Introduction
Pseudomonas aeruginosa is a common clinical
cause of gram-negative bacterial, nosocomial infections (1), and causes serious infections in
neutropenic and immunocompromised patients (2). Within intensive care units, P.
aeruginosa has become the most common gram-negative bacterial
species associated with severe hospital-acquired infections
(2,3). At present, the worldwide morbidity and
mortality rates of P. aeruginosa are 18 and 61% respectively
(1–3). The treatment of P. aeruginosa
infections in a clinical setting remains a notable challenge. The
capacity of patients to ingest the appropriate antibiotics in a
timely manner positively affects prognosis of severe
pseudomonas-infection (4). As such,
this variable serves as an important controllable risk factor
(4,5). Clinical infection with P.
aeruginosa may be associated with an increase in 30-day
mortality in patients. Treatment with appropriate antibiotics, such
as β-lactam and fluoroquinolone, is associated with the prognosis
(6). However, the use of appropriate
antibiotic treatment does not consistently show satisfactory
effects on patients (7,8). It has previously been suggested that
the inappropriate use of antibiotics in the treatment of P.
aeruginosa bacteraemia may be minimised by a combination
antibiotic regimen, in which the sensitivity of results is
determined following treatment (8).
Inappropriate use of empirical antibiotic therapy has been
identified as an independent contributor to the high hospital
mortality rate of P. aeruginosa bacteraemia (8,9).
Combination therapy has been shown to yield improved results
compared with single treatment of P. aeruginosa bacteraemia
(6,9), and combination empirical antimicrobial
therapy directed against gram-negative bacteria may be a more
appropriate treatment approach than monotherapy (10). Despite the merits of relevant studies
on empirical combination therapy, it is still unclear whether the
use of combination therapy is more effective than monotherapy in
treating P. aeruginosa infection (10–18). In
the present study a meta-analysis was conducted and the mortality
of patients treated with either combination therapy or the
appropriate monotherapy for P. aeruginosa bacteraemia was
compared and evaluated.
Materials and methods
Search terms
Several electronic bibliographic databases were
searched including the Chinese Biomedical Literature
Database (Wanfang, China), China Academic Journals Full-text
database, Cochrane Library, PubMed and Embase for the
identification of relevant studies (as of April 2017). The included
search terms were: Pseudomonas aeruginosa, bacteremia,
monotherapy, combination therapy, antibiotic, mortality and
outcome. The databases were searched manually to identify
potentially relevant studies. The reference lists of all retrieved
articles were also searched to find research that could qualify for
the study. Only articles written in Chinese or English were
considered; articles written in German, French, Spanish, Italian
and Greek were not evaluated. Ultimately, all included papers were
written in English. The study inclusion criteria were as follows:
i) The study compared the efficacy of monotherapy and combination
therapy; ii) retrospective and prospective studies; iii) the
treatments discussed in the study included at least one antibiotic
agent, which was reported following sustained or initial
antibacterial spectrum results (8);
and iv) the study results included data on mortality.
Study selection
Two experienced independent reviewers (S-YT and
S-WZ) subsequently read through the results and decided which
studies were appropriate to be included in the meta-analysis
(5,10–25). Any
differences in opinion between the two reviewers were resolved by
discussion until a consensus was reached. The following data was
extracted from each qualified study: Name of first author, type of
publication, type of study design, gender and age of patients,
sample size, length of hospital stay, type of treatment, type and
choice of drugs, mortality, outcomes, number of different
populations, and odds ratio (OR) and 95% confidence interval (CI)
results. The possible risk estimates were extracted and adjusted
using hybrid variables.
Quality assessment
The selected studies were evaluated using a system
based on the cohort study using the Newcastle-Ottawa scale
(26), which provides a score for
studies between 1–9 ‘stars’. Three aspects were used to assess the
quality of studies: i) Choice of learning study, ii) organisational
evaluation and iii) evaluation of comparison results. As there is
dispute over the number of stars that must be used as an indicator
of high-quality studies (27–33), the
included studies were compared; studies that received ≥7 stars
(7,8,9) were
defined as high-quality studies, and those that scored ≤6 were
not.
Statistical methods
Statistical analysis was conducted using Stata
version 12.0 software (StataCorp LP, College Station, TX, USA). ORs
with 95% CIs were extracted from studies to evaluate the outcomes
of mortality. Cochrane's X2 Q and I2 tests were employed
to assess the differences in data from different studies.
Stochastic models were applied to heterogeneity studies (P<0.1
or I2>50%) (34,35). The
Mantel-Haenszel fixed-effect model was used to calculate pools or
studies when P>0.10 and I2≤50%; otherwise, the
Dersimonian and Laird's random-effects model was used to combine
results (36). A sensitivity
analysis was also conducted to examine the effects of each study on
mixed outcomes. To establish the effects of clinical heterogeneity
on meta-analysis, a subgroup analysis was conducted based on study
characteristics. Egger's precision-weighted linear regression tests
and funnel charts were used to assess potential publication bias
(37). When a study demonstrated
potential publication bias, the nonparametric correction and
filling method was applied. The filling method evaluates the
possibility of ‘missing’ studies that may exist and recalculates
the pool or merges them (34,35). The
results of the meta-analysis were stratified by types of study and
treatment. P<0.05 was considered to indicate a statistically
significant difference, unless otherwise stated.
Results
Search results
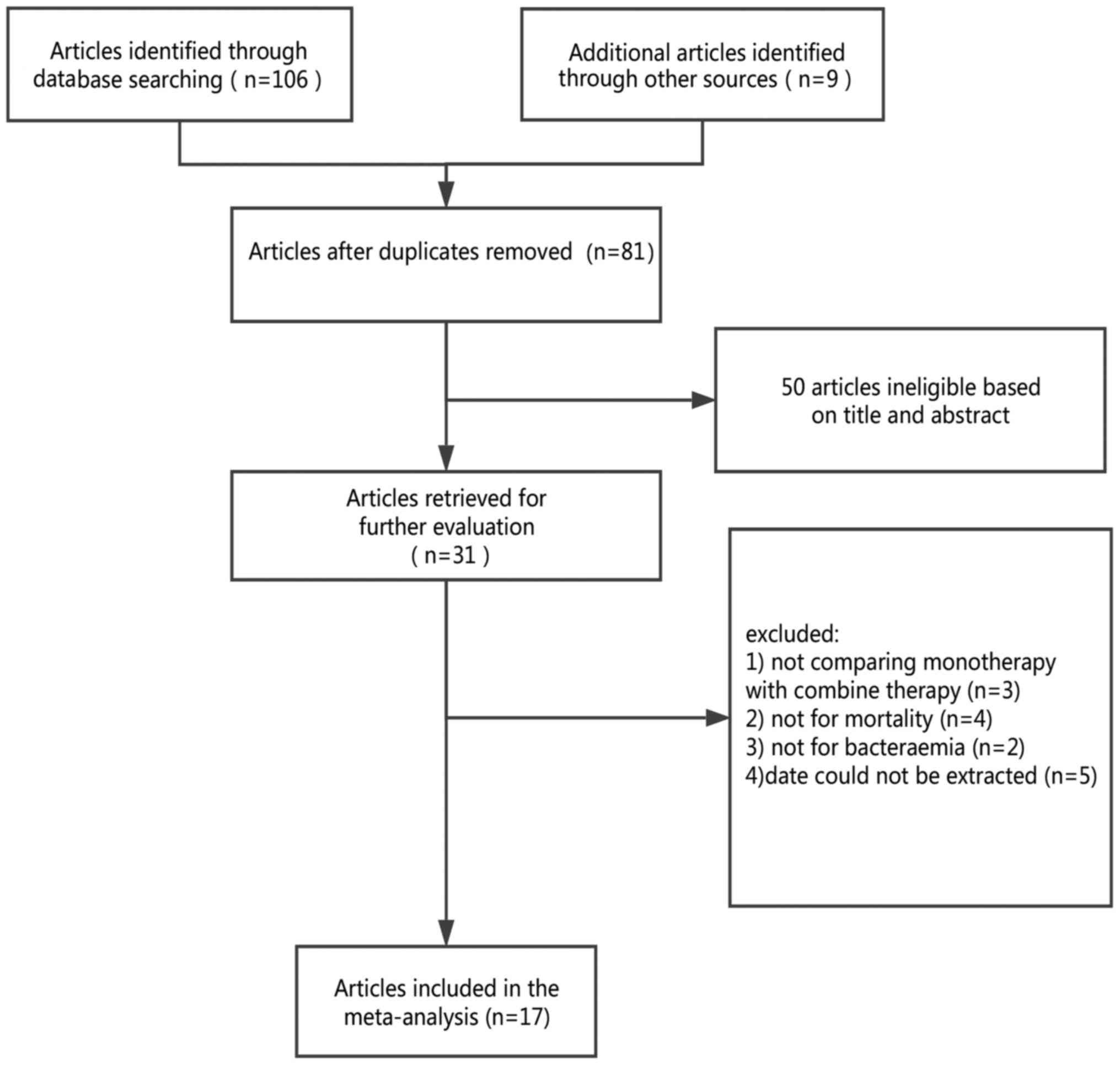
Fig. 1 demonstrates
the process of study selection and the number of studies excluded
at each stage. In the initial search 115 studies were identified,
and following a review of the titles, 31 studies were considered
for inclusion. The summaries of those 31 studies were reviewed and
all studies that were considered eligible were retrieved. Among
these studies 14 were excluded for the following reasons: 3 studies
did not compare monotherapy and combination therapy; 4 studies did
not include mortality rate in the assessment of results; 2 were
excluded because patient infection did not cause bacteraemia; and 5
were excluded as data could not be extracted. Therefore, following
the screening process 17 studies qualified (5,10–25) and
were included in the meta-analysis; they covered a total of 2,504
patients with cases of P. aeruginosa bacteraemia.
