Introduction
Glioblastoma (GBM) is the most common primary brain
tumor in adults, accounting for ~12–15% of all intracranial
neoplasms (1). Despite advances in
surgical, medical and radiation therapies, the mortality of GBM
remains high, with a median survival ranging between 40 and 70
weeks (2). Like other primary brain
tumors, the extracranial metastasis of GBM is extremely rare,
occurring in <2% of all GBMs (3–8). A
recently published meta-analysis of 88 cases of extracranial GBM
between 1928 and 2009 demonstrated that the prognosis is
particularly poor in this subset of patients, with a median
survival from metastasis to death of 1.5 months; however, there has
been a progressive prolongation of this interval of 0.7 months per
decade between 1940 and 2000 (9).
Patients treated with surgery, radiation, chemotherapy and
cerebrospinal fluid (CSF) shunting exhibit the longest average
survival interval from metastasis to death.
Unique barriers in the brain, including the
blood-brain barrier, thickened basement membrane of blood vessels
and thickened dura mater, lack of extracellular matrix and other
characteristics unique to GBM, prevent hematogenous and lymphatic
spread. The majority of metastases reportedly occur either through
leptomeningeal or intramedullary dissemination to the spinal cord
or following a breach in the abovementioned barriers, e.g., through
craniotomy or intraventricular shunt placement. In the latter,
metastasis is considered to occur by direct spread or tumor
seeding. Metastases of malignant gliomas to the soft tissue,
muscle, or skin, are even more rare, with only nine cases reported
in the literature (10). We herein
present three cases of GBM metastasis: one to the lung, one to the
soft tissue of the posterior neck and one to the lumbar intradural
space (Table I). Of note, our first
case represents the longest survival interval from diagnosis of GBM
lung metastases to death reported in the literature thus far. We
also reviewed the relevant literature in an attempt to delineate
the molecular and genetic basis for GBM metastasis and the
treatment strategies for this aggressive disease.
 | Table I.Summary of case reports. |
Table I.
Summary of case reports.
| Case | Age/gender | Site of
metastasis | Time from Dx to Met
(months) | Time from Dx to Met
(months) | Time from Met to
death (months) | Surgery | Chemotherapy | Radiation |
|---|
| 1 | 29/F | Lung | 22 | 35 | 13 | Gross total
resection, 2 repeat resections, vp shunt | Temozolomide,
bevacizumab, carboplatin | 60 Gy, re-irradiation
38.5 Gy |
| 2 | 29/M | Soft tissue of
posterior neck | 13 | 17 | 4 | Subtotal resection,
repeat resection | Procarbazine,
lomustine, vincristine | 60 Gy |
| 3 | 62/M | Spine and sacral
nerve root | 0 | 6 | 6 | None | None | 46 Gy whole-brain, 46
Gy C-spine, 5,000 cGy sacral |
Case reports
Case 1
A 29-year-old woman presented with a 6-month history
of progressively worsening headaches, vision loss and cachexia. The
magnetic resonance imaging (MRI) revealed a complex 7-cm mass in
the right posterior temporal and parietal lobes (Fig. 1) with multiple intramural cysts,
exhibiting extensive septal and nodular enhancement within the
lesion. There was also perilesional edema with a 5-mm midline shift
to the left side. The patient underwent gross total resection
followed by adjuvant chemotherapy with temozolomide and radiation
therapy (60 Gy). The patient then was continued on maintenance
temozolomide and exhibited significant resolution of her symptoms.
