Introduction
Pulmonary metastasectomy (PM) is currently the
standard therapy for metastatic osteosarcoma. The evidence
supporting the benefit from this surgical intervention is based on
retrospective data reporting encouraging 5-year overall survival
(OS) rates of 20–40% and the possibility of cure with this surgical
approach. By contrast, death almost always ensues when such
patients are treated with systemic chemotherapy alone (1–5).
In the absence of randomized data, retrospective
studies have been mainly focused on the analysis of prognostic
factors in an attempt to identify selection criteria for the
optimal operative candidates (1–5).
However, there remains controversy regarding the optimal population
that are candidates for PM. Therefore, we performed this
retrospective study to investigate factors that may predict
long-term survival in our patient population. As PM is aimed at
complete resection of the metastases, we aimed to investigate
factors associated with survival in a population achieving complete
remission (CR) following surgery.
Materials and methods
Eligible patients and data
extraction
Following acquisition of Institutional Review Board
approval, we reviewed the medical records of patients with
osteosarcoma to identify patients who had undergone PM between
January, 2000 and August, 2013 at King Hussein Cancer Center,
Amman, Jordan. Patients with gross residual disease following PM
(i.e., patients who did not achieve complete surgical remission)
were excluded.
The following data were extracted from medical
records and filled on data collection sheets: Age at detection of
pulmonary metastasis, gender, histological osteosarcoma subtype,
mode of pulmonary metastasis (at presentation or at recurrence),
timing of pulmonary metastasis (at diagnosis, during neoadjuvant or
adjuvant chemotherapy, or following completion of chemotherapy) and
the relapse-free interval (RFI), defined as the interval from the
resection of the primary tumor until detection of lung metastasis.
The RFI was considered to be 0 for patients who presented with
primary metastatic disease at initial diagnosis.
In addition, we extracted data on the
characteristics of metastatic nodules, therapeutic details,
including any peri-operative chemotherapy, sites of recurrence and
data on repeated PM.
The common practice at our institution is to
initiate multi-agent chemotherapy, including cisplatin and
doxorubicin or ifosfamide-containing regimens, prior to PM and to
continue such therapy in the adjuvant setting following
surgery.
Definitions
We defined resectability as the ability to remove
all metastatic nodules without gross residual disease according to
the thoracic surgeons' assessment at our institution; this
definition also requires a controlled/controllable primary tumor
and absence of extrapulmonary metastatic sites at the time of
assessment.
We defined CR as absence of any evidence of gross
residual disease following PM, irrespective of the status of the
microscopic resection margins.
Additionally, we defined OS as the interval from the
resection of lung metastasis until the last follow-up or death and
disease-free survival (DFS) as the time period following resection
of pulmonary metastases during which a patient remained alive with
no signs of disease.
Statistical analysis
The Kaplan-Meier survival analysis was applied to
assess survival. Demographic and disease-related factors were
evaluated with the log-rank test for possible effect on OS;
comparisons with P<0.05 were considered to be statistically
significant. A multivariate analysis using the backward stepwise
Cox regression model was performed on statistically significant
variables identified in the univariate analysis. All the
statistical analyses were performed using SPSS software, version 16
(SPSS Inc, Chicago, IL, USA).
Results
Patient characteristics
Between January, 2000 and August, 2013, 135 patients
with osteosarcoma of the extremity were treated and followed up at
our institution. A total of 62 patients had pulmonary metastasis,
either at initial presentation or at recurrence. Of the patients
with pulmonary metastasis, 28 underwent PM; 3 of those patients had
gross residual disease following surgery and were excluded (2 with
residual unresectable chest wall and pleural metastasis and 1 due
to refusal of a planned above-knee amputation to treat the primary
tumor). The 25 patients who were free of gross residual disease
following PM were included in this analysis (5 patients with
metastasis at diagnosis and 20 patients with metastasis at the time
of relapse).
The sites of the primary tumors were the femur in 14
cases, the tibia in 7 cases and the humerous in 4 cases. Data on
pathological necrosis of the primary tumor were available for 23 of
the patients, of whom 6 had necrosis ≥90% and 17 had necrosis
<90%.
The median RFI for patients who presented with
metastasis at relapse was 17.6 months (range, 4.5–63 months).
In the 5 patients with metastasis at diagnosis, the
primary tumor and the pulmonary metastases were completely resected
in staged procedures following chemotherapy, which was initiated in
a neoadjuvant setting and continued as adjuvant therapy following
surgery; all the patients underwent resection of the primary tumor
prior to PM. In the 20 patients with metastasis at relapse,
locoregional recurrences were observed in 4 patients and were
completely resected prior to PM. Of the 20 patients with metastasis
at relapse, 15 received peri-operative chemotherapy.