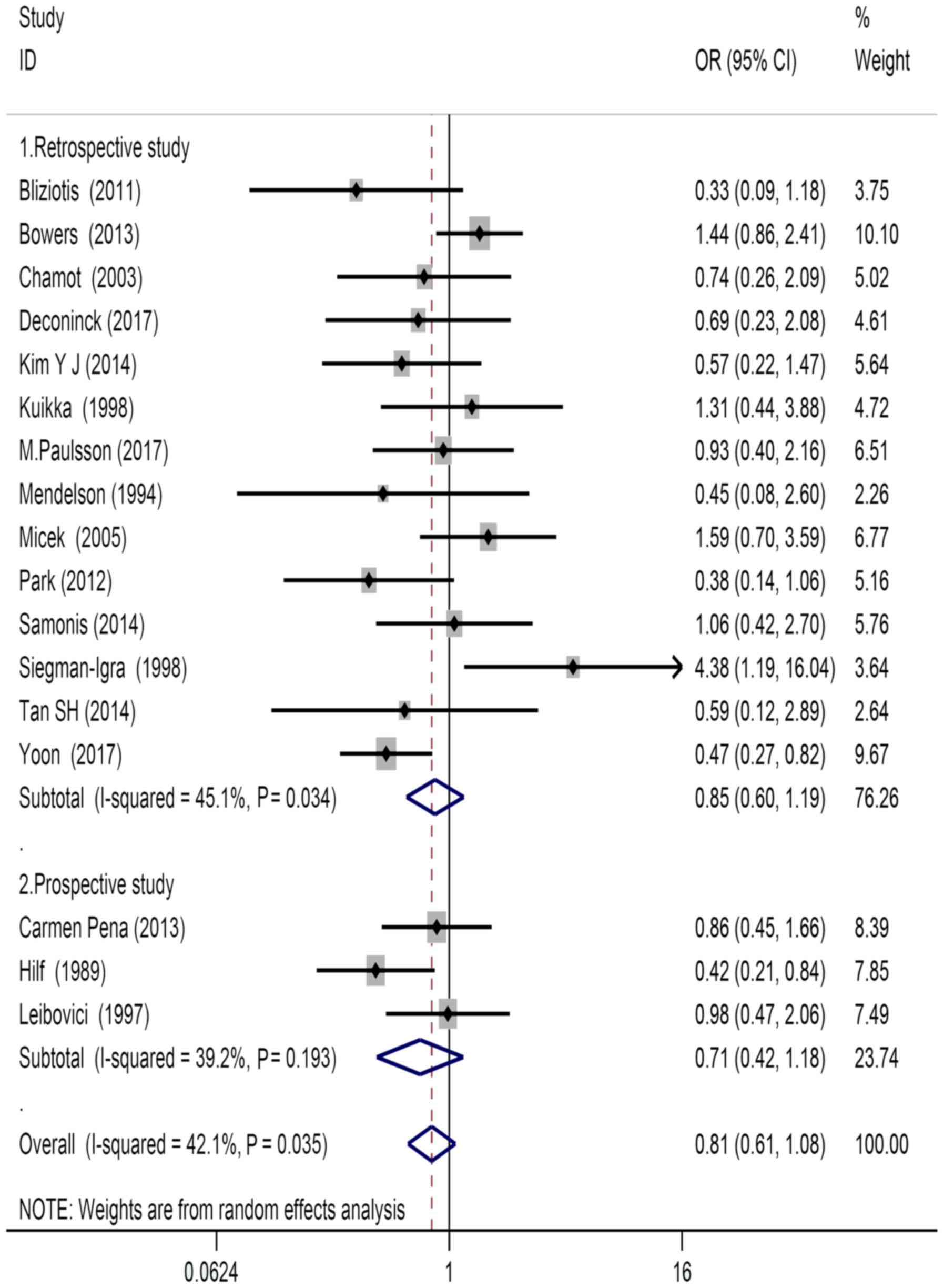
Study characteristics
Within the qualified studies, 14 were retrospective
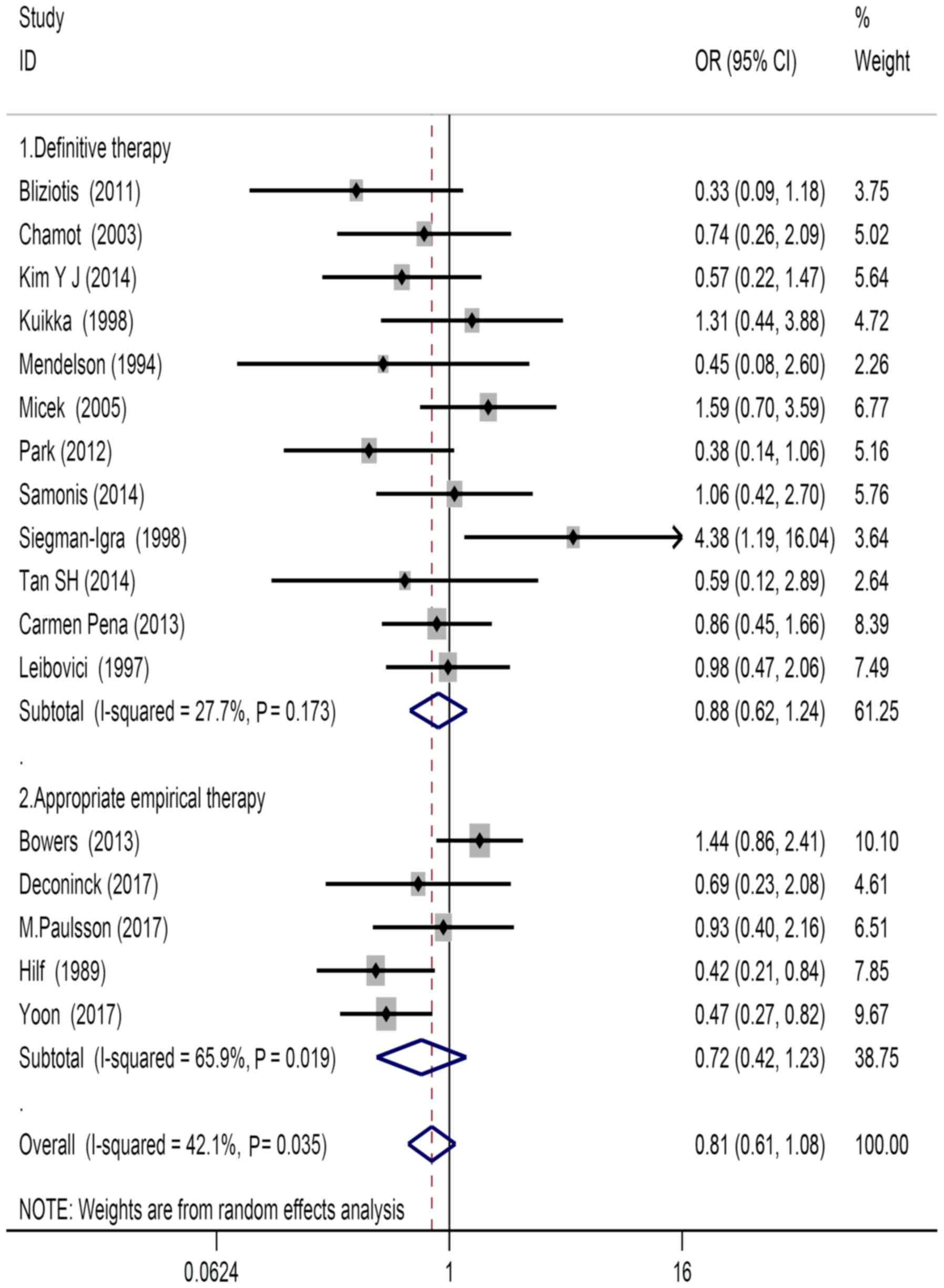
studies and 3 were prospective studies (Fig. 2). There were 5 studies that reported
outcomes of empirical treatment and 12 studies that reported
outcomes of definitive treatment (Fig.
3). There were 4 studies conducted in the United States, 7 in
Europe, 6 in Asia and 1 was conducted in the United States and
Singapore (Table I). According to
the Newcastle-Ottawa Scale, 16 of the included studies scored >6
and were rated as good or excellent quality (Table I).
 | Table I.Characteristics of the eligible
studies included in the meta-analysis of monotherapy vs.
combination therapy for Pseudomonas aeruginosa
bacteraemia. |
Table I.
Characteristics of the eligible
studies included in the meta-analysis of monotherapy vs.
combination therapy for Pseudomonas aeruginosa
bacteraemia.