The maintenance therapy was interrupted for 3 months due to the
development of cytopenias and secondary infections. Approximately
14 months after the initial presentation, the patient complained of
increasing headaches and had new-onset seizures. The cranial MRI
revealed abnormal enhancing areas involving the right lateral
aspect of the tentorium cerebelli and right transverse
sinus-sigmoid sinus junction, consistent with tumor recurrence. The
patient was re-irradiated (38.5 Gy) and exhibited an initial
resolution of the headaches, which recurred 3 months later. Repeat
MRI revealed a nodular 3.2×2.6-cm mass along the right lateral
aspect of the tentorium, with abnormal leptomeningeal enhancement
adjacent to the mass and of the cranial nerves VIII and IX. On
biopsy, the lesion proved to be radiation necrosis rather than
tumor. However, a preoperative chest X-ray revealed asymptomatic
bilateral, multiple rounded hyperdensities in the lungs, suggestive
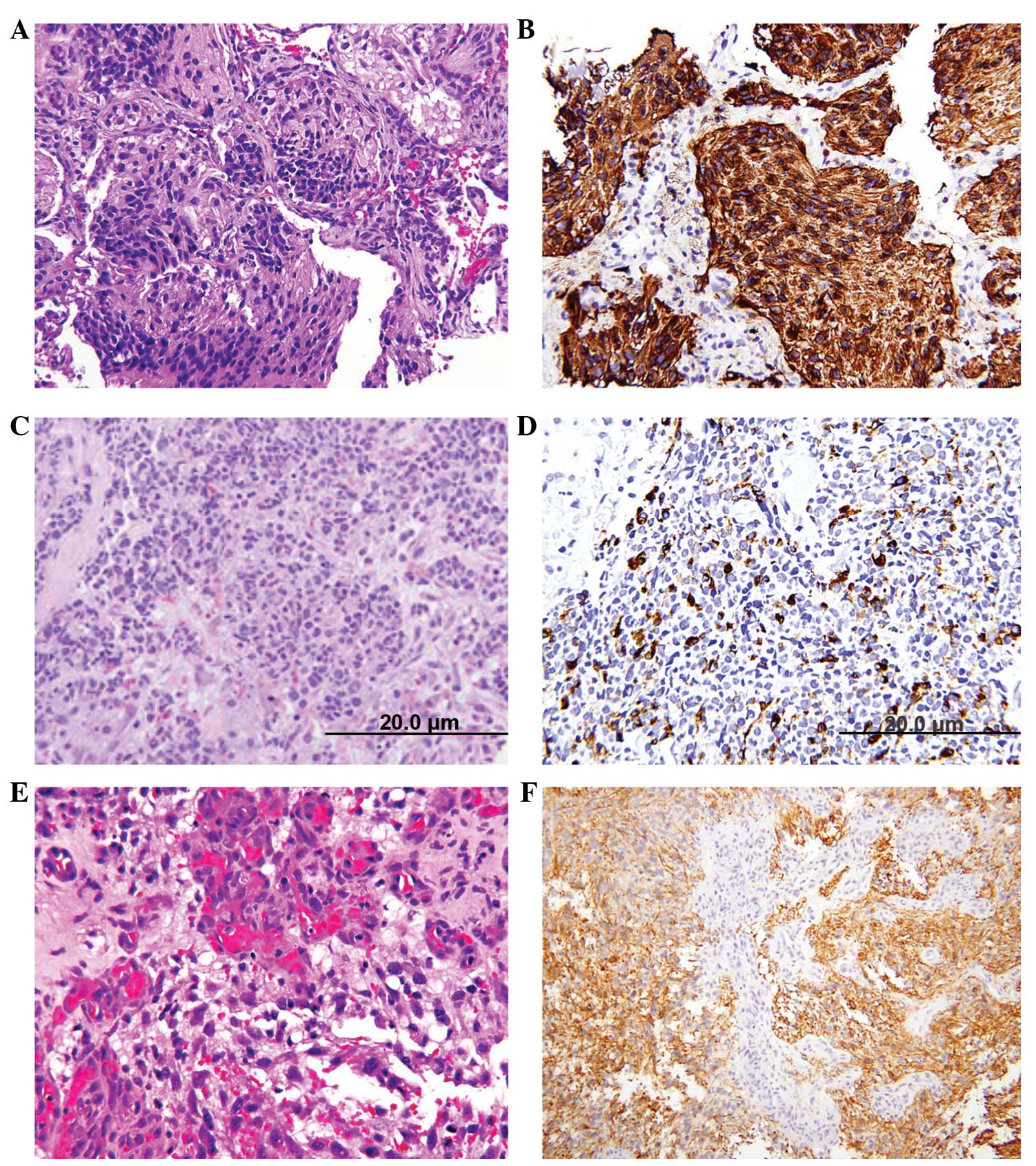
of pulmonary metastases (Fig. 1),
which measured 3.4×4.2 cm on computed tomography (CT). The biopsy
was consistent with metastatic GBM (Fig.
2). Immunohistochemical staining for S100 protein and glial
fibrillary acidic protein (GFAP) was positive in the tumor cells.
