Introduction
Triple-negative breast cancer (TNBC) is a term that
defines breast cancers with a lack of expression of estrogen
receptor (ER), progesterone receptor (PR) and human epidermal
growth factor receptor 2 (Her2). It accounts for 10-20% of all
breast tumors (1) and exhibits a
more aggressive behavior than other molecular subtypes of breast
cancer. Unlike other breast cancer subtypes (i.e.,
ER+/PR+; Her2+ breast cancers),
there is currently no targeted therapy available for TNBC, although
immunotherapy is available for advanced TNBC that expresses
programmed cell death ligand 1 (PD-L1); however, this performed in
combination with chemotherapy.
High-risk early-stage breast cancer is frequently
associated with a high recurrence rate (2). Neoadjuvant chemotherapy (NACT) is the
gold standard treatment in this setting (3-5).
In addition, the patients with pathological complete
response (pCR) following NACT have longer disease-free and overall
survival rates (6-9).
The pCR has a strong prognostic value and is a surrogate endpoint
for clinical trials testing neoadjuvant treatment in patients with
early-stage breast cancer, including TNBC (7,10).
Despite its aggressive behavior, TNBC is
particularly sensitive to cytotoxic chemotherapy (known as the
‘triple-negative paradox’) (11).
The pCR is achieved in ~30-40% of TNBC cases following standard
anthracycline plus cyclophosphamide- and taxane-based NACT
(12).
At the molecular level, TNBC is a heterogeneous
disease based on transcriptional and mutational heterogeneity. The
biology of TNBC is characterized by an increased immunological
infiltrate, a basal-like and mesenchymal phenotype, as well as a
deficiency in homologous recombination (13).
Genomic instability in the homologous recombination
repair gens (i.e., BRCA1 and BRCA2) provides specific therapeutic
opportunities for the use of DNA double-strand break-inducing
agents: Platinum salts, anthracyclines, cyclophosphamide and
poly-ADP-ribose polymerase (PARP) inhibitors (14-16).
Platinum agents, such as carboplatin and cisplatin are cytotoxic
DNA-damaging compounds which lead to cell apoptosis (17).
Several trials have investigated the benefits of the
addition of platinum agents to NACT regimens for TNBC with proven
activity, efficacy and safety. In patients with TNBC, the addition
of platinum agents is associated with significantly increased pCR
rates; however, event-free and overall survival data remain
inconclusive (18). To the best of
our knowledge, to date, there is currently no available no
meta-analysis comparing the pCR following NACT with the two
principal and most commonly used platinum representatives,
cisplatin and carboplatin.
The present study conducted a systematic review and
meta-analysis of clinical trials in order to elucidate the
differences and benefits of the addition of carboplatin or
cisplatin to NACT for patients with TNBC.
Data and methods
Search strategy
A PubMed and Cochcrane Register of Controlled Trials
search was conducted for published studies evaluating the pCR
following platinum-based NACT for patients with TNBC from 1990 to
November, 2020. The key medical terms used were: (breast cancer)
AND breast cancer [MeSH Terms] AND [‘1990/01/01’(PDat):
‘2020/06/30’(PDat)] AND Humans [Mesh] AND English [lang] AND
triple-negative AND [cisplatin (MeSH Terms)] OR carboplatin [MeSH
Terms] OR platinum [MeSH Terms] AND [neoadjuvant therapy (MeSH
Terms)] OR neoadjuvant treatment [MeSH Terms] AND breast cancer
[MeSH Terms]. Only studies in the English language were
selected.
Selection criteria
The eligibility criteria included prospective
(randomized and open-label studies) and retrospective studies
evaluating the pCR (both in the breast and axilla; ypT0N0) in
patients with TNBC treated with cisplatin or carboplatin-based
NACT. The reference lists of the included studies were examined in
order to identify additional relevant articles. A flow-chart of the
literature search is presented in Fig.
1.
From this analysis, studies with <20 patients,
phase 1 studies and platinum single-agent studies were excluded.
Data selection and extraction were performed by AN, AV and ST
independently and data entry was performed by RV. The results were
reviewed by the coordinating author (TC).
The primary endpoint of the present meta-analysis
was the pooled pCR for the comparison of cisplatin vs.
carboplatin-based NACT in TNBC.
Data extraction
The following information was extracted from each
study/article: The first author and the year of publication, study
design, the number of patients included, the neoadjuvant treatment
by type (carboplatin or cisplatin), the number of cycles and the
percentage of pCRs in the patients with TNBC.
Statistical analysis
The analysis was conducted using the Comprehensive
Meta-Analysis software, version 2 (https://www.meta-analysis.com). As an indicator of the
effect size, the event rate (the rate of pCR) was used. Publication
bias analysis was performed computing the Begg and Mazumdar rank
correlation test. This test computes the rank order correlation
(Kendall's tau-b) between the effect size and the standard error
(which is driven primarily by the sample size). This determines
whether large studies tend to be included in the analysis,
regardless of their effect size, whereas small studies are more
likely to be included when they exhibit a relatively large effect
size. For the moderation analysis, statistical comparisons were
performed between the categories of each moderator (the case of
categorical moderators) and meta-regressions for continuous
moderators. The confidence intervals for the effect sizes were
constructed in a parametric manner, for a probability of 95%, by
adding on each side of the effect size, the product between its
standard error and the critical Z-value 1.96.