|
|
|
|
|
| Drugs |
| Mortality
(mortality cases/total) |
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Author, year | Study design | Study period | Country | Therapy type | Combination
therapy | Monotherapy | Mortality
outcome | Combination
therapy | Monotherapy | Study
qualitya | Independent risk
factors | (Refs.) |
|---|
| Bowers et
al, 2013 | Retrospective | 2002–2011 | USA/Singapore | Appropriate
empirical therapy | More than one
antipseudomonal agent | An antipseudomonal
antimicrobial agent | Mortality | 30/82 | 82/286 | 9 | Diabetes mellitus,
liver cirrhosis, respiratory conditions, renal disease | (12) |
| Park et al,
2012 | Retrospective | 1997–2011 | South Korea | Appropriate
empirical therapy | A β-Lactam
antibiotic and either an aminoglycoside or ciprofloxacin | A β-lactam or
ciprofloxacin | 28 days | 10/33 | 17/32 | 9 | APACHE II score,
liver cirrhosis, immunosuppression, hematologic malignancy | (23) |
| Bliziotis et
al, 2011 | Retrospective | 2001–2007 | Greece/Italy | Definitive
treatment | A β-Lactam and an
aminoglycoside or a quinolone | β-Lactam
antibiotic | Mortality | 6/31 | 8/19 | 9 | AIDS, HIV, solid
tumor, respiratory dysfunction, cardiovascular dysfunction | (11) |
| Micek et al,
2005 | Retrospective | 1997–2002 | USA | Definitive
treatment | A β-lactam and an
aminoglycoside | A β-lactam or
ciprofloxacin | Mortality | 13/59 | 16/106 | 8 | APR-DRG score,
shock | (5) |
| Chamot et
al, 2003 | Retrospective | 1988–1998 | Switzerland | Definitive
treatment | A β-lactam and an
administration of an administration of an aminoglycoside together
with ciprofloxacin | A β-lactam or
aminoglycoside or fluoroquinolones | 30 days | 10/46 | 9/33 | 8 | Simple sepsis,
severe sepsis, shock | (10) |
| Siegman-Igra et
al, 1998 | Retrospective | 1990–1992 | Israel | Definitive
treatment | A fluoroquinolone,
a third-generation cephalosporin, cilastatin or a ureidopenicillin
in combination with an aminoglycoside | A fluoroquinolone,
a third-generation a third-generation cephalosporin or
imipenem/cilastatin | Overall
mortality |
7/15 |
7/42 | 7 | Malignancy,
neutropenia | (15) |
| Kuikka and
Valtonen, 1998 | Retrospective | 1976–1982,
1992–1996 | Finland | Definitive
treatment | A β-lactam and
either an aminoglycoside or quinolone | β-lactam or
ciprofloxacin | 30 days | 11/41 | 7/32 | 7 | Leukopenia,
cholelithiasis, COPD, alcohol abuse, indwelling urinary
catheter | (21) |
| Mendelson et
al, 1994 | Retrospective | 1978–1992 | USA | Definitive
treatment | Ceftazidime,
piperacillin, cefoperazone, aztreonam and an aminoglycoside
(gentamicin, tobramycin) | Ceftazidime,
piperacillin, cefoperazone, aztreonam or ciprofloxacin | Mortality |
4/15 |
4/9 | 6 | HIV, cryptococcal
meningitis, pneumocystis pneumonia | (22) |
| Leibovici et
al, 1997 | Prospective | 1988–1995 | Israel | Definitive
treatment | A β-lactam and an
aminoglycoside | A β-lactam | Mortality | 16/77 | 20/95 | 7 | Septic shock,
malignancy, neutropenia, congestive heart failure | (20) |
| Hilf et al,
1989 | Prospective | 1982–1986 | USA | Definitive
treatment | An aminoglycoside
and an antipseudomonal β-lactam | Antipseudomonal
antibiotics including aminoglycoside, β-lactam | 10 days | 38/143 | 20/43 | 7 | Malignancy,
neutropenia, pneumonia, MODS | (19) |
| Peña et al,
2013 | Prospective | 2010–2011 | Spain | Definitive
treatment | A β-lactam +
aminoglycoside, fluoroquinolones or colistin | A β-lactam or
aminoglycoside or fluoroquinolones or colistin | 30 days | 13/71 | 70/339 | 9 | Hepatobiliary
HIV/AIDS, diabetes mellitus, MODS | (18) |
| Kim et al,
2014 | Retrospective | 2010–2012 | South Korea | Definitive
treatment | A β-lactam and
aminoglycosides fluoroquinolones, colistin and fluoroquinolones or
aminoglycoside | A β-lactam,
fluoroquinolones, colistin or aminoglycosides | 14 days | 6/42 | 32/141 | 9 | Diabetes mellitus,
liver cirrhosis, malignancy, hypertension | (16) |
| Samonis et
al, 2014 | Retrospective | 2004–2010 | Greece | Definitive
treatment | A β-lactam +
aminoglycoside/fluoroquinolone/colistin or colistin + other | A β-Lactam or
fluoroquinolone, colistin | Mortality | 12/37 | 14/45 | 8 | Chronic lung
disease, diabetes mellitus, chronic heart disease, chronic renal
disease | (17) |
| Tan SH et
al, 2014 | Retrospective | 2007–2008 | Singapore | Definitive
treatment | A β-lactam +
aminoglycosides or ciprofloxacin | A β-Lactam or
aminoglycosides or ciprofloxacin | 30 days |
2/14 | 17/77 | 9 | SAPS II score,
HIV/AIDS, diabetes mellitus, cardiovascular dysfunction | (25) |
| Deconinck et
al, 2017 | Retrospective | 1994–2014 | France | Appropriate
empirical therapy | A β-Lactam + an
aminoglycoside, aquinolone or colistin | A β-Lactam,
aminoglycoside, fluoroquinolone or colistin | 30 days | 32/85 |
7/15 | 9 | Shock, SAPS II,
multiresistant strains | (13) |
| Paulsson et
al, 2017 | Retrospective | 2005–2010 | Sweden | Appropriate
empirical therapy | Carbapenem,
cefotaxime + tobramycin or piperacillin | Cefotaxime,
cefuroxime or piperacillin | 30 days | 16/79 | 12/56 | 7 | COPD, neurological
paresis, diabetes mellitus, heart disorder, AIDS | (14) |
| Yoon | Retrospective | 2012–2015 | South Korea | Appropriate
empirical therapy | A β-Lactam and an
aminoglycoside or a quinolone | A β-lactam or | 30 days | 25/85 | 84/179 | 9 | Septic shock,
neutropenia, Pitt bacteraemia score | (24) |
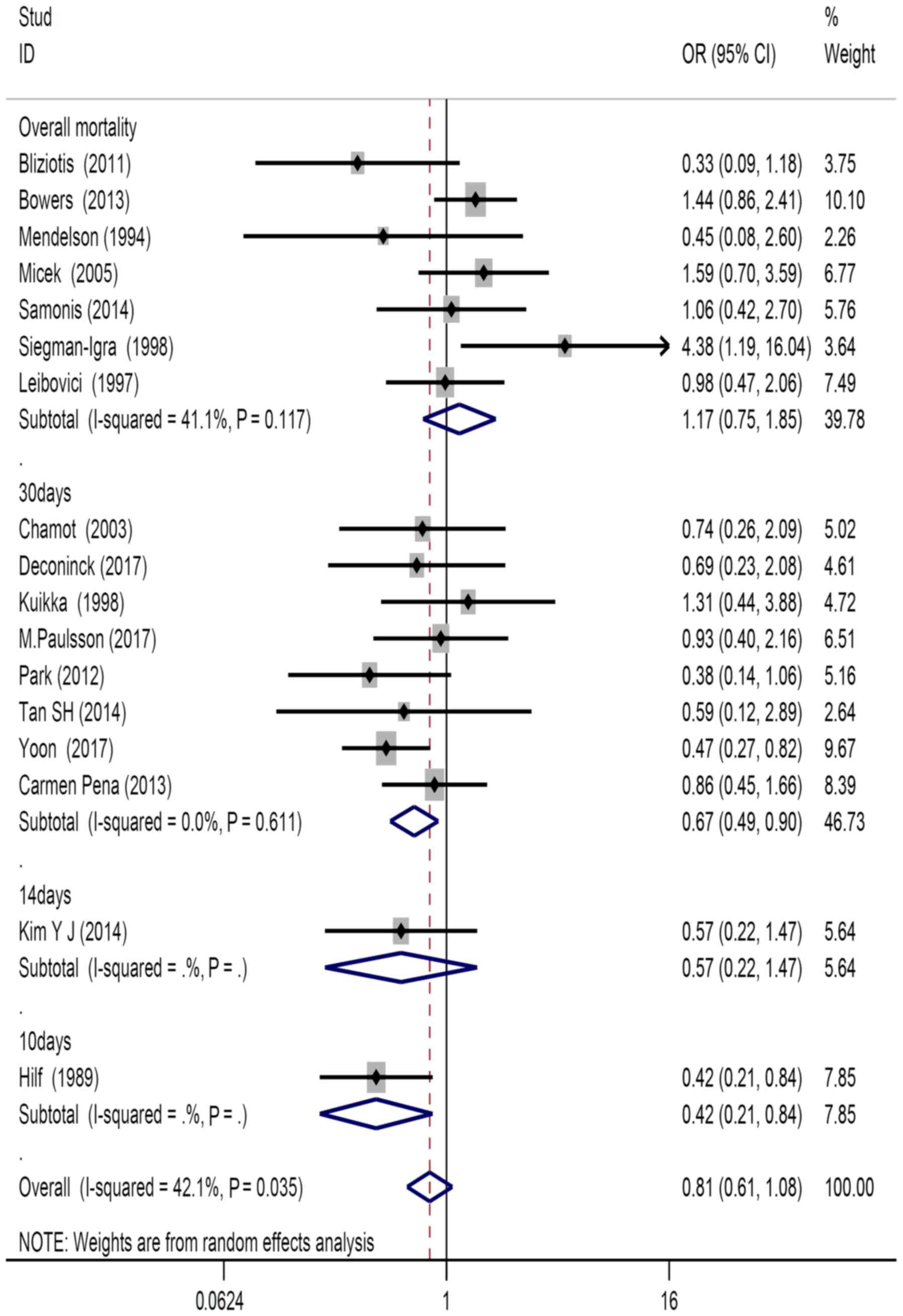
Mortality
There were 8 studies that used survival for 30 days,
1 that used survival for 14 days and 1 that used survival for 10
days as the desired outcome of the study. There were 7 studies that
considered overall survival as the desired outcome. In terms of
mortality, significant difference was observed between patients who
received definitive treatment compared with those who received the
appropriate empirical treatment (OR=0.81, 95% CI=0.61–1.08;
Fig. 3).
