Introduction
Coronary heart disease is a leading cause of death
and long-term disability worldwide (1). Although important progress has been
made in preventing coronary heart disease, the mortality rate still
increased from 12.3 million in 1990 to 17.3 million in 2013
worldwide, with an increase of 41% (2). There is currently a lack of effective
treatment available for patients with coronary heart disease and
the 5-year mortality rate is as high as 50% (3). Myocardial infarction is defined as the
death of cardiomyocytes caused by long-term ischemia (4). The main causes of death from
myocardial infarction are progressive congestive heart failure,
secondary severe arrhythmia, and sudden death (5). Therefore, there is a need to study new
drugs for treating myocardial ischemia.
Tetrandrine, a bisbenzylisoquinoline alkaloid with a
molecular formula of
C33H42N2O6, is the main
biologically active ingredient extracted from the root of
Stephania tetrandra S. Moore (6). It has been experimentally and
clinically shown to have a variety of pharmacological effects,
including muscle relaxation (7),
allergy alleviation (8),
antiarrhythmic (9),
antihypertensive (10),
antibacterial (11) and antitumor
(12) properties and
anticoagulation effects (13). In
recent years, extensive and in-depth research into its
pharmacological effects has been conducted. In terms of
cardiovascular pharmacology, tetrandrine was found to be a natural
non-selective calcium channel blocker and an antagonist of
calmodulin (14). Previous studies
have shown that tetrandrine has a better protective effect on
myocardium compared with the sham operation group (15). It has been reported that tetrandrine
can reduce the occurrence of ventricular arrhythmia in rats with
myocardial ischemia-reperfusion, suggesting that it has a
protective effect on arrhythmia caused by ischemia (16). However, to the best of our
knowledge, so far, no study reported the role of tetrandrine in
myocardial infarction. The current study hypothesized that
tetrandrine may attenuate left ventricular dysfunction and
remodeling in rats with myocardial infarction.
Materials and methods
Experimental groups
A total of 30 male Sprague-Dawley rats (weight,
200-250 g) from Shanghai Animal Research Center (http://www.slarc.org.cn/slarcWebSite/homeIndex.action)
were randomly divided into six groups (n=5/group) as follows: i)
Healthy control group; ii) Sham operation group; iii) Myocardial
infarction model group; iv) myocardial infarction + low-dose
tetrandrine group (10 mg/kg); v) myocardial infarction +
medium-dose tetrandrine group (50 mg/kg); and vi) myocardial
infarction + high-dose tetrandrine group (80 mg/kg), according to a
previous study (17). All rats were
housed at 21±2˚C, 0.03% CO2, 30-70% relative humidity
and 12/12 h light/dark cycle with free access to food and water. No
rats died during the surgery. The present study was approved by the
Ethics Committee of The Third Clinical Institute Affiliated to
Wenzhou Medical University (Wenzhou, China).
Rat myocardial infarction model
Rats in the myocardial infarction model and sham
operation groups were anesthetized with 3% sodium pentobarbital
(Hangzhou Xiaoyong Biotechnology Co., Ltd.; 30 mg/kg) by
intraperitoneal injection. Subsequently, in order to fully expose
the surgical area, the chest and axillary hair was shaved with a
small animal shaver and disinfected with iodine and 75% ethanol.
Tracheal intubation was subsequently performed, and rats were
operated on after confirming that they were unresponsive to
pinching. After turning on the external light source and the
microscope switch, the ventilator was turned on and the parameters
(respiratory ratio, 2:1; tidal volume, 6-8 ml; frequency 70
times/min) were set. Subsequently, the rats were connected to a
ventilator and observed for breathing. When the thoracic
undulations and the ventilator frequency were consistent, the
intubation was considered successful, indicating that myocardial
infarction could be induced. Each rat was placed on the right side.
The ophthalmic scissors were fixed under the axilla of the left
forelimb and micro scissors were used to open the thorax between
the third and fourth intercostal space to fully expose the heart.
Rats in the sham operation group were sutured after thoracotomy. In
order to fully expose the left anterior descending (LAD) coronary
artery, micro straight forceps were used to gently pinch and tear
pericardium under the left atrial appendage. Under the microscope,
the direction or possible location of LAD was identified. A needle
holder, 5-0 suture and a needle were used to apply a non-invasive
suture next to the pulmonary artery cone below the root of the left
atrial appendage to completely block LAD coronary artery blood flow
for 3 min. After the ligation was completed, 5-0 sutures were used
to completely suture the thorax (seamless, no dislocation) and
suture each layer of muscles and skin. After the surgery, the rats
were observed for abnormal breathing. After the rats naturally
awakened, the ventilator and tube were removed. Finally, the rats
were reared normally as aforementioned. The tetrandrine groups were
administered 10, 50 or 80 mg/kg tetrandrine orally once a day at a
fixed time starting from the second day after surgery by
intragastric intubation. The rats in the sham operation and
myocardial infarction groups were administered the same volume of
normal saline in the same way. After 4 weeks, arterial blood was
collected from each group. All rats were euthanized by 3% sodium
pentobarbital (150 mg/kg) by intraperitoneal injection and the left
ventricle tissue was removed. The present study complied with the
Guide for the Care and Use of Laboratory Animals of the National
Institutes of Health (18).