The patient presented 4 months later with recurrent headaches as
well as gait alterations. The MRI showed hydrocephalus and a
ventriculoperitoneal shunt was placed. At 24 months after the
initial diagnosis, systemic chemotherapy with bevacizumab and
carboplatin was reinitiated for progressive disease and continued
for 6 months, followed by single-agent bevaciszumab when a
restaging cranial MRI demonstrated progressive disease with
extension of the tumor into the right posterior fossa. At that
time, the patient underwent a third resection. Despite an initial
improvement in the headaches and ataxia, the patient subsequently
exhibited a significant decline in function, generalized weakness
and, at 34 months, entered hospice and declined further care. The
patient succumbed to the disease 1 month later, 35 months after the
initial diagnosis.
Case 2
A 29-year-old man presented with a 2-week history of
confusion, lethargy and a decline in the ability to perform his
daily activities. On examination, the patient was oriented to
person and place. There were no lateralizing focal neurological
deficits. A CT and MRI of the head revealed a large left frontal
lobe mass measuring 6.5×7.5 cm, with areas of calcification and
surrounding edema, exerting a mass effect on the ipsilateral
lateral ventricle. The mass exhibited diffuse heterogeneous
enhancement and small areas of cystic components, along with a
small hemorrhage within the mass. The patient underwent left
frontal craniotomy for subtotal tumor resection. On pathological
examination of the surgical specimen, the tumor was diagnosed as
anaplastic oligodendroglioma. Immunohistochemical staining for GFAP
was strongly positive in a significant proportion of the tumor
cells. The patient improved clinically and became more lucid.
Postoperatively, the patient received radiation therapy (60 Gy) and
chemotherapy with procarbazine, lomustine and vincristine for 6
weeks. Three months after the initial surgery, the patient
presented with a symptomatic recurrence of his left frontal lobe
mass and underwent another resection. Compared to the previous
specimen, there was an overwhelming predominance of neoplastic
astrocytes, upgrading the tumor to GBM. At 13 months from the
initial diagnosis, the patient presented with a progressively
enlarging, pain-free, right posterior neck mass. Following a needle
biopsy and histopathological examination, the neck mass exhibited
similar characteristics to the central nervous system (CNS) tumor
and was diagnosed as metastatic GBM (Fig.
2). Immunohistochemical stains with antibodies directed against
S100 protein and GFAP were reactive with the tumor cells.
Synaptophysin immunostaining, which was initially non-reactive, was
found to be positive, possibly representing a more primitive clone
with divergent differentiation, similar to that seen in primitive
neuroectodermal tumors. The patient succumbed to the disease 4
months later, 17 months after the initial diagnosis.
Case 3
A 62-year-old man presented with right-sided low
back pain and pain in the buttocks, which occasionally radiated
down the lateral aspects of his right leg. The patient did complain
of occasional frontal headaches over the past several years;
however, the neurological examination was unremarkable. An MRI of
the lumbar spine revealed a homogenously enhancing mass in the
L5-S1 region to the right of the midline, measuring 9×10×15 mm and
exerting a moderate mass effect, pushing the thecal sac to the left
(Fig. 3). The imaging characteristics
were considered to be suggestive of a right S1 schwannoma. The
electromyogram was consistent with right S1 radiculopathy. The
patient underwent a L5 laminectomy for resection of the intradural
tumor. The pathological specimen was diagnosed as GBM and the tumor
cells stained positive for GFAP, S100 and vimentin (Fig. 2). This unusual diagnosis prompted an
MRI of the brain, which revealed a ring-enhancing mass in the left
mediotemporal lobe, measuring 2.5×2.8×2.4 cm, and an 8-mm nodular
focus of enhancement adjacent to the left inferior frontal gyrus
(Fig. 3). An MRI scan of the cervical
and thoracic spine was also performed, revealing posterior
arachnoid thickening at the C6–7 level, which was consistent with
leptomeningeal spread of the disease. The patient was scheduled to
receive 46 Gy whole-brain radiation in 2-Gy daily fractions, 46 Gy
cervical spine radiation in 2-Gy daily fractions and 5,000 cGy
sacral radiation in 200-cGy daily fractions. Although the patient
tolerated treatment well, with improved headaches and back pain
after receiving a total of 49 Gy, he decided to discontinue
treatment. The patient subsequently exhibited increased fatigue,
worsening low back pain and an abrupt decline in functional status.
