Introduction
Wegener's granulomatosis (WG) is a necrotizing
granulomatous vasculitis that affects small arteries, veins and
capillaries. Occasionally, large arteries in the upper and lower
respiratory tract, and kidney are also involved. The joints, eyes
and skin may also be affected in certain cases (1).
The disease was described for the first time in 1931
(2). Subsequently, Wegener et
al described the disease in a more comprehensive manner
(3). In that study, the disease was
first described as a systemic, septic vascular disease (3). However, the cause of this disease is
unknown. The annual incidence is 0.4/10 million people. WG affects
all age groups, with the peak incidence in individuals aged 30–50
years. The prevalence is slightly elevated in males (4). Previously, the average survival time of
untreated Weneger's granulomatosis was 5 months, with 80% of the
patients succumbing to respiratory or renal failure within a year.
Additionally, >90% of the patients succumbed to the disease
within two years (5). At present the
majority of patients can have long-term relief under proper
treatment.
The disease is divided into systemic and limited
forms, depending on clinical manifestations (6). WG does not have unique symptoms.
General symptoms include fever, fatigue, and anemia. Specific
symptoms vary depending on the involved organ. Thus, the disease
may manifest in the upper respiratory tract with runny nose, nose
bleeds, nasal mucosa ulcers and nasal scab. Lower airway symptoms
include chest tightness, cough, and hemoptysis. Kidney involvement
manifests with proteinuria, hematuria, or renal insufficiency.
Ocular manifestations include blurred vision and decreased visual
acuity. Affected joints are marked by joint pain.
Due to its non-specific symptoms, WG is often
underrecognized or misdiagnosed in the clinic. In the current
study, we present three cases of WG to describe clinical and
pathological characteristics in order to improve the identification
of WG and reduce diagnostic errors.
Clinical cases
Ethics approval
Approval for the present study was obtained from The
First People's Hospital of Xuzhou (Jiangsu, China).
Case 1
A 40-year-old male patient presented to The First
People's Hospital of Xuzhou (Jiangsu, China) with a high
temperature, cough, and hemoptysis that lasted for >1 month
prior to admission to the Hospital. The patient was previously
diagnosed with tuberculous pleurisy in another hospital a year
earlier and received anti-tuberculosis drugs for 8 months.
Following admission, the patient was found to have a temperature of
39.2°C. Computerized tomography (CT) was performed, which revealed
multiple pulmonary nodules and irregular patchy shadows in both
lungs. The laboratory examination demonstrated positive serum
anti-neutrophil cytoplasmic and negative perinuclear (c- and
p-ANCA, respectively) staining.
A percutaneous CT-guided lung biopsy was obtained.
The biopsy specimen was fixed with 10% formalin and
paraffin-embedded. Sections (4 µm) were stained with hematoxylin
and eosin staining Maixin Biotechnology Co., Ltd. (Shanghai, China)
and observed under a light microscope Olympus CH30 (Tokyo, Japan).
Parallel slides were stained with periodic acid-Schiff and acid
fast staining, and evaluated under a microscope.
