Introduction
Due to the growing public interest in breast cancer
and the widespread use of mammographic screening, the early
detection rate of breast cancer has increased. Increased breast
tissue density, however, may make mammograms more difficult to
interpret. Dense breast tissue is considered one of the major risk
factors of breast cancer, although the underlying mechanism has yet
to be elucidated (1). Mammographic
breast density refers to the percentage of fibroglandular tissues
in the breast. The incidence of breast cancer was found 4-6-fold
higher in a group with higher breast density compared to that in
another, lower density group (2,3).
As a factor associated with mammographic breast
density, the insulin-like growth factor (IGF) system has been well
documented and reported to be of more relevance to premenopausal
women (4,5). The IGF system acts as a factor
controlling growth in the human body and plays an important role in
the development of normal breast tissues. The IGF system consists
of IGF-1, IGF-2, IGF-1 receptor (IGF-1R), IGF-2R and six
IGF-binding proteins (IGFBPs) (6).
Notably, IGF-1 and IGFBP in the blood are reported to affect breast
density. Normal dense breast tissues exhibit a higher expression of
IGF-1 compared to non-dense breast tissue, which suggests that
IGF-1 is associated with mammographic density (7). However, rather than observing the IGF-1
expression in tissues, examining the expression of receptors and
downstream signaling molecules activated by these receptors may
provide more accurate information on its relevance to breast tissue
density. To the best of our knowledge, no previous studies have
investigated the relevance of IGF-1R expression in breast cancer
tissues to breast density. By investigating the correlation between
mammographic density and IGF-1R expression, we may determine
whether IGF-1R expression is associated with the mechanism
underlying dense breast tissue constituting a risk factor for
breast cancer.
In terms of its structure, IGF-1R is similar to
insulin receptors and consists of an α chain that has two
extracellular binding domains and two transmembrane β chains,
forming a heterodimer. IGF-1R is a transmembrane tyrosine kinase
receptor and its expression is known to be involved in mitosis,
advancement and metastasis of breast cancer (8,9). Unlike
other tyrosine kinase receptors, IGF-1R is subject to autocrine,
paracrine and endocrine controls (10). In normal breast epithelial tissues,
IGF-1R reportedly exhibits a homogenous moderate expression.
Although IGF-1R expression in breast cancer has been limitedly
investigated, its overexpression in tumour tissues shows a wide
distribution, namely 39–93% (11,12). The
overexpression of IGF-1R promotes anti-apoptosis, cell adhesion,
mitosis and malignant cell transformation, resulting in breast
cancer (12–14). Although certain studies reported that
the overexpression of IGF-1R in breast cancer is closely associated
with estrogen receptors (ERs) and serves as a good prognostic
factor, other studies reported conflicting results; thus, the
findings on the clinical significance of IGF-1R overexpression in
tumours are not consistent across studies (15–18).
The present study aimed to investigate the
correlations between IGF-1R expression in breast cancer tissues,
mammographic density and other clinicopathological factors and
determine the clinical significance of IGF-1R overexpression.
Patients and methods
Patients
A total of 167 breast cancer patients (median age
47years; range, 20–81 years) who were operated at the Department of
Surgery of Severance Hospital between January, 2000 and December,
2001 were analyzed. Patient information, including age, height,
weight, menopausal status, medication history, survival and
recurrence status and clinicopathological data, including tumour
size, nuclear grade, histological grade and lymph node metastasis,
were obtained from electronic medical records. The mean follow-up
was 91 months (range, 5–115 months). Mammographic breast density
and IGF-1R overexpression were correlated with clinicopathological
parameters and analyzed by overall survival (OS) and disease-free
survival (DFS). This study conformed to the guidelines of the local
Ethics Committee.