Despite being encouraged to complete the radiation therapy and
receiving information on available home-health psychiatric
services, the patient declined further treatment and was
transferred to hospice 3 months after the initial diagnosis. The
patient succumbed to the disease 3 months later, 6 months after the
initial diagnosis.
Discussion
Extracranial metastasis of GBM is extremely rare,
occurring in <2% of patients. When either extra- or intracranial
metastasis occurs, the median time from initial tumor diagnosis to
recognition of metastases is 8.5 months (9). Several theories on why GBM is rarely
associated with extracranial metastasis have been proposed.
According to one of those theories, due to the highly aggressive
behavior of GBMs, patients succumb to their intracranial disease
before there is sufficient time for distant metastasis to develop.
The majority of the patients succumb to GBM within 20 months,
usually secondary to intracranial mass effect or invasion,
sometimes with elevation of the intracranial pressure. Since
metastasis is rare, systemic staging or screening with body CT,
MRI, or positron emission tomography imaging is not standard
practice. Therefore, metastasis may occur more frequently than what
is reported in the literature, but is not clinically recognized
prior to fatal brain herniation. In fact, there are two reports of
metastatic GBM following bilateral lung transplantation from a
donor with GBM, highlighting that there may be unrecognized GBM
micrometastases at the time of death (10,11).
Another theory suggest that there are unique
barriers in the brain that prevent hematogenous and lymphatic
spread, including the dura and the thickened basement membrane of
the blood vessels. As a result, most cases of metastasis are
considered to occur following craniotomy or intraventricular shunt
placement, during which time tumor cells gain access to the blood
stream through defects in the meningeal and parenchymal blood
vessels that are created from such manipulation (12). Stereotactic biopsies may also cause
disease spread, most likely through seeding of tumor cells during
the invasive procedure (1,13,14). In
cases with scalp metastasis in close proximity to the craniotomy or
biopsy site, it is difficult to establish whether it is a result of
true blood-born metastasis or seeding of tumor cells. However,
Armstrong et al (15) recently
reported a case of a scalp metastasis circumscribed within the soft
tissue, several centimeters away from the craniotomy site, where
neither an indwelling catheter or an established breach of the dura
was present. Although cases 1 and 2 (metastases to the lung and
posterior neck, respectively) occurred months after craniotomy,
these metastatic sites are more distant compared to the scalp and
local cranial vault tissues and, thus, are more likely attributable
to blood-born metastasis rather than local tumor seeding at the
time of the initial craniotomy.
Mentrikoski et al (12) proposed that another reason primary
brain tumors rarely metastasize outside of the CNS is the lack of
extracellular matrix protein. In other organs, tumors metastasize
by first invading through connective tissue, basement membranes and
blood vessels. It is hypothesized that, as there is a near absence
of collagen and fibronectin within the CNS, malignant CNS tumor
cells lack a component necessary for metastasizing outside the CNS.
However, fibronectin may very well be present in GBM cells, as
demonstrated in the following study: Using reverse
transcription-polymerase chain reaction, immunocytochemistry and
enzyme-linked immunosorbent assay, Lin et al (16) demonstrated that the expression of
vascular endothelium-derived fibronectin was more prominent in
endothelial cells of high-grade gliomas compared to those of
low-grade gliomas. The authors also demonstrated that the
interaction of glioma cells and vascular endothelial cells in
vitro induced fibronectin release from vascular endothelial
cells, which in turn stimulated glioma cell migration. This
migration was inhibited by fibronectin-blocking antibody. These
observations challenge the popular view that there is a near
absence of collagen and fibronectin within the CNS and explain how
endothelial cells in GBMs have the ability to invade through
connective tissue and subsequently metastasize distally.
The rarity of GBM growing outside the CNS was also
investigated by Mourad et al (17). The authors implanted brain tumor cells
characterized with respect to in vitro and in vivo
morphology, growth rate, anchorage-independent growth, GFAP
expression and cytogenetic analysis and major histocompatibility
complex typing. Intracerebral and systemic GBM growth was assayed
in three different rodent models with increasingly different
immunological variants between the implanted cells and the murine
host, an isograft, an allograft and a xenograft. The authors
demonstrated growth of intracerebral and systemic tumors in
isografts, growth of intracerebral tumors and suppression of
systemic tumors in allografts and lack of growth of intracerebral
and systemic tumors in xenografts. The results indicated that tumor
cells implanted outside the CNS were able to form tumors, unless
there was a significant difference between the immunotype of the
implanted cells and the host, suggesting the role of the immune
response in controlling these neoplasms and supporting that there
are physical and systemic barriers that impede systemic GBM
metastasis. GBMs appear to be antigenic -not immunogenic- and,
therefore, should be amenable to targeted immunotherapy.