A total of 14 patients had unilateral pulmonary
metastatic disease, whereas 11 underwent resection of bilateral
metastatic pulmonary nodules through staged thoracotomies. As
regards the number of surgeries, the staged thoracotomy for
bilateral pulmonary nodules was considered as one PM surgery.
A total of 10 patients underwent resection of
solitary metastatic nodules, 6 patients underwent resection of 2–5
nodules and 7 patients underwent resection of >5 nodules (range,
6–21 nodules) during the first PM. A total of 8 patients required
repeated PM (range, 2–3 metastasectomies). Apart from 1 patient who
required a lobectomy, all the other patients underwent resection of
the pulmonary nodules through wedge resections during the first PM.
In 5 patients, at least one of the nodules was resected with a
positive margin (R1 resection) in the first PM. Furthermore, 5
patients had detectable tumor cells reaching the visceral pleural
surface in at least one of the resected nodules detected at
pathological examination of the resected specimen. There was no
reported mortality within 1 month of the first PM.
Recurrence and survival outcomes
Following PM, 8 patients remained free of disease
and 17 had documented recurrences at a mean interval of 8.7 months
(range, 3–35 months) following the first PM. The first recurrence
was limited to the lungs in 11 patients, 8 of whom had repeated
PMs, as mentioned above. The remaining 6 patients had lung
recurrence in addition to at least one extrapulmonary site as their
first presentation of recurrent disease; bone metastasis occurred
in 4 of those patients. None of the patients had extrapulmonary