Results
Identification of relevant
studies
Upon an initial search, 290 relevant articles were
identified for evaluation. Based on the inclusion and exclusion
criteria, 266 articles were excluded. Case reports, clinical
reports and clinical trials that did not provide pCR rates were
excluded. Additionally, studies in which data extraction was
impossible according to the triple-negative molecular subtype were
also excluded. Ultimately, 24 studies were selected for analysis,
comprising 1,711 patients with TNBC (19-42).
In total, 20 studies were prospective studies and five were
retrospective studies. There were 6 studies with cisplatin (5
prospective and 2 retrospective studies, including one arm from a
retrospective study with both arms) with a total of 325 patients
with TNBC. The remaining studies (18 studies) were with carboplatin
(15 prospective studies and 3 retrospective studies, including one
arm from a retrospective study with both cisplatin and carboplatin
arms) with a total of 1,386 patients with TNBC (one study included
cisplatin and carboplatin as well). The characteristics of the
included trials are presented in Table
I.
 | Table ICharacteristics of the studies
included in the current meta-analysis. |
Table I
Characteristics of the studies
included in the current meta-analysis.
| Authors/(Refs.),
year | Type of study | NLTN/not TNBCs | Protocol | pCR TNBCs with
platinum (%) | pCR TNBCs without
platinum (%) | pCR not TNBCs with
(%) | ORRs TNBCs with vs.
without platinum (%) | BCS (%) | DFS/OS (%) | DFS/OS pCR vs. no
pCR pts (%) | Median FU
(months) |
|---|
| Frasci et al
(40), 2009 | Prospective
series | 74/0 | wCDDP + wEPI +
wPAC | 62 | - | - | 98.3 | - | 76/89 | 90/95.6 | 41 |
| Torrisi et
al (33), 2008 | Prospective
series | 30/0 | EPI d1-2 + CDDP d1
+ 5-FU ci d 1 (q21d) x 4 -> PAC d 1,8,15 (q28d) x 3 | 40 | - | - | 86 | 86 | - | - | 17 |
| Chen et al
(38), 2010 | Phase 2 | 24/71 | wPAC + wCBDCA d1,
8,15 (q28d) | 33 | - | - | - | - | - | - | - |
| Gogas et al
(42), 2010 | Phase 2 | 46 | PAC -> CBDCA
AUC6 | 9.5 | - | - | 60 | - | -/66 | - | 45 |
| Chang et al
(37), 2010 | Prospective
series | 11/63 | CBDCA AUC6 d1
(q21d) + 3wDOC d1 (q21d) x 4 | 54.6 | - | 20.9 | - | - | - | - | 22.8 |
| Silver et al
(32), 2010 | | 28 | CDDP 75
mg/m2 (q21d) | 21 | - | - | - | - | - | - | - |
| Alba et al
(20), 2012 | Phase 2
randomized | 93 | EC d1 q 21 x 4 +
3wDOC ± CBDCA AUC5 d1 (q21d) x 4 | 30 | 35 | - | 77 vs. 70 | 72 vs. 67 | - | - | - |
| Hurley et al
(22), 2013 | Retrospective
series | 144 | CBDCA AUC5 or
wCBDCA or 3wCDDP + 3wDOC or wDOC x 4 ± AC x 4 | 31 | - | - | - | 7.6 | 55/61 | 81 vs.44/78
vs.51 | 48 |
| Roy et al
(26), 2013 | Phase 2 | 9/48 | DOC d1 (q14d) +
CBDCA AUC6 d2 (q14d) x 4 | 44 | - | 11.9 | - | 34 | - | - | 38 |
| Sikov et al
(31), 2015 | Phase 2
randomized | 443 | wPAC x 12 -> AC
d1 (q14d) X 4 ± wCBDCA ± bevacizumab (10 mg/kg) d1 (q14d) x 9 | 54 vs.