Rat myocardial infarction model and
treatment effect evaluation
Rats in each group were evaluated for cardiac
function by ultrasonography every 3 days for 4 weeks (18). From the ultrasound images, the left
ventricular end-diastolic diameter (LVIDd) and left ventricular
end-systolic diameter (LVIDs) were measured. In addition, the
corresponding ejection fraction (EF%) and left ventricular
fractional shortening rate (FS%) were automatically calculated with
M-mode and 2D echocardiography (ACUSON Sequoia; Siemens
Healthineers).
Hematoxylin and eosin (H&E)
staining
Fresh myocardial tissue was fixed in 4%
paraformaldehyde for 24 h at 37˚C. Subsequently, the tissue was
dehydrated in ascending alcohol series. The fixed tissue was
embedded in paraffin and cooled at -20˚C. After the wax solidified,
the wax block was removed from the embedding box and trimmed. The
trimmed wax block was sliced to a thickness of 4 µm. Paraffin
sections were subsequently stained. Briefly, paraffin sections were
dewaxed (using xylene) into water. Sections were stained with
Harris hematoxylin for 5-10 min at 37˚C. After rinsing with tap
water, paraffin sections were differentiated with 1% hydrochloric
acid alcohol for 10 sec. After 10 min of rinsing in tap water,
paraffin sections were washed with PBS for 5 min at 37˚C. Then, the
sections were stained with eosin staining solution for 1-3 min at
37˚C. After the slides were dehydrated, they were sealed with
neutral gum and observed under an optical microscope (Olympus
Corporation; magnification, x50 or x400).
TUNEL staining
Myocardial tissue sections were prepared as
described in H&E staining. TUNEL staining was performed using
TUNEL apoptosis detection kit [cat. no. ATK00001; Pujian Biological
(Wuhan) Technology Co., Ltd. (AtaGenix); http://www.atagenix.com/]. All experimental groups
were incubated with 1X DNase I buffer for 10 min. A TUNEL test
solution was prepared according to the manufacturer's instructions.
Each section was incubated with an appropriate amount of TUNEL
detection solution for 60 min at 37˚C, and then 0.05 µg/µl of DAPI
solution was incubated at room temperature for 10 min in the dark.
Sections were immersed 3 times in PBS solution at room temperature
for 5 min each time, and mounted with anti-fluorescence quenching
mounting media [cat. no. ATK00001; Pujian Biological (Wuhan)
Technology Co., Ltd. (AtaGenix)]. The results were observed under a
fluorescence microscope (magnification, x400) in five random fields
of view. The excitation wavelength range was 450-500 nm, and the
emission wavelength range was 515-565 nm.
Biochemical testing
The triglyceride (TG), total cholesterol (TC), high
density lipoprotein (HDL) and low-density lipoprotein (LDL) levels
in the arterial blood were examined using TG assay kit (cat. no.
C061), TC determination kit (cat. no. C063), HDL assay kit (cat.
no. K076) and LDL assay kit (cat. no. K075) (all from Changchun
Huili Biotech Co., Ltd.; http://www.cchuili.com/).
Western blot analysis
The frozen myocardial tissue samples (-20˚C) were
lysed on ice with RIPA lysis buffer (cat. no. P0013B; Beyotime
Institute of Biotechnology) for 30 min at 4˚C and centrifuged at
3,280 x g at 4˚C for 10 min. The supernatant was then transferred
to a new microcentrifuge tube. The protein concentration was
measured by the BCA method (cat. no. P0009; Beyotime Institute of
Biotechnology). A total of 20 µg protein samples were used for
SDS-PAGE and subsequently transferred to a PVDF membrane and
blocked with 5% non-fat milk-PBS solution at room temperature for 1
h. The membrane was incubated with primary antibodies at 4˚C
overnight, followed by an incubation with horseradish
peroxidase-conjugated secondary antibodies (1:5,000; cat. no.
ab97040; Abcam) for 1 h at room temperature. Finally, protein bands
were visualized by an ECL kit (Thermo Fisher Scientific, Inc.). The
grayscale value was determined using ImageJ software (version
2.1.4.7; National Institutes of Health).
