Introduction
Previous studies have reported that Kyolic aged
garlic extract improves cardiovascular function, including
peripheral and central blood pressure, central pulse pressure and
arterial stiffness, assessed using pulse wave velocity (PWV) in
adults with elevated PWV levels (1-5).
Central hemodynamic measures and arterial stiffness are regarded as
more important predictors than peripheral blood pressure for
cardiovascular disease, as concluded by expert consensus (6). The ability of an artery to expand and
contract in response to blood pressure changes may decrease as a
result of arterial stiffness (7).
Arterial stiffness increases with age by 1.43 m/s every 10 years
(8). This hardening of the blood
vessel wall occurs as a result of age-related structural changes,
including vascular calcification and the loss of elastin and
collagen fibers in the arterial wall and atherosclerosis (9). The consequence of this reduced
compliance is an increase in PWV, a method used for the assessment
of arterial stiffness (6,10). PWV is measured non-invasively
either directly by carotid-to-femoral aortic tonometry using the
SphygmoCor device (Cardiex) (11)
or indirectly by brachial pulse wave analysis with a computerized
algorithm using the Mobil-O-Graph device with a blood pressure cuff
(IEM GmbH) (12). The
Mobil-O-Graph's computerized algorithm is based on age and gender
adjusted population references values (13) and has been validated against the
gold standard tonometry for PWV (14).
Exercise is considered one of the most effective
approaches for the treatment and management of cardiovascular
disease (15,16). The amount of exercise an individual
is able to perform is dependent on their aerobic capacity and
exercise tolerance (17). Aerobic
capacity is limited by the ability of the cardiovascular system to
deliver oxygen to the working musculature (18). In addition to aerobic capacity,
lactate threshold, defined as the exercise intensity at which blood
lactate concentrations accumulate faster than they can be removed,
also decreases with age (19).
However, the lactate threshold does not appear to change with age
when expressed relative to percentage of
volume-maximal-oxygen-consumption (VO2max) (20).
An increased VO2max results in an
increased tolerance and ability to exercise and is reflected by
lower levels of exertion and a later onset of blood lactate
accumulation and reflects both the effect of the metabolic activity
and the economy of the movement. An individual's lactate threshold
represents applied aerobic power and aerobic capacity, which is
considered the single biggest driver of success in endurance events
(21). The concentration of blood
lactate levels is used to objectively monitor exercise intensity
during resistance and dynamic exercise (22). Delayed muscle soreness and
prolonged recovery can be assessed using the 10 point Likert Pain
Scale (23).
Aerobic capacity, measured by VO2max
during moderate to high intensity exercise, is inversely related to
arterial stiffness (24).
Age-related decline in aerobic capacity and lactate threshold leads
to reduced endurance performance (19,25).
Measures of aerobic capacity, including VO2max, defined
by maximal stroke volume (ml/beat), as well as heart rate
(beats/min) and arterio-venous O2 (ml/100 ml) decline
with age (19). Additionally, the
age-related decline in VO2max is independent of the
expected age-related decline in muscle mass (26). The arteries stiffen with age and
lead to an increase in aortic input impedance as well as vascular
afterload, thereby impeding the ejection of blood from the left
ventricle during systole and consequently reducing stroke volume
during exercise (19).
Animal studies suggest garlic supplements could
ameliorate physical fatigue and increase exercise tolerance and
oxygen uptake (27-29).
Additionally, a number of human clinical studies have reported that
garlic supplements improve aerobic capacity, in both an acute (5 h)
(30,31) and a sub-chronic (6 week) setting
(32). The cross-sectional study
by Ince et al (30),
involving 10 male athletes, reported that 900 mg of garlic powder
ingested 5 h before high intensity exercise significantly improved
VO2max. Another previously published cross-sectional
study by Womack et al (31), involving 18 fit males, also
reported that 900 mg of garlic powder ingested 3 h prior to high
intensity exercise significantly improved VO2max. A 6
week trial testing the effect of garlic oil on cardiac performance
and exercise tolerance in 30 patients with coronary artery disease
found garlic to significantly reduce the heart rate at peak
exercise and significantly reduce the work load upon the heart,
resulting in improved exercise tolerance (32). Increased arterial stiffness may be
a contributor to sudden cardiac events in otherwise physically fit
middle-aged endurance athletes. In Melbourne alone in the previous
10 years, 2 middle-aged (55-65 years) male masters open water
swimmers died due to an unexpected cardiac arrest during races
(33,34).
Recent advances in the study of cardiovascular
biomarkers include proteomics analysis. A urinary proteomics panel
has been shown to predict endpoints associated with cardiovascular
disease and cardiac events, including heart attack and stroke, in
asymptomatic patients independent of age and sex (35-37).
The validated proteomic profile consists of a panel of 25 urinary
polypeptide markers, which show significant differences between
patients who had a cardiac event and controls, making these
polypeptides useful biomarkers for risk assessment of future
cardiac events (36). In addition,
a study assessing the intake of 20 ml olive oil daily for 6 weeks
demonstrated statistically significant changes in cardiovascular
risk proteomic urinary biomarkers compared with the baseline
(38).
The present study aimed to assess the effect of
Kyolic aged garlic extract on arterial stiffness, aerobic capacity,
lactate threshold, muscle soreness, recovery time and urinary
proteomic biomarkers associated with cardiovascular risk in a
cohort of middle-aged recreational endurance athletes.
Materials and methods
Trial design and participants
Individuals were recruited at the National Institute
of Integrative Medicine (NIIM; Melbourne, Australia) between
October 2020-February 2024. Recreational endurance athletes (aged
40-65 years) were invited to participate in the present
double-blind parallel randomized placebo-controlled dose-response
trial of 12 weeks duration investigating the effect of Kyolic aged
garlic extract on arterial stiffness and aerobic fitness during
high intensity exercise on a cycle ergometer. Recreational
endurance athletes were defined as regularly undertaking ≥3 30
min/week moderate to high intensity exercise sessions, such as
triathlon, cycling, running or swimming.
The American Heart Association defines moderate
exercise intensity at 50-70% of the maximum heart rate and
vigorous/high exercise intensity at 70-85% of the maximum heart
rate (39). Individuals were
recruited through local fitness and masters cycling clubs, the NIIM
newsletter and NIIM social media.
Individuals were excluded from the study if they
were diagnosed with a cardiovascular condition, including a
previous heart attack or stroke, or had a chronic illness, such as
cancer. Additionally, individuals were also excluded if they had a
recent surgery or were planning any surgery or change in
medications, were pregnant during study or reported an intolerance
to garlic.
Participants were instructed to cease any garlic
supplementation prior to enrolment, and not to change their
exercise routine or diet during the 3 month trial. As Kyolic aged
garlic extract is consumed as a supplement with distinctly
different therapeutic effects compared with raw or cooked garlic,
the dietary intake of garlic was allowed to remain unchanged.
Participant allocation and trial
supplements
The study was conducted in two parts, the first
cohort was recruited between October 2020 and January 2022 and the
second cohort was recruited between January 2023 and February 2024.
Consenting eligible participants in the first cohort were randomly
allocated to the low dose consisting of two capsules of aged garlic
extract [Kyolic® Reserve Formula (Wakunaga of America,
Co., Ltd.,) containing 1.2 g AGE powder and 1.2 mg S-allylcysteine
(SAC)] or placebo (containing inert microcrystalline cellulose)
daily for 12 weeks. In the second cohort participants were randomly
allocated to the high dose consisting of four capsules of aged
garlic extract (Kyolic® Reserve Formula containing 2.4 g
AGE powder and 2.4 mg SAC) or placebo taken daily for 12 weeks. A
computer-generated permuted random number table provided by an
independent researcher not involved in recruitment, data collection
or follow-up for the present study was used for randomization.
Kyolic aged garlic extract powder was manufactured
from organically grown garlic bulbs, which have undergone a 20
month natural ageing process at room temperature. Placebo capsules
were matched in appearance to the opaque active capsules and
packaged in identical containers by the manufacturers off-site.
Activated carbo-sachets were added to each container to disguise
any odor. Participants, investigators and researchers were blinded
to treatment allocation. Blinding success was assessed at the end
of the trial by questionnaire.
Participants were instructed to start taking their
trial capsules with food to minimize belching after the first
VO2max testing session at baseline. Compliance was
assessed by questionnaire and by capsule count throughout the
study.
Assessments
Participants had four monthly appointments at NIIM
(weeks 0, 4, 8 and 12), and two appointments at the Mets
Performance exercise physiologist center (Melbourne, Australia) for
testing of aerobic capacity with VO2max on a cycle
ergometer, both at the beginning (week 0) and at the end of the
study (week 12).
Baseline demographics
Participants' age, sex, BMI, regular medication and
supplement intake and exercise routines were collected at
baseline.
Exercise routines
The participants' exercise routines were assessed
using an online questionnaire adapted from the International
Physical Assessment Questionnaire (40) to quantify the length of regular
moderate and high intensity exercises throughout the week.