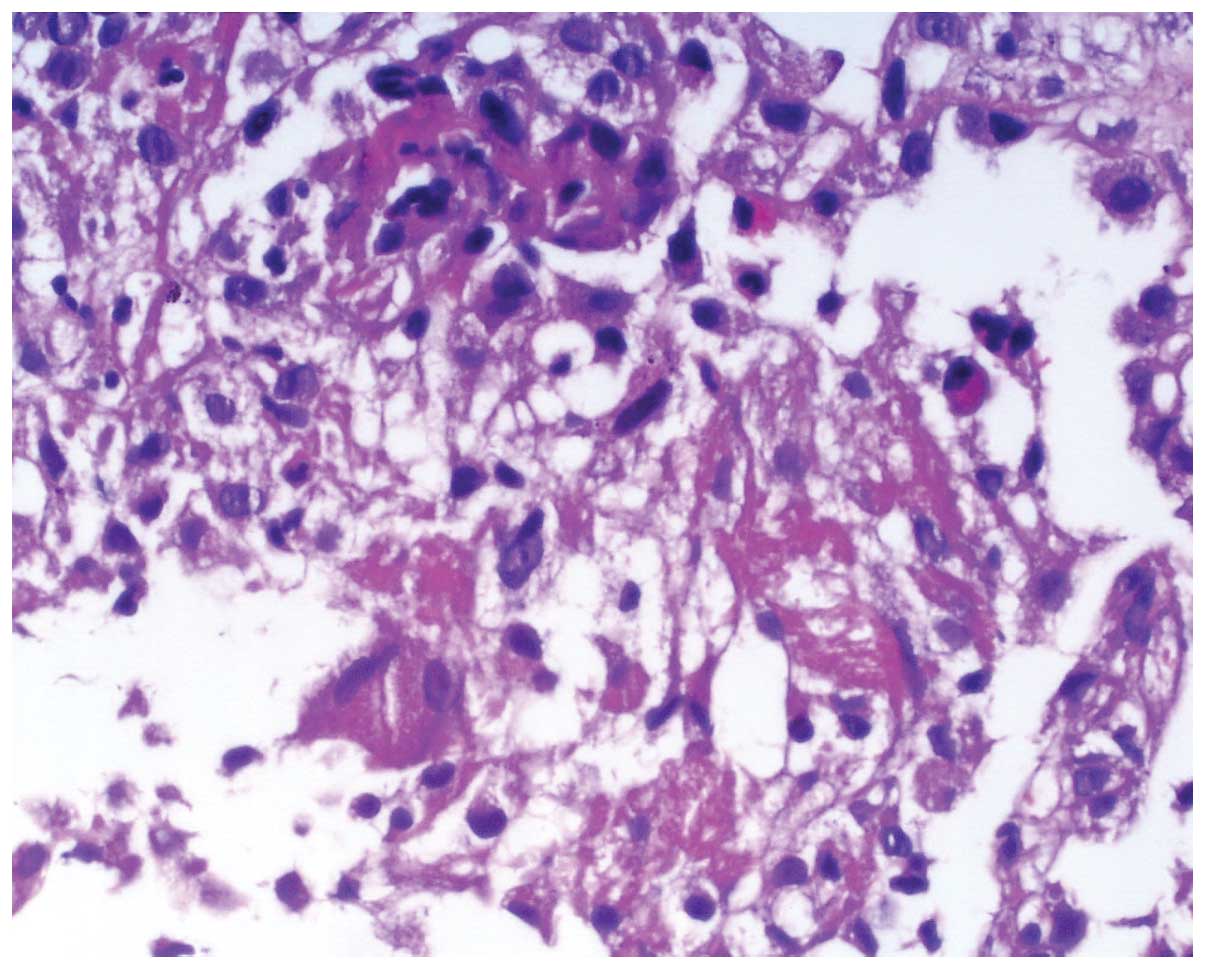
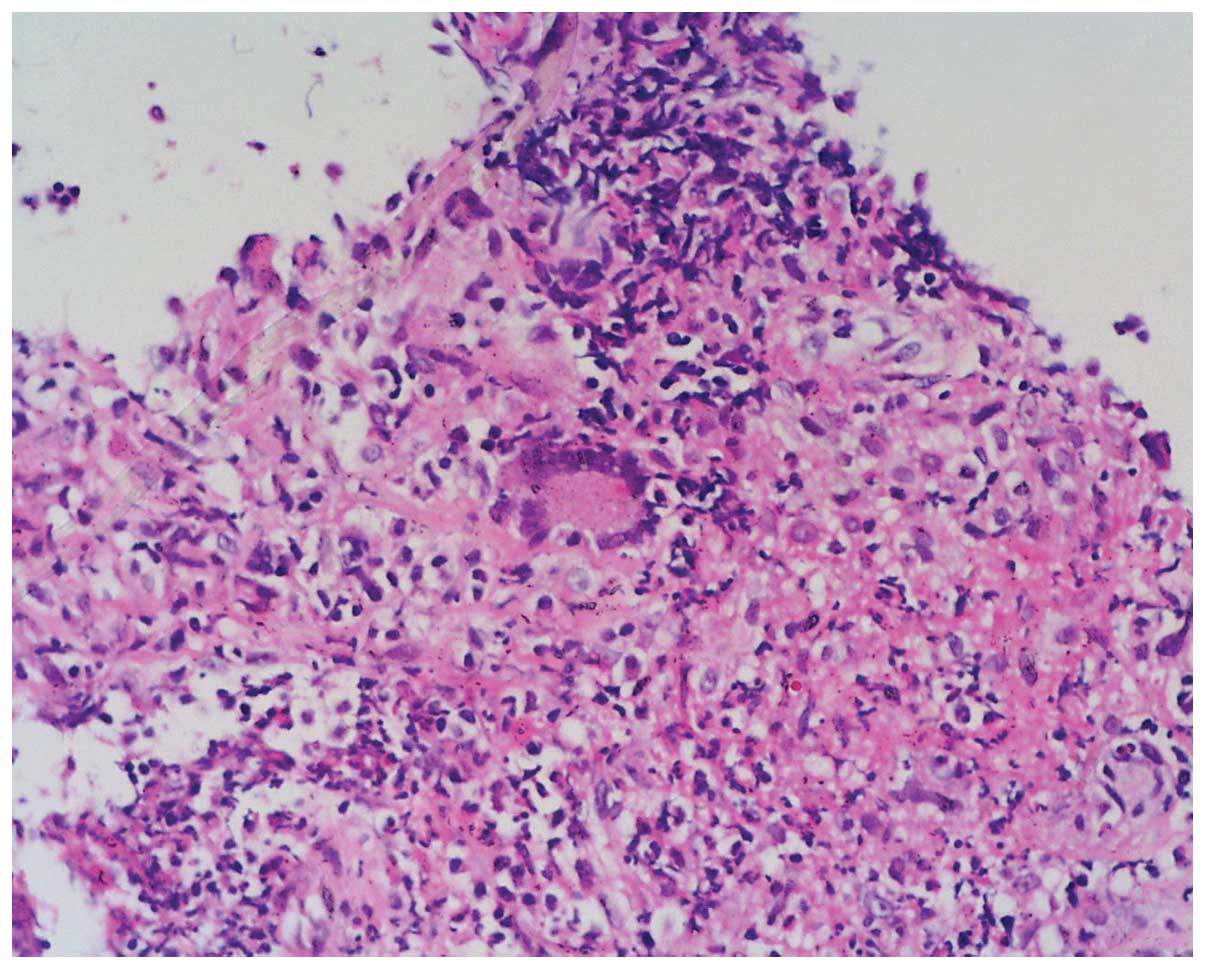
The lung biopsy yielded two blocks of 1×0.1×0.1 cm
of gray-white tissue. Microscopically, vascular cavity of the
alveolar septa showed stenosis and occlusion. Neutrophils and some
eosinophils infiltrated the vessel wall and adjacent region.
Visible lymphoplasmacytic scattered infiltration and red dye
fibrinoid deposits were evident. Unconspicuous granuloma formed by
few multinucleated giant cells with an organized structure were
identified in certain parts of the region (Figs. 1–3).
Thus, pathological diagnosis complied with the diagnosis of
ANCA-associated vasculitis (i.e., WG).
Case 2
A 66-year-old male patient reported having an
intermittent cough for 3 years. Over a month prior to admission to
the Hospital, the cough became hoarse. The patient's body
temperature was normal when he presented to the hospital. The
patient was laryngoscopically examined by an ENT specialist owing
to the hoarseness. A subglottic cauliflower neoformation with
proneness to hemorrhaging was observed. The glottis was narrow. The
vocal cord abduction was limited. A biopsy was performed and
assessed for laryngeal carcinoma. The CT revealed a number of
neoformations on the right nasal and maxillary sinuses, and
multiple pulmonary occupying lesions. A nasal neoplasm biopsy was
obtained by an ENT specialist. The laboratory examination revealed
positive serum p- and negative c-ANCA.