Another study by Park et al (18) proposed that the emergence of
neoplastic subclones may be responsible for GBM metastasis. In 6
patients with GBM metastases, primary and metastatic tumor tissue
was evaluated for common genetic alterations found in GBMs, such as
TP53 mutations, CDKN2A/p16 deletions, epidermal growth factor
receptor amplifications and allelic losses of chromosomes 1p, 10q
and 19q. In 2 of these patients, different molecular genetic
patterns were observed between the primary and metastatic lesions,
primarily differences in TP53 mutations between the CNS lesion and
the metastases or among the metastases themselves. This finding
suggests that certain metastatic lesions may be characterized by
TP53 mutations and represent the emergence of subclones that were
not necessarily dominant in the primary tumor.
Unlike GBMs, gliosarcomas, a rare variant of grade
IV gliomas, have a tendency to metastasize. Consideration of the
histological characteristics of these tumors may indicate the
possible mechanisms underlying GBM metastasis. Treatment for GBM,
particularly irradiation, may cause sarcomatous metaplasia of glial
cells and help GBMs acquire the necessary extracellular matrix
proteins for vascular invasion and hematogenous dissemination to
distant extracranial sites. Gliosarcomas consist of an admixture of
gliomatous and sarcomatous components and are more likely to invade
connective tissue. Thus, these tumors exhibit a greater propensity
for extracranial metastasis. For a long time, gliosarcoma was
considered to be a GBM, in which the vascular elements had become
sarcomatous. Recent molecular studies, however, have refuted this
theory and proposed that the sarcomatous component arises from
metaplastic transformation of glial cells rather than vascular
elements. Beaumont et al (19)
reviewed these molecular characteristics, which include identical
p53 and PTEN mutations, p16 deletions and amplification of MDM2 and
CDK4. Common cytogenetic abnormalities have also been demonstrated
in the two lineages, including trisomy 7, deletion of 9p, monosomy
10 and 17 and non-random chromosome X inactivation. Although
sarcomatous metaplasia appears to be a possible mechanism of
extracranial metastasis for GBMs, sarcomatous components were not
identified on histological review of our three cases.
Spinal metastasis of GBM, in contrast to extra-axial
metastases, is more common, has been extensively described in
autopsy series and is considered to occur through either
leptomeningeal or intramedullary dissemination. Symptomatic spinal
metastases largely occur in relatively younger patients with a
longer duration of survival. However, upon diagnosis of such a
metastasis the prognosis is dismal, with a mean subsequent survival
time of 2.8 months and poor response of the metastatic disease to
radiation therapy (20–22). CSF cytology is poorly sensitive for
spinal metastasis; however, GFAP expression appears to be a
histological marker for potential spinal spread. Patients with
GFAP-negative tumors, representing the presence of poorly
differentiated astrocytic glioma cells, exhibit aggressive CSF
dissemination with little infiltration at the primary site, whereas
the opposite is observed for GFAP-positive, highly differentiated
tumor cells (23,24). Case 3 described in our series was
characterized by spinal metastasis; however, it should be noted
that the patient initially presented with radicular symptoms prior
to the diagnosis of the primary brain tumor; furthermore, he was
aged >60 years and his tumor was GFAP-positive. However, the
survival time from diagnosis to death was the poorest of all three
patients, which is consistent with the poor prognosis of GBM spinal
metastases reported in the literature. The treatment of patients
with spinal GBM metastases remains challenging, as there are few
precedents in the clinical literature. Available data suggest
chemotherapy, spinal irradiation and palliative resection, although
the prognosis remains poor (25).
The standard treatment for intracranial GBM is
maximal safe surgical resection, followed by concurrent
radiotherapy and chemotherapy (26).
