Introduction
Traumatic brain injury has one of the highest
incidences among all types of trauma, with mortality rate as high
as 30–50% (1). Brain injury can be
categorized into four types: Diffuse axonal injury, diffuse brain
swelling, diffuse microvascular injury and hypoxic brain damage
(2). At the early stage of brain
injury, local nerve cells and tissues are damaged, leading to
blood-brain barrier damage and multiple cytokine releases (3). Cytokines serve key roles in the
pathogenesis and outcome of brain injury (4).
Insufficient supply of oxygen (5) and inflammation (4) are vital in the development of brain
injury. An insufficient supply of oxygen is hard to correct at
normal temperature and pressure (6).
However, in hyperbaric oxygen (HBO) therapy, the diffused oxygen
content can increase up to 20 times, with increased oxygen
difference between alveoli and pulmonary vein (7,8).
Therefore, brain tissue oxygen partial pressure and oxygen storage
capacity are significantly improved, thereby reducing cerebral
hypoxia, preventing cerebral hypoxic-ischemic brain damage and
improving brain circulation (9). It
has previously been demonstrated that oxygen supply is closely
associated with prognosis after brain injury (10).
Brain injury produces multiple cytokines from the
site of injury or the whole brain, including interleukins (ILs)
(11), tumor necrosis factor-α
(TNF-α) (12), interferons (13) and basic fibroblast growth factor
(14). These cytokines serve
critical roles at different stages of brain injury. For example,
TNF-α can directly activate and induce leukocyte endothelial cell
adhesion at the site of injury (15). Then, the leukocytes release a series
of chemical factors, causing tissue damage (16).
In the present study, the levels of serum TNF-α and
IL-1β were detected before and after HBO combined with nimodipine
treatment in patients with diffuse brain injury. The efficacy of
HBOHBO combined with nimodipine as a target intervention in the
early stages of trauma was evaluated.
Materials and methods
Subjects
A total of 80 patients with brain injury were
recruited from October 2013 to October 2015 within 24 h after
injury. Patients included 62 males and 18 females, with ages
ranging from 18 to 45 years. The characteristics of included
subjects are shown in Table I.
Patients were included if they: i) were diagnosed by CT or MRI; ii)
had no other injuries; iii) had a Glasgow Coma Scale (GCS) score of
5–8 (17); iv) had no history of
major underlying diseases at admission; and v) gave consent for
treatment. Patients were excluded if they: i) were <18 years or
>45 years old; ii) had any underlying brain diseases, such as
brain tumors; iii) had a history of major chronic diseases,
including hypertension, coronary heart disease, diabetes or liver
and kidney dysfunction; iv) were pregnant or breastfeeding; v) had
a history of epilepsy; vi) had multiple drug allergies; and vii)
had other factors that could influence GCS score, including mental
retardation. Prior written and informed consent was obtained from
every patient. The study was approved by the ethics review board of
the Second Hospital of Hebei Medical University (Shijiazhuang,
China).
 | Table I.General characteristics of
subjects. |
Table I.
General characteristics of
subjects.
| Characteristic | Group A | Group B | Group C | Group D |
|---|
| n | 20 | 20 | 20 | 20 |
| Sex
(male/female) | 14/6 | 17/3 | 15/5 | 16/4 |
| Age (years) | 39.15±3.65 | 40.25±3.14 | 38.26±2.78 | 40.19±2.25 |
| Time from injury to
admission (h) | 5.15±2.04 | 4.84±2.16 | 4.32±2.28 | 4.60±2.14 |
| GCS at admission | 6.03±1.34 | 6.42±1.56 | 6.27±1.48 | 6.24±1.85 |
| Cause of injury
(n) |
|
|
|
|
| Car accident | 13 | 12 | 11 | 15 |
| Fall | 2 | 2 | 2 | 1 |
| Crashing | 3 | 4 | 5 | 3 |
| Crash | 1 | 1 | 2 | 1 |
| Other | 1 | 1 | 0 | 0 |
| Type of brain injury
(n) |
|
|
|
|
| Brain contusion and
laceration | 7 | 8 | 6 | 6 |
| Intracranial
hematoma | 5 | 6 | 6 | 5 |
| Subarachnoid
hemorrhage | 5 | 4 | 4 | 4 |
| Primary brain stem
injury | 1 | 0 | 1 | 1 |
| Diffuse axonal
injury | 2 | 2 | 3 | 4 |
Grouping and treatment
All patients were randomly divided into four groups
(n=20 in each group): Group A, conventional treatment; Group B,
conventional treatment + nimodipine; Group C, conventional
treatment + HBO therapy; and Group D, conventional treatment +
nimodipine + HBO therapy.
Patients in Group A received conventional treatment,
which included dehydration agents, corticoids, vitamins, hemostatic
agents and neurotrophic drugs, including 250 ml mannitol (20%),
i.v., for consecutive 5 days (18),
and aescine sodium (10–20 mg in 0.9% NaCl solution, in a total
volume of 100 ml) via i.v., once or twice each day (19). Hematoma or decompression craniectomy
procedures were performed if necessary.