Gross examination of the biopsy of the glottis
revealed a bean-sized mass of pale gray-red broken tissue.
Microscopically, squamous epithelium showed hyperplasia in the
superficial areas, partial disappearance of epithelium, visible
necrosis, fibrin exudation, fibrinoid necrosis of parts of the
vascular wall, and neutrophil infiltration. Small multinucleated
giant cells were observed near the necrotic exudation (Figs. 4 and 5). Pathological diagnosis did not exclude
WG. Gross examination of the nasal biopsy demonstrated a mass of
ash-red and gray-white tissue with the size of 4×2.5×1 cm. Some
parts of the tissue were soft, while other parts flexible.
Microscopically, there were numerous lymphocytes, plasma cells and
neutrophils within the tissue. Fibrinoid necrosis was evident in
part of the vascular wall. Necrotic tissue was basophilic and
distributed in a patchy manner. Granuloma was formed by few
multinucleated giant cells, and was scattered or focally
distributed. Small suppurative foci formed in parts of the region
(Figs. 6 and 7). Based on the pathological findings, a WG
diagnosis was made which was confirmed by positive ANCA staining,
and negative fungal PAS and acid-fast staining.
Case 3
A 26-year-old male patient experienced bilateral
exophthalmos for >6 months prior to admission. Five days prior
to admission, the symptoms in the right eye worsened. The CT
revealed a tumor in the procuratorial right orbital area with
unclear border and uniform texture. The patient was diagnosed with
WG in another hospital and treated with prednisone (20 mg/day). The
right eye proptosis was aggravated after common colds. The
laboratory examination demonstrated negative serum p- and positive
c-ANCA.
Gross examination of the right orbital tumor
resection revealed a block of gray ash-red tissue with a sized of
3×2.5×1 cm, as well as a gray and pinkish-gray section. The texture
was flexible. Microscopically, there were lymphocytes, plasma cells
and neutrophils infiltrating the tissue, including fat tissue and
striated muscle. Part of the small vascular wall showed fibrinoid
necrosis. Patchy necrosis was basophilic. Partial necrosis was
distributed around the periphery of fibrinoid necrosis of small
vessels. The typical granulation-like structure comprised
multinucleated giant cells (Figs. 8
and 9). Pathological diagnosis
confirmed WG.
Treatment and prognosis
In all three patients, symptoms were relieved
following a large dose of hormone treatment. During the active
phase with prednisone (Weihai Disu Pharmaceutical Co., Ltd.,
China), 1.0 to 1.5 mg were administered once per day for 4–6 weeks.
When the disease was relieved, we reduced prednisone dose and
maintained in a small doses. The patients were discharged and
followed up for 6 months. All three patients recovered well.
Discussion
WG is a rare autoimmune disease that mainly affects
small vessels. Necrotizing vasculitis and granulomatous
inflammation are basic pathological characteristics of this
disease. WG is a multisystem disorder disease. Organ involvement
defines clinical manifestations (7).
The symptoms also include nasal and paranasal sinusitis, lung
disease and progressive renal failure. The joints, eyes, and skin
may also be affected in certain patients.
The causes of this disease remain to be determined.
In the current study, three cases of WG were investigated to
determine whether pathological examination in combination with
appropriate clinical and imaging data would be useful to identify
this disease in patients. The pathological examination showed
typical tissue necrosis, vasculitis and the formation of granuloma
structure. Typical chronic granulomatous inflammation performance
was not necessarily obvious in biopsies, but manifested as a single
scattering multinucleated giant cell or several multinucleated
giant cells. Tissue necrosis was basophilic or fibrinoid, with
infiltrating neutrophils, lymphocytes or plasma cells. The
proliferation and edema of vascular endothelial cells caused
luminal stenosis and occlusion. Vascular wall showed fibrinoid
necrosis. Addtionally, it was found that due to extensive
neutrophil aggregation, a small abscess may form.