Arterial stiffness, pulse wave
velocity (PWV) and blood pressure
Arterial stiffness was assessed by non-invasive
validated methods measuring PWV (41) using the SphygmoCor Xcel (Cardiex)
(11) in cohort 1 and the
Mobil-O-Graph device (IEM GmbH) (12) in cohort 2, due to the SphygmoCor
Xcel no longer being supported in Australia from 2023. The
Mobil-O-Graph has been validated against the gold standard
tonometry for central blood pressure (14) and pulse wave analysis (42). However, PWV measurements are not
directly comparable, whereby the Mobil-O-graph measured
consistently lower PWV values compared with the SphygmoCor
tonometer (43), therefore the PWV
was presented separately for each cohort. The SphygmoCor Xcel
(11) measures PWV directly by
tonometry from carotid to femoral artery, while the patient is in a
supine position. The Mobil-O-Graph (12) is a non-invasive device measuring
central hemodynamic measures via a blood pressure cuff, such as
blood pressure, pulse pressure, heart rate and PWV, an indicator
for arterial stiffness. PWV is the speed in which the blood travels
through the arteries in m/sec and is derived from the brachial
pulse and indirectly calculated by a computerized algorithm and
compared with age- and sex-adjusted population references
values.
Participants were advised to refrain from drinking
coffee or having a large meal for at least 2 h prior to the
measurements and after at least 5 min of rest. Blood pressure was
taken using a calibrated and validated digital sphygmomanometer
(Omron HEM-907; Omron Healthcare Singapore Pte Ltd) (44).
Aerobic fitness, capacity,
VO2max and lactate threshold
Aerobic fitness was measured by VO2max
and aerobic and anaerobic/lactate threshold during high-intensity
exercise using a cycle ergometer test station. The cyclist was
connected to an oxygen analyzer, which measured the ratio of
CO2 to the volume of oxygen intake. Blood lactate
concentration was measured using a finger prick throughout the
exercise workout.
VO2 max is defined as the maximum amount
of oxygen your body can take in, transport via the blood stream
into the muscles and utilize in 1 min.
Relative VO2 max (ml/kg/min) measures the
maximum amount of oxygen that an individual can utilize during
intense or maximal exercise, in ml/kg body weight/min. Absolute
VO2 max (ml/min) is the total volume of oxygen
regardless of body weight and is important for non-weight bearing
activities such as swimming and flat cycling.
Cycle ergometer test procedure and
bike protocol
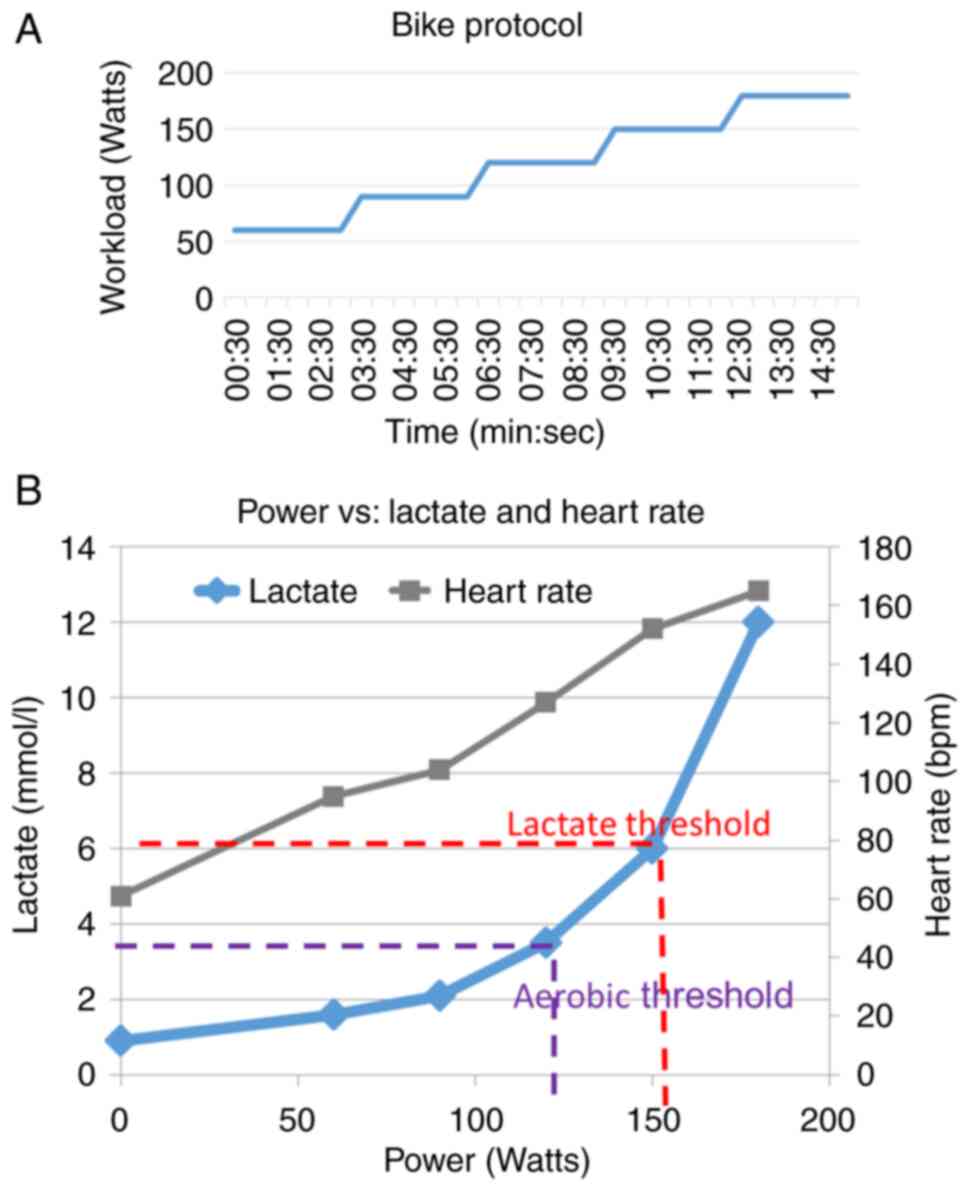
The exercise workloads were selected to gradually
progress in increments from moderate to maximal intensity. In the
present study workload in increments of 30 Watts of power was
increased every 3 min, starting at 60 Watts (Fig. 1A).
Aerobic and anaerobic lactate
threshold
When exercising, energy is first produced
aerobically by using oxygen and primarily by burning fat and
carbohydrates, such as glucose. The aerobic threshold is reached
when the production of energy starts to become dominated by
anaerobic glycolysis (sugars) rather than the oxidation (aerobic in
nature) of fats. Anaerobic energy production without oxygen
produces lactate or lactic acid, and the lactate threshold is
defined as the level of exercise intensity causing lactate to
accumulate in the blood at a faster rate than it can be removed
(Fig. 1B).
The lactate threshold test consisted of multiple
blood lactate concentration measurements by a finger prick at the
immediate completion of each incremental workload (30 Watts) during
the cycling test, which was conducted until the participant's
maximal intensity was reached. The lactate threshold occurs at a
percentage of an athlete's VO2max based on their
training status. In untrained individuals the lactate threshold is
reached at ~50-60% of VO2max and in trained individuals
at ~70-80% of VO2max. A higher lactate threshold
correlates to better overall athletic performance.
Recovery time and muscle soreness and
pain
Recovery time was assessed in days by a simple
questionnaire, and muscle soreness by a pain 10-point Likert scale
at baseline and at 12 weeks.
Proteomics
Urinary proteomic analysis was carried out by the
Commonwealth Scientific and Industrial Research Organisation Land
and Water following the protocol published by Zimmerli et al
(35), featuring a panel of 22
cardiovascular risk-relevant peptides using high-resolution liquid
chromatography-mass spectrometry (LC-MS). Proteins (>3 KDa) were
removed from urine samples using Amicon Centrifugal Filter Units at
16,100 x g at room temperature for 5-10 min using an Eppendorf
centrifuge. Urine samples were normalized to the measured
creatinine concentration and urine samples were dried in a
speed-Vac. Sample pellets were resuspended in 40 ul of 0.1% formic
acid in preparation for LC-MS analysis and 5 ul was injected onto
the LC-MS for analysis. Samples were desalted and concentrated with
a trap column (PepMap100 C18 5 mm x 300 µm, 5 µm, Thermo
Scientific. Inc.) and separated on a nano column (PepMap100 C18 150
mm x 75 µm, 2 µm, Thermo Scientific. Inc.) using an
UltimateTM 3000 RSLC nano LC system (Thermo Scientific.
Inc.). Flow rate was 300 nl/min and system temperature was 35˚C.