In addition to conventional therapy, patients in
Group B received infusion of nimodipine (8 mg in 500 ml of 5%
glucose) after exclusion of further bleeding and hematoma formation
by computed tomography (CT) scan. The nimodipine was administered
at 1 mg/h within the first 2 h, and this was increased to 2 mg/h if
vital signs remained stable for a full course of 14 days. If the
vital signs were unstable, the observation was suspended.
In addition to conventional therapy, patients in
Group C received HBO therapy. Patients inhaled pure oxygen for 30
min through an oxygen mask at a pressure of 0.2 MPa in an HBO
chamber. After a break of 10 min, patients re-inhaled pure oxygen
for 20 min. Then, the pressure was reduced to 0.15 MPa and patients
inhaled pure oxygen for 10 min. The pressure then continued
decreasing to 0.1 MPa over 15 min. The HBO therapy was administered
once a day for 20 days.
In addition to conventional therapy, patients in
Group D received the conventional therapy combined with HBO therapy
and infusion of nimodipine (8 mg in 500 ml of 5% glucose) after
exclusion of further bleeding and hematoma formation by CT scan.
Detailed procedures were the same as those for Group B.
Sampling and detection of serum TNF-α
and IL-1β
Blood samples were drawn before treatment and at 8,
24, 48 and 72 h after injury. The blood sample was placed in 45°C
water bath for 10 min, followed by centrifugation at 955.78 × g for
5 min. Detection of TNF-α and IL-1β levels was performed using
Human TNF-α and IL-1β ELISA kits (ml028611 mibio and ml001543
mibio, Hengyuan Biotech, Shanghai, China). All samples were
detected immediately. Briefly, all samples were reacted at 37°C for
30 min; enzyme-labeled reagents were added after washing 5 times
and reacted at 37°C for 30 min. Subsequently, chromogenic reagents
were added after washing 5 times and reacted at 37°C for 10 min.
The OD value at 450 nm was recorded 15 min after the buffer was
added.
CT values
Head CT was performed using a Brilliance iCT machine
(Philips Medical Systems B.V., Eindhoven, The Netherlands). The CT
values were recorded.
Detection of cerebral artery blood
flow velocity (VmMCA) and GCS score
Transcranial Doppler ultrasound was used to measure
bilateral middle VmMCA and GCS scores were calculated for all
patients at 8, 24, 48, and 72 h after treatment. GCS scores were
based on evaluation of eye movement, language ability and body
movements, and were categorized into 3 types: Light coma (13–14
points), moderate coma (9–12 points) and deep coma (3–8 points)
(5).
Statistical analysis
SPSS 18.0 (SPSS, Inc., Chicago, IL, USA) was used
for statistical analysis. Quantitative data are expressed as the
mean ± standard deviation and were analyzed using
independent-sample student's t-tests. Group data were compared
using one-way analysis of variance, and pairwise comparisons were
performed using the Student-Newman-Keuls test. Qualitative data
were analyzed using the χ2 test. Correlations were
analyzed using Pearson's correlation coefficient. P<0.05 was
considered to indicate a statistically significant difference.
Results
Serum TNF-α content
To determine the dynamic changes in TNF-α level,
serum TNF-α level was detected before treatment and at 8, 24, 48
and 72 h after treatment. As shown in Table II, at all time points, the serum
TNF-α level was the lowest in Group D. Compared with Group A, the
level of TNF-α was significantly lower in Groups B, C and D at 8,
24, 48 and 72 h after treatment (P<0.05). In all groups, the
serum TNF-α level was low before treatment, peaked at 8 h after
treatment and then gradually decreased at 24, 48 and 72 h after
treatment. Compared with at 8 h, TNF-α levels were increased in the
early stage of trauma and decreased after HBO therapy combined with
nimodipine treatment. These results indicated that the TNF-α levels
decreased after HBO therapy combined with nimodipine treatment,
which suggested that the TNF-α may be involved in the pathgensesis
of brain injury.
| Table II.Serum tumor necrosis factor-α content
(µg/l). |
Table II.
Serum tumor necrosis factor-α content
(µg/l).
| Group | Before treatment | 8 h after
treatment | 24 h after
treatment | 48 h after
treatment | 72 h after
treatment |
|---|
| Group A |
120.2±3.5a |
135.4±2.6 |
125.8±2.5a |
110.4±3.5a |
102.4±2.7a |
| Group B |
115.3±2.4a,b |
129.1±2.3b |
120.3±2.5a,b |
102.3±2.5a,b |
95.6±2.2a,b |
| Group C |
113.7±2.3a,b |
125.3±2.1b |
110.3±2.2a,b |
97.5±1.8a,b |
88.7±2.4a,b |
| Group D |
110.5±2.3a,b |
119.8±3.2b |
98.2±2.2a,b |
89.5±2.1a,b |
75.5±2.2a,b |
Serum IL-1β content
To determine the dynamic changes in IL-1βs, serum
IL-1β level was detectedbefore before treatment and at 8, 24, 48
and 72 h after treatment. As shown in Table III, the serum IL-1β level was
significantly decreased in Groups B, C and D at alltime pointsall
scompared with Group A (P<0.05). In all groups, the serum IL-1β
level peaked at 8 h after treatment and gradually decreased at 24,
48 and 72 h after treatment. Compared with at 8 h, IL-1β level was
significantly lower before treatment and at 24, 48 and 72 h after
treatment (P<0.05). These results indicated that IL-1β increases
in the early stage of trauma and may be involved in the
pathogenesis of brain injury.
| Table III.Serum interleukin-1β content
(µg/l). |
Table III.