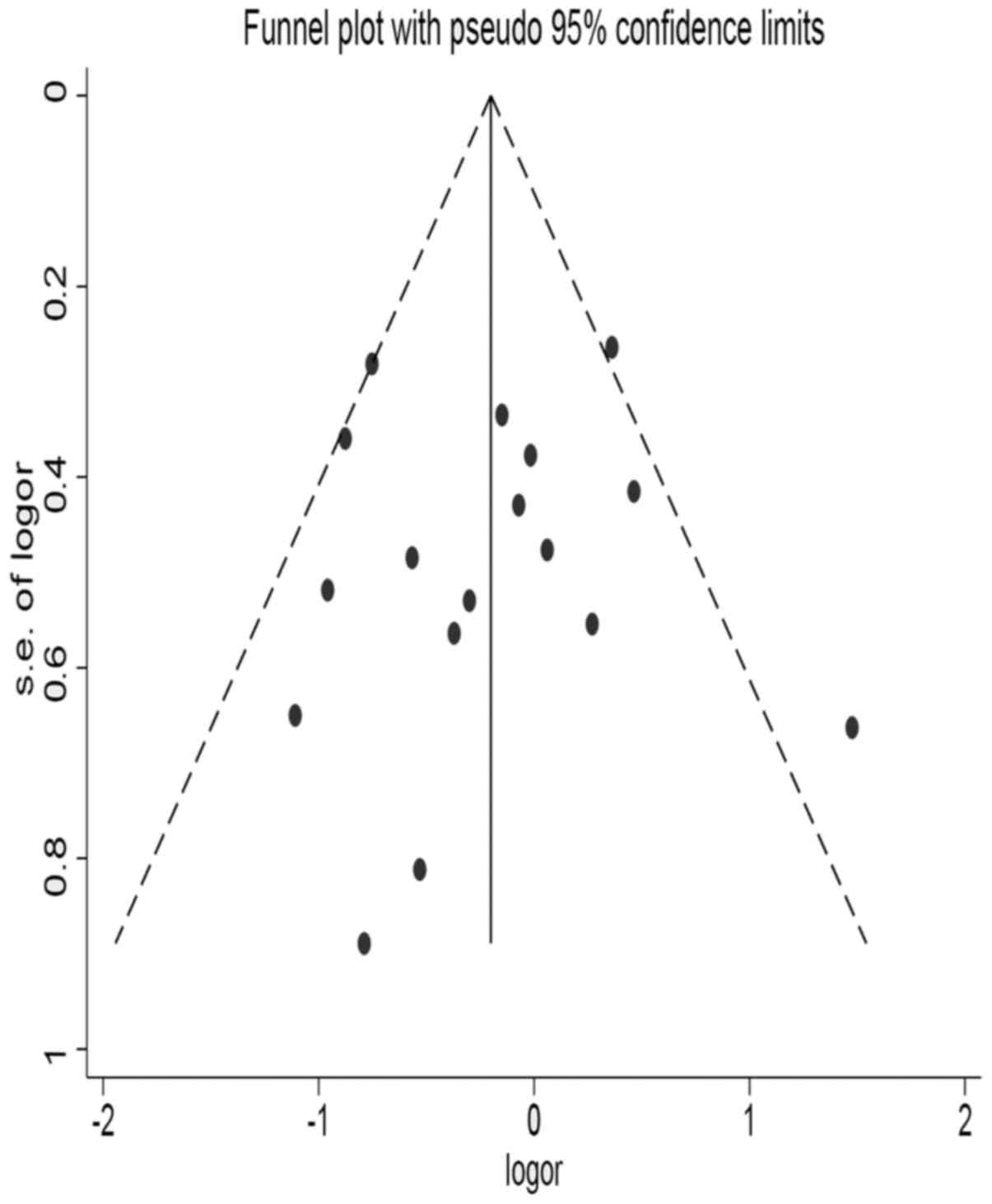
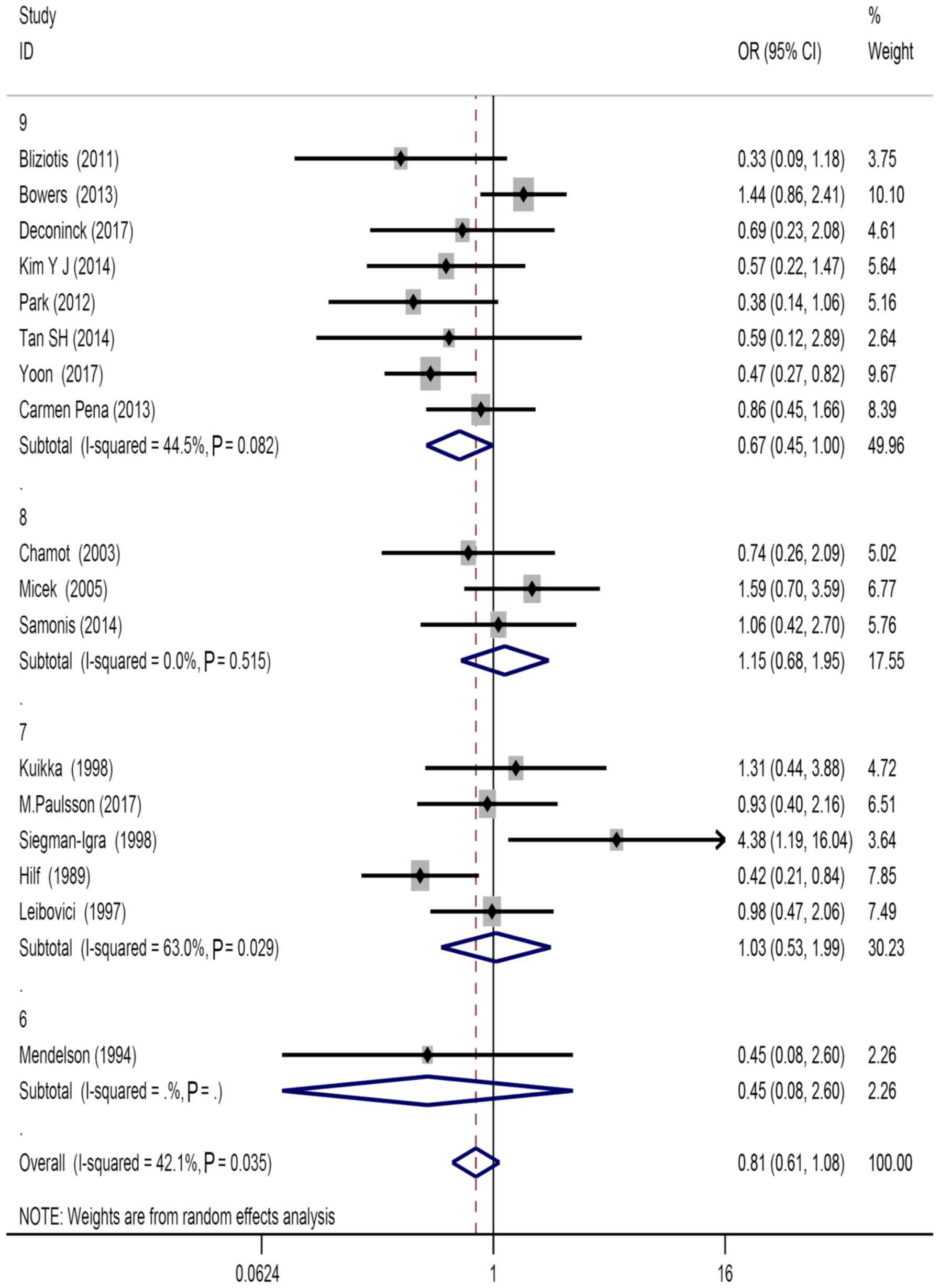
Publication bias
Considering the observed heterogeneity (P=0.035;
I2=42.1%) of the 17 included studies, a random-effects
model was used for their analysis (Fig.
2). The following factors were considered: Source of patients,
types of study design (OR=0.85, 95% CI=0.60–1.19, P=0.034), types
of treatment (OR=0.72, 95% CI=0.42–1.23, P=0.019), study population
(OR=0.74, 95% CI=0.41–1.33, P=0.036), literature quality score
(OR=0.67, 95% CI=0.45–1.00, P=0.082), and mortality of subgroup
stratification analysis (OR=1.17, 95% CI=0.75–1.85, P=0.117;
Table II). Retrospective and
prospective studies were significantly different in subgroup
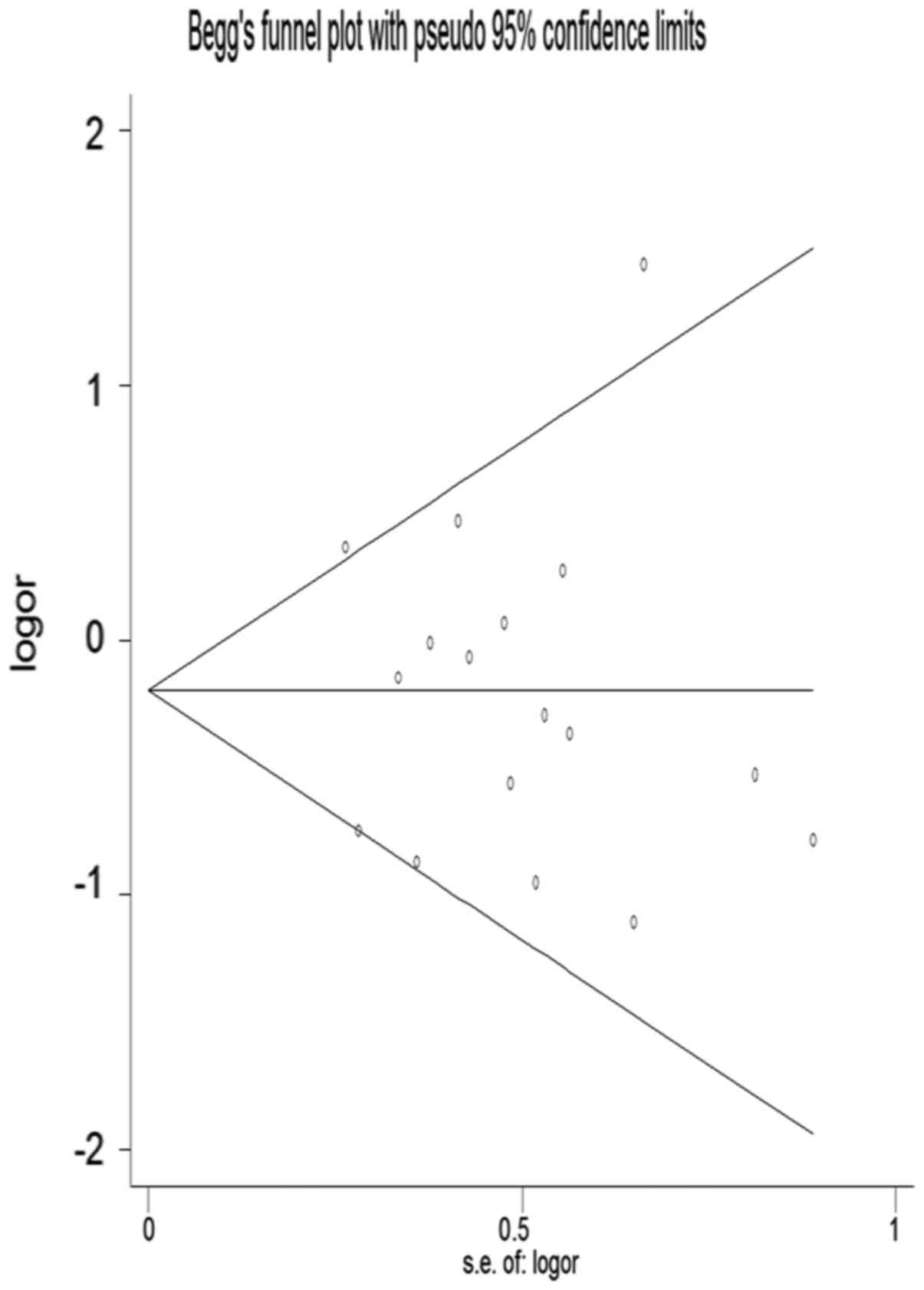
analysis. Visual inspection of the funnel plots revealed asymmetry
among studies (Fig. 4).