Mobile phase A consisted of water and 0.1% (v/v) formic acid and
mobile phase B consisted of 80% (v/v) acetonitrile and 0.08% (v/v)
formic acid. Urine peptides were eluted using a gradient of 5 to
60% solvent B for 20 min and 60 to 99% solvent B for 7 min. The
eluted peptides were ionized with a Nanospray Flex Ion Source
(Thermo Scientific. Inc.). The spray voltage was set to 2.3 kV and
the temperature of the heated capillary was set at 300˚C. Sweep
nitrogen gas flow rate was at 1.5l/min and source pressure was at
1.48 Torr. After ionization, mass spectra (MS1) and tandem mass
spectra (MS/MS) analysis was performed using an Orbitrap Fusion MS
(Thermo Scientific. Inc.). MS survey scans of peptide precursors
were performed in the Orbitrap detector and the scan range was 400
to 1500 m/z at resolution of 120 K (at 200 m/z). The target value
of automatic gain control (AGC) was set as 4 x 105. The
maximum injection time for the MS was 50 ms. MS/MS was performed on
the most abundant precursors of charge states 2+ to 7+ with
intensity greater than 1 x 105. They were isolated by
the quadrupole with a window of 1.6 m/z. Fragmentation was achieved
by high-energy collisional dissociation (HCD) with collision energy
of 28%. Fragments were detected in the ion trap detector in rapid
scan rate mode. The AGC target was 4 x 103, maximum
injection time was 300 ms and the dynamic exclusion was 15 sec. The
instrument was set to run in top speed mode with a three sec cycle
for both the MS and MS/MS scans.
A list of 81 urinary peptides identified by Brown
et al (36) was used to
search peptides in the urine samples. Precursor mass tolerance was
set to 10 ppm and product ions were searched at 0.6 Da. No-Enzyme
(unspecific) was selected. Modification included Oxidation (+15.995
Da). Creatinine, a clearance protein, was measured to adjust for
differences in urinary concentration between patients due to
hydration variances. Urine creatinine concentration was measured
using an ELISA-based assay using a Creatinine Urinary Detection Kit
(cat. no. EIASCR; Invitrogen; Thermo Fisher Scientific, Inc.) and
measured using a UV-Vis spectrometer at a wavelength of 490 nm.
Each urine sample was diluted 1:20 and 50 µl was used for the assay
as per the manufacturer's protocol.
Statistical analysis
Primary outcome measures were aerobic fitness,
including VO2max, aerobic and lactate threshold and
power. Secondary outcome measures were recovery time, muscle
soreness, PWV and proteomic biomarkers. Analyses were performed
using SPSS Inc. (version 26; IBM Corp.). P<0.05 was considered
to indicate a statistically significant difference.
Differences between groups at baseline were assessed
by χ2 test or Fisher's Exact test if the values were
<5 for categorical variables and by an unpaired Student's t-test
for continuous variables.
The participant's mean change score (value at 12
weeks- value at baseline) was calculated for each outcome measure
and ANCOVA with Bonferroni's correction was performed. Relevant
baseline values were used as co-variates to assess the mean
differences between groups (garlic vs. placebo).
For the main statistical analyses, cohort 1 and
cohort 2 were combined (low and high dose), and subgroup analysis
was performed by cohort.
Polypeptide data were normalized to creatinine
clearance protein. Missing values were replaced by one-fifth of the
minimum positive values of their corresponding variables. The
acquired data were then log10 transformed and scaled using the
mean-centred value and divided by the SD of each variable. Data
were then subjected to univariate and multivariate statistical
analysis using SIMCA (version 17.01; Sartorius Stedim Biotech;
Sartorius AG). GraphPad Prism (version 9.3.0; Dotmatics) was used
for descriptive statistical analysis and plot generation.
A 15 peptide quality assurance and quality control
(QAQC) standard consisting of 15 heavy isotope-labelled peptides
(cat number 88321; Thermo Fisher Scientific, Inc.) was analysed
throughout the analytical sequence and was found to be with a 5%
relative standard deviation, demonstrating good analytical
performance of the column and MS detector.
Results
Participants
The trial was conducted in two parts whereby the
first cohort, allocated the low trial supplement dose, was
recruited between October 2020 and January 2022 during the COVID-19
lockdowns and the second cohort, allocated the high trial
supplement dose, was recruited between January 2023 and February
2024.
A total of 108 potential participants were screened
for eligibility, with a total of 24 either not fitting inclusion
criteria (n=18) or losing interest shortly after enrollment into
the study (n=6). Of the potential participants, one was not
eligible on medical grounds due to a high PWV reading at screening
prompting a consultation with a cardiologist and a subsequent
diagnosis of severe coronary artery disease, despite not having any
other risk factors such as hypertension or high cholesterol. A
further nine participants withdrew after baseline VO2max
testing, either due to losing interest in the study (n=4), the long
travel distance to and from the study site (n=2), COVID-19 lockdown
(n=1), study-unrelated gastroenteritis (n=1) or medical advice from
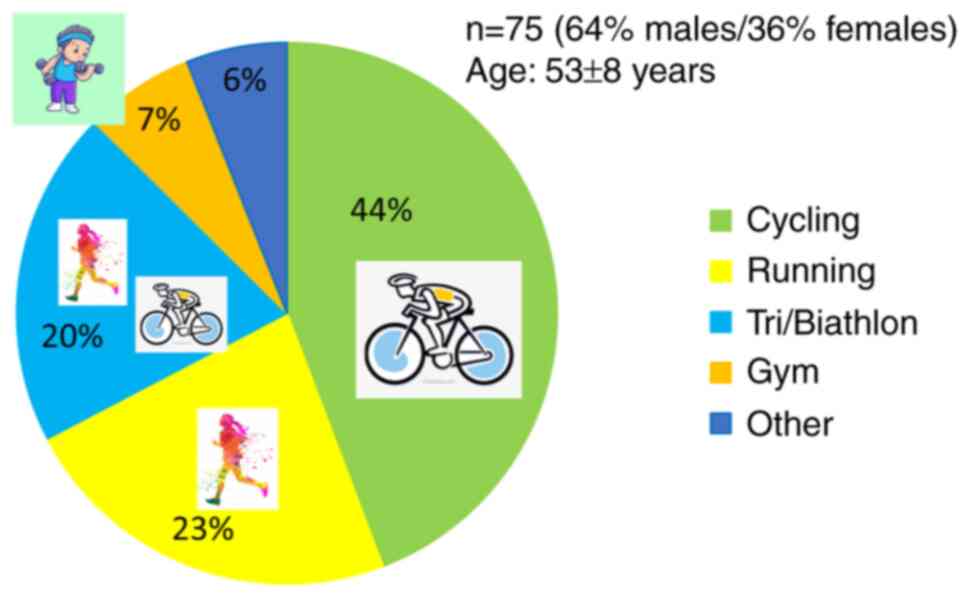
the patient's doctor (n=1). In total, 75 participants completed the
study, including 37/40 (92%, cohort-1) and 38/40 (95%, cohort-2).
The mean age was 53±8 years and two-thirds of the participants were
male (Table I).
 | Table IParticipant characteristics of cohort
1 and cohort 2. |
Table I
Participant characteristics of cohort
1 and cohort 2.
| | P-value | |
|---|
| Characteristic | All participants
(n=75) | Garlic-treated
group (n=37) | Placebo-treated
group (n=38) | between groups |
|---|
| Age, years (mean ±
SD) | 52.6±8.1 | 52.8±7.4 | 53.1±8.1 | ns |
| Male/female, n
(%) | 48/27 (64/36%) | 23/14 (62/38%) | 25/14 (66/34%) | ns |
| BMI,
kg/m2 (mean ± SD) | 24.2±3.1 | 24.9±3.2 | 23.6±2.8 | ns |
| Type of exercise, n
(%) | | | | |
|
Cycling | 33 (44%) | 16 (43%) | 17 (45%) | ns |
|
Running | 17 (23%) | 8 (22%) | 9 (24%) | ns |
|
Tri-/biathlon | 15 (20%) | 8 (22%) | 7 (18%) | ns |
|
Gym | 5 (7%) | 2 (5%) | 3 (8%) | ns |
|
Other | 5 (7%) | 3 (8%) | 2 (5%) | ns |
| Medications, n
(%) | | | | |
|
None | 52 (69%) | 28 (76%) | 24 (71%) | ns |
|
Statin | 5 (7%) | 1 (3%) | 4 (10%) | ns |
|
Blood
pressure medication | 6 (8%) | 4 (11%) | 2 (5%) | ns |
|
Anti-depressant | 6 (8%) | 2 (5%) | 4 (10%) | ns |
|
Other | 7 (9%) | 3 (8%) | 4 (10%) | ns |
| Supplements, n
(%) | | | | |
|
None | 33 (44%) | 12 (32%) | 21 (55%) | ns |
|
Magnesium | 25 (33%) | 15 (41%) | 10 (26%) | ns |
|
Other | 43 (57%) | 25 (68%) | 26 (68%) | ns |
All participants in the first cohort were serious
endurance athletes who trained an average of 1.5 h daily with
moderate to high intensity exercise (~1 h moderate and ~30 min high
intensity) of either cycling, running or swimming. The majority
(86%) of participants in cohort-1 were cyclists, cycling up to 400
km or 17 h per week (Table
II).
| Table IIExercise regimes performed by cohorts
1 (A) and 2 (B). |
Table II
Exercise regimes performed by cohorts
1 (A) and 2 (B).
| A, Cohort 1 |
|---|
| Characteristic | All, participants
n=39 | Garlic-treated,
group n=19 | Placebo-treated,
group n=20 | P-value between
garlic- and placebo-treated groups | P-value between
cohorts 1 and 2 |
|---|
| Cycle/run/other,
% | 86/11/3 | 84/16/0 | 88/6/6 | | |
| Exercise regime,
mean ± SD | | | | | |
| Moderate intensity,
min/week | 379±304 | 443±357 | 318±238 | ns | 0.004 |
|
min/day | 54±43 | 32±51 | 45±34 | | |
| High intensity,
min/week | 280±299 | 212±226 | 344±350 | ns | 0.001 |
|
min/day | 40±42 | 30±32 | 49±50 | | |
| B, Cohort 2 |
| Characteristic | All, participants
n=39 | Garlic-treated,
group n=19 | Placebo-treated,
group n=20 | P-value between
garlic- and placebo-treated groups | P-value between
cohorts 1 and 2 |
| Cycle/run/other,
% | 36/34/30 | 37/26/37 | 32/42/26 | ns | |
| Exercise regime,
mean ± SD | | | | | |
| Moderate intensity,
min/week | 213±159 | 194±109 | 235±202 | ns | 0.004 |
|
min/day | 30±22 | 28±16 | 34±29 | | |
| High intensity,
min/week | 105±101 | 101±76 | 110±125 | ns | 0.001 |
|
min/day | 15±14 | 14±11 | 16±18 | | |
The second cohort was significantly less athletic
overall compared with the first cohort, training an average of 45
min daily of moderate to high intensity exercise (~30 min moderate
and ~15 min high intensity) (Table
II). Participants in cohort-2 exercised through a variety of
sports including cycling, running, rowing, swimming, kick boxing,
Bikram hot yoga and underwater hockey (Table II, Fig. 2).