Serum interleukin-1β content
(µg/l).
| Group | Before
treatment | 8 h after
treatment | 24 h after
treatment | 48 h after
treatment | 72 h after
treatment |
|---|
| Group A |
125.2±2.5a |
140.2±2.6 |
132.8±2.1a |
119.4±2.5a |
110.4±2.3a |
| Group B |
120.3±2.4a,b |
135.1±2.5b |
128.3±2.4a,b |
110.3±2.3a,b |
105.6±2.5a,b |
| Group C |
115.7±2.1a,b |
129.3±2.4b |
120.3±2.5a,b |
104.5±2.8a,b |
100.7±2.2a,b |
| Group D |
110.5±2.2a,b |
120.8±2.2b |
115.2±2.3a,b |
98.5±2.3a,b |
89.5±2.1a,b |
VmMCA comparisons
To determine the vascular contraction after acute
brain injury, VmMCA was measured before treatment and at 8, 24, 48
and 72 h after treatment. In each group, the VmMCA was highest at
24 h (Table IV). At all time
points, the VmMCA was significantly lower in Groups B, C and D
compared with Group A (P<0.05). In addition, VmMCA was
significantly lower before treatment and at 48 and 72 h after
treatment compared with 8 h after treatment (P<0.05). VmMCA was
significantly higher at 24 h after treatment compared with 8 h
after treatment (P<0.05). These findings suggest that nimodipine
could dilate cerebral blood vessels, relieve spasms and slow the
blood flow in the bilateral middle cerebral arteries.
| Table IV.Comparisons of cerebral arterial
blood flow velocity (cm/s). |
Table IV.
Comparisons of cerebral arterial
blood flow velocity (cm/s).
| Group | Before
treatment | 8 h after
treatment | 24 h after
treatment | 48 h after
treatment | 72 h after
treatment |
|---|
| Group A |
78.2±1.5a |
125.12±2.1 |
168.8±1.1a |
108.24±2.2a |
86.4±2.1a |
| Group B |
77.1±2.1a–c |
103.1±2.1b |
141.3±1.4a–c |
85.3±1.3a–c |
77.6±1.5a–c |
| Group C |
82.5±1.1a,b |
114.3±1.4b |
158.3±1.5a,b |
96.5±1.8a,b |
82.7±1.2a,b |
| Group D |
75.5±1.2a–c |
91.8±1.2b |
130.2±1.3a–c |
76.5±1.3a,b,c |
74.5±2.1a–c |
GCS score
To determine the severity of brain damage, GCS score
was evaluated before treatment and at 8, 24, 48 and 72 h after
treatment. At all time points, the GCS score in Groups B, C and D
was significantly increased compared with Group A (P<0.05;
Table V). The largest increases were
in Group D. In all groups, the GCS score gradually increased over
time, with the exception of Groups B, C and D at 72 h, which
exhibited slight decreases compared with 48 h. In all groups, the
GCS score at 24 h, 48 h and 72 h after treatment was significantly
higher compared with 8 h after treatment (P<0.05). These results
indicated that patient brain damage gradually recovered after brain
injury. Furthermore, when compared with the conventional therapy,
the bilateral carotid blood flow velocity is faster in the
craniocerebral injury when treated with nimodipine combined with
HBO therapy.
| Table V.Glasgow Coma Scale scores. |
Table V.
Glasgow Coma Scale scores.