The primary antibodies (1:1,000) were as follows:
Anti-ryanodine receptor (RyR2; cat. no. ab2868; Abcam);
anti-phosphorylated (p)-RYR-2 (cat. no. ab59225; Abcam);
anti-calmodulin (CaM; cat. no. sc-137079; Santa Cruz Biotechnology,
Inc.); anti-CaM-dependent protein kinase IIδ (CaMKIIδ; cat. no.
ab181052; Abcam); anti-protein kinase A (PKA; cat. no. sc-390548;
Santa Cruz Biotechnology, Inc); anti-FK506 binding protein 12.6
(FKBP12.6; cat. no. bs-16093R; BIOSS); anti-cleaved-caspase3 (cat.
no. ab49822; Abcam) and anti-pro-caspase3 (cat. no. ab32499;
Abcam). β-actin (cat. no. bs-0061R; BIOSS) was used as an internal
control.
Statistical analysis
All statistical analyses were performed using
GraphPad Prism 7.0 (GraphPad Software, Inc.). Data are presented as
the mean ± SD. Each experiment was repeated at least three times.
Multiple comparisons were performed using one-way analysis of
variance followed by Tukey's post hoc test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Construction of a rat model of
myocardial infarction
The LVIDd, LVIDs, EF% and FS% of rats in each group
were measured using ultrasonography (Fig. 1A). The results showed that in the
myocardial infarction model rats, the levels of LVIDd (Fig. 1B) and LVIDs (Fig. 1C) were significantly higher than
those in the sham operation group. After treatment with different
doses of tetrandrine, the levels of LVIDd and LVIDs were
significantly decreased compared with those in the myocardial
infarction model group. As shown in Fig. 1D and E, compared with the sham operation group,
the levels of EF% and FS% were significantly lower in the
myocardial infarction model group. However, 80 mg/kg tetrandrine
treatment significantly increased the levels of EF% and FS%
compared with the myocardial infarction model group. These results
indicated that tetrandrine might alleviate myocardial
infarction.
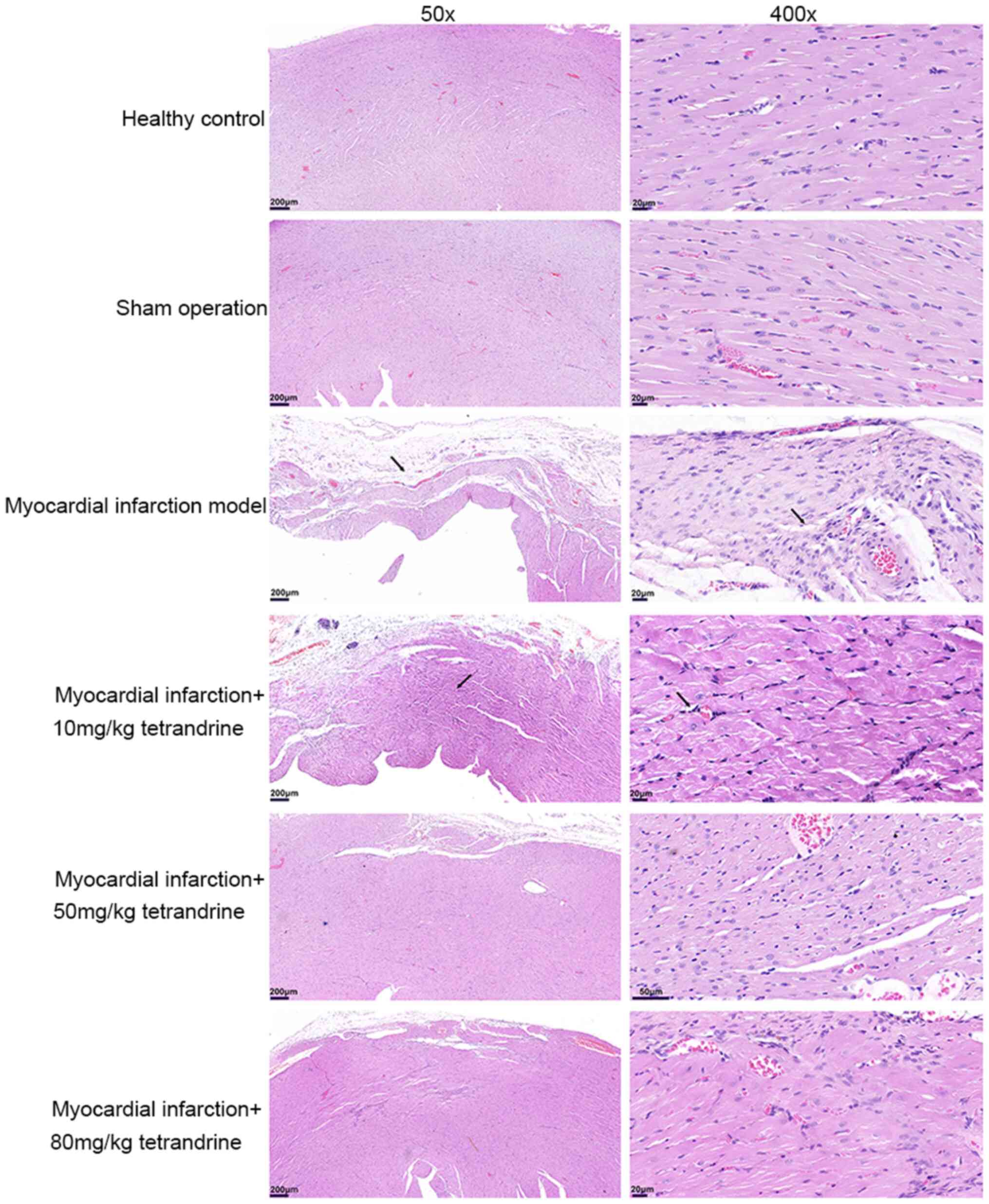
Tetrandrine alleviates the
pathological characteristics of rat models of myocardial
infarction
The H&E results showed that the myocardial cells
of rats in the healthy control group and sham operation group were
neatly arranged, dense, complete and clear, with uniform
intercellular spaces and low levels of extracellular matrix
(Fig. 2). Compared with the sham
operation group, increased volume of the surviving cardiomyocytes,
loose and disordered cell arrangement, contracted or dissolved
nuclei, widened intercellular space and broken or disappeared
myocardial rhabdoms were observed in the myocardial infarction
model group (Fig. 2). In the
tetrandrine-treated group, the degree of myocardial infarction in