Blood pressure and PWV
At baseline there were no statistical differences in
blood pressure or PWV between the garlic vs. placebo groups.
However, at the end of the study, a marked improvement in blood
pressure and PWV was observed in the Kyolic group compared with the
placebo group in a subgroup of participants with elevated blood
pressure (>135 mmHg SBP), as well as in PWV (Table III).
| Table IIIBlood pressure and pulse wave
velocity (cohort-1 & cohort-2, n=75). |
Table III
Blood pressure and pulse wave
velocity (cohort-1 & cohort-2, n=75).
| | Baseline | 12 weeks | 12
weeks-baseline | Garlic vs.
placebo |
|---|
| Variable and
treatment group | Participant number,
n | Mean | SD | Mean | SD | Estimated marginal
mean | SE | Mean
difference | SE | P-value |
|---|
| SBP, mmHg | | | | | | | | | | |
|
Garlic | 37 | 129.2 | 13.1 | 122.8 | 11.7 | -6.8 | 1.4 | -0.6 | 2.0 | ns |
|
Placebo | 38 | 130 | 13.9 | 122.5 | 15.4 | -7.4 | 1.4 | | | |
| SBP >135
mmHg | | | | | | | | | | |
|
Garlic | 14 | 142.1 | 4.4 | 130.6 | 8.2 | -12.4 | 2.5 | -2.9 | 3.5 | ns |
|
Placebo | 14 | 144.4 | 10.8 | 134.8 | 15.2 | -9.5 | 2.5 | | | |
| DBP, mmHg | | | | | | | | | | |
|
Garlic | 37 | 76.5 | 10.3 | 74.4 | 8.2 | -2.6 | 1.3 | 1.3 | 1.8 | ns |
|
Placebo | 38 | 78.4 | 9.2 | 74.1 | 10.6 | -3.9 | 1.3 | | | |
| PWV cohort 1,
m/s | | | | | | | | | | |
|
Garlic | 18 | 10.0 | 1.5 | 9.5 | 1.3 | -0.6 | 0.3 | 0.03 | 0.4 | ns |
|
Placebo | 19 | 10.2 | 1 | 9.8 | 1.2 | -0.7 | 0.3 | | | |
| PWV cohort 2,
m/s | | | | | | | | | | |
|
Garlic | 19 | 7.5 | 1.1 | 7.3 | 1.0 | -0.2 | 0.1 | -0.15 | 1.8 | ns |
|
Placebo | 19 | 7.8 | 0.9 | 7.7 | 0.9 | -0.1 | 0.1 | | | |
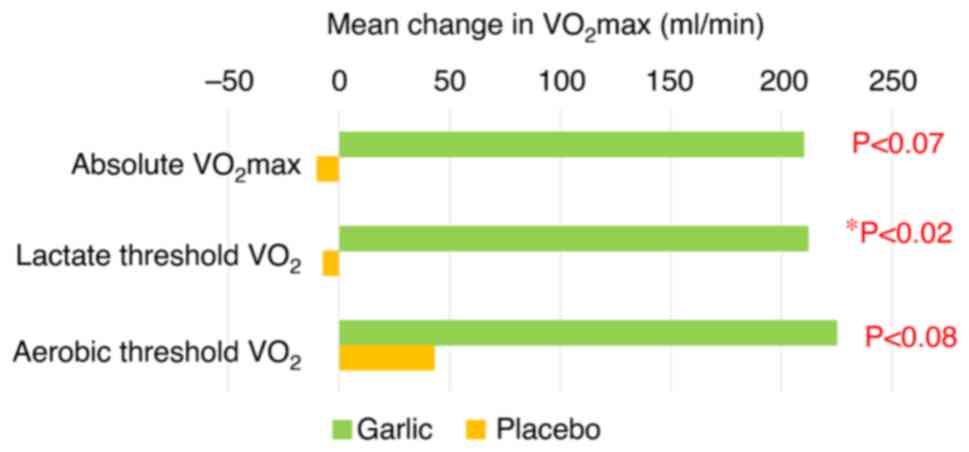
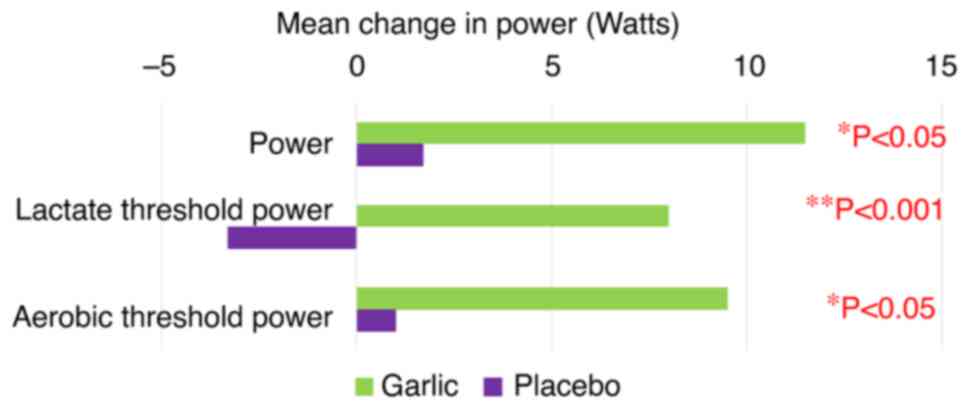
Primary outcome measures of aerobic
fitness, VO2max, lactate threshold and power
Kyolic aged garlic extract significantly improved
aerobic fitness, as evidenced by increased absolute
VO2max (mean difference, 133±83 ml/min; P<0.07),
power (mean difference, 10.2±4.9 W; P<0.04), lactate threshold
to power output (mean difference, 11.8±3.2 W; P<0.001), lactate
threshold to oxygen uptake (mean difference, 174±72 ml/min;
P<0.02) and aerobic threshold to power output (mean difference,
9.1±4.5 W; P<0.045) (Table IV,
Figs. 3 and 4).
| Table IVAerobic capacity measures of cohorts
1 and 2. |
Table IV
Aerobic capacity measures of cohorts
1 and 2.