However, clinical studies evaluating different treatment strategies
for metastatic disease are sparse and the optimal treatment for
metastatic disease has not been determined. From our case series
and from the review of current literature, two patterns of GBM
distal metastasis emerge, namely neuroaxial and systemic
metastasis. In patients with neuroaxial dissemination, there may be
a role for debulking surgery and irradiation. Our patient in case 3
received craniospinal radiation following initial resection of the
spinal metastasis. By contrast, for patients with systemic distal
metastasis, organ-specific considerations should be made when
planning adjuvant therapy (27). The
phenomenon of an intracerebral tumor continuing to grow while the
same tumor diminishes in response to systemic chemotherapy has been
well described in animal and human models (28). In terms of definitive oncological
treatment for metastatic GBM, our case series and other reports
reviewed here suggest that treatment should focus on systemic
chemotherapy. Lun et al (9)
conducted a meta-analysis of 88 cases of extracranial metastasis of
GBM and found that patients treated with surgery + radiation +
chemotherapy + cerebrospinal shunting exhibited the longest average
survival interval from metastasis to death compared to those
treated with surgery alone, radiation alone, surgery + radiation,
or surgery + radiation + chemotherapy.
The optimal chemotherapeutic agents, however, have
yet to be defined. The most commonly used treatments include
temozolomide and nitrosurea-based agents (26,29–31).
Methylguanine-DNA methyltransferase tumor status and higher levels
of expression in tumors may confer resistance to alkylating agents
(32). Bevacizumab, a vascular
endothelial growth factor A-binding antibody, has also been used as
a monotherapy or in combination with chemotherapy (33,34).
However, recent randomized controlled studies in the United States
and Europe have demonstrated the lack of efficacy of bevacizumab
(35,36). Our patient in case 1 with GBM
metastasis to the lung received treatment with bevacizumab in
combination with carboplatin. The combination of multiple
resections, systemic chemotherapy, bevacizumab and
ventriculoperitoneal shunting in this patient resulted in 13 months
of survival from metastasis to death - the longest reported
survival of lung metastases from GBM to date. Lun et al
(9) found that lung metastasis is a
statistically significant prognostic factor of poor outcomes, with
a relative decrease of 2.7 months in the interval from detection of
extracranial metastases to death. From our experience with this
case, it appears that bevacizumab may be a valuable adjunct in this
subset of patients, who have traditionally had an extremely poor
prognosis.
Recent reports help explain why bevacizumab may not
be effective in arresting disease progression. As explained above,
the invasive quality of GBM is partly mediated by vascular
proliferation. The abnormal endothelium of GBM that allows this
proliferation and, possibly, vascular invasion and subsequent
distant metastasis, was recently described by Wang et al
(37), who identified stem-like cells
in GBM tumors by expression of CD133. A subset of these cells
expresses vascular endothelial cadherins, CD144. The authors
demonstrated that when CD133+/144+
(double-positive cells) were cultured in endothelial medium, they
differentiated into endothelial cells with a downregulation of
CD144 and upregulation of endothelial markers, including CD105,
which were capable of forming vascular networks within abnormal,
thickened channels. In addition, when
CD133+/CD144− cancer stem cells were
co-cultured with GBM tumor cells, some of the
CD133+/CD144− cells converted to
double-positive cells. Both double-positive and
CD133+/CD144− cells resulted in highly
infiltrative tumors when implanted in the striatum of
immunodeficient mice. The investigators then tested the effects of
bevacizumab and
N-[N-(3,5-difluorophenacteyl)-L-alanyl]-S-phenylglycine t-butyl
ester, a γ-secretase inhibitor that inhibits Notch signaling, on
the conversion of CD133+/CD144− to
double-positive cells and the conversion of double-positive cells
to CD105+ cells. Bevacizumab did not block the
conversion of CD133+/CD144− to
double-positive cells, but did prevent double-positive cells from
differentiating into endothelial cells (CD105+). On the
other hand, N-[N-(3,5-difluorophenacteyl)-L-alanyl]-S-phenylglycine
t-butyl ester had the opposite effect; it blocked the conversion of
CD133+/144− to double-positive cells but did
not affect further maturation, explaining the inefficacy of
bevacizumab alone in the treatment of GBM and suggesting that
combination therapy with both agents may be the optimal
treatment.