The diagnostic standards of WG were proposed by the
American Rheumatism Association in 1990 and include the following
(8): i) Nasal or stomatitis symptoms
(pain or painless oral ulcers, bloody nasal discharge); ii)
microscopic hematuria (red blood cells >5/high power field) or
red blood cell casts; iii) chest X-ray film reveals nodules, fixed
infiltration, or cavity formation; and iv) biopsy shows
granulomatous inflammation of arteries or arterioles, and
surrounding tissue.
Two or more positive criteria indicates a diagnostic
sensitivity of 88.2% and specificity of 92% (8).
Pathological examination is important for diagnosing
WG. Serum ANCA examination and biopsy findings become increasingly
important in the diagnosis of WG, especially in cases with no
microscopic hematuria or red blood cell casts. The use of ANCA
significantly increased diagnostic accuracy in WG7. However, an
ANCA analysis has yet to be included in the diagnostic criteria of
WG by the American Rheumatism Association (8). ANCA are heterologous antibodies against
neutrophil cytoplasmic antigens (9).
These antibodies are divided into cytoplasmic (c-ANCA), perinuclear
(PANCA), and atypical (X-ANCA) types. Of these three types, c-ANCA
are most commonly found in WG, with the specificity of diagnosis
reaching 95–98% (9,10). Fewer than 10% of the patients can
also express p-ANCA, while some patients are ANCA-negative
(10,11).
Other diseases, such as the Churg-Strauss syndrome
or microscopic polyangiitis, can also be associated with positive
ANCA. Furthermore, the production of ANCA is associated with
infection or treatment with certain drugs (12). Therefore, diagnosis of WG should
include clinical manifestation, pathological diagnosis, laboratory
tests, and imaging data.
A differential diagnosis should be performed with
the following diseases: i) rhinitis, nasosinusitis: These diseases
present with lymphocyte and plasma cell infiltration, and tissue
edema. There is no vasculitis or multinucleated cell aggregation
forming granuloma, and less tissue necrosis (13).ii) Nasal NK/T cell lymphoma: This is a
type of lymphoma where lymphocytes have empty pale cytoplasm or
distorted nucleus (atypical lymphocytes). It may present with
substantial coagulation necrosis and infiltration of neoplastic
lymphocytes to the vascular center (14). However, granulomas formed by
multinucleated cells were not typically identified. iii)
Tuberculosis is a disease that often appears with caseous necrosis,
surrounded with giant cell of Langerhans, and the formation of
large quantities of epithelioid cells (15). Typically, acid-fast staining is
positive. iv) Lymphomatoid granulomatosis (16): This disease is associated with
angiocentric and vascular damage of extranodal lymphoid tissue
proliferation. Infiltrating cells are small lymphocytes, plasma
cells, and large atypical lymphocytes. Granulomas and neutrophil
infiltration are absent. Furthermore, this disease does not affect
the upper respiratory tract. v) Microscopic polyangiitis (17): This is systemic necrotizing
vasculitis involving small vessels. It often manifests with
necrotizing glomerulonephritis and pulmonary capillary
inflammation. Involvement of the upper respiratory tract and
presence of pulmonary shadows are rare. vi) Allergic granulomatous
angiitis (18): The disease often
appears as pulmonary and extrapulmonary small artery, with vein
inflammation and necrosis, and granulomas. There can be some
eosinophil infiltration in peripheral blood and tissue lesions.
Allergic granulomatous angiitisis often associated with the
occurrence of asthma.
WG is most commonly treated with glucocorticoid
hormones. Immunosuppressive agents may also be used. Prognosis in
untreated WG is extremely poor. Over 90% of the patients die of
respiratory failure and/or renal failure within two years. Early
diagnosis of WG and timely treatment can effectively reduce the
mortality rate, especially when a combination therapy of
glucocorticoids with cyclophosphamide is administered. This therapy
can lead to long-term remission.
In conclusion, the study on the three cases of WG
has demonstrated that tissue necrosis, vasculitis, and the
formation of granuloma are typical microscopic indicators of WG.
Furthermore, fibrinoid necrosis of the vessel wall and surrounding
tissue, and presence of multi-nucleated giant cells can also be
indicative of WG.