| | Baseline | 12 weeks | 12
weeks-baseline | Garlic compared
with placebo |
|---|
| Variable | Participant number,
n | Mean | SD | Mean | SD | Estimated marginal
mean | SE | Mean
difference | SE | P-value |
|---|
| Absolute
VO2max, ml/min | | | | 3 | | | | | | |
|
Garlic | 34 | 3,119 | 935 | 3,280 | 946 | 165 | 59 | 133 | 83 | 0.07 |
|
Placebo | 36 | 3,022 | 1,054 | 3,058 | 1,004 | 32 | 58 | | | |
| Relative
VO2max, ml/kg/min | | | | | | | | | | |
|
Garlic | 34 | 39.8 | 11.6 | 41.8 | 10.8 | 1.9 | 0.8 | 1.9 | 1.5 | ns |
|
Placebo | 36 | 41.1 | 11.3 | 41.6 | 1.7 | 0.6 | 0.8 | | | |
| Power, W | | | | | | | | | | |
|
Garlic | 34 | 235 | 71 | 246 | 72 | 11.7 | 3.5 | 10.2 | 4.9 | 0.04 |
|
Placebo | 36 | 224 | 74 | 226 | 72 | 1.5 | 3.4 | | | |
| Lactate T Power,
W | | | | | | | | | | |
|
Garlic | 34 | 186 | 61 | 194 | 63 | 8.4 | 2.3 | 11.8 | 3.2 | <0.001 |
|
Placebo | 36 | 178 | 65 | 174 | 62 | -3.5 | 2.2 | | | |
| VO2max
HR, bpm | | | | | | | | | | |
|
Garlic | 34 | 163 | 17 | 166 | 15 | 3.1 | 1.1 | 1.9 | 1.5 | ns |
|
Placebo | 36 | 164 | 16 | 165 | 16 | 1.3 | 1.1 | | | |
| Lactate T HR,
bpm | | | | | | | | | | |
|
Garlic | 34 | 148 | 16 | 153 | 23 | 5.3 | 2.3 | 4.7 | 3.3 | ns |
|
Placebo | 36 | 148 | 15 | 149 | 17 | 0.6 | 2.3 | | | |
| Lactate T
VO2, ml/min | | | | | | | | | | |
|
Garlic | 34 | 2,647 | 820 | 2,768 | 902 | 125 | 50 | 174 | 72 | 0.018 |
|
Placebo | 36 | 2,556 | 927 | 2,510 | 835 | -49 | 52 | | | |
| Lactate T
%VO2max, % | | | | | | | | | | |
|
Garlic | 34 | 85.1 | 7.6 | 83.5 | 7.9 | -1.3 | 1.2 | 1.2 | 1.7 | ns |
|
Placebo | 36 | 84.5 | 6.7 | 82.3 | 6.2 | -2.5 | 1.2 | | | |
| Aerobic T Power,
W | | | | | | | | | | |
|
Garlic | 34 | 138 | 50 | 147 | 54 | 9.7 | 3.2 | 9.1 | 4.5 | 0.045 |
|
Placebo | 36 | 130 | 56 | 131 | 52 | 0.6 | 3.1 | | | |
| Aerobic T HR,
bpm | | | | | | | | | | |
|
Garlic | 34 | 127.4 | 16.6 | 128.6 | 16.7 | 1.2 | 9.5 | -1.6 | 2.2 | ns |
|
Placebo | 36 | 125 | 17.4 | 128.1 | 17.7 | 2.8 | 8.7 | | | |
| Aerobic T
VO2, ml/min | | | | | | | | | | |
|
Garlic | 34 | 2,123 | 688 | 2,232 | 785 | 113.5 | 48 | 106 | 67 | ns |
|
Placebo | 36 | 2,026 | 824 | 2,038 | 694 | 7.2 | 47 | | | |
| Aerobic T
%VO2max, % | | | | | | | | | | |
|
Garlic | 34 | 68.2 | 8.1 | 67.1 | 8.9 | -0.5 | 1.3 | 0.3 | 1.8 | ns |
|
Placebo | 36 | 66.5 | 8.9 | 66.9 | 6.7 | -0.2 | 1.2 | | | |
Comparison of baseline aerobic fitness
between low dose and high dose cohorts
While there were no significant differences between
the garlic and the placebo groups in participants' types of sports
(Table II, Fig. 2), there were differences in
exercise regimes and fitness levels between the first cohort (low
dose) and the second cohort (high dose) at baseline. While the
first cohort exercised a mean of ~90 min/day (54 min of moderate
intensity and 40 min of high intensity/day), the second cohort
exercised a mean of 45 min/day (30 min moderate and 15 min high
intensity/day), which was approximately one-half of the time
exercising and at a lower intensity compared with the first cohort
(Table V).
| Table VExercise regime and aerobic fitness
at baseline in the low- and high-dose garlic groups. |
Table V
Exercise regime and aerobic fitness
at baseline in the low- and high-dose garlic groups.
| | Low dose, n=37 | High dose,
n=34 | | |
|---|
| Variable | Mean ± SD | Mean ± SD | Mean difference ±
SE | P-value |
|---|
| Moderate intensity
exercise, min/day | 54±43 | 30±22 | 14±8 | 0.001 |
| High intensity
exercise, min/day | 40±42 | 15±14 | 25±7 | 0.004 |
| Absolute
VO2max, ml/max | 3,467±930 | 2,654±877 | 813±215 | <0.001 |
| Relative
VO2max, ml/kg/min | 45±11 | 36±10 | 9±3 | <0.001 |
| Power, W | 257±67 | 200±65 | 57±16 | <0.001 |
| Lactate T Power,
W | 211±58 | 151±50 | 61±13 | <0.001 |
| Lactate T
VO2, ml/min | 2,993±841 | 2,184±686 | 810±183 | <0.001 |
| Aerobic T Power,
W | 160±52 | 106±37 | 55±11 | <0.001 |
| Aerobic T
VO2, ml/min | 2,404±781 | 1,720±533 | 684±160 | <0.001 |
As the baseline levels of certain aerobic fitness
measurements, such as VO2max, were significantly
different between the two cohorts (low dose vs. high dose,
P<0.001), a dose-response analysis was not feasible (Table V). The baseline fitness of the two
cohorts would have influenced or confounded any dose-dependent
outcome measures. However, in both cohorts, the Kyolic group had
statistically significant improvements in aerobic fitness compared
with the placebo group (Table
SI).
Compared with cohort 2, aerobic capacity improved
significantly in cohort 1, as evidenced by increased absolute
VO2max (mean difference, 238±105 ml/min; P<0.03),
power (mean difference, 16.2±7.3 W; P<0.035), lactate threshold
to power output (mean difference, 16.9±5.4 W; P<0.003), lactate
threshold to oxygen uptake (mean difference, 269±104 ml/min;
P<0.014) and aerobic threshold to oxygen uptake (mean
difference, 245±90 ml/min; P<0.01; Table SI).
Recovery time and muscle soreness
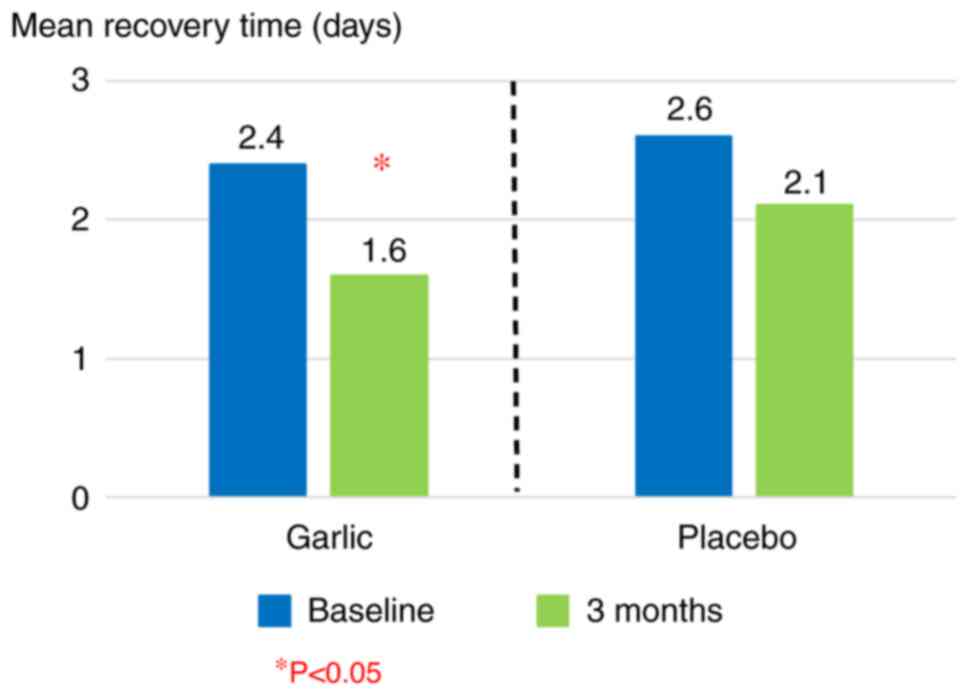
Kyolic aged garlic extract significantly improved
aerobic fitness, as evidenced by quicker recovery times compared
with the placebo group in both treatment cohorts combined (n=70;
mean difference, -0.6±0.3 days; P<0.05) (Table VI, Fig. 5). Additionally, the difference in
the recovery time was more pronounced in the cohort 1 (low dose),
with the garlic-treated group recovering significantly quicker
compared with the placebo group after exercise (mean difference,
-1.1±0.5 days; P<0.025) (Table
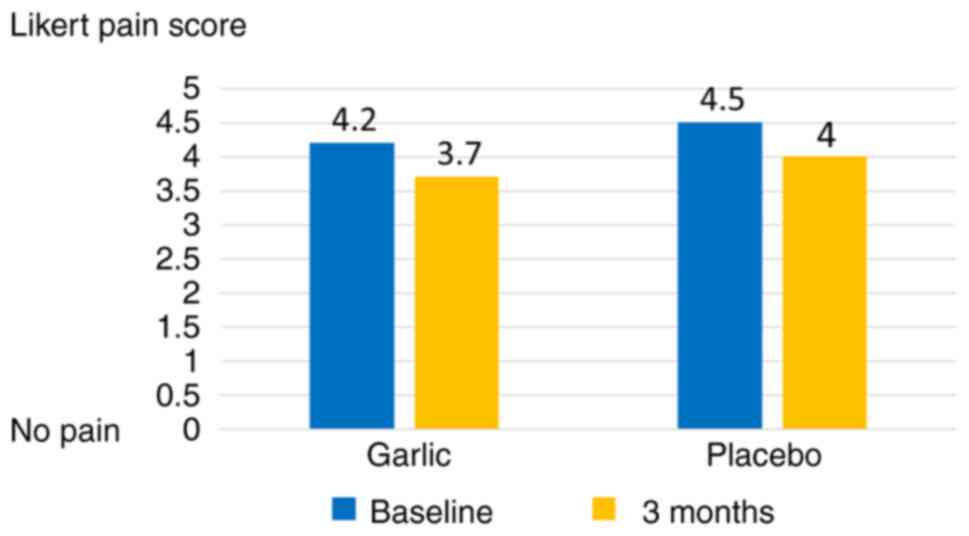
VI). Muscle soreness was reduced in both groups compared with
baseline (albeit not significantly; Fig. 6).