metastasis without lung recurrence. The 5-year RFS for the entire
cohort was 21%.
The median follow-up for the patients following PM
was 25 months (range, 2–62 months). At the time of this analysis,
15 patients had succumbed to the disease, whereas none of the
patients had died from other causes. The OS rate was 30% at 5 years
(median survival time, 25 months).
The results of the univariate analysis for the
effect of factors of interest on OS are summarized in Table I.
 | Table IResults of univariate analysis. |
Table I
Results of univariate analysis.
| Factors | Patient no.
(%)(n=25) | Median OS
(months) | 5-year OS (%) | Log-rank P-value |
|---|
| Age (years) | | | | |
| <20 | 10 (40) | Unreached | 58 | 0.064 |
| ≥20 | 15 | (60) | 23.2 | 14 |
| Gender | | | | |
| Male | 18 (72) | 25 | 21.6 | 0.35 |
|
Female | 7 (28) | 33.3 | 43 | |
| Histological
subtype | | | | |
|
Chondroblastic | 8 (32) | 13.4 | 13 | 0.015 |
|
Other | 17 (68) | 33.3 | 37 | |
| Tumor necrosis | | | | |
|
<90% | 17 (68) | 23.2 | 8 | 0.011 |
| ≥90% | 6 (24) | Unreached | 69 | 69 |
| ND | 2 (8) | | | |
| RFI (months) | | | | |
|
<12 | 11 (44) | 24.6 | 30 | 0.74 |
| ≥12 | 14 (56) | 29 | 27 | |
| Peri-PM
chemotherapy | | | | |
| Yes | 20(80) | Unreached | 63 | 0.13 |
| No | 5 (20) | 24.6 | 19 | |
| Number of
nodules | | | | |
|
<3 | 12 (48) | 25 | 27 | 0.85 |
| ≥3 | 13 (52) | 24.8 | 29 | |
| Laterality | | | | |
|
Unilateral | 13 (52) | 25 | 33 | 0.58 |
|
Bilateral | 12 (48) | 29 | 26 |
| Size (cm) | | | | |
|
<3 | 11 (44) | 32 | 36 | 0.91 |
| ≥3 | 11 (44) | 24 | 30 | |
| ND | 3 (12) | | | |
| Metastasis during
CTX | | | | |
| Yes | 3 (12) | 11.0 | 0 | <0.0001 |