In conclusion, extracranial metastasis of GBM is a
rare phenomenon and the published literature regarding this disease
entity is sparse. The role of molecular and genetic factors in
metastatic GBM may have implications in terms of therapeutic
targets and adjuvant treatments; however, more thorough genetic
profiling in larger case series is mandated. The interactions of
glioma cells and their vascular niche is an additional component of
GBM invasion and metastasis to consider, as is the presence of
extracellular matrix proteins that emerge as a result of this
interaction. As our therapeutic armamentarium for intracranial GBMs
continues to evolve, along with a better understanding of their
biology, and as we are able to prolong the survival of patients
with such tumors, the number of cases of metastatic GBMs may
continue to increase. In this study, we elucidated the role of
systemic chemotherapy with temozolamamide ± bevacizumab in the
treatment of metastatic GBMs; however, the role of staging for
prognosis and specific treatment paradigms must be further
defined.
References
|
1
|
Saad AG, Sachs J, Turner CD, et al:
Extracranial metastases of glioblastoma in a child: case report and
review of the literature. J Pediatr Hematol Oncol. 29:190–194.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rajagopalan V, El Kamar FG, Thayaparan R
and Grossbard ML: Bone marrow metastases from glioblastoma
multiforme – a case report and review of the literature. J
Neurooncol. 72:157–161. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Datta CK, Weinstein JD, Bland JE, Brager
PM and Stewart MA: A case of cervical lymph node metastasis
resulting from glioblastoma multiforme. W V Med J. 94:276–278.
1998.PubMed/NCBI
|
|
4
|
Fecteau AH, Penn I and Hanto DW:
Peritoneal metastasis of intracranial glioblastoma via a
ventriculoperitoneal shunt preventing organ retrieval: case report
and review of the literature. Clin Transplant. 12:348–350.
1998.PubMed/NCBI
|
|
5
|
Piccirilli M, Brunetto GM, Rocchi G,
Giangaspero F and Salvati M: Extra central nervous system
metastases from cerebral glioblastoma multiforme in elderly
patients. Clinico-pathological remarks on our series of seven cases
and critical review of the literature. Tumori. 94:40–51.
2008.PubMed/NCBI
|
|
6
|
Templeton A, Hofer S, Töpfer M, et al:
Extraneural spread of glioblastoma – report of two cases.
Onkologie. 31:192–194. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Widjaja A, Mix H, Gölkel C, et al:
Uncommon metastasis of a glioblastoma multiforme in liver and
spleen. Digestion. 61:219–222. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yasuhara T, Tamiya T, Meguro T, et al:
Glioblastoma with metastasis to spleen – case report. Neurol Med
Chir (Tokyo). 43:452–456. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lun M, Lok E, Gautam S, Wu E and Wong ET:
The natural history of extracranial metastasis from glioblastoma
multiforme. J Neurooncol. 105:261–273. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Armanios MY, Grossman SA, Yang SC, White
B, Perry A, Burger PC and Orens JB: Transmission of glioblastoma
multiforme following bilateral lung transplantation from an
affected donor: case study and review of the literature. Neuro
Oncol. 6:259–263. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen H, Shah AS, Girgis RE and Grossman
SA: Transmission of glioblastoma multiforme after bilateral lung
transplantation. J Clin Oncol. 26:3284–3285. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mentrikoski M, Johnson MD, Korones DN and
Scott GA: Glioblastoma multiforme in skin: a report of 2 cases and
review of the literature. Am J Dermatopathol. 30:381–384. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bouillot-Eimer S, Loiseau H and Vital A:
Subcutaneous tumoral seeding from a glioblastoma following
stereotactic biopsy: case report and review of the literature. Clin
Neuropathol. 24:247–251. 2005.PubMed/NCBI
|
|
14
|
Sloan AE, Ahluwalia MS, Valerio-Pascua J,
et al: Results of the NeuroBlate System first-in-humans phase I
clinical trial for recurrent glioblastoma: clinical article. J
Neurosurg. 118:1202–1219. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Armstrong TS, Prabhu S, Aldape K, et al: A
case of soft tissue metastasis from glioblastoma and review of the
literature. J Neurooncol. 103:167–172. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lin ZX, Yang LJ, Huang Q and Fu J:
Activated vascular endothelia regulate invasion of glioma cells
through expression of fibronectin. Chin Med J (Engl).
123:1754–1761. 2010.PubMed/NCBI
|
|
17
|
Mourad PD, Farrell L, Stamps LD, Chicoine
MR and Silbergeld DL: Why are systemic glioblastoma metastases
rare? Systemic and cerebral growth of mouse glioblastoma. Surg
Neurol. 63:511–519. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Park CC, Hartmann C, Folkerth R, et al:
Systemic metastasis in glioblastoma may represent the emergence of
neoplastic subclones. J Neuropathol Exp Neurol. 59:1044–1050.