rats was markedly reduced compared with the myocardial infarction
model group in a dose-dependent manner, and the residual myocardium
showed an island-like distribution (Fig. 2). These results revealed that
tetrandrine could alleviate the pathological characteristics of
myocardial infarction in rats.
Tetrandrine alleviates myocardial
apoptosis in rats with myocardial infarction
The TUNEL results showed that almost no apoptotic
cardiomyocytes in the healthy control group and sham operation
group were observed, while there were numerous apoptotic
cardiomyocytes in the myocardial infarction model group (Fig. 3). Tetrandrine (10, 50 and 80 mg/kg)
improved cardiomyocyte apoptosis in the myocardial infarction
model. These results showed that tetrandrine alleviated myocardial
apoptosis in rats with myocardial infarction.
Tetrandrine significantly inhibits the
levels of TG, TC and LDL and increases the levels of HDL in the
arterial blood of rats with myocardial infarction
The TC, TG, LDL and HDL levels were measured in the
arterial blood. The results showed that the levels of TC (Fig. 4A), TG (Fig. 4B) and LDL (Fig. 4C) in the arterial blood of rats with
myocardial infarction were significantly higher than that in rats
in the healthy control group and sham operation group. However, 50
and 80 mg/kg tetrandrine significantly inhibited the levels of TC,
TG and LDL in the arterial blood of rats with myocardial
infarction. Furthermore, the level of HDL in the arterial blood of
rats with myocardial infarction was significantly lower than that
in rats in the healthy control group and sham operation group. This
effect was alleviated by 50 and 80 mg/kg tetrandrine (Fig. 4D).
Tetrandrine restores calcium
homeostasis in rats with myocardial infarction
Western blotting was used to detect the levels of
cleaved-caspase-3, pro-caspase-3, RyR2, p-RyR2, CaMKIIδ, PKA, CaM
and FKBP12.6 in myocardial tissues of each group of rats (Fig. 5A). The results showed that there was
no significant difference in cleaved-caspase-3, pro-caspase-3 and
cleaved-caspase-3/pro-caspase-3 levels between healthy control and
sham operation groups (Fig. 5B-D).
Furthermore, the level of RyR2 and pro-caspase-3 was not different
between the groups included in the present study. The expression
level of cleaved-caspase-3 (Fig.
5B), the cleaved-caspase-3/pro-caspase-3 ratio (Fig. 5D) p-RyR2 (Fig. 5E), p-RyR2/RyR2 ratio (Fig. 5F), CaMKIIδ (Fig. 5G), PKA (Fig. 5H), and CaM (Fig. 5I) levels were significantly higher
in the myocardial tissue of rats with myocardial infarction
compared with the healthy control and sham operation groups.