| No | 22 (88) | 29.0 | 33 | |
| Detection of
metastasis | | | | |
| At
initial diagnosis | 5 (20) | 32.0 | 40 | 0.43 |
| At
recurrence | 20 (80) | 24.8 | 27 | |
| Status of resection
margins | | | | |
| R0 | 19 (76) | 25 | 38 | 0.36 |
| R1 | 6 (24) | 29 | 0 | |
| Visceral pleural
involvement | | | | |
|
Yes | 5 (20) | 13.1 | 0 | 0.007 |
| No | 20 (80) | 32 | 39 | |
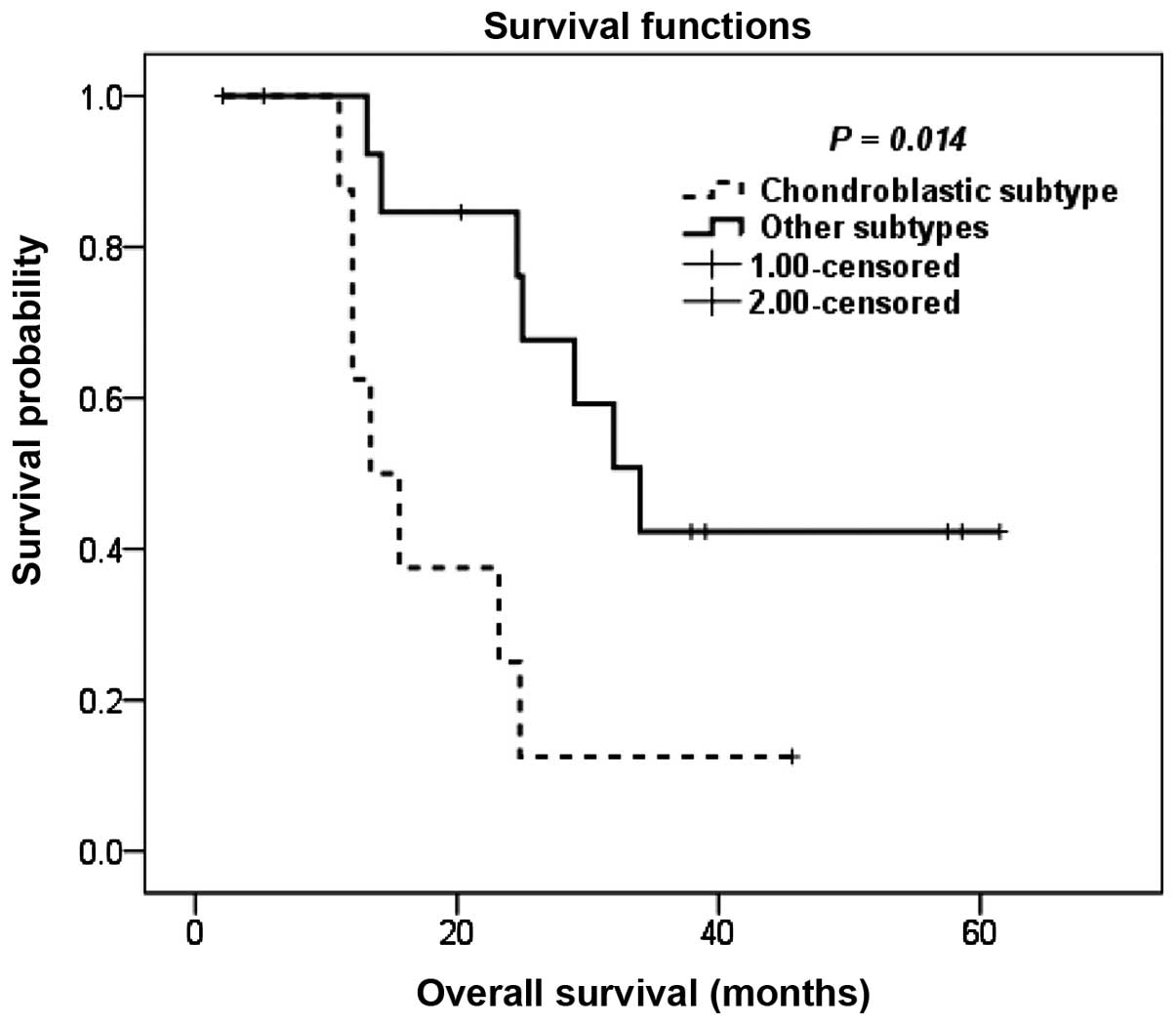
Patients with the chondroblastic subtype exhibited
inferior OS compared to patients with other histological subtypes,
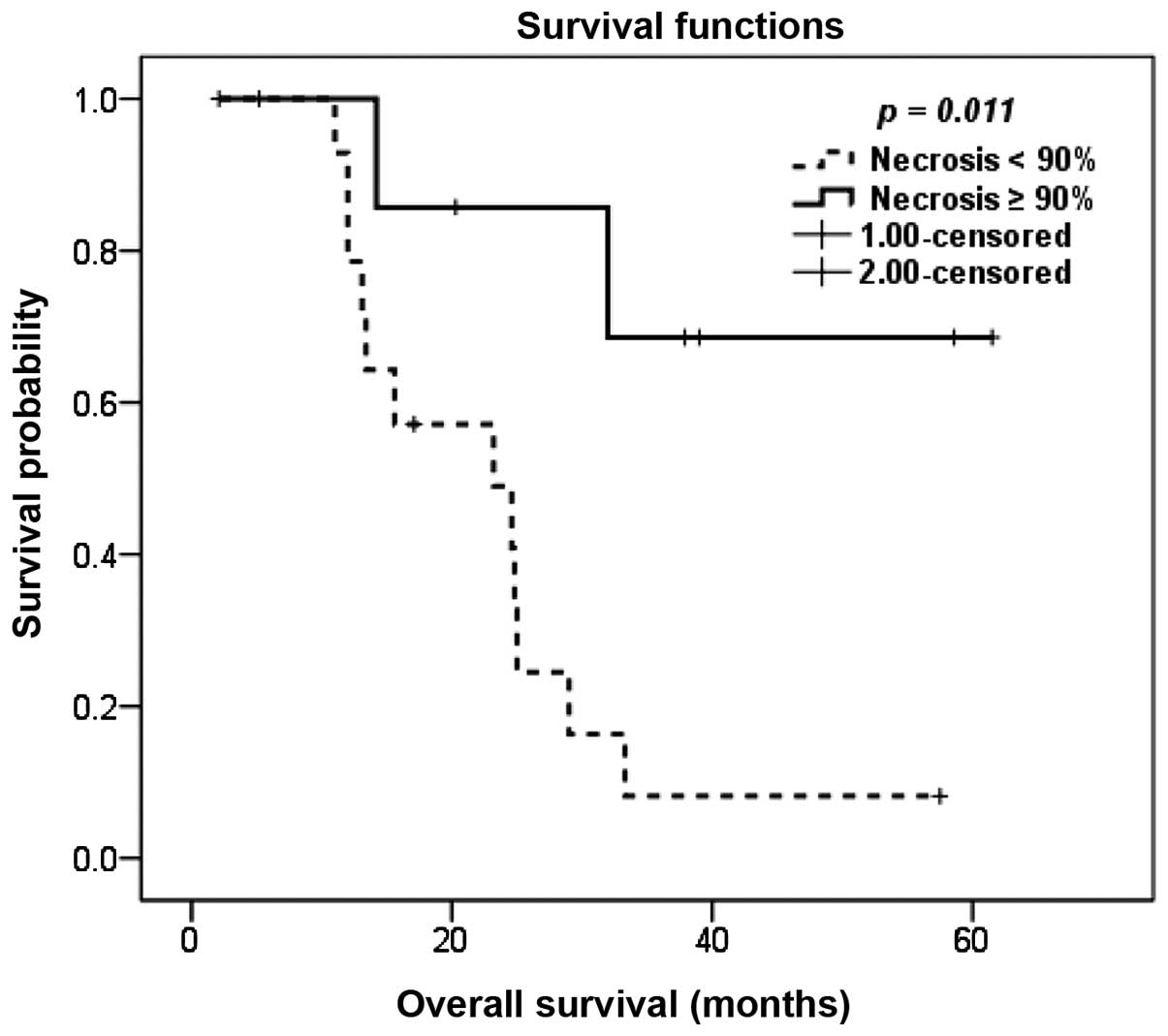
with a 5-year OS of 13 and 37%, respectively (P=0.014; Fig. 1). The degree of pathological
necrosis in the primary tumor following neoadjuvant chemotherapy
also exerted a significant effect on OS, with a 5-year OS of 8 and
69% for tumor necrosis of <90 and ≥90%, respectively (P=0.011;
Fig. 2).
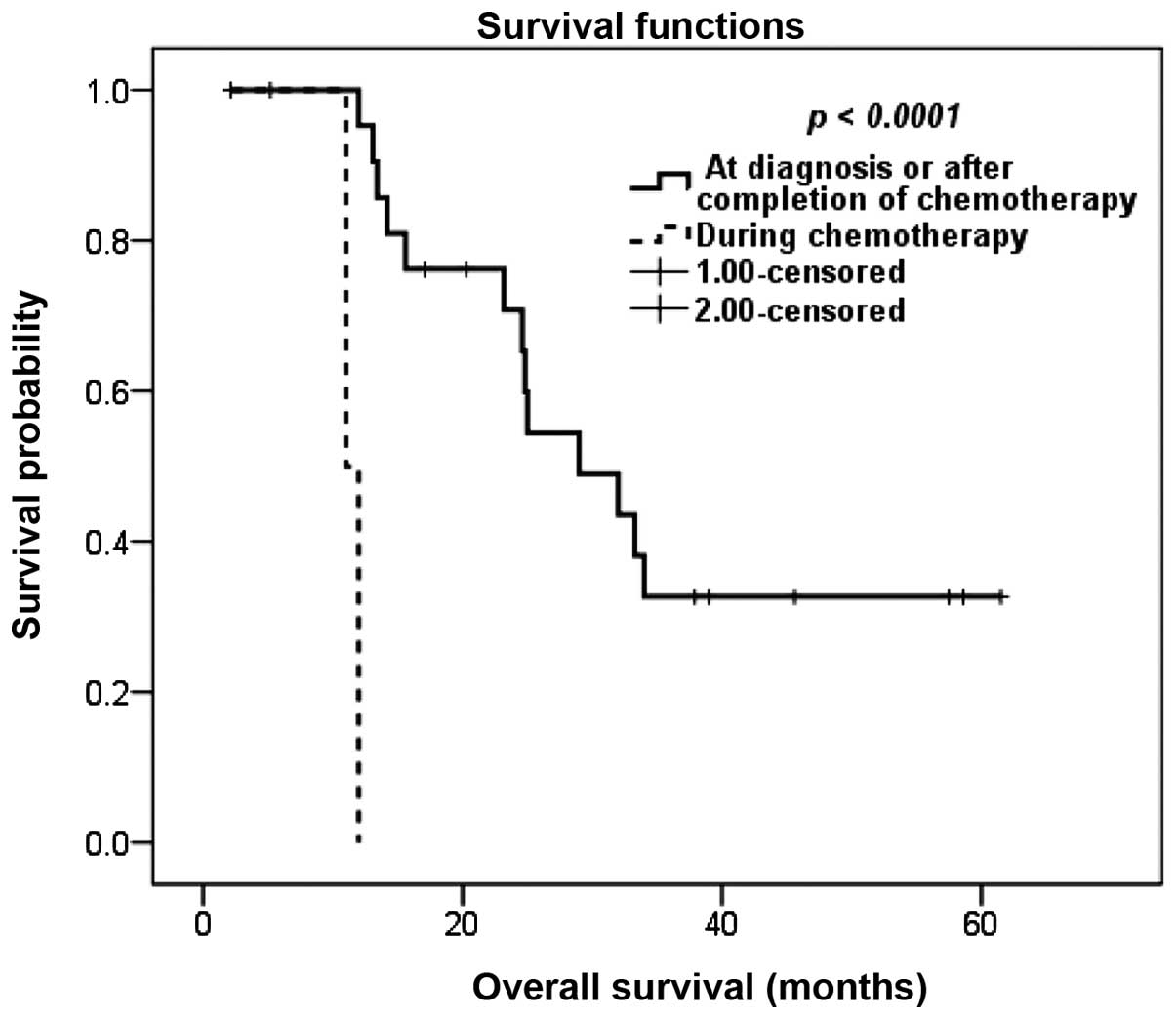
Although the RFI did not affect OS, we observed a
significant association between the timing of detection of
metastasis in relation to chemotherapy and survival. Patients with
metastasis detected during neoadjuvant or adjuvant chemotherapy
fared significantly worse compared to patients whose metastases
were detected at initial diagnosis or following completion of
chemotherapy; the 5-year OS rate for the latter group was 33%,
whereas patients with metastasis detected during neoadjuvant or
adjuvant chemotherapy exhibited a 1-year OS of 0% (P<0.0001;
Fig. 3).
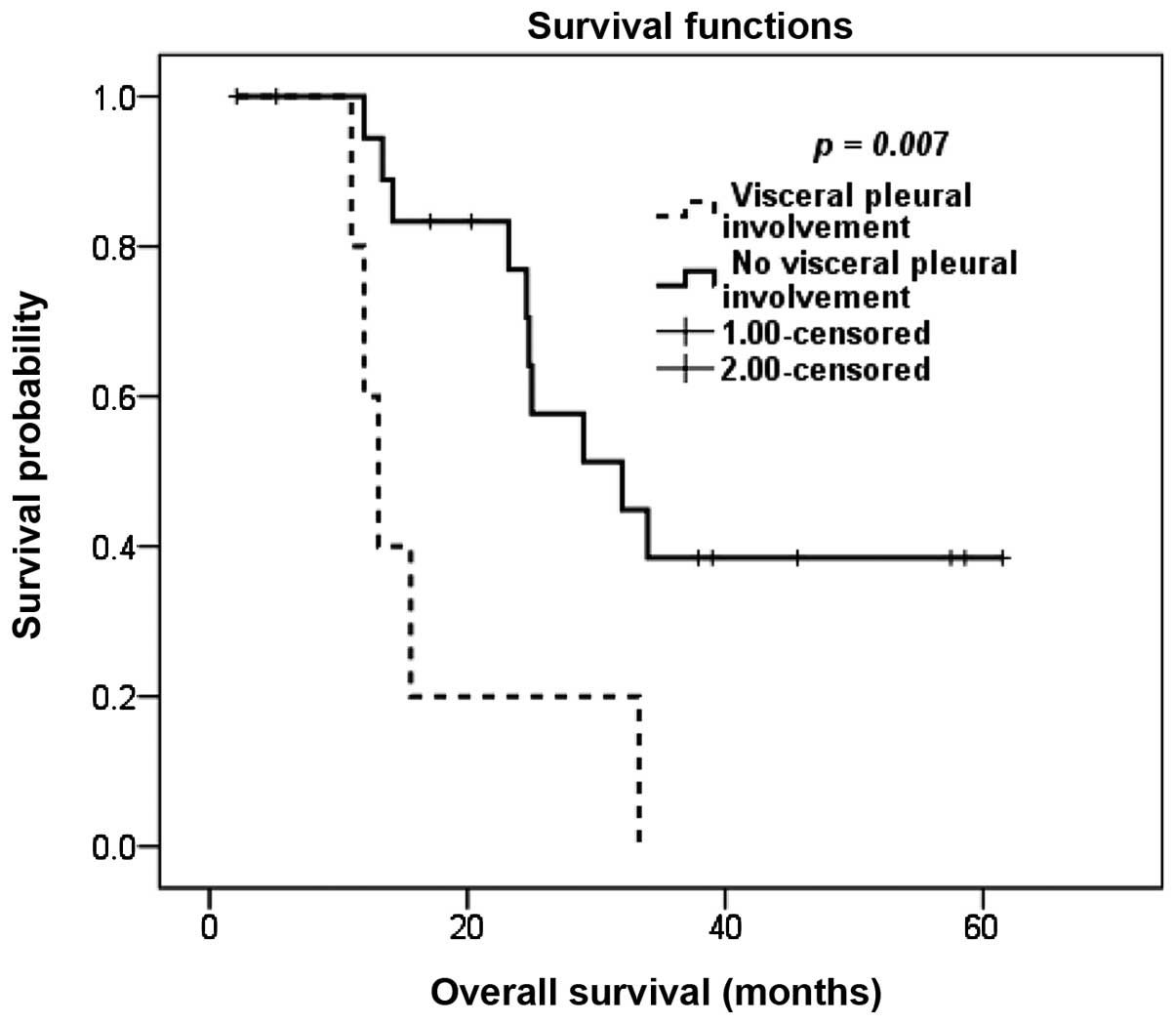
Based on our analysis, patients with positive
resection margins in any of the resected nodules did not have
