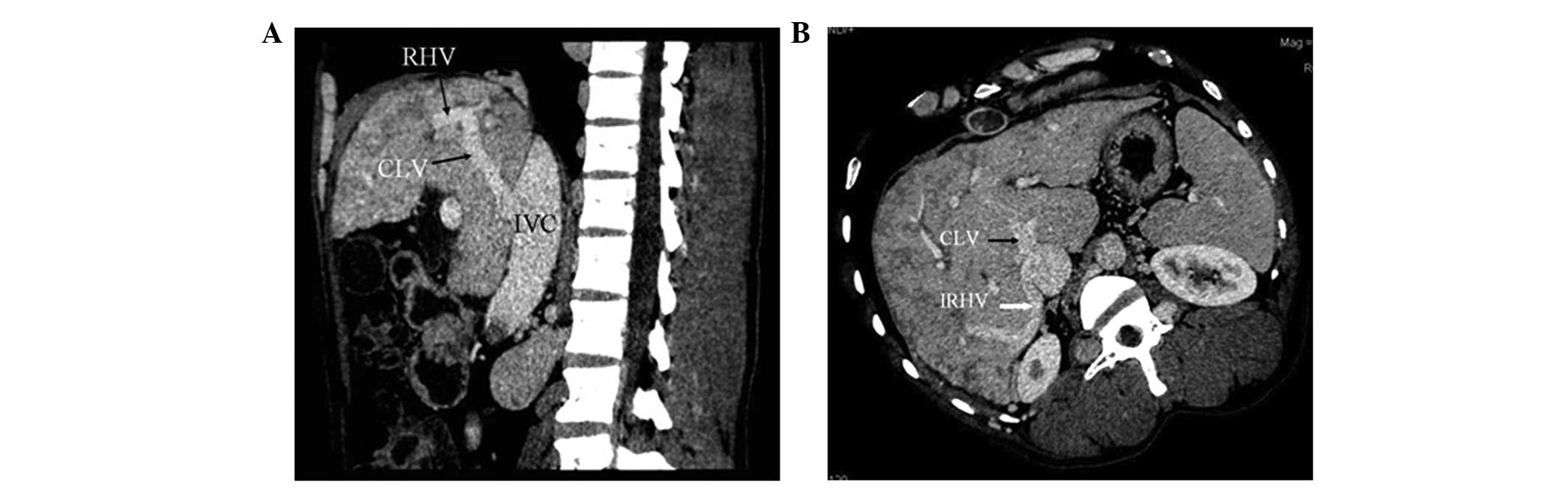 |
Figure 1
|
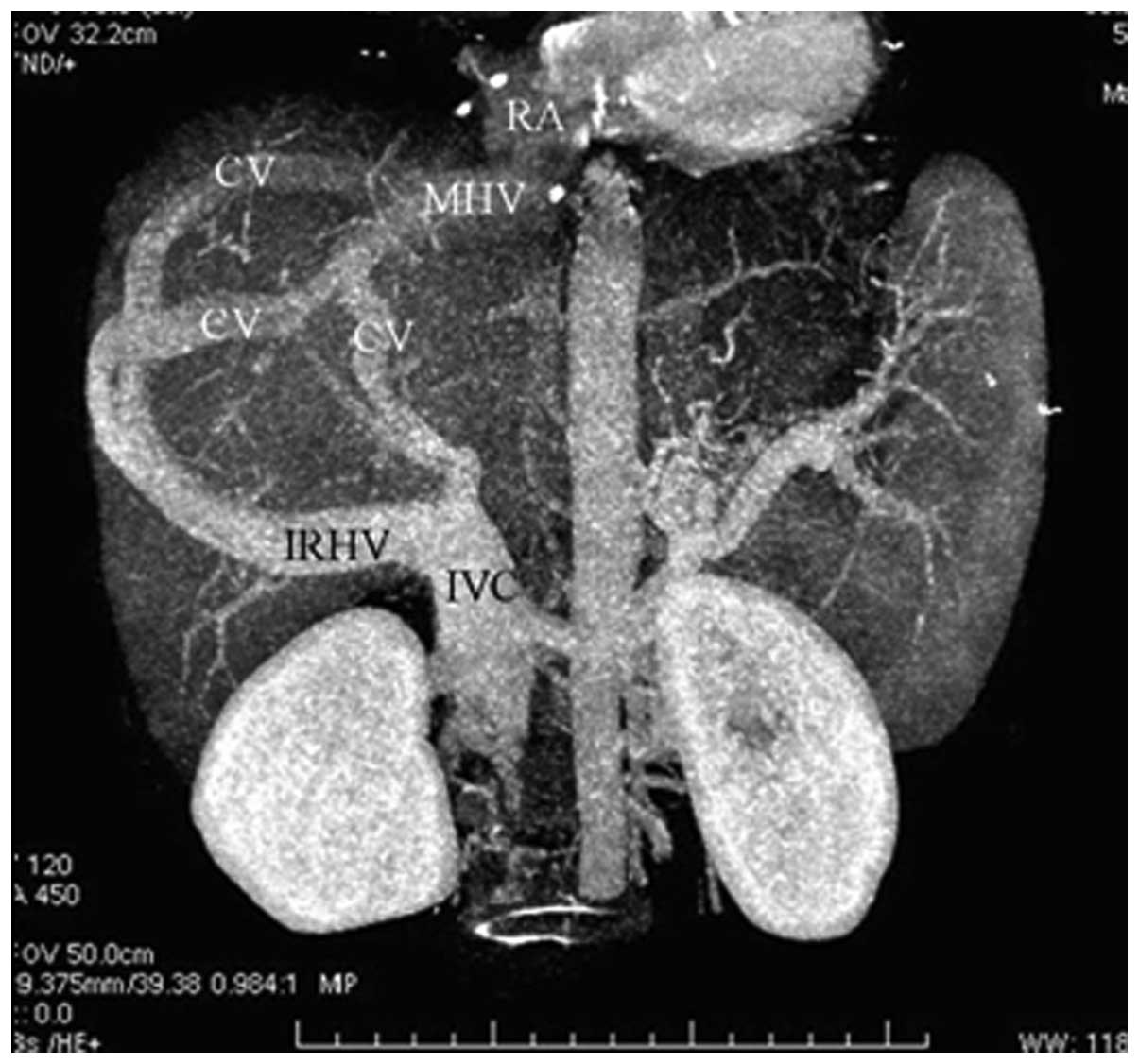 |
Figure 2
|
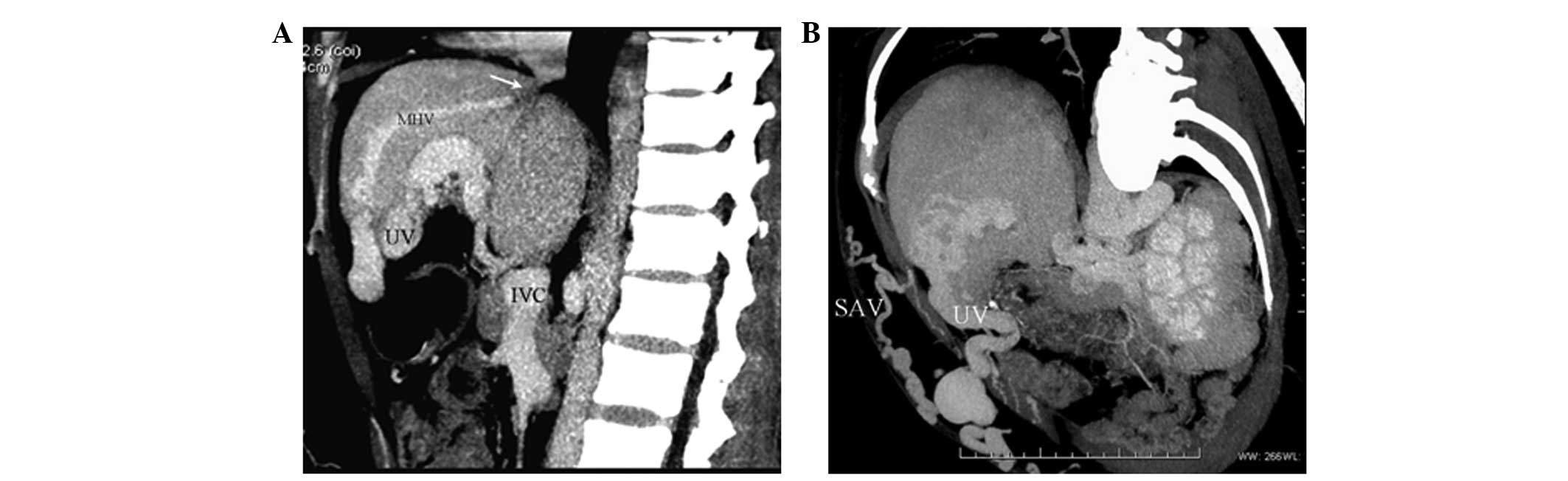 |