Consolidation effect was assessed to review the influence results
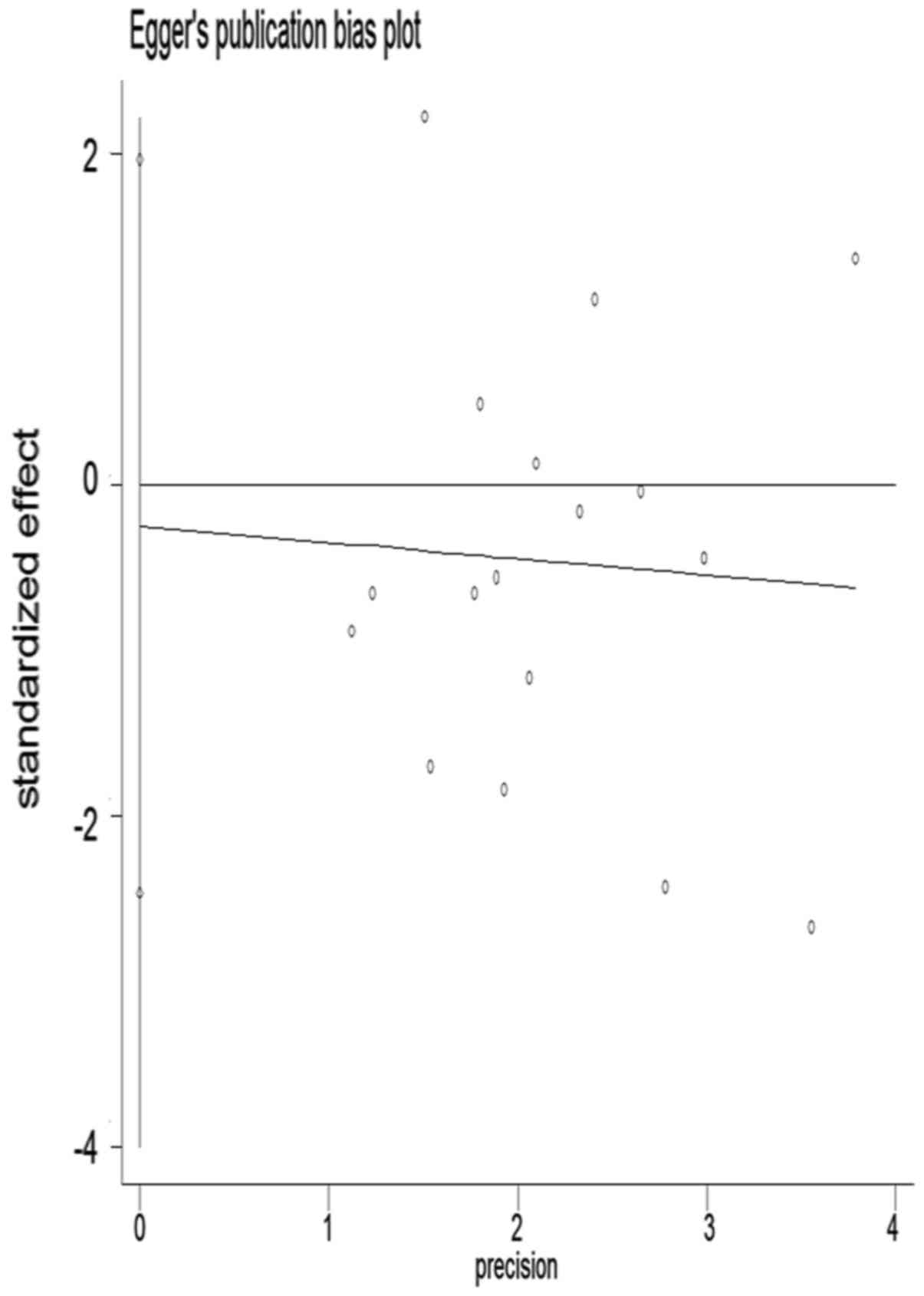
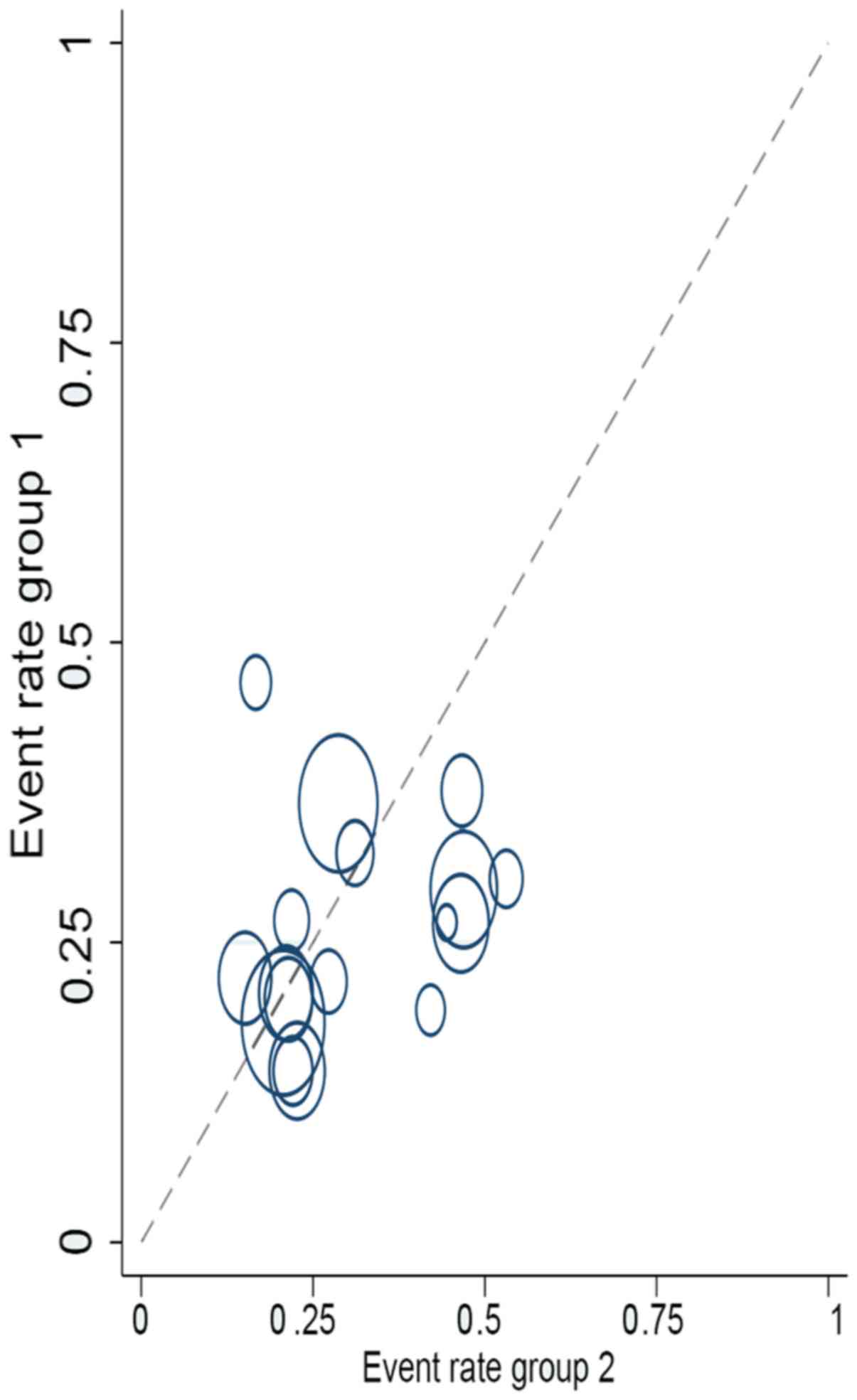
for each study (Fig. 5). Begger's
and Egger's tests were conducted to determine publication bias
(Figs. 6 and 7) and L'Abbé analysis was performed to
assess the heterogeneity of effect sizes, which revealed no marked
heterogeneity (Fig. 8). The Z-value
and P-value of Begger's test reached 0.21 and 0.805, respectively,
and the t-value and P-value of Egger's test totalled −0.24 and
0.815 respectively. Both P-values of Egger's test and Begger's test
were >0.05. Therefore, these results indicated that there was no
compelling evidence to affirm that results obtained were free from
published publication bias.
| Table II.Stratified analyses of pooled
ORs. |
Table II.
Stratified analyses of pooled
ORs.
|
|
|
|
| Heterogeneity
test |
|
|---|
|
|
|
|
|
|
|
|---|
| Factor | Level | No. of studies | Pooled OR (95%
CI)a | P-value | I2
(%) | (Refs.) |
|---|
| All studies | – | 17 | 0.81
(0.61–1.08) | 0.035 | 42.1 | (5,10–18,31–37) |
| Study
population | Asian | 6 | 0.74 (0.41,
1.33) | 0.036 | 58.0 | (15,16,32,35–37) |
|
|
Non-Asiana | 11 | 0.88 (0.65,
1.20) | 0.196 | 26.0 | (5,10–14,17,18,31,33,34) |
| Study design | Prospective
cohorta | 3 | 0.71 (0.42,
1.18) | 0.193 | 39.2 | (18,31,32) |
|
| Retrospective
cohort | 14 | 0.85 (0.60,
1.19) | 0.034 | 45.1 | (5,10–17,33–37) |
| Therapy type | Definitive
therapy | 12 | 0.88 (0.62,
1.24) | 0.173 | 27.7 | (5,10,11,15–18,32–35,37) |
|
| Appropriate
empirical therapy | 5 | 0.72 (0.42,
1.23) | 0.019 | 65.9 | (12–14,31,36) |
| Study quality | 9 stars | 8 | 0.67 (0.45,
1.00) | 0.082 | 44.5 | (11–13,16,18,35–37) |
|
| 8 stars | 3 | 1.15 (0.68,
1.95) | 0.515 | – | (5,10,17) |
|
| 7 stars | 5 | 1.03 (0.53,
1.99) | 0.029 | 63.0 | (14,15,31–33) |
|
| 6
starsb | 1 | 0.45 (0.08,
2.60) | – | – | (34) |
| Outcome | Overall
mortality | 7 | 1.17 (0.75,
1.85) | 0.117 | 41.1 | (5,11,12,14,15,17,34) |
|
| 30-day
mortality | 8 | 0.67 (0.49,
0.90) | 0.611 | 0 | (10,13,14,18,33,35–37) |
|
| 14-day
mortalityb | 1 | 0.57 (0.22,
1.47) | – | – | (16) |
|
| 10-day
mortalityb | 1 | 0.42 (0.21,
0.84) | – | – | (31) |
Subgroup and sensitivity analysis
Table II
demonstrates the stratified analysis designed to focus OR of 0.85
(95% CI=0.60–1.19) for 14 retrospective cohorts and the 12 studies
with specific definitive therapy OR of 0.88 (95% CI=0.62–1.24). A
strong correlation was identified in studies conducted in Asian
countries, and study quality and mortality did not significantly
affect the results (Figs. 9–11).