statistically significant differences in OS compared to patients
with negative resection margins, although there was a
non-significant tendency towards an inferior OS for patients with
positive margins. However, the detection of malignant cells at the
visceral pleural surface of any of the resected pulmonary nodules
was correlated with inferior survival; the 3-year OS rate was 0%
for patients with visceral pleural involvement and the 5-year OS
rate was 39% for patients with no visceral pleural involvement
(P=0.007; Fig. 4).
In the multivariate analysis, the chondroblastic
subtype was the sole independent prognostic factor (P=0.044),
whereas the effect of metastasis detected during chemotherapy on
survival approached statistical significance (P=0.051; Table II).
| Table IIResults of multivariate analysis for
factors affecting overall survival. |
Table II
Results of multivariate analysis for
factors affecting overall survival.
| Clinical
variables | Hazard ratio | 95% CI | P-value |
|---|
| Histological
subtype | | | |
|
Chondroblastic | 4.6 | 1.0–21.3.. | 0.044 |
| Other
subtypes | 1 | | |
| Extent of primary
tumor necrosis | | | |
|
<90% | 3.80 | 0.7320.0 | 0.092 |
|
≥90% | 1 | | |
| Detection of
metastasis | | | |
| During
chemotherapy | 10.8 | 0.93126.4 | 0.051 |
| At
diagnosis or after completion of chemotherapy | 1 | | |
| Visceral pleural
involvement | | | |
|
Present | 1.3 | 0.315.26 | 0.730. |
|
Absent | 1 | | |
Finally, we assessed the effect of a number of
prognostic factors that we identified in the univariate analysis on
OS outcomes and observed significant differences in survival
between three groups of patients: The median OS for patients with