However, 50 and 80 mg/kg tetrandrine significantly inhibited the
levels of cleaved-caspase-3, decreased the
cleaved-caspase-3/pro-caspase-3 ratio, and inhibited the levels of
p-RyR2, CaMKIIδ, PKA and CaM in the myocardial tissue of rats with
myocardial infarction. As shown in Fig.
5J, in the myocardial tissues of rats with myocardial
infarction, the expression level of FKBP12.6 was significantly
lower than that in the healthy control and sham operation groups,
and this effect was reversed by tetrandrine.
 | Figure 5Tetrandrine restores calcium
homeostasis in rats with myocardial infarction. (A) Representative
images of western blotting. Protein levels of (B)
cleaved-caspase-3, (C) pro-caspase3, (D)
cleaved-caspase3/pro-caspase3 ratio, (E) p-RyR2, (F) p-RyR2/RyR2
ratio, (G) CaMKIIδ, (H) PKA, (I) CaM and (J) FKBP12.6 in myocardial
tissue of each group of rats. *P<0.05;
**P<0.01; ***P<0.001; and
****P<0.0001. RyR, ryanodine receptor; CaM,
calmodulin; CaMKIIδ, CaM-dependent protein kinase IIδ; PKA, protein
kinase A; FKBP12.6, FK506 binding protein 12.6; p, phosphorylated;
ns, no significant difference. |
Discussion
A myocardial infarction model was successfully
established in the current study. The findings revealed that
tetrandrine could attenuate left ventricular dysfunction in rats
with myocardial infarction by restoring calcium homeostasis. The
present study provides a novel insight into the potential
mechanisms of tetrandrine treatment of myocardial infarction.
To adapt to excessive heart pressure load, cardiac
function is increased. The wall thickness and the stress of the
left ventricle wall are increased to improve the contractile
function of the heart, as a mechanism of early compensation
(19). However, continuous pressure
overload can promote myocardial hypertrophy, necrosis and apoptosis
of myocardial cells, impair the contraction and/or diastolic
function of the heart, and eventually develop into chronic heart
failure or cause sudden cardiac death (19). In the present study, a myocardial
infarction model was constructed by ligation of the left descending
coronary artery in rats. Ultrasonography or hemodynamics can be
used to detect and evaluate cardiac function (20). The current results showed that the
levels of LVIDd and LVIDs were significantly higher and the levels
of EF% and FS% were lower in the myocardial infarction model rats
compared with the sham operation group, and these effects were
alleviated by tetrandrine. Furthermore, the H&E staining
results showed that tetrandrine could alleviate the pathological
characteristics of myocardial infarction model rats. TUNEL results
showed that tetrandrine alleviated myocardial apoptosis in rats
with myocardial infarction.
The potential mechanisms of tetrandrine treatment of
myocardial infarction were further investigated. The protein levels
of p-RyR2, CaMKIIδ, PKA and CaM were significantly higher in the
myocardial tissue of rats with myocardial infarction compared with
the healthy control and sham operation groups, and these effects
were reversed by tetrandrine. Furthermore, in the myocardial tissue
of rats with myocardial infarction, the expression level of
FKBP12.6 was significantly lower than that in the healthy control
and sham operation groups, and this effect was reversed by
tetrandrine. These results indicated that tetrandrine alleviated
calcium homeostasis in rats with myocardial infarction. Previous
studies have confirmed that the stability of the RyR is disrupted
during heart failure due to sarcoplasmic reticulum diastolic
Ca2+ leakage, which constitutes the myocardial
cytological basis for diastolic dysfunction and fatal arrhythmia
(4,21). RyR can be divided into three
subtypes and RyR2 is the only RyR type expressed in cardiomyocytes
(22). Ca2+ leakage
refers to the abnormal release of Ca2+ caused by an
abnormal opening or incomplete closing of the RyR2 channel during
diastole (23). The RyR2 channel is
a large complex of signaling molecules composed of four isoform
subunits with a molecular weight of 565 kDa (24). There are also numerous accessory
proteins that regulate the function of RyR2, including CaM,
CaMKIIδ, PKA and FKBP12.6. CaM is the main calcium-binding protein
in cardiomyocytes (25). When
Ca2+ increases in cardiomyocytes, CaM and
Ca2+ combine to form a complex, which is activated and
acts on the substrate protein CaMKIIδ. PKA and CaMKIIδ catalyze the
phosphorylation of RyR2, and PP1 and PP2A catalyze the
dephosphorylation of RyR2(26). The
combination of FKBP12.6 and RYR2 stabilizes the RYR2 channel
complex. After RyR2 is phosphorylated, it separates from FKBP12.6
and opens. After dephosphorylation, it binds to FKBP12.6 and
closes. In humans and rodents, Ser2808 and Ser2830 have been
proposed to serve as the sites for PKA phosphorylation regulation
of RyR2, and Ser2814 is a site for CaMKIIδ phosphorylation
regulation of RyR2(27). Excessive
phosphorylation of RyR2 or knockdown of FKBP12.6 in myocardial
cells can separate RyR2 from FKBP12.6 and induce its opening,
resulting in unstable RyR2 channels and increased sensitivity to
Ca2+ (28). Therefore,
calcium homeostasis imbalance caused by Ca2+ leakage is
an important cause of pathophysiological changes in myocardial
failure (29). Considering the
aforementioned mechanism of RyR2 dysfunction in the pathogenesis of
heart failure, RyR2 is expected to become an important targeted
therapy for heart failure (30).