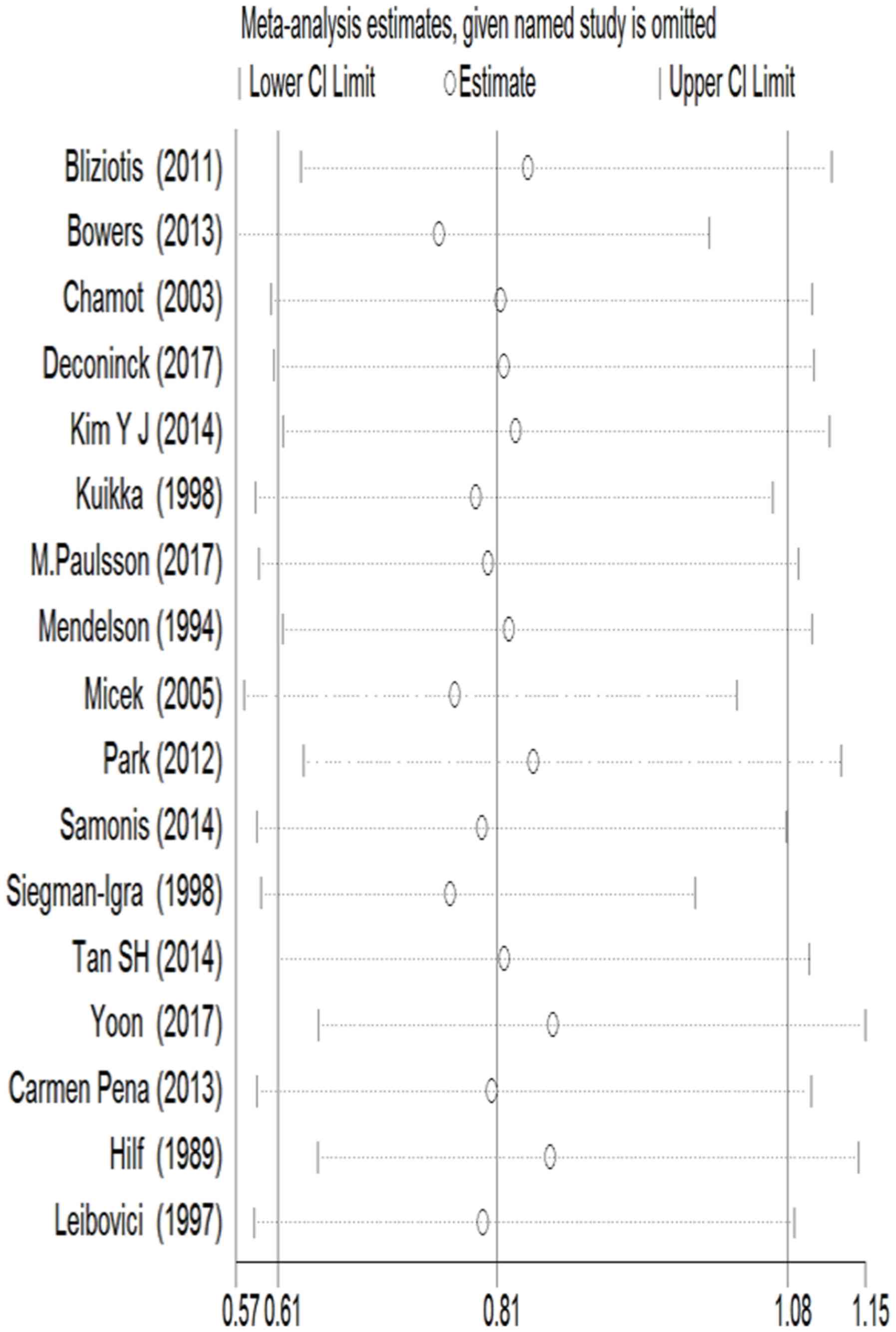
The contribution of studies to overall prevalence
and 95% CIs was evaluated. In sensitivity analyses, surveyed time
strip was omitted and then results were combined with a single
dataset on pooled ORs. Corresponding pooled ORs did not change
significantly from 0.67 (95% CI=0.45–1.00) to 0.85 (95%
CI=0.60–1.19). Therefore, the results obtained were considered
statistically strong.
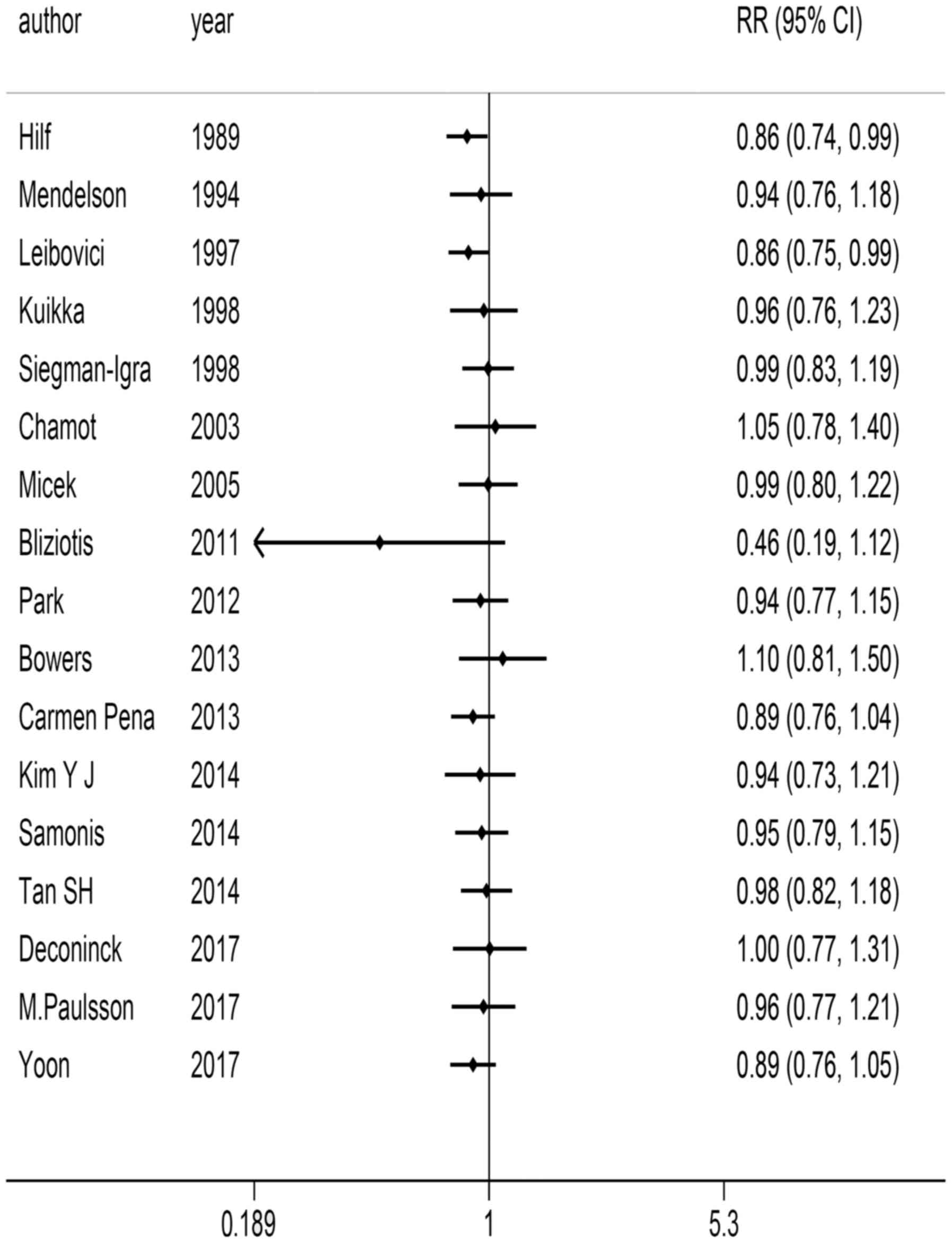
Cumulative meta-analysis
Heterogeneity inspection was conducted initially and
the effects, combined effects and their corresponding CI were
evaluated to obtain the Q statistic and its corresponding P-value.
Heterogeneity=27.63 (degree of freedom=16), P=0.035 and
I2=42.1%. Given that no clear heterogeneity was observed
among studies, cumulative analysis was performed using a
random-effects model. Fixed number of years and sample size were
considered for cumulative meta-analysis. Organised in chronological
order, OR value and 95% CI were stable and demonstrated good change
trend, aside from the study by Bliziotis et al (11) (Fig.