41b | | - | - | 57 vs. 40 | - | - | - |
| Ando et al
(30), 2014 | Phase 2
Randomized | 181 | wCBDCA AUC5 + wPAC
-> (CEF) CTX + EPI + 5-FU | 61.2 | 26.3 | - | 84.1 vs 70.3 | NR | - | - | - |
| Kern et al
(25), 2016 | Prospective
series | 30 | CBDCA AUC6 + DOC
d1 | 50 (q21d) | - | - | - | 100 | - | - | - |
| Zhu et al
(35), 2016 | Phase 2 | 14/96 | CBDCA AUC 5 + PAC ±
trastuzumab (6 mg/mg), bi-weekly | 57.14 | - | - | - | - | - | - | - |
| AL-Tweigeri et
al (19), 2016 | Phase 2 | 51/29 | (FEC100) EPI + CTX
+ 5-FU d1 (q21d) -> CDDP + DOC ± trastuzumab d1 (q21d) | 36 | - | - | - | NR | 67/86 | 96/95 vs 57/82 | 43 |
| Cancello et
al (36), 2015 | Phase 2 | 34 | EPI + CDDP + 5-FU
d1 (q21d) -> PAC d1,8,15 (q28d) + CTX 50 mg/day for 12
weeks | 56 | - | - | - | - | - | - | 27 |
| Shinde et al
(29), 2015 | Retrospective
series | 10/29 | CBDCA AUC6 +
wPAC | 60 | - | 31 | - | - | - | - | - |
| Zhang et al
(34), 2016 | Phase 2
randomized | 91 | EPI + PAC d1/2
(q21d) vs. PAC + CBDCA AUC5 d2/1 (q21d) | 38.6 vs. 14 | - | - | 89.4 vs. 79.5 | - | 71.1 vs. 52.8/7 0.1
vs. 72.5 | - | 55 |
| De Iuliis et
al (23), 2017 | | 24/37 | CBDCA AUC2 + PAC ±
trastuzumab | 83 | - | - | 61,39 | 57 | - | - | 48 |
| Sharma et al
(28), 2017 | Phase 2 | 190 | CBDCA AUC6 + DOC +
MGFS (q21d) | 55 | - | - | - | - | - | - | - |
| Gluz et al
(41), 2018 | Randomized
trial | 336 | Arm A: PAC + GEM
d1,8 (q3w) Arm B: PAC+ CBDCA AUC2 d1,8 (q3w) | 45.9 | 28.7 | - | - | - | - | - | - |
| Hahnen et al
(21), 2017 | Randomized Clinical
Trial | 291 | Arm A: PAC+ NPLD +
bevacizumab + CBDCA AUC2 Arm B: PAC + NPLD + bevacizumab | 56.8 | 41.4 | - | - | - | 85.3/- | - | 35 |
| Jovanovic et
al (24), 2017 | Phase 2 | 145 | CDDP + PAC ±
everolimus | 40 | - | - | - | - | - | - | 42 |
| Fontaine et
al (39), 2019 | Prospective phase
2 | 63 | wPAC + CBDCA AUC2
-> EPI + CTX + MGFS | 54 | - | - | - | - | - | - | 22 |
| Schmid et al
(27), 2020 | Randomized
double-blind trial | 1174 | PAC + CBDCA +
pembrolizumab; PAC + CBDCA + pembro placebo -> DOC/EPI +
CTX | 68.9/54.9 | - | - | - | - | - | - | 15,5 |
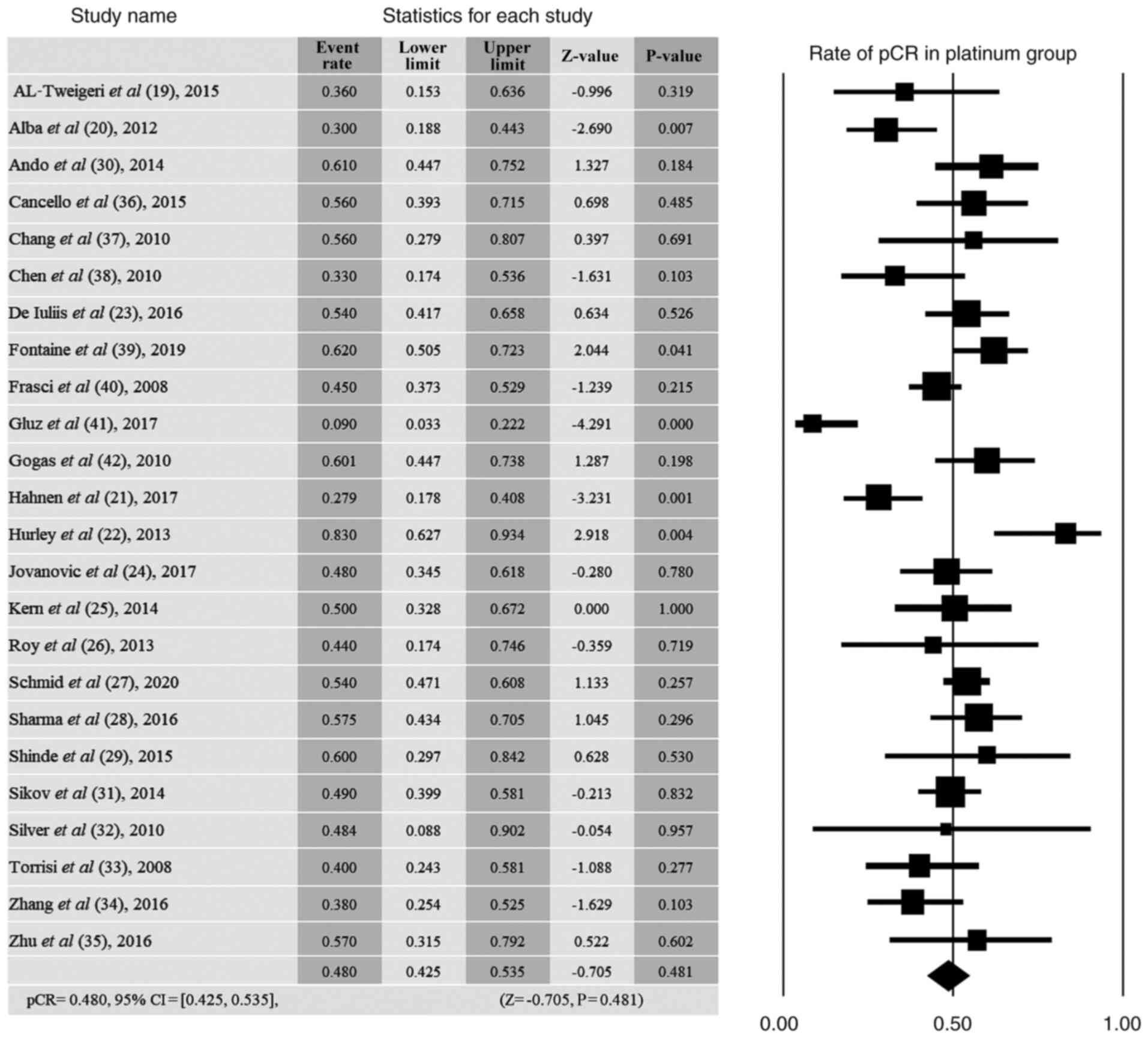
Heterogeneity of the included
studies
The distribution of effects proved to be
significantly heterogeneous, Q(24)=65.13, P<0.001, which indicates
that it would be reasonable to test several possible moderators of
pCR rate variability. The heterogeneity test investigates whether
the effect sizes from each study are sufficiently enough to
consider that they come from different populations. In other words,
the data upon which the analysis was performed is the distribution
of the effect sizes from each study, which is represented in the
forest plot (Fig. 2).