Promoting the interaction between FKBP12.6 and RyR2 and inhibiting
PKA or CaMKIIδ-mediated RyR2 hyperphosphorylation can enhance the
stability of the RyR2 channel. Therefore, FKBP12.6, PKA and CaMKIIδ
may become potential therapeutic targets for heart failure, which
requires further research (31).
According to previous reports, tetrandrine can inhibit
extracellular Ca2+ influx, interfere with intracellular
Ca2+ distribution, maintain intracellular
Ca2+ homeostasis, and block various pathophysiological
processes caused by abnormal calcium signaling (32). Tetrandrine can inhibit the increase
of intracellular Ca2+ induced by KCl in a dose-dependent
manner. In addition, its high concentration can also reduce the
instantaneous increase in intracellular Ca2+ induced by
caffeine (33). Tetrandrine can
reduce diastolic blood pressure, ameliorate left ventricular
hypertrophy and remodeling in hypertensive rats, reduce myocardial
cell calcium overload, and increase myocardial myosin ATPase,
Na+-K+-ATPase and Ca2+-ATP enzyme
activity (34). Recent studies have
reported that tetrandrine can reduce myocardial hypertrophy,
ventricular enlargement and pulmonary congestion in a model of
myocardial hypertrophy caused by aortic constriction (35,36).
It has been hypothesized that tetrandrine may act by inhibiting the
activation of the oxygen free radical-dependent ERK1/2 signal
transduction pathway (15).
Previous studies have reported that the use of tetrandrine in
rabbits after myocardial infarction induced by isoproterenol can
reduce myocardial damage through antioxidative effects (35), and that tetrandrine has
antioxidative and antifibrotic effects on the human heart, and
improves ventricular compliance (36).
The present study further elucidated the mechanisms
of ventricular myocyte calcium homeostasis and left ventricular
remodeling in ischemic cardiomyopathy. By measuring the effect of
tetrandrine on cardiac function in rats with ischemic
cardiomyopathy, the results confirmed that tetrandrine could play a
role in improving cardiac function in rats with ischemic
cardiomyopathy. The effect of tetrandrine on the expression of
regulatory proteins involved in ventricular calcium homeostasis in
ischemic cardiomyopathy was also studied. However, further research
is required to confirm this mechanism.
A myocardial ischemic injury model was established
in the present study. The findings revealed that tetrandrine can
protect the ischemic myocardium. In summary, previous research
suggested that tetrandrine can have protective effects on ischemic
heart, including reversing ventricular remodeling, reducing infarct
size, inducing antioxidative and antifibrotic effects, improving
cardiac function and reducing the occurrence of arrhythmia. The
specific mechanism may be associated with the maintenance of
intracellular Ca2+ homeostasis and antioxidative and
antifibrotic effects.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WJ conceived and designed the study. YW, WZ and FY
conducted most of the experiments, performed data analysis and
wrote the manuscript. SH, HC and RZ participated in the acquisition
of data and helped draft the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Third Clinical Institute Affiliated to Wenzhou
Medical University (Wenzhou, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Liao J, Wang J, Liu Y, Li J and Duan L:
Transcriptome sequencing of lncRNA, miRNA, mRNA and interaction
network constructing in coronary heart disease. BMC Med Genomics.
12(124)2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Agha G, Mendelson MM, Ward-Caviness CK,
Joehanes R, Huan TX, Gondalia R, Salfati E, Brody JA, Fiorito G,
Bressler J, et al: Blood leukocyte DNA methylation predicts risk of
future myocardial infarction and coronary heart disease.