0–1 risk factors, patients with 2 risk factors and patients with ≥3
risk factors was unreached, 23.2 months and 12.0 months,
respectively (P<0.0001; data not shown).
Discussion
Approximately 30–40% of patients with initially
non-metastatic osteosarcoma eventually develop lung metastasis
(6–8) and almost half of these relapses
become evident within 18 months of continuation of chemotherapy
(9,10). Furthermore, 10–20% of osteosarcoma
patients present with metastatic disease at initial diagnosis
(11,12).
An important characteristic of metastasis in
osteosarcoma that makes PM an attractive therapeutic option is the
propensity for isolated pulmonary metastasis, which is the most
common pattern of systemic recurrence, contributing to 65–80% of
relapses (10,13). Furthermore, isolated pulmonary
metastasis is the most common pattern of metastasis in patients
with primary metastatic disease (12).
The prognostic factors for survival following PM in
osteosarcoma are controversial; therefore, the selection of optimal
candidates for this type of surgery is a subject under debate.
Although the achievement of CR is the most consistently identified
prognostic factor (1,10,12–16),
contradicting data have been reported regarding the significance of
the other factors.
Data from literature have been inconsistent
regarding the effect of the number of pulmonary nodules on
post-metastasectomy survival. Certain studies suggested that the
number of nodules adds prognostic information (1,5,7,8,17),
whereas other studies failed to confirm a significant association
between the number of nodules and survival (18,19).