Figure 3
|
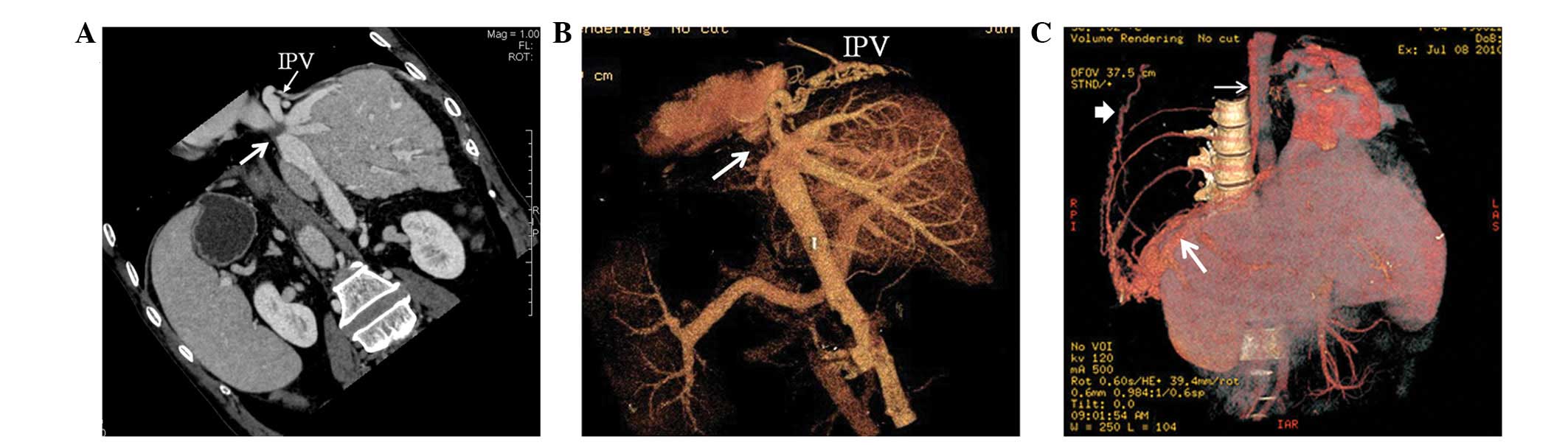 |
Figure 4
|
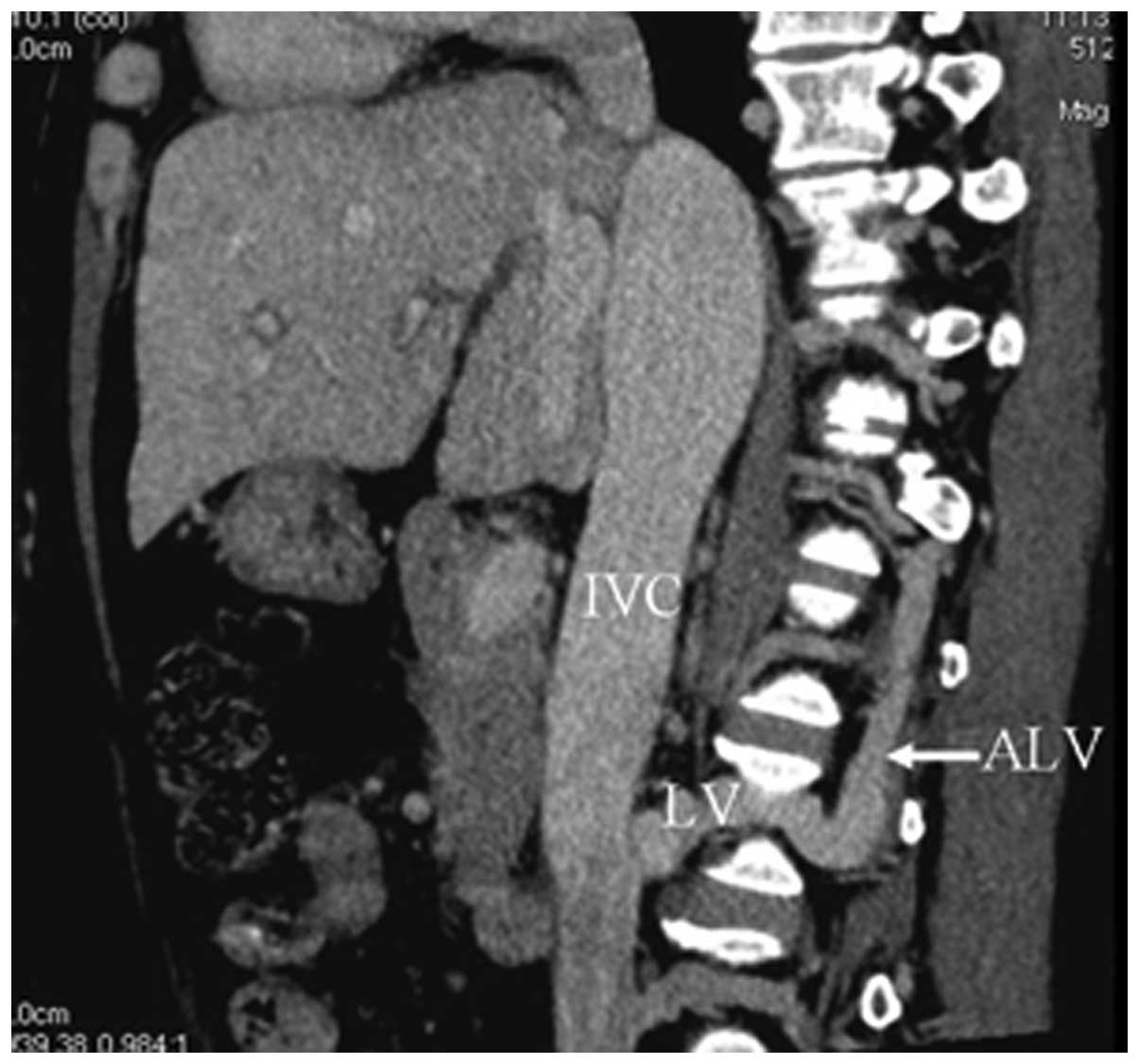 |
Figure 5
|
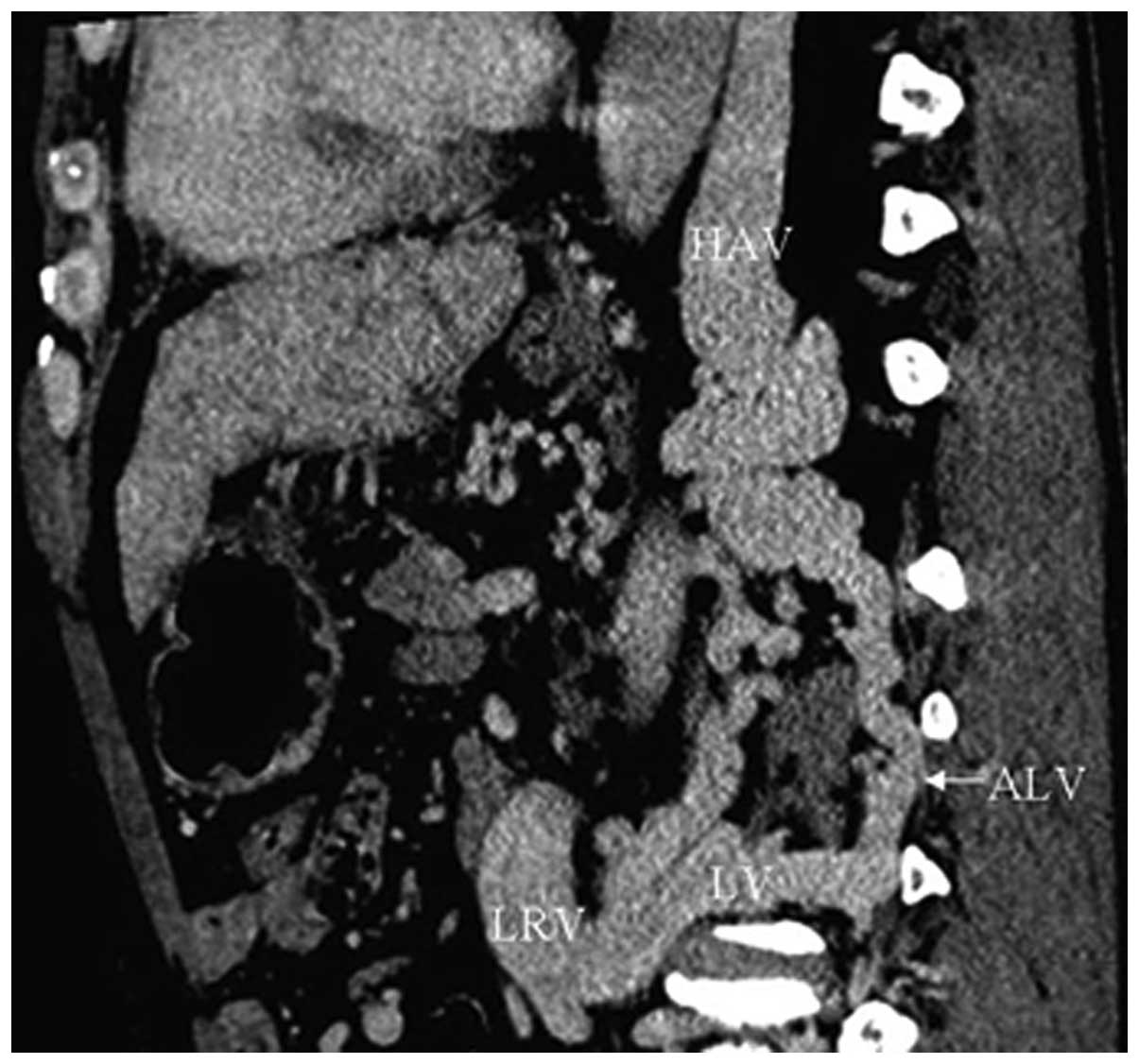 |
Figure 6
|
 |
Figure 7
|
 |
Figure 8
|
 |
Figure 9
|
 |
Figure 10
|
View References
|
1
|
Janssen HL, Garcia-Pagan JC, Elias E, et
al: European Group for the Study of Vascular Disorders of the
Liver: Budd-Chiari syndrome: a review by an expert panel. J
Hepatol. 38:364–371. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bogin V, Marcos A and Shaw-Stiffel T:
Budd-Chiari syndrome: in evolution. Eur J Gastroenterol Hepatol.