Circulation. 140:645–657. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhou M, Bao Y, Li H, Pan Y, Shu L, Xia Z,
Wu D, Lam KSL, Vanhoutte PM, Xu A, et al: Deficiency of adipocyte
fatty-acid-binding protein alleviates myocardial
ischaemia/reperfusion injury and diabetes-induced cardiac
dysfunction. Clin Sci (Lond). 129:547–559. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Thygesen K, Alpert JS and White HD: Joint
ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial
Infarction. Universal definition of myocardial infarction. J Am
Coll Cardiol. 50:2173–2195. 2007.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Winkler A, Jaguś-Jamioła A,
Uziębło-Życzkowska B, Orski Z, Krzyżanowski K, Smalc-Stasiak M and
Kiliszek M: Predictors of appropriate interventions and mortality
in patients with implantable cardioverter-defibrillators. Pol Arch
Intern Med. 129:667–672. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Yuan X, Dou Y, Wu X, Wei Z and Dai Y:
Tetrandrine, an agonist of aryl hydrocarbon receptor, reciprocally
modulates the activities of STAT3 and STAT5 to suppress Th17 cell
differentiation. J Cell Mol Med. 21:2172–2183. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kwan CY, Ma FM and Hui SC: Inhibition of
endothelium-dependent vascular relaxation by tetrandrine. Life Sci.
64:2391–2400. 1999.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Liou JT, Lin CS, Liao YC, Ho LJ, Yang SP
and Lai JH: JNK/AP-1 activation contributes to tetrandrine
resistance in T-cell acute lymphoblastic leukaemia. Acta Pharmacol
Sin. 38:1171–1183. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sakurai Y, Kolokoltsov AA, Chen CC,
Tidwell MW, Bauta WE, Klugbauer N, Grimm C, Wahl-Schott C, Biel M
and Davey RA: Ebola virus. Two-pore channels control Ebola virus
host cell entry and are drug targets for disease treatment.
Science. 347:995–998. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhang J, Yu B, Zhang XQ, Sheng ZF, Li SJ,
Wang ZJ, Cui XY, Cui SY and Zhang YH: Tetrandrine, an
antihypertensive alkaloid, improves the sleep state of
spontaneously hypertensive rats (SHRs). J Ethnopharmacol.
151:729–732. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lee YS, Han SH, Lee SH, Kim YG, Park CB,
Kang OH, Keum JH, Kim SB, Mun SH, Seo YS, et al: The mechanism of
antibacterial activity of tetrandrine against Staphylococcus
aureus. Foodborne Pathog Dis. 9:686–691. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yu M, Liu T, Chen Y, Li Y and Li W:
Combination therapy with protein kinase inhibitor H89 and
Tetrandrine elicits enhanced synergistic antitumor efficacy. J Exp
Clin Cancer Res. 37(114)2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Westra IM, Oosterhuis D, Groothuis GM and
Olinga P: Precision-cut liver slices as a model for the early onset
of liver fibrosis to test antifibrotic drugs. Toxicol Appl
Pharmacol. 274:328–338. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ohta T, Yasuda W, Hasegawa A, Ito S and
Nakazato Y: Effects of inhibitors for tyrosine kinase and
non-selective cation channel on capacitative Ca(2+) entry in rat
ileal smooth muscle. Eur J Pharmacol. 387:211–220. 2000.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Shen DF, Tang QZ, Yan L, Zhang Y, Zhu LH,
Wang L, Liu C, Bian ZY and Li H: Tetrandrine blocks cardiac
hypertrophy by disrupting reactive oxygen species-dependent ERK1/2
signalling. Br J Pharmacol. 159:970–981. 2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ai J, Gao HH, He SZ, Wang L, Luo DL and
Yang BF: Effects of matrine, artemisinin, tetrandrine on cytosolic
[Ca2+]i in guinea pig ventricular myocytes. Acta
Pharmacol Sin. 22:512–515. 2001.PubMed/NCBI
|
|
17
|
Pilz PM, Hamza O, Gidlöf O, Gonçalves IF,
Tretter EV, Trojanek S, Abraham D, Heber S, Haller PM, Podesser BK
and Kiss A: Remote ischemic perconditioning attenuates adverse
cardiac remodeling and preserves left ventricular function in a rat
model of reperfused myocardial infarction. Int J Cardiol.
285:72–79. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Peng L and Zhao Y, Li Y, Zhou Y, Li L, Lei
S, Yu S and Zhao Y: Effect of DJ-1 on the neuroprotection of
astrocytes subjected to cerebral ischemia/reperfusion injury. J Mol
Med (Berl). 97:189–199. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Zhang TJ, Guo RX, Li X, Wang YW and Li YJ:
Tetrandrine cardioprotection in ischemia-reperfusion (I/R) injury
via JAK3/STAT3/Hexokinase II. Eur J Pharmacol. 813:153–160.