| Table VIRecovery time and muscle
soreness. |
Table VI
Recovery time and muscle
soreness.
| A, Cohort 1 and
2 |
|---|
| | Baseline | 12 weeks | Within groups | Garlic compared
with placebo | Between groups |
|---|
| Variable | Participants,
n | Mean | SD | Mean | SD | Mean change | SD | Mean
difference | SE | P-value |
|---|
| Recovery time,
days | | | | | | | | | | |
|
Garlic | 37 | 2.6 | 1.7 | 1.6 | 1.4 | -1.0 | 1.2 | -0.6 | 0.3 | 0.05 |
|
Placebo | 37 | 2.4 | 1.7 | 2.1 | 1.4 | -0.4 | 1.5 | | | |
| Muscle soreness,
1-10 | | | | | | | | | | |
|
Garlic | 35 | 4.2 | 1.8 | 3.7 | 2.1 | -0.52 | 2.0 | -0.06 | 0.45 | ns |
|
Placebo | 35 | 4.5 | 1.9 | 4.0 | 2.3 | -0.51 | 1.8 | | | |
| B, Cohort 1 |
| | Baseline | 12 weeks | Within groups | Garlic compared
with placebo | Between groups |
| Variable | Participants,
n | Mean | SD | Mean | SD | Mean change | SD | Mean
difference | SE | P-value |
| Recovery time,
days | | | | | | | | | | |
|
Garlic | 18 | 2.9 | 2.0 | 1.7 | 1.5 | -1.2 | 1.3 | -1.1 | 0.5 |
0.025* |
|
Placebo | 19 | 2.9 | 1.2 | 2.7 | 1.5 | 0.1 | 1.5 | | | |
| C, Cohort 2 |
| | Baseline | 12 weeks | Within groups | Garlic compared
with placebo | Between groups |
| Variable | Participants,
n | Mean | SD | Mean | SD | Mean change | SD | Mean
difference | SE | P-value |
| Recovery time,
days | | | | | | | | | | |
|
Garlic | 19 | 2.3 | 1.4 | 1.4 | 0.8 | -0.8 | 1.0 | -0.2 | 0.4 | ns |
|
Placebo | 19 | 2.1 | 1.1 | 1.5 | 1.1 | -0.6 | 1.4 | | | |
Cardiovascular risk-related proteomic
urinary biomarkers
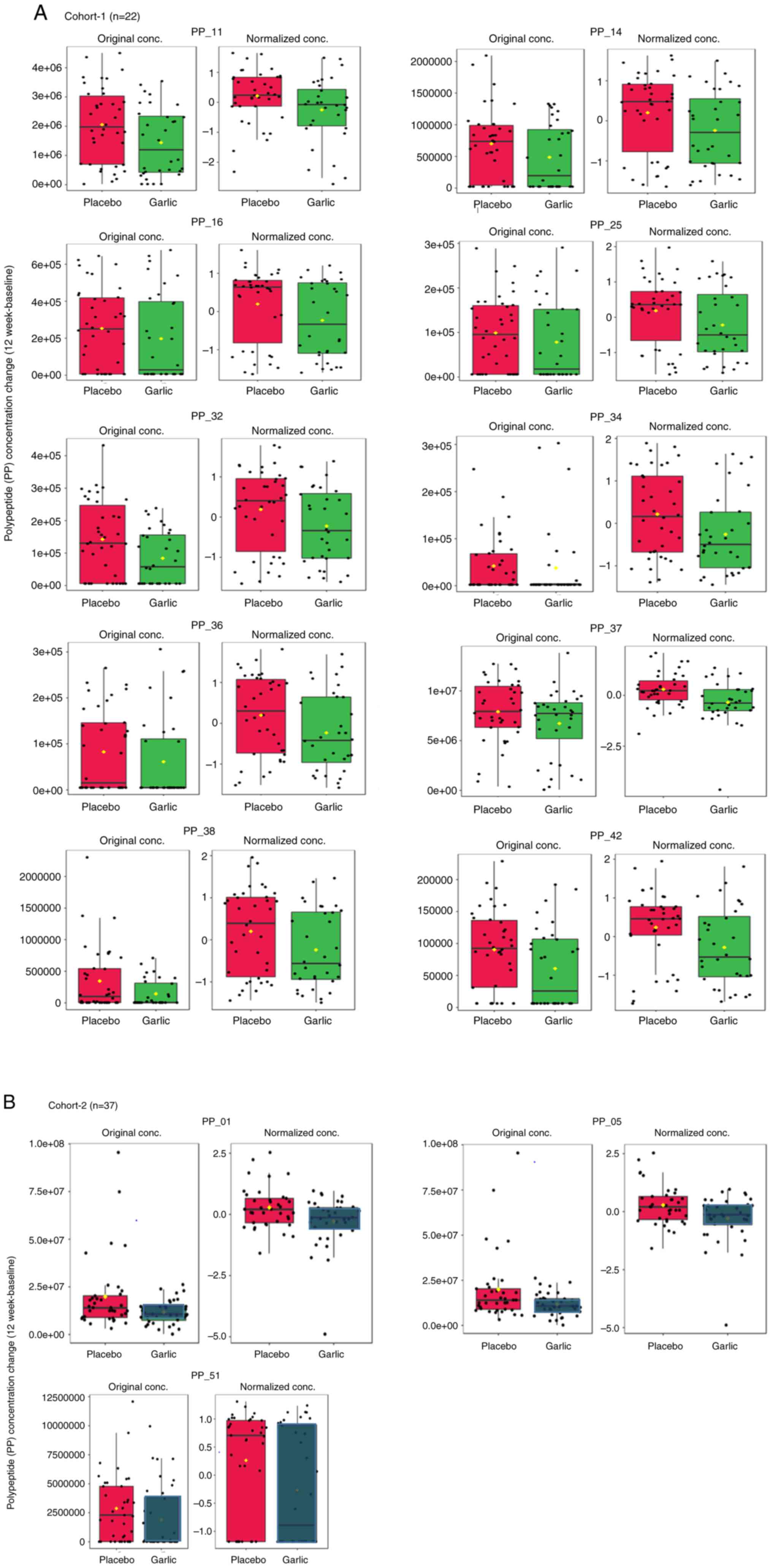
In a subgroup of participants from the first cohort
(n=22) and the second cohort (n=37), a panel of 22 polypeptides and
their derivates were tested. As higher concentrations of these
polypeptides have been associated with higher cardiovascular risk,
a reduction in the levels of these polypeptides is desirable. It
was demonstrated that a subset of polypeptides significantly
decreased in the Kyolic group compared with the placebo group,
leading to an improved cardiovascular risk proteomic profile in the
Kyolic group at the end of the study (Table VII, Fig. 7). Proteomic analysis differed
between the cohorts. In the low dose cohort, 10/22 (45%) of the
peptide concentrations were significantly reduced in the Kyolic
group compared with the placebo (Fig.
7a) and 3/22 (13%) were significantly reduced in the second
cohort (Fig. 7b). Furthermore, the
mean polypeptide baseline levels varied between the cohorts.
Therefore, a combined proteomic analysis of both cohorts was not
statistically meaningful.
| Table VIIList of PPs with significant
differences in PP concentration change between the garlic group
compared with the placebo group. |
Table VII
List of PPs with significant
differences in PP concentration change between the garlic group
compared with the placebo group.
| Cohort | PP | Description |
|---|
| HD | PP_01 |
Uromodulin_53181 |
| HD | PP_05 |
Uromodulin_45496 |
| LD | PP_11 | Collagen alpha-1(I)
chain_77018 |
| LD | PP_14 | Collagen alpha-1(I)
chain_80551 |
| LD | PP_16 | Collagen alpha-2(I)
chain_127354 |
| LD | PP_25 | Collagen alpha-2(I)
chain_68036 |
| LD | PP_32 | Membrane associated
progesterone receptor component 1_49958 |
| LD | PP_34 | Collagen alpha-1(I)
chain_127852 |
| LD | PP_36 | Collagen alpha-2(I)
chain_125628 |
| LD | PP_37 |
Beta-1,3-galactosyltransferase6_44592 |
| LD | PP_38 | Collagen
alpha-1(III) chain_49295 |
| LD | PP_42 | Collagen alpha-1(I)
chain_45384 |
| HD | PP_51 | Collagen
alpha-1(III) chain_111001 |
Compliance, tolerability and
blinding
Compliance was satisfactory, with all participants
taking their trial supplements >95% according to protocol.
Tolerability was high, with 1 participant in the
placebo group noting a weight gain of 2-3 kg over the course of the
study and 1 participant in the garlic group noting a lower heart
rate. In the garlic group, 1 participant reported burping, which
did not bother her and another participant noted that her menstrual
cycle improved becoming more regular and less painful.