Publication bias
The risk of publication bias was calculated using
the Begg and Mazumdar rank correlation test. This test computes the
rank order correlation (Kendall's tau-b) between the rate of pCR
obtained in each study and the standard error (which is primarily
driven by the sample size) to identify whether large studies tend
to be included in the analysis regardless of their pCR rate,
whereas small studies would be more likely to be included when they
exhibit a relatively large pCR rate. The rank order correlation
(Kendall's tau-b) analysis between the pCR rate and the standard
error did not reveal any significant differences, which indicated
no publication bias (tau-b=-0.090, P=0.528).
The present study performed a meta-analysis of
published trials, which included both prospective and retrospective
studies, representing a mixed population of patients with
early-stage TNBC with different prognoses and responses to NACT.
The NACT protocols were very heterogeneous, and platinum agents
were associated with very different regimens (conventional and
non-conventional combinations).
Overall, the pooled weighted pCR rate in patients
with TNBC treated with platinum-based NACT was 48.0%. The results
revealed a non-significant overall rate of pCR=0.480, (95% CI,
0.425-0.535), compared with the rate of pCR obtained in random
conditions (Z=-0.705, P=0.481; Fig.
2).
According to the type of platinum agent used, the
analysis of the pCR rate revealed no significant differences
between the rate of pCR obtained with carboplatin vs. cisplatin
treatment (Table II). In addition,
no significant differences were observed between the rates of pCR
obtained under carboplatin vs. cisplatin treatment. The effect
sizes for both categories of the moderator did not differ
significantly (carboplatin: pCR rate, 0.470; 95% CI, 0.401-0.539;
cisplatin: pCR rate, 0.473; 95% CI, 0.379-0.568) (Table II). The comparison between these
two categories revealed no significant differences [Q(1)=0.003; P=0.959]. Thus, as shown in
Table II, no significant
differences were observed between the rates of pCR obtained under
carboplatin vs. cisplatin treatment.
| Table IIAnalysis of the pCR rate as a
function of treatment (carboplatin vs cisplatin). |
Table II
Analysis of the pCR rate as a
function of treatment (carboplatin vs cisplatin).
| | Heterogeneity
between categories |
|---|
| Treatment | No. of studies | pCR rate | Inf (95% CI%) | Sup (95% CI%) | Z value | P-value | Q-value | df | P-value |
|---|
| Carboplatin | 18 | 0.470 | 0.401 | 0.539 | -0.859 | 0.390 | 0.003 | 1 | 0.959 |
| Cisplatin | 7 | 0.473 | 0.379 | 0.568 | -0.559 | 0.576 | | | |
According to the BRCA status, there was a slightly
higher pCR rate for BRCA-positive patients, although no
statistically significant differences were observed in comparison
to the rate obtained for BRCA-negative patients. This analysis is
perhaps as rather inconclusive due to the low number of studies
that reported separate results for BRCA-positive and -negative in
patients with TNBC (Table III).
The pCR rate for BRCA-positive patients observed was 62.6% and that
for BRCA-negative patients was 45.2%.
| Table IIIAnalysis of the pCR rate as a
function of BRCA (only 4 studies reported results separately,
positive vs. negative). |
Table III
Analysis of the pCR rate as a
function of BRCA (only 4 studies reported results separately,
positive vs. negative).
| | Heterogeneity
between categories |
|---|
| Treatment | No. of studies | pCR rate | Inf (95% CI%) | Sup (95% CI%) | Z value | P-value | Q-value | df | P-value |
|---|
| Negative | 3 | 0.452 | 0.294 | 0.621 | -0.547 | 0.584 | 2.534 | 1 | 0.111 |
| Positive | 3 | 0.626 | 0.495 | 0.740 | 1.892 | 0.059 | | | |
Discussion
The present meta-analysis aimed to complement
previous systematic review and meta-analysis studies (18,43,44)
that analyzed the effects of platinum agents in TNBC as a class,
without differentiation between the agents used (carboplatin and
cisplatin) in this setting.