2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sun M, Chen M, Dawood F, Zurawska U, Li
JY, Parker T, Kassiri Z, Kirshenbaum LA, Arnold M, Khokha R and Liu
PP: Tumor necrosis factor-alpha mediates cardiac remodeling and
ventricular dysfunction after pressure overload state. Circulation.
115:1398–1407. 2007.PubMed/NCBI View Article : Google Scholar
|
|
21
|
O'Brien F, Venturi E and Sitsapesan R: The
ryanodine receptor provides high throughput Ca2+-release
but is precisely regulated by networks of associated proteins: A
focus on proteins relevant to phosphorylation. Biochem Soc Trans.
43:426–433. 2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Yano M, Kobayashi S, Kohno M, Doi M,
Tokuhisa T, Okuda S, Suetsugu M, Hisaoka T, Obayashi M, Ohkusa T,
et al: FKBP12.6-mediated stabilization of calcium-release channel
(ryanodine receptor) as a novel therapeutic strategy against heart
failure. Circulation. 107:477–484. 2003.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Landstrom AP, Dobrev D and Wehrens XHT:
Calcium signaling and cardiac arrhythmias. Circ Res. 120:1969–1993.
2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Peng W, Shen H, Wu J, Guo W, Pan X, Wang
R, Chen SR and Yan N: Structural basis for the gating mechanism of
the type 2 ryanodine receptor RyR2. Science.
354(aah5324)2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Rocchetti M, Sala L, Dreizehnter L, Crotti
L, Sinnecker D, Mura M, Pane LS, Altomare C, Torre E, Mostacciuolo
G, et al: Elucidating arrhythmogenic mechanisms of long-QT syndrome
CALM1-F142L mutation in patient-specific induced pluripotent stem
cell-derived cardiomyocytes. Cardiovascular Res. 113:531–541.
2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Fischer TH, Herting J, Tirilomis T, Renner
A, Neef S, Toischer K, Ellenberger D, Förster A, Schmitto JD,
Gummert J, et al: Ca2+/calmodulin-dependent protein
kinase II and protein kinase A differentially regulate sarcoplasmic
reticulum Ca2+ leak in human cardiac pathology.
Circulation. 128:970–981. 2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Huke S and Bers DM: Ryanodine receptor
phosphorylation at Serine. 2030, 2808 and 2814 in rat
cardiomyocytes. Biochem Biophys Res Commun. 376:80–85.
2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
MacMillan D: FK506 binding proteins:
Cellular regulators of intracellular Ca2+ signalling.
Eur J Pharmacol. 700:181–193. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Luo M and Anderson ME: Mechanisms of
altered Ca(2)(+) handling in heart failure. Circ Res. 113:690–708.
2013.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Yamamoto T, Yano M, Xu X, Uchinoumi H,
Tateishi H, Mochizuki M, Oda T, Kobayashi S, Ikemoto N and
Matsuzaki M: Identification of target domains of the cardiac
ryanodine receptor to correct channel disorder in failing hearts.
Circulation. 117:762–772. 2008.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sag CM, Wagner S and Maier LS: Role of
oxidants on calcium and sodium movement in healthy and diseased
cardiac myocytes. Free Radic Biol Med. 63:338–349. 2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Huang T, Xu S, Deo R, Ma A, Li H, Ma K and
Gan X: Targeting the Ca(2+)/Calmodulin-dependent protein kinase II
by Tetrandrine in human liver cancer cells. Biochem Biophys Res
Commun. 508:1227–1232. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Wang B and Xiao JG: Effect of tetrandrine
on free intracellular calcium in cultured calf basilar artery
smooth muscle cells. Acta Pharmacol Sin. 23:1121–1126.
2002.PubMed/NCBI
|
|
34
|
Rao MR: Effects of tetrandrine on cardiac
and vascular remodeling. Acta Pharmacol Sin. 23:1075–1085.
2002.PubMed/NCBI
|
|
35
|
Pinelli A, Trivulzio S, Brenna S, Galmozzi
G and Rossoni G: Pretreatment with tetrandrine has protective
effects against isoproterenol-induced myocardial infarction in
rabbits. In Vivo. 24:265–270. 2010.PubMed/NCBI
|
|
36
|
Teng G, Svystonyuk D, Mewhort HE, Turnbull
JD, Belke DD, Duff HJ and Fedak PWM: Tetrandrine reverses human
cardiac myofibroblast activation and myocardial fibrosis. Am J
Physiol Heart Circ Physiol. 308:H1564–H1574. 2015.PubMed/NCBI View Article : Google Scholar
|