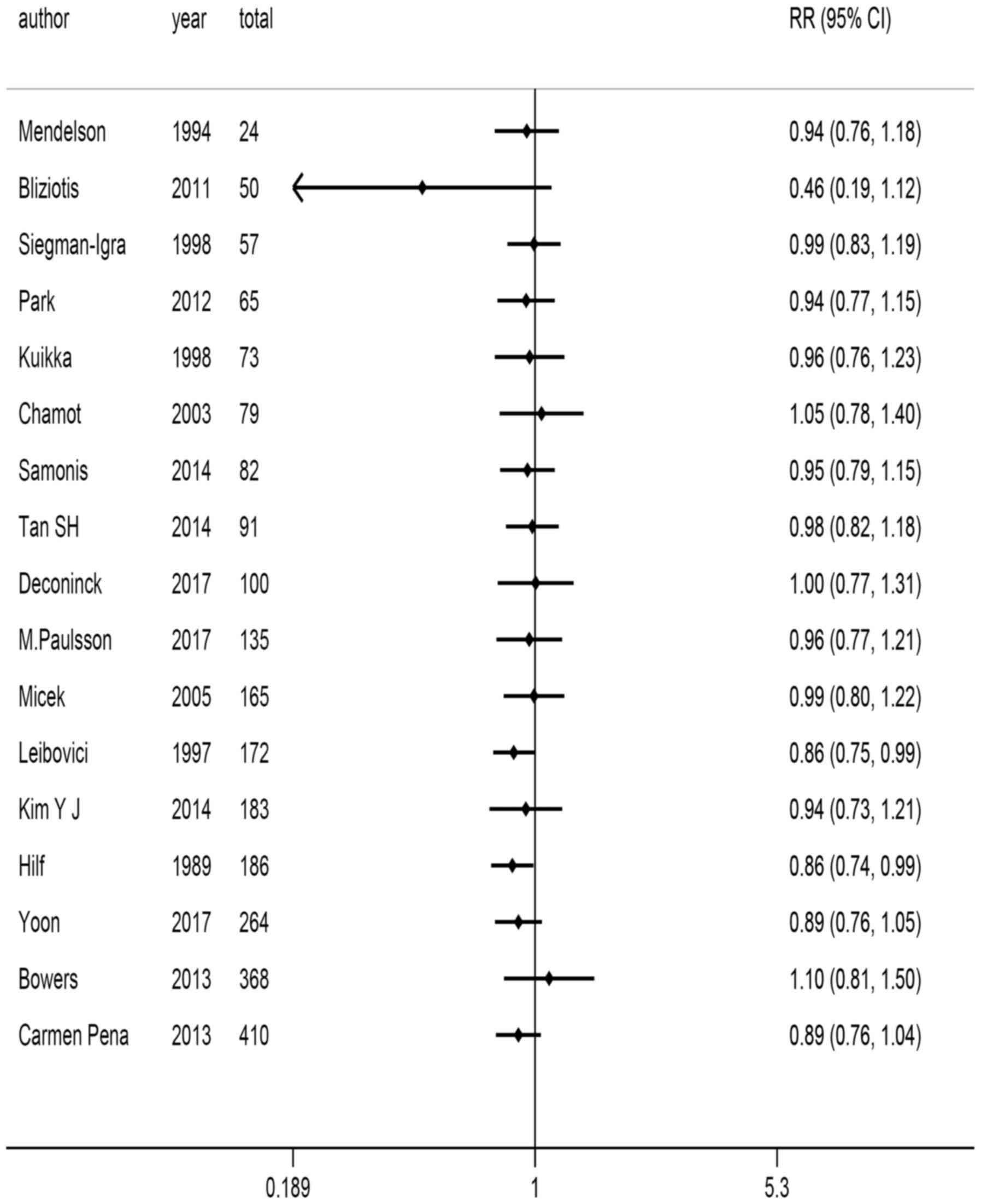
12). Based on sample size order following accumulation, when a
large sample was included, the range of OR values and 95% CI (0.89;
0.76–1.04) was decreased (Fig.
13).
Discussion
The present study consisted of a meta-analysis that
compared the effects of using either a combination of antibiotics
or a single antibiotic for the treatment of P. aeruginosa
bacteraemia. A total of 17 studies were systematically reviewed and
compared. The antibiotic and appropriate empirical treatments used
were determined by extracting data from the studies, and the
patients' all-cause mortality associated with P. aeruginosa
bacteraemia was analysed. No significant differences were
identified between monotherapy and combination therapy in regards
to mortality. Therefore, definite combination therapy and
appropriate combination of therapies failed to independently
provide additional benefits for patient treatment. However, in the
subgroup analysis process significant differences were observed in
types of study design and types of treatment. In particular, the
use of β-lactam and cephalosporin antibiotics as an empirical
treatment were able to significantly reduce the mortality rate of
patients.
In clinical treatment, patient mortality associated
with P. aeruginosa bacteraemia remains high (61%) despite
the progress of antibiotic therapy; thus, an improved treatment
approach is required (38).
Bliziotis et al (11)
reported that combination therapy was superior to monotherapy in
treating patients with P. aeruginosa bacteraemia; however,
81% of patients (25/31) who received monotherapy only received
β-lactam, which cannot be considered the optimum monotherapy owing
to the increased mortality rate associated with this drug compared
with other monotherapies (20,21,39).
Micek et al (5) observed that
compared with single antibiotics, combination therapy yielded
improved effects. However, given the open clinical design of the
study, patients in a single-treatment group may be more likely to
receive additional antibiotics and were therefore considered
treatment failures in these studies. The number of patients
included in meta-analysed subgroups were assessed in each
randomised controlled study. As such, the baseline comparable P.
aeruginosa bacteraemia infection between monotherapy and
combination therapy groups was not established. Confounding factors
in the remaining studies may be attributed to lack of
randomisation, thus leading to incorrect conclusions (39). Another previous meta-analysis also
performed a similar comparison by using β-lactam monotherapy and a
combination of β-lactam and aminoglycosides on immunoreactive
sepsis patients (6); the results
revealed that association of combination therapy with single
treatments was not advantageous in all-cause mortality or other
treatment failure in patient subgroups with P. aeruginosa
bacteraemia infection. By contrast, another study focused on
analysis of patients with gram-negative bacteraemia. Following
subgroup analysis of the results it was identified that combination
antibiotic treatment led to a reduction in the mortality rates of
P. aeruginosa bacteraemia compared with monotherapy, however
these results were not representative of all gram-negative
bacteraemia studied (6,40). As previously revealed, inferior
quality and heterogeneity of studies considered in these
meta-analyses resulted in unreliable clinical data. Differences
among patients were also notable and results often differed
(39). A recent meta-analysis
studied the effects of carbapenem-resistant P. aeruginosa
bacteraemia on mortality (41).
Another meta-analysis study on the benefits of clinical treatment
was conducted through the use of an empirical combination therapy
using β-lactam combined with an aminoglycoside or fluoroquinolones
and β-lactam monotherapy for P. aeruginosa infection
(42). In a subgroup analysis (5
studies) of P. aeruginosa bacteraemia, the results of the
clinical treatment demonstrated no significant difference in
mortality between patients treated with monotherapy and combination
therapy. According to the above variances, a meta-analysis was
conducted in the present study; to the best of our knowledge P.
aeruginosa bacteraemia, although common in patients with
bacteraemia, is not very common in clinical settings. Thus, the
sample size was limited. The present review also indicated limited
clinical reviews and prospective study design. Owing to these
limitations, baseline comparison of P. aeruginosa
bacteraemia infection between monotherapy and combination therapy
was not established. Therefore, difficulty arose from completing
large randomised prospective clinical trials. Patient complications
also differed; multidrug-resistant (MDR) P. aeruginosa
strains became increasingly common and varied in terms of selection
of drug types. Therefore, studies were not analysed according to
specific antibiotics, as the present meta-analysis was performed
with different antimicrobial therapies. In several studies
(13,14,16,18,24),
comparisons between selected empirical antibiotic therapy and
definitive treatment were retrospectively analysed. Other studies
rated the Chronic Health Evaluation score of in-patients (12,16,23,25).
Appropriate treatment involves antibiotic isolation therapy for
certain in-vitro-sensitive agents, especially for
aminoglycoside antibiotic-sensitive patients (19,35). The
use of monotherapy for treatment of P. aeruginosa
bacteraemia was considered inappropriate in previous studies
comparing single and combination therapies (10,15).
Some meta-analyses conducted from the perspective of treatment and
mortality compared effectiveness of combination antibiotics and
monotherapy in clinical treatment of P. aeruginosa (43). The present meta-analysis did not
focus on survival rate and quality evaluation. A limitation of the
present study was the lack of scope in comparing study type and
treatment selection. For patients with MDR bacterial infection and
P. aeruginosa, providing combination antibiotic therapy may
improve results as this method increases possibility of appropriate
treatment (42). In addition to the
appropriate choice of empirical treatment, the severity of
complications is another risk factor that may also affect mortality
rate of patients during bacterial infections including P.
aeruginosa (42). Combination
therapy with P. aeruginosa also presents potential risks,
particularly drug toxicities, including aminoglycoside antibiotics
associated with human renal toxicity (6). Likelihood of repeated infection in
clinical patients and the increased cost must also be considered in
comparing combination therapy with monotherapy.
Limitations of meta-analysis conducted in the
present study were recognised. The quality of included studies may
be questioned due to incomplete or inaccurate data collection. The
research on adjustment of these confusing factors is limited and
therefore cannot be studied for potential co-founder influence,
including severity of disease and potential for concurrent
conditions. The funnel plot and Egger's test indicated a
possibility of publication bias, however trim-and-fill analysis
revealed that results did not change. Only sensitivity analysis and
evaluation, patient source, study types, treatment options and
mortality were analysed. Finally, only studies published in English
were included. This may introduce language bias, possibly resulting
in incomplete study and thus reducing accuracy of analysis of the
treatment results.
In conclusion, the results demonstrated no
significant difference in mortality between patients administered
with combined antibiotic or monotherapy treatment against P.
aeruginosa bacteraemia. Combination therapy may be associated
with clinical treatment of monotherapy, particularly when used in
empirical therapy. These results were mainly obtained from
retrospective and secondary studies. Thus, no definite conclusions
may be drawn regarding combination of effectiveness and single
therapy in patients and groups. Relevant evidence obtained was also
limited. Therefore, large-scale and well-designed studies must be
developed and conducted on credibility of treatment mechanisms to
determine whether a causal association exists.
References
|
1
|
Papagheorghe R: Bloodstream infections in
immunocompromised hosts. Roum Arch Microbiol Immunol. 71:87–94.