| Group | Before
treatment | 8 h after
treatment | 24 h after
treatment | 48 h after
treatment | 72 h after
treatment |
|---|
| Group A |
7.03±1.2a |
7.41±2.1 |
8.80±1.1a |
9.52±2.2a |
10.05±1.1a |
| Group B |
6.24±1.3a,b |
7.65±1.7b |
9.92±1.4a,b |
11.15±1.3a,b |
10.96±1.3a,b |
| Group C |
6.53±1.3a,b |
7.92±1.4b |
10.19±1.5a,b |
11.36±1.3a,b |
11.20±1.2a,b |
| Group D |
6.58±1.2a,b |
8.26±1.2b |
12.21±1.4a,b |
13.44±1.3a,b |
12.65±2.1a,b |
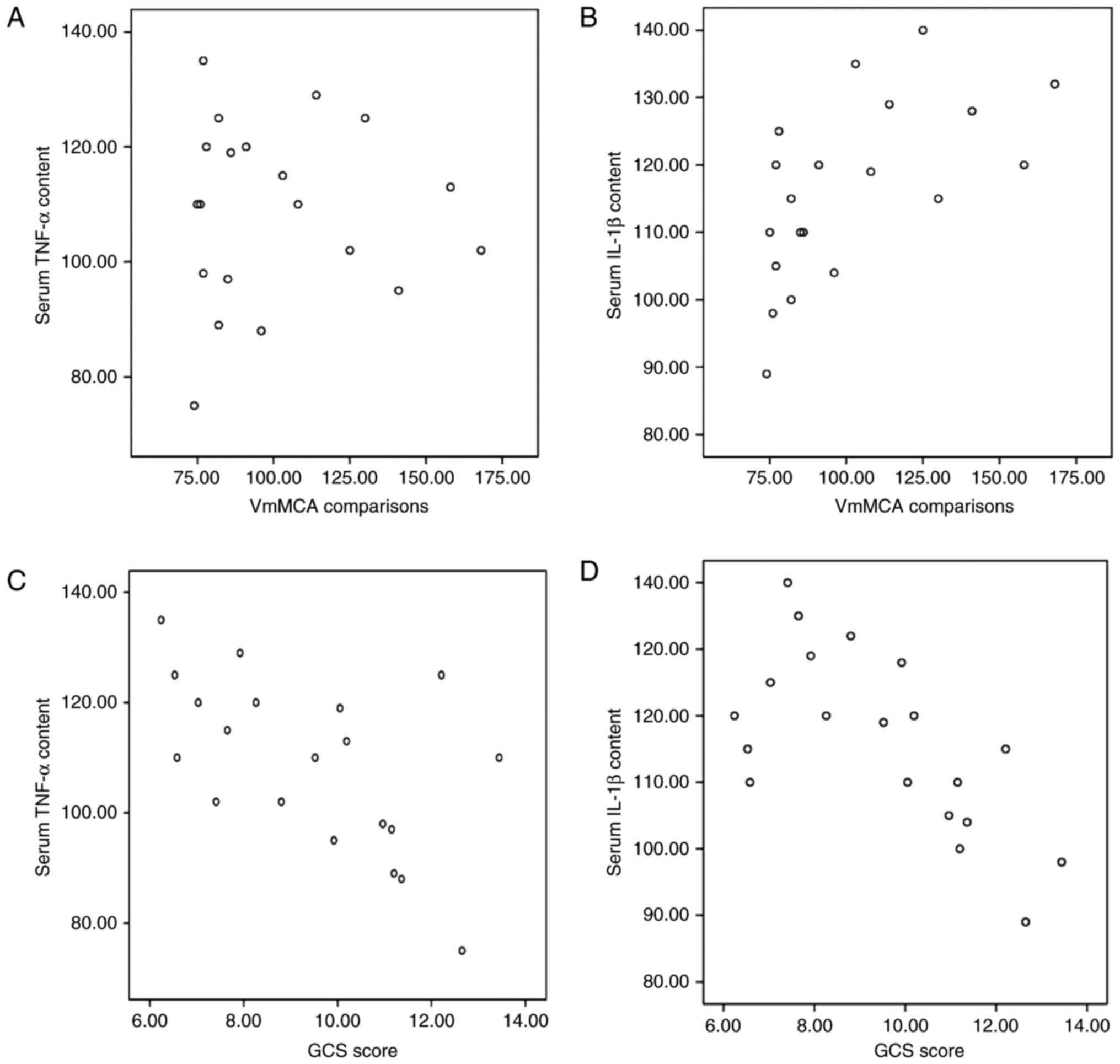
Correlation between serum TNF-α/IL-1β
and VmMCA or GCS
Correlation analyses were performed to evaluate the
association between serum TNF-α/IL-1β and VmMCA or GCS. Serum TNF-α
and IL-1β levels were positively correlated with VmMCA (r=0.38 and
r=0.73, respectively; P<0.05; Fig. 1A
and B). Serum TNF-α and IL-1β levels were negatively correlated
with GCS (r=−0.89 and r=−and 0.78, respectively; P<0.05;
Fig. 1C and D). These results
indicate that serum TNF-α and IL-1β levels are positively
correlated with VmMCA and negatively correlated with GCS.