In our study, we did not identify any prognostic correlation
between the number of resected nodules and survival, suggesting
that, when all the nodules are completely resected, their number
loses its significance as a prognostic factor.
There is evidence in the literature that the timing
of pulmonary metastasis is associated with prognosis. Certain
studies demonstrated that the time interval from the resection of
the primary tumor until the detection of pulmonary metastasis
affects survival (8,19), whereas other studies suggested that
the timing in relation to chemotherapy is significant in terms of
prognosis (1,2). In our study, we did not identify any
correlation between the RFI and survival. Furthermore, we did not
observe any difference in survival between patients with metastasis
at diagnosis and those with metastasis at recurrence; however,
patients whose metastases were detected during treatment with
neoadjuvant or adjuvant chemotherapy fared significantly worse
following PM compared to those whose metastases were detected at
initial diagnosis or following completion of chemotherapy. Similar
to our data, other studies demonstrated that the timing of
metastasis in relation to chemotherapy correlates with survival
(1,2).
Progression on adjuvant chemotherapy may be a
confounding factor that leads to an apparent correlation between
RFI of <1 year and OS in certain studies. It may be hypothesized
that the subgroup of patients who relapsed within 1 year of
definitive therapy of the primary tumor includes a proportion of
patients who developed disease progression during adjuvant
chemotherapy and, as such, the survival of the entire subgroup may
appear worse, as it includes a subpopulation of patients whose
disease is refractory to chemotherapy.
Consistent with our data, Harting et al
demonstrated a correlation between the degree of necrosis in the
primary tumor following neoadjuvant chemotherapy and
post-metastasectomy survival (19). It was demonstrated that the extent
of necrosis in the primary tumor was also correlated with the
survival of patients who did not achieve surgical remission
(12). By contrast, certain
studies failed to identify any correlation between
post-metastasectomy survival and the extent of necrosis in the
primary tumor (20) or in the
resected pulmonary metastases (7).
There is currently paucity of data in the literature
regarding the effect of histological subtype on survival following
PM in osteosarcoma, as the majority of the studies do not include
this factor in their analysis. To the best of our knowledge, our
study is the first to suggest an association between the
chondroblastic subtype and survival following PM. In addition, the
prognostic effect of pathological identification of visceral
pleural involvement in any of the resected nodules on patient
survival has not been previously reported for patients with
metastatic osteosarcoma. However, until additional confirmation of
these prognostic factors in further large-scale studies, the effect
of those factors on survival must be interpreted with caution due
to the limited number of patients in our series.
The contribution of perioperative chemotherapy to
the improved survival of patients with metastatic osteosarcoma who
achieved CR following surgery remains unclear. Although there have
been data demonstrating that chemotherapy is associated with
improved survival in patients with relapsed osteosarcoma who have
unresectable metastatic disease, several studies reported that
administering chemotherapy does not result in an additional
improvement in the survival of patients with metastatic
ostrosarcoma who achieve complete surgical remission (13,15).
However, a subanalysis on the effect of perioperative chemotherapy
on the survival of patients who achieved complete surgical
remission demonstrated a survival advantage for the subgroup with
>3 lung nodules (15).
Therefore, some investigators suggest withholding perioperative
chemotherapy in patients with disease characteristics suggesting
less aggressive tumor biology, such as patients with solitary
nodules and prolonged RFI.
The main limitations to our study were the small
sample size, rendering any exploratory subanalysis infeasible, the
retrospective design and our inability to report quality of life
for the included patients. In addition, the respiratory status
following PM was not addressed in the present study, which is a
consistent limitation among all studies according to a recent
systematic review (21). However,
despite these limitations, our study may provide additional
information on the current outcomes following PM in osteosarcoma,
given the fact that all of our patients were treated recently and
in a setting of multimodality therapy and, as such, may be more
relevant to the current clinical practice. In addition, our study
suggested that chondroblastic histological subtype and visceral
pleural involvement of the resected nodules may add important
prognostic information; however, additional confirmation of those
two identified prognostic factors is required by future
studies.
In conclusion, PM is associated with long-term
survival and the possibility of cure for patients with pulmonary
metastatic osteosarcoma. Factors associated with less favorable
tumor biology, including poor necrosis in the primary tumor,
detection of metastasis during primary chemotherapy and
chondroblastic subtype predicted poor prognosis. In addition,
pathological identification of visceral pleural involvement in any
of the resected pulmonary nodules also predicted poor survival in
our series.