References
|
1
|
Hoffman GS, Kerr GS, Leavitt RY, Hallahan
CW, Lebovics RS, Travis WD, Rottem M and Fauci AS: Wegener
granulomatosis: an analysis of 158 patients. Ann Intern Med.
116:488–498. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Klinger H: Grenzformen der periarteritis
nodosa. Frankf Z Pathol. 42:455–480. 1931.(In German).
|
|
3
|
Wegener F: Über generalisierte, septische
Efäberkrankungen. Verh Dtsch Pathol Ges. 29:202–210. 1936.(In
German).
|
|
4
|
Lu ZY and Zhong NS: Internal Medicine.
Beijing: People's Medical Publishing House. 884–885. 2011.
|
|
5
|
Gadó KI, Zszabó L, Csákó L and Domján G:
Wegener's granulomatosis. Orv Hetil. 154:1083–1095. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen DY, Liang LQ and Zhan ZP: Limited and
severe Wegener's granulomatosis: clinical features. Chin Remedies
Clin. 10:489–492. 2010.(In Chinese).
|
|
7
|
Yu SY and Sun B: Clinical Diagnosis and
Treatment of Respiratory Department of Internal Medicine. Beijing:
Union Medical College Press. 2010.
|
|
8
|
Leavitt RY, Fauci AS, Bloch DA, Michel BA,
Hunder GG, Arend WP, Calabrese LH, Fries JF, Lie JT, Lightfoot RW
Jr, et al: The American College of Rheumatology 1990 criteria for
the classification of Wegener's granulomatosis. Arthritis Rheum.
33:1101–1107. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Vassilopoulos D, Niles JL, Villa-Forte A,
Arroliga AC, Sullivan EJ, Merkel PA and Hoffman GS: Prevalence of
antineutrophil cytoplasmic antibodies in patients with various
pulmonary diseases or multiorgan dysfunction. Arthritis Rheum.
49:151–155. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zak-Gołab A, Hrycek A, Holecki M and
Chudek J: Diagnostic value of antineutophil cytoplasmic antibodies.
Wiad Lek. 64:37–42. 2011.(In Polish). PubMed/NCBI
|
|
11
|
Chen M, Yu F, Zhang Y and Zhao MH:
Antineutrophil cytoplasmic autoantibody-associated vasculitis in
older patients. Medicine (Baltimore). 87:203–209. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kallenberg CG: Key advances in the
clinical approach to ANCA-associated vasculitis. Nat Rev Rheumatol.
10:484–493. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Stierna P and Carlsöö B: Histopathological
observations in chronic maxillary sinusitis. Acta Otolaryngol.
110:450–458. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chubachi A, Imai H, Nishimura S, Saitoh M
and Miura AB: Nasal T-cell lymphoma associated with hemophagocytic
syndrome. Immunohistochemical and genotypic studies. Arch Pathol
Lab Med. 116:1209–1212. 1992.PubMed/NCBI
|
|
15
|
Sweany HC and Seiler HH: The pathology and
bacteriology of resected lesions in pulmonary. Dis Chest.
29:119–152. 1956. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Feng RE, Liu HR, Liu TH, Chen J, Ling Q,
Shi XH, Zhong DR, Luo YF and Cao JL: Pulmonary lymphomatoid
granulomatosis: An immunohistochemical and gene rearrangement
study. Zhonghua Bing Li Xue Za Zhi. 40:460–464. 2011.(In Chinese).
PubMed/NCBI
|
|
17
|
Chinese Medical Association of
Rheumatology: Microscopic polyangiitis diagnosis and treatment
guidelines. Chin J Rheumatol. 15:259–261. 2011.(In Chinese).
|
|
18
|
Jones RB, Tervaert JW, Hauser T, Luqmani
R, Morgan MD, Peh CA, Savage CO, Segelmark M, Tesar V, van Paassen
P, et al: European Vasculitis Study Group: Rituximab versus
cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med.
363:211–220. 2010. View Article : Google Scholar : PubMed/NCBI
|