17:33–35. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gai YH, Cai SF, Guo WB, Zhang CQ, Liang B,
Jia T and Zhang GQ: Sonographic classification of draining pathways
of obstructed hepatic veins in Budd-Chiari syndrome. J Clin
Ultrasound. 42:134–142. 2014. View Article : Google Scholar
|
|
4
|
Bargalló X, Gilabert R, Nicolau C, et al:
Sonography of Budd-Chiari Syndrome. AJR Am J Roentgenol.
187:W33–W41. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kanamura T, Murakami G, Hirai I, et al:
High dorsal drainage routes of Spiegel’s lobe. J Hepatobiliary
Pancreat Surg. 8:549–556. 2001. View Article : Google Scholar
|
|
6
|
Bargalló X, Gilabert R, Nicolau C, et al:
Sonography of the caudate vein: value in diagnosing Budd-Chiari
syndrome. AJR Am J Roentgenol. 181:1641–1645. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Xing X, Li H and Liu WG: Clinical studies
on inferior right hepatic veins. Hepatobiliary Pancreat Dis Int.
6:579–584. 2007.PubMed/NCBI
|
|
8
|
Gabella G: Hepatic vein. Gray’s Anatomy.
Williams PL and Bannister LH: 38th edition. Churchill Livingstone;
London: pp. 16021995
|
|
9
|
Kapur S, Paik E, Rezaei A and Vu DN: Where
there is blood, there is a way: unusual collateral vessels in
superior and inferior vena cava obstruction. Radiographics.
30:67–78. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nakamura S and Tsuzuki T: Surgical anatomy
of the hepatic veins and the inferior vena cava. Surg Gynecol
Obstet. 152:43–50. 1981.PubMed/NCBI
|
|
11
|
Ueda K, Matsui O, Kadoya M, et al: CTAP in
Budd-Chiari syndrome: evaluation of intrahepatic portal flow. Abdom
Imaging. 23:304–308. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Karaosmanoglu D, Karcaaltincaba M, Akata
D, Ozmen M and Akhan O: CT, MRI, and US findings of incidental
segmental distal hepatic vein occlusion: a new form of Budd-Chiari
syndrome? J Comput Assist Tomogr. 32:518–522. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Akaki S, Kanazawa S, Gochi A, et al:
Asymptomatic membranous obstruction of the inferior vena cava due
to large intrahepatic collaterals. Cardiovasc Intervent Ridio.
18:403–405. 1995. View Article : Google Scholar
|
|
14
|
Kamba M, Ochi S, Ochi H, et al:
Asymptomatic membranous obstruction of the inferior vena cava
forming intrahepatic collateral pathways. J Gastroenterol.
30:783–785. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gai YH, Cai SF, Fan HL and Liu QW:
Diagnosis of the cavo-hepato-atrial pathway in Budd-Chiari syndrome
by ultrasonography. Exp Ther Med. 8:793–796. 2014.PubMed/NCBI
|
|
16
|
Cho OK, Koo JH, Kim YS, et al: Collateral
pathways in Budd-Chiari syndrome: CT and venographic correlation.
AJR Am J Roentgenol. 167:1163–1167. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Edwards EA: Functional anatomy of the
porta-systemic communications. AMA Arch Intern Med. 88:137–154.
1951. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fleming RJ and Seaman WB: Roentgenographic
demonstration of unusual extra-esophageal varices. Am J Roentgenol
Radium Ther Nucl Med. 103:281–290. 1968. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Terasaki M, Kitai T, Morimoto T, et al:
Hemodynamics and hepatic energy metabolism in canine model of acute
hepatic venous occlusion with mesocaval shunt. Eur Surg Res.
26:19–27. 1994. View Article : Google Scholar : PubMed/NCBI
|