The data of the present study demonstrated a pCR
rate of 48.0% (pCR, 0.480; 95% CI, 0.425-0.535) in patients with
TNBC treated with platinum-based NACT. The current analyses
confirmed that the addition of platinum agents confers a higher
response rate in TNBC, 48.0 vs. 30-40% without addition of platinum
agents, as previously observed by Petrelli et al (43). In the present study, the pooled pCR
rate is similar that obtained in the study by Poggio et al
(18) and Petrelli et al
(43), with pCR rates of 51 and
45%, respectively.
In the meta-analysis by Petrelli et al, the
pooled pCR rate for 1,598 patients with TNBC treated with
platinum-based NACT was 45% (43).
Poggio et al (18) also
observed a significantly increased pCR rate (51%) in patients with
TNBC treated with platinum-based NACT. In the present study,
according to the type of platinum agent used, the analysis of the
pCR rate did not reveal any significant differences between that
obtained with carboplatin vs. cisplatin treatment (47.0 vs.
47.3%).
Poggio et al (18) reported a significant incidence of
grade 3 and 4 hematological adverse events (AEs), and no increased
risk of grade 3 and 4 neuropathy with platinum-based NACT. Given
the lack of available data, the selection of the most effective
platinum agent to be added to the neoadjuvant setting remains
unclear, and the decision is guided by the patient characteristics
and the decision made by the respective physician. Both carboplatin
and cisplatin demonstrate toxicity consistent with their known
safety profiles, with AEs occurring as anticipated for these
well-known chemotherapy drugs (45).
BRCA mutations can be found in around 15-25% of
patients with TNBC (46). It has
been demonstrated that BRCA DNA repair defects determine a
sensitivity to DNA-damaging agents, such as platinum salts and PARP
inhibitors (16). The present study
found that patients with TNBC who harbored a BRCA mutation had
higher pCR rates compared to patients who were negative for BRCA
mutations; however, the differences were not statistically
significant.
These results are in accordance with the results of
the meta-analysis by Caramelo et al (46), where a pCR rate of 58.4% was
achieved in BRCA-positive patients with TNBC who received
platinum-based NACT vs. one of 50.7% for BRCA-negative patients;
their results did not reach statistical significance either.
However, not all studies have found the same positive response to
neoadjuvant platinum-based chemotherapy in BRCA-positive patients
with TNBC. The GeparSixto trial demonstrated that the addition of
platinum agents did not improve the pCR rate in BRCA-positive
patients vs. those without BRCA mutations (36.4 vs. 55%) (21). Another meta-analysis confirmed the
results from GeparSixto trial and suggested that the addition of
platinum agents did not statistically improve the pCR rate (43.4
vs. 33.9%; OR, 1.340; 95% CI, 0.677-2.653; P=0.400) (47). The benefits of the addition of
platinum agents to the neoadjuvant setting in BRCA-positive
patients with TNBC still needs to be evaluated, considering the
limited number of patients with BRCA mutations.
In a retrospective analysis of 144 patients with
locally advanced TNBC, Hurley et al (22) evaluated the use of carboplatin and
cisplatin. In the cisplatin-based NACT group (97 patients) a pCR
rate of 35 (36.1%; HR, 0.32; P=0.009) was observed, vs. one of 10
(21.3%; HR, 0.40; P=0.002) in the carboplatin-based NACT group (47
patients), suggesting that cisplatin was superior to carboplatin,
although with a different toxicity profile.
In conclusion, the present meta-analysis of
published studies included both prospective and retrospective
studies, representing a mixed population of early-stage TNBC with
different prognoses and responses to NACT. The NACT protocols were
very heterogeneous and the platinum agents were associated with
markedly different regimens. To the best of our knowledge, the
present study performed the first meta-analysis that investigated
the efficacy of carboplatin and cisplatin as different chemotherapy
agents in the neoadjuvant treatment of patients with TNBC. The
results revealed that NACT improved the pCR rate in TNBC,
regardless of the platinum agent used. Carboplatin represents a
viable option in terms of accessibility, affordability and a more
favorable toxicity profile.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AN, AV and ST performed the data selection and data
extraction independently. RV performed data entry. SP and AD
performed the statistical analysis. RV and TC, the coordinating
author, were involved in the conception and the design of the study
and reviewed the final results. RV, AN and TC confirm the
authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gluz O, Liedtke C, Gottschalk N, Pusztai
L, Nitz U and Harbeck N: Triple-negative breast cancer-current
status and future directions. Ann Oncol. 20:1913–1927.
2009.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hudis CA and Gianni L: Triple-negative
breast cancer: An unmet medical need. Oncologist. 16 (Suppl
1):S1–S11. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Burstein HJ, Curigliano G, Loibl S, Dubsky
P, Gnant M, Poortmans P, Colleoni M, Denkert C, Piccart-Gebhart M,
Regan M, et al: Estimating the benefits of therapy for early-stage
breast cancer: The St. Gallen international consensus guidelines
for the primary therapy of early breast cancer 2019. Ann Oncol.