Blinding was successful in both cohorts. In the low
dose cohort 1, the majority (80%) were unsure of their group
allocation, while 5% guessed their group allocation incorrectly,
verifying successful blinding. In the high dose cohort 2, a greater
proportion guessed correctly (37%) compared with the low dose
cohort 1 (16%) and two-thirds (63%) were unsure or incorrect
(Table VIII).
| Table VIIIBlinding of study. |
Table VIII
Blinding of study.
| Assumed group
allocation | All, n (%) | Low dose cohort, n
(%) | High dose cohort, n
(%) |
|---|
| Correct | 20 (27%) | 6 (16%) | 14 (37%) |
| Incorrect | 15 (20%) | 2 (5%) | 13 (34%) |
| Unsure | 40 (53%) | 29 (78%) | 11 (29%) |
| Total | 75 (100%) | 37 (100%) | 38 (100%) |
Discussion
The results of the study demonstrated that Kyolic
aged garlic extract significantly improved aerobic fitness in
middle-aged endurance athletes within 12 weeks, as evidenced by the
increased oxygen uptake, power, lactate threshold-to-power output,
lactate threshold-to-oxygen uptake, and quicker recovery times
observed when compared with the placebo group. Furthermore,
arterial flexibility, assessed by PWV, improved more in the Kyolic
aged garlic group compared with the placebo group. These results
are in line with previous animal (27-29)
and human studies (30-32),
whereby garlic supplements ingested for an acute or sub-chronic
period significantly ameliorated physical fatigue, increased
exercise tolerance and increased oxygen uptake, resulting in
overall higher aerobic capacity.
A number of human studies involving 10(30) or 18(31) male athletes investigated the acute
effect of garlic on aerobic capacity and found that 900 mg of
garlic powder ingested 3 or 5 h, respectively, before high
intensity exercise significantly improved the VO2max. A
6 week trial testing the effect of garlic oil on cardiac
performance and exercise tolerance in 30 patients with coronary
artery disease reported that garlic oil significantly reduced heart
rate at peak exercise, leading to improved exercise tolerance
(32).
In addition, the present study demonstrated that
Kyolic aged garlic extract improved the cardiovascular risk
proteomic biomarker profile compared with the placebo group, which
was in line with previously published results (35,38).
Lower concentrations of a panel of 25 urinary polypeptides/protein
biomarkers (35) have been
associated with reduced cardiovascular risk, such as heart attack
and stroke, independent of age and sex in asymptomatic patients
(36,37). The present study demonstrated that
Kyolic aged garlic extract was effective at significantly lowering
the concentrations of a subset of the aforementioned biomarkers
compared with the placebo group after 3 months of supplementation.
Therefore, the present study adds to previous research
demonstrating that diet and exercise are effective in improving the
proteomic cardiovascular risk profile. A study involving 69 healthy
participants showed that olive oil ingested daily over 6 weeks
significantly improved certain cardiovascular risk proteomic
biomarkers compared with the baseline (38). Additionally, exercise reduced the
cardiovascular risk proteomic profile in a cohort of 88 patients
with coronary artery disease, while there was no change in the
inactive patients (35).
The present study had several strengths, involving a
reasonable sample size of 75 middle-aged endurance athletes
completing the trial with high compliance and having access to
specialized equipment and the expertise of professional exercise
physiologists for objective and accurate measures of the primary
outcome variables related to aerobic fitness. Furthermore, the
findings of the effect of Kyolic aged garlic extract compared with
placebo were comparable in both athletically diverse cohorts, while
more pronounced within in the fitter cohort 1, suggesting that
Kyolic aged garlic extract may be effective in improving aerobic
capacity independent of baseline aerobic fitness.
However, the athletic disparity between the two
cohorts limited the opportunity for a meaningful comparative
dose-response analysis. The more athletic cohort 1 (low dose Kyolic
aged garlic extract) exercised a mean of 1.5 hours/day at a
moderate to high intensity and had significantly greater aerobic
fitness at baseline, compared with cohort 2 (high dose Kyolic aged
garlic extract) who exercised a mean of 45 min/day. The differences
in aerobic fitness between the cohorts at baseline were
significantly greater when compared with any changes caused by the
treatment intervention within each cohort, confounding any
meaningful comparative analysis by dose. Future studies could plan
recruitment for both Kyolic aged garlic extract doses within a
shorter time period, perhaps using a block randomization of
alternating 10 low dose/10 high dose interventions, which increases
the likelihood of drawing participants who have a similar level of
athleticism. A further limitation in this study concerned the
assessment of arterial stiffness, as PWV was measured using
different devices in each cohort. Due to unforeseen circumstances,
the SphygmoCor tonometer (11)
used to measure PWV in cohort 1 was no longer serviced in Australia
during the cohort 2 study period, therefore, the Mobil-O-graph
device (12) was used for cohort
2. While both devices have been validated against the gold standard
tonometry for central blood pressure (14) and pulse wave analysis (42), PWV measurements taken with
different devices have been shown not to be directly comparable
(43). Therefore, the present
analysis could not combine the measurements from both cohorts,
reducing the statistical power due to the smaller sample size. This
also impacted the hypothesis that more flexible arteries, assessed
by PWV, would improve aerobic fitness due to increased oxygen
uptake, as this could not be measured. A further limitation was the
assessment of recovery time in days by a simple questionnaire which
was administered on a monthly basis. To improve precision and
reduce subjectivity, future studies could use an online daily or
weekly diary assessing the recovery in hours rather than days (e.g.
36 hours vs. 1 or 2 days). Additionally, a combined proteomic
analysis of both cohorts was confounded by the baseline differences
in polypeptide levels between the cohorts. In cohort 1, 45% of the
polypeptides tested were significantly reduced in the Kyolic aged
garlic extract group compared with the placebo, whereas 13% of the
polypeptides were significantly reduced in the cohort 2. Further
research should be conducted to explore the factors that caused the
difference in proteomic and metabolomic profiles at baseline in
endurance athletes with different aerobic fitness levels.
Furthermore, longer-term studies are needed to explore the
sustained effect of Kyolic aged garlic extract on aerobic fitness
and associated cardiovascular morbidity and mortality.
The present study demonstrated that Kyolic aged
garlic extract significantly improved aerobic fitness within 12
weeks in middle-aged endurance athletes, as evidenced by increased
VO2max, increased lactate threshold, quicker recovery
and improved cardiovascular risk proteomic profile. Furthermore,
these findings are in line with previous research providing
evidence that Kyolic aged garlic extract reduces arterial
stiffness, a process that occurs with age. An increase in arterial
flexibility is associated with slower blood flow, which in turn
improves oxygen uptake, reduces lactate production and muscle
soreness linked to recovery and improves overall aerobic fitness.
While previous research with Kyolic aged garlic extract focused on
comparatively ‘unhealthy’ populations with cardiovascular risk
factors such as hypertension, the present study provided evidence
for the use of Kyolic aged garlic extract to benefit a ‘healthier’
middle-aged population.
Supplementary Material
Aerobic capacity of
cohortsa,b.
Acknowledgements
The authors are grateful to the exercise
physiologists from Mets Performance who conducted the aerobic
fitness testing, including VO2max testing and lactate
analysis of the study participants using a cycle ergometer. The
abstract was presented at the 2024 International Garlic Symposium
in Munich, Germany (45). The
authors would like to acknowledge Olympian cyclist Kathy Watt, OAM,
who assisted with recruitment of the endurance cyclists in the
present study.
Funding
Funding: KR received a travel sponsorship from Wakunaga of
America Co., Ltd. to attend the 2024 International Garlic Symposium
in Munich, Germany. The present trial was supported by a grant from
Wakunaga of America Co., Ltd. who supplied trial capsules and
provided funding for the costs of tests, research assistance and
open access publication. The sponsor was not involved in study
design, data collection, analysis or preparation of the
manuscript.
Availability of data and materials
The data generated in the present study may be found
in the Commonwealth Scientific and Industrial Research Organisation
Data Access portal at the following URL: https://data.csiro.au/collection/csiro:64384.
Authors' contributions
KR and AS conceptualised the study, KR acquired
funding and oversaw data collection and data entry conducted by YP.
DB undertook proteomics data analysis and uploaded the raw data to
a public database. KR undertook data analysis and prepared the
manuscript with contributions from co-authors. YP and KR confirm
the authenticity of all the raw data, with DB's input of raw
proteomics data. All authors approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the National
Institute of Integrative Medicine Human Research Ethics Committee
EC00436 (approval no. 0062N_2020; Melbourne, Australia) and written
informed consent was obtained from each individual for
participation in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ried K and Fakler P: Potential of garlic
(Allium sativum) in lowering high blood pressure: mechanisms of
action and clinical relevance. Integr Blood Press Control. 7:71–82.
2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ried K, Frank OR and Stocks NP: Aged
garlic extract lowers blood pressure in patients with treated but
uncontrolled hypertension: A randomised controlled trial.
Maturitas. 67:144–150. 2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ried K, Frank OR and Stocks NP: Aged
garlic extract reduces blood pressure in hypertensives: a
dose-response trial. Eur J Clin Nutr. 67:64–70. 2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ried K, Travica N and Sali A: The effect
of aged garlic extract on blood pressure and other cardiovascular
risk factors in uncontrolled hypertensives: the AGE at Heart trial.