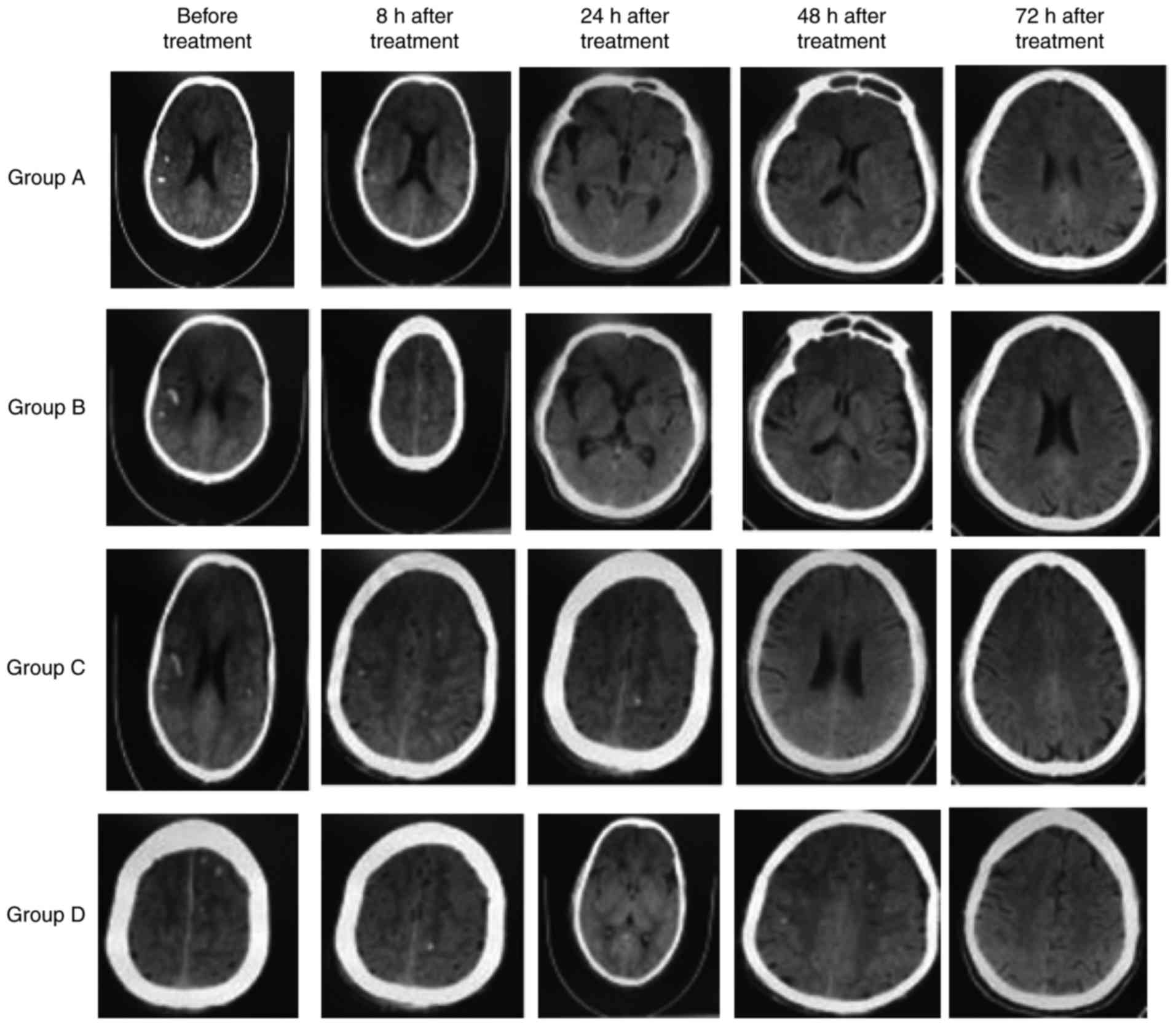
Head CT
To determine brain structural change, head CT was
performed before treatment and at 8, 24, 48 and 72 h after
treatment. Punctate hemorrhage was observed in all groups on CT
with a value of 68±2.37 HU before treatment (Table VI). Over time, punctate hemorrhage
was reduced in all groups (Fig. 2).
CT values also decreased over time in all groups. Compared with
before treatment, the CT values at 8, 24, 48 and 72 h after
treatment were significantly decreased (P<0.05; Table VI). Furthermore, Groups A, B and C
exhibited significantly higher CT values at all time points
compared with group D (P<0.05). These results indicated that
patients treated with nimodipine and HBO therapy exhibit fewer
brain structural changes compared with either treatment alone.
| Table VI.Computed tomography values (HU). |
Table VI.
Computed tomography values (HU).
| Group | Before
treatment | 8 h after
treatment | 24 h after
treatment | 48 h after
treatment | 72 h after
treatment |
|---|
| Group A |
68.2±2.3a |
61.2±2.3a,b |
55.6±2.1a,b |
52.4±2.5a,b |
45.4±2.1a,b |
| Group B |
67.3±2.1a |
58.1±2.1a,b |
52.3±2.2a,b |
48.2±2.2a,b |
42.6±2.7a,b |
| Group C |
66.7±2.5a |
55.3±2.2a,b |
50.3±2.1a,b |
45.5±2.4a,b |
40.7±2.2a,b |
| Group D |
67.5±2.2 |
52.4±2.4b |
48.2±2.5b |
42.3±2.3b |
37.5±2.3b |
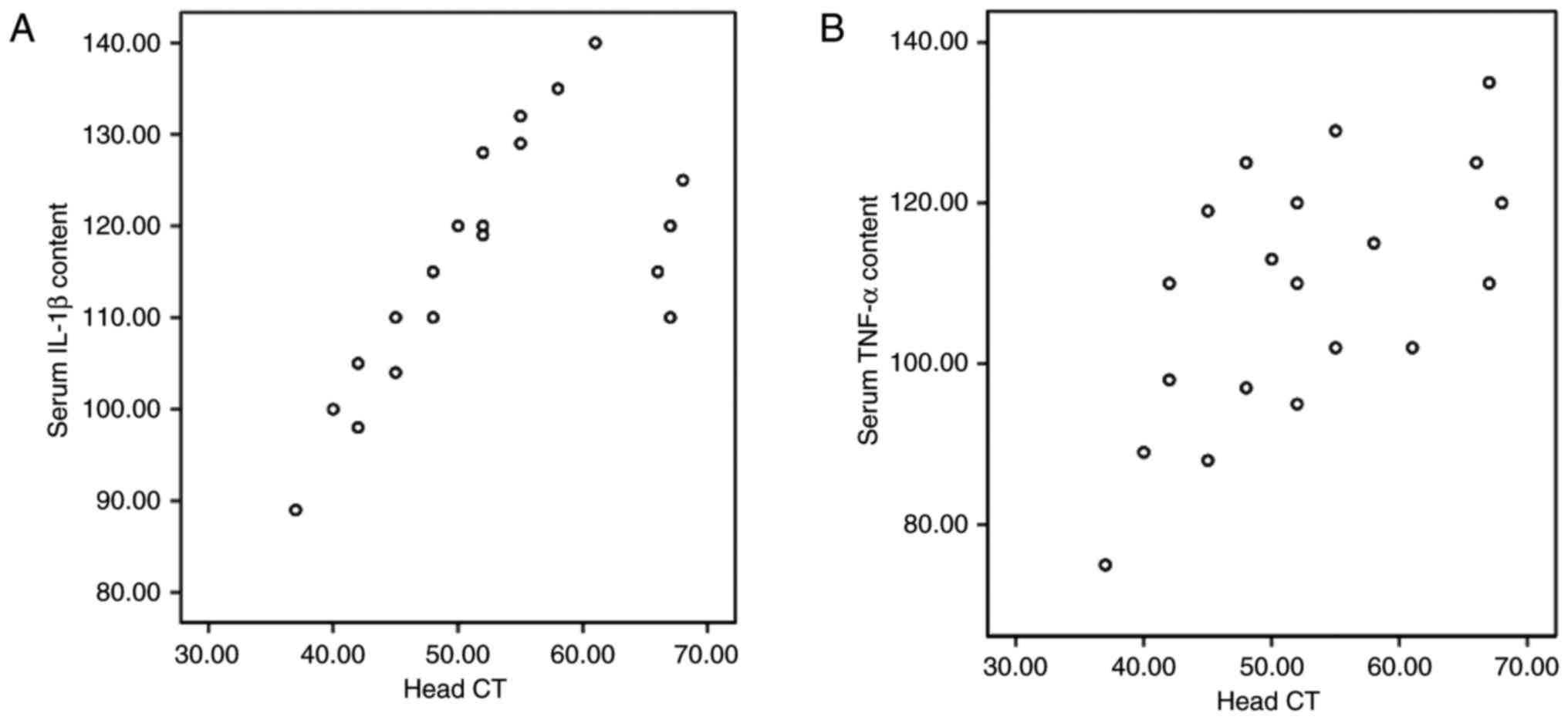
Correlation between serum TNF-α/IL-1β
and CT values
Correlation analyses were performed to evaluate the
association between serum TNF-α/IL-1β and CT values. Serum TNF-α
and IL-1β were positively correlated with CT value (r=0.73 and
r=0.89, respectively; P<0.05), as shown in Fig. 3. These results indicated that serum
TNF-α and IL-1β levels are positively correlated with brain
structural damage. Furthermore, the findings suggest that HBO
therapy could alleviate the hypoxic condition in the craniocerebral
injury, and nimodipine could improve the circulation and reduce the
production of TNF-α.