30:1541–1557. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cardoso F, Kyriakides S, Ohno S,
Penault-Llorca F, Poortmans P, Rubio IT, Zackrisson S and Senkus E:
ESMO Guidelines Committee. Early breast cancer: ESMO clinical
practice guidelines for diagnosis, treatment and follow-up. Ann
Oncol. 30:1194–1220. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Pusztai L, Foldi J, Dhawan A, DiGiovanna
MP and Mamounas EP: Changing frameworks in treatment sequencing of
triple-negative and HER2-positive, early-stage breast cancers.
Lancet Oncol. 20:e390–e396. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Huang M, O'Shaughnessy J, Zhao J,
Haiderali A, Cortés J, Ramsey SD, Briggs A, Hu P, Karantza V, Aktan
G, et al: Association of pathologic complete response with
long-term survival outcomes in triple-negative breast cancer: A
meta-analysis. Cancer Res. 80:5427–5434. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Cortazar P, Zhang L, Untch M, Mehta K,
Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L,
Valagussa P, et al: Pathological complete response and long-term
clinical benefit in breast cancer: The CTNeoBC pooled analysis.
Lancet. 384:164–172. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sikov WM, Polley MY, Twohy E, Perou CM,
Singh B, Berry DA, Tolaney SM, Somlo G, Port ER, Ma CX, et al:
CALGB (alliance) 40603: Long-term outcomes (LTOs) after neoadjuvant
chemotherapy (NACT) +/- carboplatin (Cb) and bevacizumab (Bev) in
triple-negative breast cancer (TNBC). J Clin Oncol. 37 (Suppl
15)(S591)2019.
|
|
9
|
Spring LM, Fell G, Arfe A, Trippa L,
Greenup R, Reynolds K, Smith BL, Moy B, Isakoff S, Parmigiani G and
Bardia A: Abstract GS2-03: Pathological complete response after
neoadjuvant chemotherapy and impact on breast cancer recurrence and
mortality, stratified by breast cancer subtypes and adjuvant
chemotherapy usage: Individual patient-level meta-analyses of over
27,000 patients. Cancer Res. 79 (Suppl 4):GS2–03. 2019.
|
|
10
|
European Medicines Agency: The role of the
pathological complete response as an endpoint in neoadjuvant breast
cancer studies, 2014 https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-role-pathological-complete-response-endpoint-neoadjuvant-breast-cancer-studies_en.pdf.
Accessed March 20, 2014.
|
|
11
|
Carey LA, Dees EC, Sawyer L, Gatti L,
Moore DT, Collichio F, Ollila DW, Sartor CI, Graham ML and Perou
CM: The triple negative paradox: Primary tumor chemosensitivity of
breast cancer subtypes. Clin Cancer Res. 13:2329–2334.
2007.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Liedtke C, Mazouni C, Hess KR, André F,
Tordai A, Mejia JA, Symmans WF, Gonzalez-Angulo AM, Hennessy B,
Green M, et al: Response to neoadjuvant therapy and long-term
survival in patients with triple-negative breast cancer. J Clin
Oncol. 26:1275–1281. 2008.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Denkert C, Liedtke C, Tutt A and von
Minckwitz G: Molecular alterations in triple-negative breast
cancer-the road to new treatment strategies. Lancet. 389:2430–2442.
2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Stockmans G, Deraedt K, Wildiers H,
Moerman P and Paridaens R: Triple-negative breast cancer. Curr Opin
Oncol. 20:614–620. 2008.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Collignon J, Lousberg L, Schroeder H and
Jerusalem G: Triple-negative breast cancer: Treatment challenges
and solutions. Breast Cancer (Dove Med Press). 8:93–107.
2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yang F, Kemp CJ and Henikoff S:
Anthracyclines induce double-strand DNA breaks at active gene
promoters. Mutat Res. 773:9–15. 2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kelland L: The resurgence of
platinum-based cancer chemotherapy. Nat Rev Cancer. 7:573–584.
2007.PubMed/NCBI View
Article : Google Scholar
|
|
18
|
Poggio F, Bruzzone M, Ceppi M, Pondé NF,
La Valle G, Del Mastro L, de Azambuja E and Lambertini M:
Platinum-based neoadjuvant chemotherapy in triple-negative breast
cancer: A systematic review and meta-analysis. Ann Oncol.
29:1497–1508. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
AL-Tweigeri T, AlSayed A, Alawadi S,
Ibrahim M, Ashour W, Jaafar H, Abulkhair O, AL-Abdulkarim H, Khalid
H and Ajarim D: Gulf Oncology Research Group (GORG-001). A
multicenter prospective phase II trial of neoadjuvant epirubicin,
cyclophosphamide, and 5-fluorouracil (FEC100) followed by
cisplatin-docetaxel with or without trastuzumab in locally advanced
breast cancer. Cancer Chemother Pharmacol. 77:147–153.
2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Alba E, Chacon JI, Lluch A, Anton A,
Estevez L, Cirauqui B, Carrasco E, Calvo L, Segui MA, Ribelles N,
et al: A randomized phase II trial of platinum salts in basal-like
breast cancer patients in the neoadjuvant setting. Results from the
GEICAM/2006-03, multicenter study. Breast Cancer Res Treat.