Integr Blood Press Control. 9:9–21. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ried K, Travica N and Sali A: The effect
of Kyolic aged garlic extract on gut microbiota, inflammation and
cardiovascular health in hypertensives: The GarGIC trial. Frontiers
in Nutrition. 5(122)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Laurent S, Cockcroft J, Van Bortel L,
Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C,
Wilkinson I and Struijker-Boudier H: European Network for
Non-invasive Investigation of Large Arteries. Expert consensus
document on arterial stiffness: methodological issues and clinical
applications. Eur Heart J. 27:2588–2605. 2006.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Zieman SJ, Melenovsky V and Kass DA:
Mechanisms, pathophysiology, and therapy of arterial stiffness.
Arterioscler Thromb Vasc Biol. 25:932–943. 2005.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Nunan D, Fleming S, Hametner B and
Wassertheurer S: Performance of pulse wave velocity measured using
a brachial cuff in a community setting. Blood Pressure Monitoring.
19:315–319. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Lee HY and Oh BH: Aging and arterial
stiffness. Circ J. 74:2257–2262. 2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Luft FC: Molecular mechanisms of arterial
stiffness: New insights. J Am Soc Hypertens. 6:436–438.
2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
SphygmoCor XCEL, Cardiex USA. Available
from: https://cardiex.com/products/sphygmocor-xcel/.
|
|
12
|
Mobil-O-Graph IEM, Germany. Available
from: https://www.iem.de/en_US/mobil-o-graph.
|
|
13
|
Nunan D, Wassertheurer S, Lasserson D,
Hametner B, Fleming S, Ward A and Heneghan C: Assessment of central
haemomodynamics from a brachial cuff in a community setting. BMC
Cardiovasc Disord. 12(48)2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Weiss W, Gohlisch C, Harsch-Gladisch C,
Tölle M, Zidek W and van der Giet M: Oscillometric estimation of
central blood pressure: validation of the Mobil-O-Graph in
comparison with the SphygmoCor device. Blood Press Monit.
17:128–131. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Naci H and Ioannidis JP: Comparative
effectiveness of exercise and drug interventions on mortality
outcomes: Metaepidemiological study. Br J Sports Med. 49:1414–1422.
2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Fagard RH: Exercise therapy in
hypertensive cardiovascular disease. Prog Cardiovasc Dis.
53:404–411. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Myers J, Gullestad L, Bellin D, Ross H,
Vagelos R and Fowler M: Physical activity patterns and exercise
performance in cardiac transplant recipients. J Cardiopulm Rehabil.
23:100–106. 2003.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bassett DR and Howley ET: Limiting factors
for maximum oxygen uptake and determinants of endurance
performance. Med Sci Sports Exerc. 32:70–84. 2000.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Tanaka H and Seals DR: Endurance exercise
performance in Masters athletes: age associated changes and
underlying physiological mechanisms. J Physiol. 586:55–63.
2008.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Maffulli N, Testa V and Capasso G:
Anaerobic threshold determination in master endurance runners. J
Sports Med Phys Fitness. 34:242–249. 1994.PubMed/NCBI
|
|
21
|
Faude O, Kindermann W and Meyer T: Lactate
threshold concepts. Sports Med. 39:469–490. 2009.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Abe D, Yoshida T, Ueoka H, Sugiyama K and
Fukuoka Y: Relationship between perceived exertion and blood
lactate concentrations during incremental running test in young
females. BMC Sports Sci Med Rehabil. 7(5)2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
McCormack HM, David JdL and Sheather S:
Clinical applications of visual analogue scales: A critical review.
Psychol Med. 18:1007–1019. 1988.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Vaitkevicius PV, Fleg JL, Engel JH,
O'Connor FC, Wright JG, Lakatta LE, Yin FC and Lakatta EG: Effects
of age and aerobic capacity on arterial stiffness in healthy
adults. Circulation. 88:1456–1462. 1993.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Tanaka H and Seals DR: Invited review:
Dynamic exercise performance in masters athletes: Insight into the
effects of primary human aging on physiological functional
capacity. J Applied Physiol. 95:2152–2162. 2003.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Proctor DN and Joyner MJ: Skeletal muscle
mass and the reduction of VO2max max in trained older
subjects. J Appl Physiol. 82:1411–1415. 1997.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Morihara N, Ushijima M, Kashimoto N,
Sumioka I, Nishihama T, Hayama M and Takeda H: Aged garlic extract
ameliorates physical fatigue. Biol Pharm Bull. 29:962–966.
2006.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Morihara N, Nishihama T, Ushijima M, Ide
N, Takeda H and Hayama M: Garlic as an anti-fatigue agent. Mol Nutr
Food Res. 51:1329–1334. 2007.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ushijima M, Sumioka I, Kakimoto M,
Yokoyama K, Uda N, Matsuura H, Kyo E, Suzuki A, Kasuga S, Itakura
Y, et al: Effect of garlic and garlic preparations on physiological
and psychological stress in mice. Phytotherapy Res. 11:226–230.
1997.
|
|
30
|
Ince D, Soenmez G and Ince M: Effects of
garlic on aerobic performance. Turkish J Med Sci. 30:557–561.
2000.
|
|
31
|
Womack C, Lawton D, Redmond L, Todd M and
Hargens T: The effects of acute garlic supplementation on the
fibrinolytic and vasoreactive response to exercise. J Int Soc
Sports Nutr. 12(23)2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Verma SK, Rajeevan V, Jain P and Bordia A:
Effect of garlic (Allium sativum) oil on exercise tolerance in
patients with coronary artery disease. Indian J Physiol Pharmacol.
49:115–118. 2005.PubMed/NCBI
|
|
33
|
The-Age: Charles Erasmus, a ‘gentle soul’,
loses life just metres from Big Bay Swim finish line. https://www.theage.com.au/national/victoria/charles-erasmus-a-gentle-soul-loses-life-just-metres-from-big-bay-swim-finish-line-20150223-13m3u0.html.
|
|
34
|
ABC-News: Man, 65, dies during Lorne's
Pier to Pub open water swim, Victoria. https://www.abc.net.au/news/2019-01-12/man-drowns-during-pier-to-pub-open-water-swim-race/10711120.
|
|
35
|
Zimmerli LU, Schiffer E, Zürbig P, Good
DM, Kellmann M, Mouls L, Pitt AR, Coon JJ, Schmieder RE, Peter KH,
et al: Urinary proteomic biomarkers in coronary artery disease. Mol
Cell Proteomics. 7:290–298. 2008.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Brown CE, McCarthy NS, Hughes AD, Sever P,
Stalmach A, Mullen W, Dominiczak AF, Sattar N, Mischak H, Thom S,
et al: Urinary proteomic biomarkers to predict cardiovascular
events. Proteomics Clin Appl. 9:610–617. 2015.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Delles C, Schiffer E, von Zur Muhlen C,
Peter K, Rossing P, Parving HH, Dymott JA, Neisius U, Zimmerli LU,
et al: Urinary proteomic diagnosis of coronary artery disease:
identification and clinical validation in 623 individuals. J
Hypertens. 28:2316–2322. 2010.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Silva S, Bronze MR, Figueira ME, Siwy J,
Mischak H, Combet E and Mullen W: Impact of a 6-wk olive oil
supplementation in healthy adults on urinary proteomic biomarkers
of coronary artery disease, chronic kidney disease, and diabetes
(types 1 and 2): A randomized, parallel, controlled, double-blind
study. Am J Clin Nutr. 101:44–54. 2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
American-Heart-Association. Target Heart
Rate Charts 2024. Available from: https://www.heart.org/en/healthy-living/fitness/fitness-basics/target-heart-rates.
|
|
40
|
Craig CL, Marshall AL, Sjöström M, Bauman
AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF
and Oja P: International physical activity questionnaire:
12-country reliability and validity. Med Sci Sports Exerc.
35:1381–1395. 2003.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Salvi P, Scalise F, Rovina M, Moretti F,
Salvi L, Grillo A, Gao L, Baldi C, Faini A, Furlanis G, et al:
Noninvasive estimation of aortic stiffness through different
approaches: comparison with intra-aortic recordings. Hypertension.
74:117–129. 2019.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Wassertheurer S, Kropf J, Weber T, Van der
Giet M, Baulmann J, Ammer M, Hametner B, Mayer CC, Eber B and
Magometschnigg D: A new oscillometric method for pulse wave
analysis: Comparison with a common tonometric method. J Hum
Hypertens. 24:498–504. 2010.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Kolkenbeck-Ruh A, Soepnel LM, Kim AW,
Naidoo S, Smith W, Davies J and Ware LJ: Pulse wave velocity in
South African women and children: comparison between the
Mobil-O-Graph and SphygmoCor XCEL devices. J Hypertens. 40:65–75.
2022.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Blood Pressure Monitor Omron HEM-907,
JA-Davey-Pty-Ltd Australia. Available from: https://www.omronhealthcare-ap.com/au/product/93-hem-907.
|
|
45
|
Abstract 0-13, International Garlic
Symposium. Frontiers of garlic research in health promotion and
disease prevention. Munich, Germany, 26-28 April 2024. https://garlicsymposium2024.com.
|