2000.PubMed/NCBI
|
|
19
|
Beaumont TL, Kupsky WJ, Barger GR and
Sloan AE: Gliosarcoma with multiple extracranial metastases: case
report and review of the literature. J Neurooncol. 83:39–46. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Maslehaty H, Cordovi S and Hefti M:
Symptomatic spinal metastases of intracranial glioblastoma:
clinical characteristics and pathomechanism relating to GFAP
expression. J Neurooncol. 101:329–333. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Medhkour A and Chan M: Extremely rare
glioblastoma multiforme of the conus medullaris with holocord and
brain stem metastases, leading to cranial nerve deficit and
respiratory failure: a case report and review of the literature.
Surg Neurol. 63:576–583. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vertosick FT Jr and Selker RG: Brain stem
and spinal metastases of supratentorial glioblastoma multiforme: a
clinical series. Neurosurgery. 27:516–522. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Arita N, Taneda M and Hayakawa T:
Leptomeningeal dissemination of malignant gliomas. Incidence,
diagnosis and outcome. Acta Neurochir (Wien). 126:84–92. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Onda K, Tanaka R, Takahashi H, Takeda N
and Ikuta F: Cerebral glioblastoma with cerebrospinal fluid
dissemination: a clinicopathological study of 14 cases examined by
complete autopsy. Neurosurgery. 25:533–540. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hübner F, Braun V and Richter HP: Case
reports of symptomatic metastases in four patients with primary
intracranial gliomas. Acta Neurochir (Wien). 143:25–29. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Stupp R, Mason WP, van den Bent MJ, et al:
Radiotherapy plus concomitant and adjuvant temozolomide for
glioblastoma. N Engl J Med. 352:987–996. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Astner ST, Pihusch R, Nieder C, et al:
Extensive local and systemic therapy in extraneural metastasized
glioblastoma multiforme. Anticancer Res. 26:4917–4920.
2006.PubMed/NCBI
|
|
28
|
Steinbok P, Dolman CL and Goldie JH:
Variation in response to CCNU of glioblastoma multiforme in brain
and cervical lymph node. Case report. J Neurosurg. 62:918–921.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Brandes AA, Tosoni A, Cavallo G, et al
GICNO: Temozolomide 3 weeks on and 1 week off as first-line therapy
for recurrent glioblastoma: phase II study from Gruppo Italiano
Cooperativo di Neuro-Oncologia (GICNO). Br J Cancer. 95:1155–1160.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gaviani P, Silvani A, Lamperti E, Botturi
A, Fariselli L, Simonetti G, Ferrari D and Salmaggi A: Rechallenge
with temozolomide in recurrent glioma. Neurol Sci. 32:S247–S249.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Perry JR, Rizek P, Cashman R, Morrison M
and Morrison T: Temozolomide rechallenge in recurrent malignant
glioma by using a continuous temozolomide schedule: the ‘rescue’
approach. Cancer. 113:2152–2157. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hegi ME, Diserens AC, Gorlia T, et al:
MGMT gene silencing and benefit from temozolomide in glioblastoma.
N Eng J Med. 352:997–1003. 2005. View Article : Google Scholar
|
|
33
|
Chamberlain MC and Johnston SK: Salvage
therapy with single agent bevacizumab for recurrent glioblastoma. J
Neurooncol. 96:259–269. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Friedman HS, Prados MD, Wen PY, et al:
Bevacizumab alone and in combination with irinotecan in recurrent
glioblastoma. J Clin Oncol. 27:4733–4740. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chinot OL, Wick W, Mason W, et al:
Bevacizumab plus radiotherapy-temozolomide for newly diagnosed
glioblastoma. N Engl J Med. 370:709–722. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gilbert MR, Dignam JJ, Armstrong TS, et
al: A randomized trial of bevacizumab for newly diagnosed
glioblastoma. N Engl J Med. 370:699–708. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wang R, Chadalavada K, Wilshire J, et al:
Glioblastoma stem-like cells give rise to tumour endothelium.
Nature. 468:829–833. 2010. View Article : Google Scholar : PubMed/NCBI
|