136:487–493. 2012.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Hahnen E, Lederer B, Hauke J, Loibl S,
Kröber S, Schneeweiss A, Denkert C, Fasching PA, Blohmer JU,
Jackisch C, et al: Germline mutation status, pathological complete
response, and disease-free survival in triple-negative breast
cancer: Secondary analysis of the GeparSixto randomized clinical
trial. JAMA Oncol. 3:1378–1385. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Hurley J, Reis IM, Rodgers SE,
Gomez-Fernandez C, Wright J, Leone JP, Larrieu R and Pegram MD: The
use of neoadjuvant platinum-based chemotherapy in locally advanced
breast cancer that is triple negative: Retrospective analysis of
144 patients. Breast Cancer Res Treat. 138:783–794. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
De Iuliis F, Salerno G, Corvino R,
D'Aniello D, Cefalì K, Taglieri L, Lanza R and Scarpa S:
Anthracycline-free neoadjuvant chemotherapy ensures higher rates of
pathologic complete response in breast cancer. Clin Breast Cancer.
17:34–40. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Jovanovic B, Mayer IA, Mayer EL, Abramson
VG, Bardia A, Sanders ME, Kuba MG, Estrada MV, Beeler JS, Shaver
TM, et al: A randomized phase II neoadjuvant study of cisplatin,
paclitaxel with or without everolimus in patients with stage II/III
triple-negative breast cancer (TNBC): Responses and long-term
outcome correlated with increased frequency of DNA damage response
gene mutations, TNBC subtype, AR status, and Ki67. Clin Cancer Res.
23:4035–4045. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kern P, Kalisch A, von Minckwitz G, Pütter
C, Kolberg HC, Pott D, Kurbacher C, Rezai M and Kimmig R:
Neoadjuvant, anthracycline-free chemotherapy with carboplatin and
docetaxel in triple-negative, early-stage breast cancer: A
multicentric analysis of rates of pathologic complete response and
survival. J Chemother. 28:210–217. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Roy V, Pockaj BA, Allred JB, Apsey H,
Northfelt DW, Nikcevich D, Mattar B and Perez EA: A phase II trial
of docetaxel and carboplatin administered every 2 weeks as
preoperative therapy for stage II or III breast cancer: NCCTG study
N0338. Am J Clin Oncol. 36:540–544. 2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Schmid P, Cortes J, Pusztai L, McArthur H,
Kümmel S, Bergh J, Denkert C, Park YH, Hui R, Harbeck N, et al:
Pembrolizumab for early triple-negative breast cancer. N Engl J
Med. 382:810–821. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Sharma P, López-Tarruella S, García-Saenz
JA, Ward C, Connor CS, Gómez HL, Prat A, Moreno F, Jerez-Gilarranz
Y, Barnadas A, et al: Efficacy of neoadjuvant carboplatin plus
docetaxel in triple-negative breast cancer: Combined analysis of
two cohorts. Clin Cancer Res. 23:649–657. 2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Shinde AM, Zhai J, Yu KW, Frankel P, Yim
JH, Luu T, Kruper L, Vito C, Shaw S, Vora NL, et al: Pathologic
complete response rates in triple-negative, HER2-positive, and
hormone receptor-positive breast cancers after anthracycline-free
neoadjuvant chemotherapy with carboplatin and paclitaxel with or
without trastuzumab. Breast. 24:18–23. 2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ando M, Yamauchi H, Aogi K, Shimizu S,
Iwata H, Masuda N, Yamamoto N, Inoue K, Ohono S, Kuroi K, et al:
Randomized phase II study of weekly paclitaxel with and without
carboplatin followed by cyclophosphamide/epirubicin/5-fluorouracil
as neoadjuvant chemotherapy for stage II/IIIA breast cancer without
HER2 overexpression. Breast Cancer Res Treat. 145:401–409.
2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sikov WM, Berry DA, Perou CM, Singh B,
Cirrincione CT, Tolaney SM, Kuzma CS, Pluard TJ, Somlo G, Port ER,
et al: Impact of the addition of carboplatin and/or bevacizumab to
neoadjuvant once-per-week paclitaxel followed by dose-dense
doxorubicin and cyclophosphamide on pathologic complete response
rates in stage II to III triple-negative breast cancer: CALGB 40603
(alliance). J Clin Oncol. 33:13–21. 2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Silver DP, Richardson AL, Eklund AC, Wang
ZC, Szallasi Z, Li Q, Juul N, Leong CO, Calogrias D, Buraimoh A, et
al: Efficacy of neoadjuvant cisplatin in triple-negative breast
cancer. J Clin Oncol. 28:1145–1153. 2010.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Torrisi R, Balduzzi A, Ghisini R, Rocca A,
Bottiglieri L, Giovanardi F, Veronesi P, Luini A, Orlando L, Viale
G, et al: Tailored preoperative treatment of locally advanced
triple negative (hormone receptor negative and HER2 negative)
breast cancer with epirubicin, cisplatin, and infusional
fluorouracil followed by weekly paclitaxel. Cancer Chemother
Pharmacol. 62:667–672. 2008.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Zhang P, Yin Y, Mo H, Zhang B, Wang X, Li
Q, Yuan P, Wang J, Zheng S, Cai R, et al: Better pathologic
complete response and relapse-free survival after carboplatin plus
paclitaxel compared with epirubicin plus paclitaxel as neoadjuvant
chemotherapy for locally advanced triple-negative breast cancer: A
randomized phase 2 trial. Oncotarget. 7:60647–60656.