References
|
1
|
Chen F, Miyahara R, Bando T, et al:
Prognostic factors of pulmonary metastasectomy for osteosarcomas of
the extremities. Eur J Cardiothorac Surg. 34:1235–1239. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Huang YM, Hou CH, Hou SM and Yang RS: The
metastasectomy and timing of pulmonary metastases on the outcome of
osteosarcoma patients. Clin Med Oncol. 14:99–105. 2009.PubMed/NCBI
|
|
3
|
Saltzman DA, Snyder CL, Ferrell KL,
Thompson RC and Leonard AS: Aggressive metastasectomy for pulmonic
sarcomatous metastases: a follow-up study. Am J Surg. 166:543–547.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Temeck BK, Wexler LH, Steinberg SM,
McClure LL, Horowitz M and Pass HI: Metastasectomy for sarcomatous
pediatric histologies: results and prognostic factors. Ann Thorac
Surg. 59:1385–1389. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Suzuki M, Iwata T, Ando S, et al:
Predictors of long-term survival with pulmonary metastasectomy for
osteosarcomas and soft tissue sarcomas. J Cardiovasc Surg (Torino).
47:603–608. 2006.PubMed/NCBI
|
|
6
|
Huth JF and Eilber FR: Patterns of
recurrence after resection of osteosarcoma of the extremity.
Strategies for treatment of metastases. Arch Surg. 124:122–126.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ward WG, Mikaelian K, Dorey F, et al:
Pulmonary metastases of stage IIB extremity osteosarcoma and
subsequent pulmonary metastases. J Clin Oncol. 12:1849–1858.
1994.PubMed/NCBI
|
|
8
|
Aljubran AH, Griffin A, Pintilie M and
Blackstein M: Osteosarcoma in adolescents and adults: survival
analysis with and without lung metastases. Ann Oncol. 20:1136–1141.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gelderblom H, Jinks RC, Sydes M, et al
European Osteosarcoma Intergroup: Survival after recurrent
osteosarcoma: data from 3 European Osteosarcoma Intergroup (EOI)
randomized controlled trials. Eur J Cancer. 47:895–902. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kempf-Bielack B, Bielack SS, Jürgens H, et
al: Osteosarcoma relapse after combined modality therapy: an
analysis of unselected patients in the Cooperative Osteosarcoma
Study Group (COSS). J Clin Oncol. 23:559–568. 2005. View Article : Google Scholar
|
|
11
|
Meyers PA, Heller G, Healey JH, et al:
Osteogenic sarcoma with clinically detectable metastasis at initial
presentation. J Clin Oncol. 11:449–453. 1993.PubMed/NCBI
|
|
12
|
Kager L, Zoubek A, Pötschger U, et al:
Primary metastatic osteosarcoma: presentation and outcome of
patients treated on neoadjuvant Cooperative Osteosarcoma Study
Group protocols. J Clin Oncol. 21:2011–2018. 2003. View Article : Google Scholar
|
|
13
|
Bacci G, Briccoli A, Longhi A, et al:
Treatment and outcome of recurrent osteosarcoma: experience at
Rizzoli in 235 patients initially treated with neoadjuvant
chemotherapy. Acta Oncol. 44:748–755. 2005. View Article : Google Scholar
|
|
14
|
Mialou V, Philip T, Kalifa C, et al:
Metastatic osteosarcoma at diagnosis: prognostic factors and
long-term outcome - the French pediatric experience. Cancer.
104:1100–1109. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ferrari S, Briccoli A, Mercuri M, et al:
Postrelapse survival in osteosarcoma of the extremities: prognostic
factors for long-term survival. J Clin Oncol. 21:710–715. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Leary SE, Wozniak AW, Billups CA, et al:
Survival of pediatric patients after relapsed osteosarcoma: the St.
Jude Children's Research Hospital experience. Cancer.
119:2645–2653. 2013.PubMed/NCBI
|
|
17
|
Kimura H, Suzuki M, Ando S, et al:
Pulmonary metastasectomy for osteosarcomas and soft tissue
sarcomas. Cancer & Chemotherapy. 31:1319–1323. 2004.(In
Japanese).
|
|
18
|
Pfannschmidt J, Klode J, Muley T, Hoffmann
H and Dienemann H: Pulmonary resection for metastatic
osteosarcomas: a retrospective analysis of 21 patients. Thorac
Cardiovasc Surg. 54:120–123. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Harting MT, Blakely ML, Jaffe N, et al:
Long-term survival after aggressive resection of pulmonary
metastases among children and adolescentce with osteosarcoma. J
Pediatr Surg. 41:194–199. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Buddingh EP, Anninga JK, Versteegh MI, et
al: Prognostic factors in pulmonary metastasized high-grade
osteosarcoma. Pediatr Blood Cancer. 54:216–221. 2010.PubMed/NCBI
|
|
21
|
Treasure T, Fiorentino F, Scarci M, Møller
H and Utley M: Pulmonary metastasectomy for sarcoma: a systematic
review of reported outcomes in the context of Thames Cancer
Registry data. BMJ Open. 2:e0017362012. View Article : Google Scholar : PubMed/NCBI
|