Discussion
Cerebral ischemia, hypoxia and inflammation are key
factors in brain damage after brain injury (20). Overexpression of inflammatory factors
after injury leads to environmental changes for neurons, resulting
in neuronal degeneration (21).
TNF-α elevates early after injury and is involved in the
inflammatory response (22). TNF-α
is produced by activated monocytes or macrophages in nerve tissues
such as astrocytes, microglia and neurons (22). The elevated TNF-α level in
cerebrospinal fluid and plasma after brain injury is closely
associated with disease severity (13). Leukocyte accumulation and
inflammation infiltration significantly impact the scope and extent
of brain damage (23). TNF-α can
regulate the activity of vascular endothelial cells and vascular
inflammation (12) and promote the
expression of adhesion molecules in endothelial cells. This leads
to leukocyte adhesion, aggregation and migration from capillaries
to the brain, thereby activating microglia and subsequently causing
damage (24).
HBO therapy is the inhalation of pure oxygen at
greater than normal atmospheric pressure (9). HBO treatment increases the oxygen
content and storage in brain tissue and cerebrospinal fluid,
reduces cerebral edema and intracranial pressure, promotes
functional recovery of neurons, particularly dilate vertebral
arteries to increase cerebral blood flow, restores and maintains
cell pump function and improves microcirculation (25–29). In
the present study, punctate hemorrhage was detected in all groups
before treatment. Over the treatment period, punctate hemorrhage
and CT values gradually decreased, with Group D exhibiting the
largest decrease. The serum levels of TNF-α and IL-1β were
significantly lower in Groups B, C and D compared with Group A.
Higher CT values were identified to be correlated with higher TNF-α
and IL-1β levels. These results suggest that HBO treatment can
enhance hematoma absorption to repair brain damage.