2016.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Zhu T, Liu CL, Zhang YF, Liu YH, Xu FP, Zu
J, Zhang GC, Li XR, Liao N and Wang K: A phase II trial of
dose-dense (biweekly) paclitaxel plus carboplatin as neoadjuvant
chemotherapy for operable breast cancer. Breast Cancer Res Treat.
156:117–124. 2016.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Cancello G, Bagnardi V, Sangalli C,
Montagna E, Dellapasqua S, Sporchia A, Iorfida M, Viale G, Barberis
M, Veronesi P, et al: Phase II study with epirubicin, cisplatin,
and infusional fluorouracil followed by weekly paclitaxel with
metronomic cyclophosphamide as a preoperative treatment of
triple-negative breast cancer. Clin Breast Cancer. 15:259–265.
2015.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Chang HR, Glaspy J, Allison MA, Kass FC,
Elashoff R, Chung DU and Gornbein J: Differential response of
triple-negative breast cancer to a docetaxel and carboplatin-based
neoadjuvant treatment. Cancer. 116:4227–4237. 2010.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Chen XS, Nie XQ, Chen CM, Wu JY, Wu J, Lu
JS, Shao ZM, Shen ZZ and Shen KW: Weekly paclitaxel plus
carboplatin is an effective nonanthracycline-containing regimen as
neoadjuvant chemotherapy for breast cancer. Ann Oncol. 21:961–967.
2010.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Fontaine C, Renard V, Van den Bulk H,
Vuylsteke P, Glorieux P, Dopchie C, Decoster L, Vanacker L, de
Azambuja E, De Greve J, et al: Weekly carboplatin plus neoadjuvant
anthracycline-taxane-based regimen in early triple-negative breast
cancer: A prospective phase II trial by the breast cancer task
force of the Belgian society of medical oncology (BSMO). Breast
Cancer Res Treat. 176:607–615. 2019.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Frasci G, Comella P, Rinaldo M, Iodice G,
Di Bonito M, D'Aiuto M, Petrillo A, Lastoria S, Siani C, Comella G
and D'Aiuto G: Preoperative weekly cisplatin-epirubicin-paclitaxel
with G-CSF support in triple-negative large operable breast cancer.
Ann Oncol. 20:1185–1192. 2009.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Gluz O, Nitz U, Liedtke C, Christgen M,
Grischke EM, Forstbauer H, Braun M, Warm M, Hackmann J, Uleer C, et
al: Comparison of neoadjuvant nab-paclitaxel+carboplatin vs
nab-paclitaxel+gemcitabine in triple-negative breast cancer:
Randomized WSG-ADAPT-TN trial results. J Natl Cancer Inst.
110:628–637. 2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Gogas H, Pectasides D, Kostopoulos I,
Lianos E, Skarlos D, Papaxoinis G, Bobos M, Kalofonos HP, Petraki
K, Pavlakis K, et al: Paclitaxel and carboplatin as neoadjuvant
chemotherapy in patients with locally advanced breast cancer: A
phase II trial of the hellenic cooperative oncology group. Clin
Breast Cancer. 10:230–237. 2010.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Petrelli F, Coinu A, Borgonovo K, Cabiddu
M, Ghilardi M, Lonati V and Barni S: The value of platinum agents
as neoadjuvant chemotherapy in triple-negative breast cancers: A
systematic review and meta-analysis. Breast Cancer Res Treat.
144:223–232. 2014.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Pandy JGP, Balolong-Garcia JC,
Cruz-Ordinario MVB and Que FVF: Triple negative breast cancer and
platinum-based systemic treatment: A meta-analysis and systematic
review. BMC Cancer. 19(1065)2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Lokich J and Anderson N: Carboplatin
versus cisplatin in solid tumors: An analysis of the literature.
Ann Oncol. 9:13–21. 1998.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Greenup R, Buchanan A, Lorizio W, Rhoads
K, Chan S, Leedom T, King R, McLennan J, Crawford B, Kelly Marcom P
and Shelley Hwang E: Prevalence of BRCA mutations among women with
triple-negative breast cancer (TNBC) in a genetic counseling
cohort. Ann Surg Oncol. 20:3254–3258. 2013.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Caramelo O, Silva C, Caramelo F, Frutuoso
C and Almeida-Santos T: The effect of neoadjuvant platinum-based
chemotherapy in BRCA mutated triple negative breast
cancers-systematic review and meta-analysis. Hered Cancer Clin
Pract. 17(11)2019.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Wang CJ, Xu Y, Lin Y, Zhu HJ, Zhou YD, Mao
F, Zhang XH, Huang X, Zhong Y, Sun Q and Li CG: Platinum-based
neoadjuvant chemotherapy for breast cancer with BRCA mutations: A
meta-analysis. Front Oncol. 10(592998)2020.PubMed/NCBI View Article : Google Scholar
|