2012.PubMed/NCBI
|
|
2
|
Samonis G, Vardakas KZ, Maraki S, Tansarli
GS, Dimopoulou D, Kofteridis DP, Andrianaki AM and Falagas ME: A
prospective study of characteristics and outcomes of bacteremia in
patients with solid organ or hematologic malignancies. Support Care
Cancer. 21:2521–2526. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bassetti M, Righi E and Viscoli C:
Pseudomonas aeruginosa serious infections: Mono or combination
antimicrobial therapy? Curr Med Chem. 15:517–522. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Garnacho-Montero J, Sa-Borges M,
Sole-Violan J, Barcenilla F, Escoresca-Ortega A, Ochoa M, Cayuela A
and Rello J: Optimal management therapy for Pseudomonas aeruginosa
ventilator-associated pneumonia: An observational, multicenter
study comparing monotherapy with combination antibiotic therapy.
Crit Care Med. 35:1888–1895. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Micek ST, Lloyd AE, Ritchie DJ, Reichley
RM, Fraser VJ and Kollef MH: Pseudomonas aeruginosa bloodstream
infection: Importance of appropriate initial antimicrobial
treatment. Antimicrob Agents Chemother. 49:1306–1311. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Paul M, Benuri-Silbiger I, Soares-Weiser K
and Leibovici L: Beta lactam monotherapy versus beta
lactam-aminoglycoside combination therapy for sepsis in
immunocompetent patients: Systematic review and meta-analysis of
randomised trials. BMJ. 328:6682004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Morata L, Cobos-Trigueros N, Martínez JA,
Soriano A, Almela M, Marco F, Sterzik H, Núñez R, Hernández C and
Mensa J: Influence of multidrug resistance and appropriate
empirical therapy on the 30-day mortality rate of Pseudomonas
aeruginosa bacteremia. Antimicrob Agents Chemother. 56:4833–4837.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Micek ST, Welch EC, Khan J, Pervez M,
Doherty JA, Reichley RM and Kollef MH: Empiric combination
antibiotic therapy is associated with improved outcome against
sepsis due to Gram-negative bacteria: A retrospective analysis.
Antimicrob Agents Chemother. 54:1742–1748. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Anderson ET, Young LS and Hewitt WL:
Antimicrobial synergism in the therapy of gram-negative rod
bacteremia. Chemotherapy. 24:45–54. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chamot E, Boffi El Amari E, Rohner P and
Van Delden C: Effectiveness of combination antimicrobial therapy
for Pseudomonas aeruginosa bacteremia. Antimicrob Agents Chemother.
47:2756–2764. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bliziotis IA, Petrosillo N, Michalopoulos
A, Samonis G and Falagas ME: Impact of definitive therapy with
beta-lactam monotherapy or combination with an aminoglycoside or a
quinolone for Pseudomonas aeruginosa bacteremia. PLoS One.
6:e264702011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bowers DR, Liew YX, Lye DC, Kwa AL, Hsu LY
and Tam VH: Outcomes of appropriate empiric combination versus
monotherapy for Pseudomonas aeruginosa bacteremia. Antimicrob
Agents Chemother. 57:1270–1274. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Deconinck L, Meybeck A, Patoz P, Van
Grunderbeeck N, Boussekey N, Chiche A, Delannoy PY, Georges H and
Leroy O: Impact of combination therapy and early de-escalation on
outcome of ventilator-associated pneumonia caused by Pseudomonas
aeruginosa. Infect Dis (Lond). 49:396–404. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Paulsson M, Granrot A, Ahl J, Tham J,
Resman F, Riesbeck K and Månsson F: Antimicrobial combination
treatment including ciprofloxacin decreased the mortality rate of
Pseudomonas aeruginosa bacteraemia: A retrospective cohort study.
Eur J Clin Microbiol Infect Dis. 36:1187–1196. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Siegman-Igra Y, Ravona R, Primerman H and
Giladi M: Pseudomonas aeruginosa bacteremia: An analysis of 123
episodes, with particular emphasis on the effect of antibiotic
therapy. Int J Infect Dis. 2:211–215. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim YJ, Jun YH, Yang RK, Park KG, Park YJ,
Kang JY and Kim SI: Risk factors for mortality in patients with
Pseudomonas aeruginosa bacteremia; retrospective study of impact of
combination antimicrobial therapy. BMC Infect Dis. 14:1612014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Samonis G, Vardakas KZ, Kofteridis DP,
Dimopoulou D, Andrianaki AM, Chatzinikolaou I, Katsanevaki E,
Maraki S and Falagas ME: Characteristics, risk factors and outcomes
of adult cancer patients with extensively drug-resistant
Pseudomonas aeruginosa infections. Infection. 42:721–728. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Peña C, Suarez C, Ocampo-Sosa A, Murillas
J, Almirante B, Pomar V, Aguilar M, Granados A, Calbo E,
Rodríguez-Baño J, et al: Effect of adequate single-drug vs
combination antimicrobial therapy on mortality in Pseudomonas
aeruginosa bloodstream infections: A post Hoc analysis of a
prospective cohort. Clin Infect Dis. 57:208–216. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hilf M, Yu VL, Sharp J, Zuravleff JJ,
Korvick JA and Muder RR: Antibiotic therapy for Pseudomonas
aeruginosa bacteremia: Outcome correlations in a prospective study
of 200 patients. Am J Med. 87:540–546. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Leibovici L, Paul M, Poznanski O, Drucker
M, Samra Z, Konigsberger H and Pitlik SD: Monotherapy versus
beta-lactam-aminoglycoside combination treatment for gram-negative
bacteremia: A prospective, observational study. Antimicrob Agents
Chemother. 41:1127–1133. 1997.PubMed/NCBI
|
|
21
|
Kuikka A and Valtonen VV: Factors
associated with improved outcome of Pseudomonas aeruginosa
bacteremia in a Finnish university hospital. Eur J Clin Microbiol
Infect Dis. 17:701–708. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mendelson MH, Gurtman A, Szabo S, Neibart
E, Meyers BR, Policar M, Cheung TW, Lillienfeld D, Hammer G, Reddy
S, et al: Pseudomonas aeruginosa bacteremia in patients with AIDS.
Clin Infect Dis. 18:886–895. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Park SY, Park HJ, Song MM, Park KH, Chong
YP, Kim MN, Kim SH, Lee SO, Kim YS, Woo JH and Choi SH: Impact of
adequate empirical combination therapy on mortality from bacteremic
Pseudomonas aeruginosa pneumonia. BMC Infect Dis. 12:3082012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yoon YK, Kim HA, Ryu SY, Lee EJ, Lee MS,
Kim J, Park SY, Yang KS and Kim SW; Antibiotic Stewardship
StudyGroup, : Tree-structured survival analysis of patients with
Pseudomonas aeruginosa bacteremia: A multicenter observational
cohort study. Diagn Microbiol Infect Dis. 87:180–187. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tan SH, Teng CB, Ng TM and Lye DC:
Antibiotic therapy and clinical outcomes of Pseudomonas aeruginosa
(PA) bacteraemia. Ann Acad Med Singapore. 43:526–534.
2014.PubMed/NCBI
|
|
26
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang WS, Va P, Wong MY, Zhang HL and Xiang
YB: Soy intake is associated with lower lung cancer risk: Results
from a meta-analysis of epidemiologic studies. Am J Clin Nutr.
94:1575–1583. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yang Y, Zhang D, Feng N, Chen G, Liu J,
Chen G and Zhu Y: Increased intake of vegetables, but not fruit,
reduces risk for hepatocellular carcinoma: A meta-analysis.
Gastroenterology. 147:1031–1042. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhang Y, Zheng QJ, Wang S, Zeng SX, Zhang
YP, Bai XJ and Hou TY: Diabetes mellitus is associated with
increased risk of surgical site infections: A meta-analysis of
prospective cohort studies. Am J Infect Control. 43:810–815. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gu WJ, Wang F, Tang L and Liu JC:
Single-dose etomidate does not increase mortality in patients with
sepsis: A systematic review and meta-analysis of randomized
controlled trials and observational studies. Chest. 147:335–346.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ownby RL, Crocco E, Acevedo A, John V and
Loewenstein D: Depression and risk for Alzheimer disease:
Systematic review, meta-analysis, and metaregression analysis. Arch
Gen Psychiatry. 63:530–538. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lo CK, Mertz D and Loeb M:
Newcastle-Ottawa Scale: Comparing reviewers' to authors'
assessments. BMC Med Res Methodol. 14:452014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Larsson SC, Orsini N and Wolk A: Vitamin
B6 and risk of colorectal cancer: A meta-analysis of prospective
studies. JAMA. 303:1077–1083. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Higgins JP and Green S: Cochrane Handbook
for Systematic Reviews of Interventions Version 5.1.0. The Cochrane
Collaboration; 2011, http://handbook.cochrane.orgMarch. 2011
|
|
36
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sterne JA and Egger M: Funnel plots for
detecting bias in meta-analysis: Guidelines on choice of axis. J
Clin Epidemiol. 54:1046–1055. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Traugott KA, Echevarria K, Maxwell P,
Green K and Lewis JS II: Monotherapy or combination therapy? The
Pseudomonas aeruginosa conundrum. Pharmacotherapy. 31:598–608.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chatzinikolaou I, Abi-Said D, Bodey GP,
Rolston KV, Tarrand JJ and Samonis G: Recent experience with
Pseudomonas aeruginosa bacteremia in patients with cancer:
Retrospective analysis of 245 episodes. Arch Intern Med.
160:501–509. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Safdar N, Handelsman J and Maki DG: Does
combination antimicrobial therapy reduce mortality in Gram-negative
bacteraemia? A meta-analysis. Lancet Infect Dis. 4:519–527. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhang Y, Chen XL, Huang AW, Liu SL, Liu
WJ, Zhang N and Lu XZ: Mortality attributable to
carbapenem-resistant Pseudomonas aeruginosa bacteremia: A
meta-analysis of cohort studies. Emerg Microbes Infect. 5:e272016.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Vardakas KZ, Tansarli GS, Bliziotis IA and
Falagas ME: β-Lactam plus aminoglycoside or fluoroquinolone
combination versus β-lactam monotherapy for Pseudomonas aeruginosa
infections: A meta-analysis. Int J Antimicrob Agents. 41:301–310.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hu Y, Li L, Li W, Xu H, He P, Yan X and
Dai H: Combination antibiotic therapy versus monotherapy for
Pseudomonas aeruginosa bacteraemia: A meta-analysis of
retrospective and prospective studies. Int J Antimicrob Agents.
42:492–496. 2013. View Article : Google Scholar : PubMed/NCBI
|