Calcium antagonists can disrupt calcium flow from
the outside to the inside of vascular smooth muscle cells, reduce
the cerebral vasospasm to regulate vascular muscle tension,
increase blood flow for brain tissue perfusion, prevent secondary
damage, and improve microcirculation to protect brain tissue
(30). Nimodipine is a type of
fat-soluble dihydropyridine calcium channel blocker that can
permeate the blood-brain barrier, block calcium channels to prevent
calcium influx, and promote Ca2+ release, thereby
reducing the intracellular calcium concentration (31). In the present study, the VmMCA was
lower in Group B and D compared with Group A and C, and VmMCA was
positively correlated with serum TNF-α and IL-1β decrease. These
results are indicative of the selective duration of dilation and
protection effects of nimodipine on cerebral blood vessels
(32). GCS scores increased in all
groups over the treatment period, with Group D exhibiting the
largest increase. GCS scores were positively correlated with serum
TNF-α and IL-1β levels. These results indicate that that HBO with
nimodipine may influence the serum content of TNF-α and IL-1β.
Thus, early cytokine intervention may be beneficial in improving
prognosis after diffuse brain injury.
Physiological changes in patients with diffuse brain
injuries include secondary cerebral ischemia and hypoxia, brain
tissue edema, release of inflammatory cell media and
microcirculation disorder. The pathological changes mainly include
cerebral contusion, axonal injury and increased intracranial
pressure. Notably, oxygen supply and circulation improvement are
important factors involved in the recovery of damaged brain tissue.
In the present study, the results suggested that nimodipine
combined with HBO therapy could effectively alleviate cerebral
ischemia and hypoxia, improve the cerebral circulation, and greatly
elevate the salvage rate. Because nimodipine could relieve the
cerebral vasospasm and increase the cerebral blood flow, its
treatment inevitably leads to increased cerebral blood volume and
cerebral edema. However, HBO therapy does have limitations due to
its association with barotrauma, oxygen poisoning and
compressed-airsickness in the treatment of coma patients (33), particularly those with mechanical
ventilation. Therefore, further in-depth studies are still required
to optimize the treatment options for the diffuse brain injury,
particularly for coma patients.
Acknowledgements
The authors would like to thank Professor Xiaolu
Wang at The Second Hospital of Hebei Medical University
(Shijiazhuang, China) for his technical assistance.
Funding
No funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FW and JW made substantial contributions to
conception and design. JS performed the trial and was a major
contributor in writing the manuscript. JZ obtained the patient data
regarding the diffuse brain injury. GZ made substantial
contributions to analysis and interpretation of data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Prior written and informed consent was obtained from
every patient. The study was approved by the ethics review board of
the Second Hospital of Hebei Medical University (Shijiazhuang,
China).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Li Yu and Du Yanli: High field magnetic
resonance diffusion tensor imaging in the evaluation of severe
traumatic brain injury. Zhonghua Lin Chuang Yi Shi Za Zhi (Dian zi
ban). 9:4103–4104. 2013.(In Chinese).
|
|
2
|
Graham DI, McIntosh TK, Maxwell WL and
Nicoll JA: Recent advances in neurotrauma. J Neuropathol Exp
Neurol. 59:641–651. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Vink R, Nimmo AJ and Cemak I: An overview
of new and novel pharmaco theraies for use in traumatic brain
injury. Clin Exp Pharmacol Physiol. 28:919–921. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
He XS: Recognizing the study on
inflammatory responses post traumatic brain injury. J Fourth
Military Med University. 25:7692004.
|
|
5
|
Teasdale G and Jennett B: Assessment of
coma and impaired consciousness. A practical seale. Lancet.
2:81–84. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hardy P, Johnston KM, De Beaumont L,
Montgomery DL, Lecomte JM, Soucy JP, Bourbonnais D and Lassonde M:
Pilot case study of the therapeutic potential of hyperbaricoxygen
therapy on chronic brain injury. J Neurol Sci. 253:94–105. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang HW and Liao SC: The clinical analysis
of earlyhyperbaric oxygen treatment for postoperative acute brain
injury. J Yanan University (Medical Sciences). 9:25–28. 2011.(In
Chinese).
|
|
8
|
Yu SN, He GS and Cai SZ: The clinical
analysis of earlyhyperbaric oxygen treatment for postoperative
severe brain injury. Chin J Clin Neurosurgery. 18:306–308. 2013.(In
Chinese).
|
|
9
|
Sukoff MH: Effect of hyperbaric
oxygenation. J Neurosurg. 95:544–546. 2001.PubMed/NCBI
|
|
10
|
Xiong Y, Peterson PL and Lee CP:
Alterations in cerebral energy metabolism induced by traumatic
brain injury. Neurol Res. 23:129–138. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Suehiro E, Fujisawa H, Akimura T, Ishihara
H, Kajiwara K, Kato S, Fujii M, Yamashita S, Maekawa T and Suzuki
M: Increased matrix metalloproteinase-9 in blood in association
with activation of interleukin-6 after traumatic brain injury:
Influence of hypothermic therapy. J Neumtrauma. 21:1706–1711. 2004.
View Article : Google Scholar
|
|
12
|
Merrill JE and Benveniste EN: Cytokines in
inflammatory brain lesion: Helpful and harmful. Trends Neurosci.
19:331–338. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Feng B, Tan ZM and Wang HS: The clinical
importance of tumor necrosis factor in acute brain injury. Chin J
Critical Care Med. 17:14–16. 1997.(In Chinese).
|
|
14
|
Fassbender K, Rossol S, Kammer T,
Daffertshofer M, Wirth S, Dollman M and Hennerici M:
Proinflammotory cytokines in serum of patients with acute cerebral
ischemia: Kinetics of secretion and relation to extent of brain
damage and outcome of disease. J Neurol Sci. 122:135–139. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhu T, Yao Z and Yuan HN: The changes of
TNF-α, IL-1β and IL-6 levels in postoperative rats. Chin J Trauma.
14:367–369. 1998.(In Chinese).
|
|
16
|
Si QJ: The function of Tumor necrosis
factor in myocardial ischemia/reperfusion injury. J Chin PLA
Postgraduate Med School. 15:220–222. 1994.(In Chinese).
|
|
17
|
Li H, Yang X, Shi W, Ma Z, Feng G, Wang Q,
Shen L and Xie C: Protective effects of nimodipine on
cerebrovascular function in chronic alcoholic encephalopathy. Int J
Mol Med. 33:201–208. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yang Y, Zhang Y, Wang Z, Wang S, Gao M, Xu
R, Liang C and Zhang H: Attenuation of acute phase injury in rat
intraxranial hemorrhage by cerebrolysin that inhibits brain edema
and inflammatory response. Neurochem Res. 41:748–757. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim H, Edwards NJ, Choi HA, Chang TR, Jo
KW and Lee K: Treatment strategies to attenuate perihematomal edema
in patients with intracerebral hemeorrhage. World Neurosurg.
94:32–41. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rothwell N: Interleukin-1 and neuronal
injury: Mechanisms, modification, and therapeutic potential. Brain
Behav Immun. 17:152–157. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Patel HC, Boutin H and Allan SM:
Interleukin-1 in the brain: mechanisms of action in acute
neurodegeneration. Ann NY Acad Sci. 992:39–47. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schoami E, Gallily R, Mechonlam R, Bass R
and Ben-Hur T: Cytokine production the brain following closed head
injury: Dexanabinol (HU-211)isnovel TNF-alpha inhibitor and
effective neuroprotectant. J Neuroimmuno1. 72:169–177. 1997.
View Article : Google Scholar
|
|
23
|
Fassbender K, RossoI S, Kammer T,
Daffertshofer M, Wirth S, Dollman M and Hennerici M:
Proinflammatory cytokines in serum of patients with acute cerebral
ischemia: Kinetics of secretion and relation to extent of brain
damage and outcome of disease. J Neurol Sci. 122:135–139. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hardy P, Johnston KM, De Beaumont L,
Montgomery DL, Lecomte JM, Soucy JP, Bourbonnais D and Lassonde M:
Pilot case study of the therapeutic potential of hyperbaric oxygen
therapy on chronic brain injury. J Neurol Sci. 253:94–105. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Philippon B and Munsch RC: Variations of
the cerebral blood flow after hyperbaric oxygenation in traumatic
coma. Neurochirurgie. 21:483–492. 1975.(In French). PubMed/NCBI
|
|
27
|
Isakov IuV, Anan'ev GV, Aide KhB and
Korol'kov IuI: Use of hyperbaric oxygenation in various
complications of craniocerebral injury in the acute period. Zh Vopr
Neirokhir Im N N Burdenko. 4:15–18. 1981.(In Russian).
|
|
28
|
Ren H, Wang W and Ge Z: Glasgow coma
scale, brain electric activity mapping and Glasgow outcome seale
after hyperbaric oxygen treatment of severe brain injury. Chin J
Traumatol. 4:239–241. 2001.PubMed/NCBI
|
|
29
|
Fan JZ and Xue L: Hyperbaric oxygen
therapy for pediatric brain injury. Chin J Rehabilitation.
16:74–75. 2001.(In Chinese).
|
|
30
|
Wang GT: Efficacy analysis of Nimodiping
combined with compound Danshen injection for treatment of 35 cases
with severe brain injury and encephaledema. Chin Mod Med. 16:80–84.
2009.(In Chinese).
|
|
31
|
Chen ZB, Zhang MG and Lin QX: Effective
observation of nimodiping combined with hyperbaric oxygen in severe
injury of brain. Hainan Medical J. 18:2–3. 2007.(In Chinese).
|
|
32
|
Cai ZC, Li M and Li JZ: Protective effect
of Nimodipine on porcine basilar artery oxidative stress injury
induced by hydrogen peroxide. Chin J Clin Pharmacol Ther.
12:906–910. 2007.(In Chinese).
|
|
33
|
Xu L, Li B, Yang C, Li C and Peng Y:
Clinical research on postoperative efficacy and related factors of
early simulation hyperbaric oxygen therapy for severe
craniocerebral injury. Pak J Pharm Sci. 29 1 Suppl:S273–S280.
2016.
|