Immunohistochemical (IHC)
analysis
Serial 4-µm sections of the tissue microarray block,
containing breast cancer tissue with a diameter of 3 mm, were
mounted on electrostatic slides, heat-dried at 56°C for 30 min,
deparaffinized in xylene and rehydrated through graded
concentrations of ethanol. The slides were incubated in a solution
of 3% hydrogen peroxide in methanol for 15 min to block endogenous
peroxidase activity. The slides were incubated in 0.3% bovine serum
albumin/1X Tris-buffered saline (TBS) for 20 min to reduce
non-specific background staining. A primary antibody was applied
for 30 min at room temperature. After a series of TBS rinses, the
bound antibody was detected using a polymer secondary antibody from
the Dako EnVision+ system (Dako, Carpinteria, CA, USA). The slides
were rinsed with a TBS series and visualized after a 10-min
incubation of liquid 3,3′-diaminobenzidine (DAB) in buffered
substrate (Dako) for 10 min. The slides were counterstained with
hematoxylin. IHC analysis for rabbit anti-ER antibody (RM-9101;
SP1, 1:100; Thermo Scientific, San Diego, CA, USA), mouse
anti-progesterone receptor (PR) antibody (M3569; PgR, 1:50;
DakoCytomation, Glostrup, Denmark), rabbit human epidermal growth
factor receptor 2 (HER-2) antibody (A0485; polyclonal, 1:1,500;
DakoCytomation), mouse epidermal growth factor receptor (EGFR)
antibody (NCL-EGFR-384; EGFR 25, 1:50; Novocastra, Newcastle, UK),
mouse cytokeratins (CK) 5/6 antibody (M7237; D5/16B4, 1:100;
DakoCytomation), mouse Ki-67 antibody (M7240; MIB-1, 1:10;
DakoCytomation). For IHC staining of rabbit IGF-1R antibody (3027),
tissue sections were cut and placed on Superfrost Plus microscope
slides (Fisher Scientific, San Diego, CA, USA). Using the Benchmark
XT automated IHC stainer (IRβ, 1:10; Cell Signaling Technology,
Inc., Danvers, MA, USA), the slides were stained. The sections were
deparaffinized using EZ Prep solution. CC1 standard (a pH 8.4
buffer containing Tris/Borate/EDTA) was used for antigen retrieval.
DAB inhibitor (3% H2O2; endogenous
peroxidase) was blocked for 4 min at 37°C temperature. The slides
were incubated with antibodies for 40 min at 37°C and a secondary
antibody of Univeral HRP Multimer for 8 min at 37°C. The slides
were then treated with DAB+H2O2 substrate for
8 min, followed by hematoxylin and bluing reagent counterstain at
37°C. Reaction buffer (pH 7.6 Tris buffer) was used as a washing
solution. Detection was performed using the Ventana Ultraview DAB
kit (Ventana Medical Systems, Inc., Tucson, AZ, USA).
Interpretation of IHC staining
All IHC markers were evaluated by light microscopy.
The immunostained slides were scored according to the percentage of
tumour cells exhibiting nuclear (ER, PR), cytoplasmic (CK 5/6) and
membranous (HER-2, EGFR) staining. A cut-off value of ≥1%
positively stained nuclei was used to define ER and PR positivity.
HER-2 staining was analyzed as follows: 0, no immunostaining; 1+,
weak incomplete membranous staining, <10% of the tumour cells;
2+, complete membranous staining, either uniform or weak in ≥10% of
the tumour cells; and 3+, uniform intense membranous staining in
≥30% of the tumour cells. HER-2 immunostaining was considered to be
positive when strong (3+) membranous staining was observed, whereas
cases scored as 0 or 1+ were considered to be negative. The cases
exhibiting 2+ HER-2 expression were evaluated for HER-2
amplification by fluorescent in situ hybridization (FISH).
The IGF-1R expression was scored according to the intensity of the
membranous staining within the invasive component in accordance
with the scoring of HER-2 by the HercepTest: 0, no staining or
staining observed in <10% of the tumour cells; 1+, faint or
barely perceptible membranous staining in ≥10% of the tumour cells
and cells only stained in part of their membrane; 2+, weak to
moderate complete membranous staining in ≥10% of the tumour cells;
and 3+, strong complete membranous staining in ≥10% of the tumour
cells (15). According to the IGF-1R
expression, the cases were divided into low-expression (scores 0
and 1) and overexpression groups (scores 2 and 3) (Fig. 1).
Tumour subtype classification
Breast cancer subtypes were classified according to
the IHC and FISH results for ER, PR and HER-2 as follows: Luminal A
type, ER- or/and PR-positive and HER-2-negative; luminal B type,
ER- or/and PR-positive and HER-2 overexpressed or/and amplified;
HER-2 type, ER- and PR-negative and HER-2 overexpressed or/and
amplified; triple-negative breast cancer type, ER-, PR-and HER-2
negative.
Mammographic density
The mammographic images taken at the time of
operation or within 1 year after the operation were evaluated. All
the mammograms were performed in the same clinic with the Lorad
M-III unit (Lorad Medical Systems, Danbury, CT, USA) and were
reviewed by one radiologist and one breast surgeon with experience
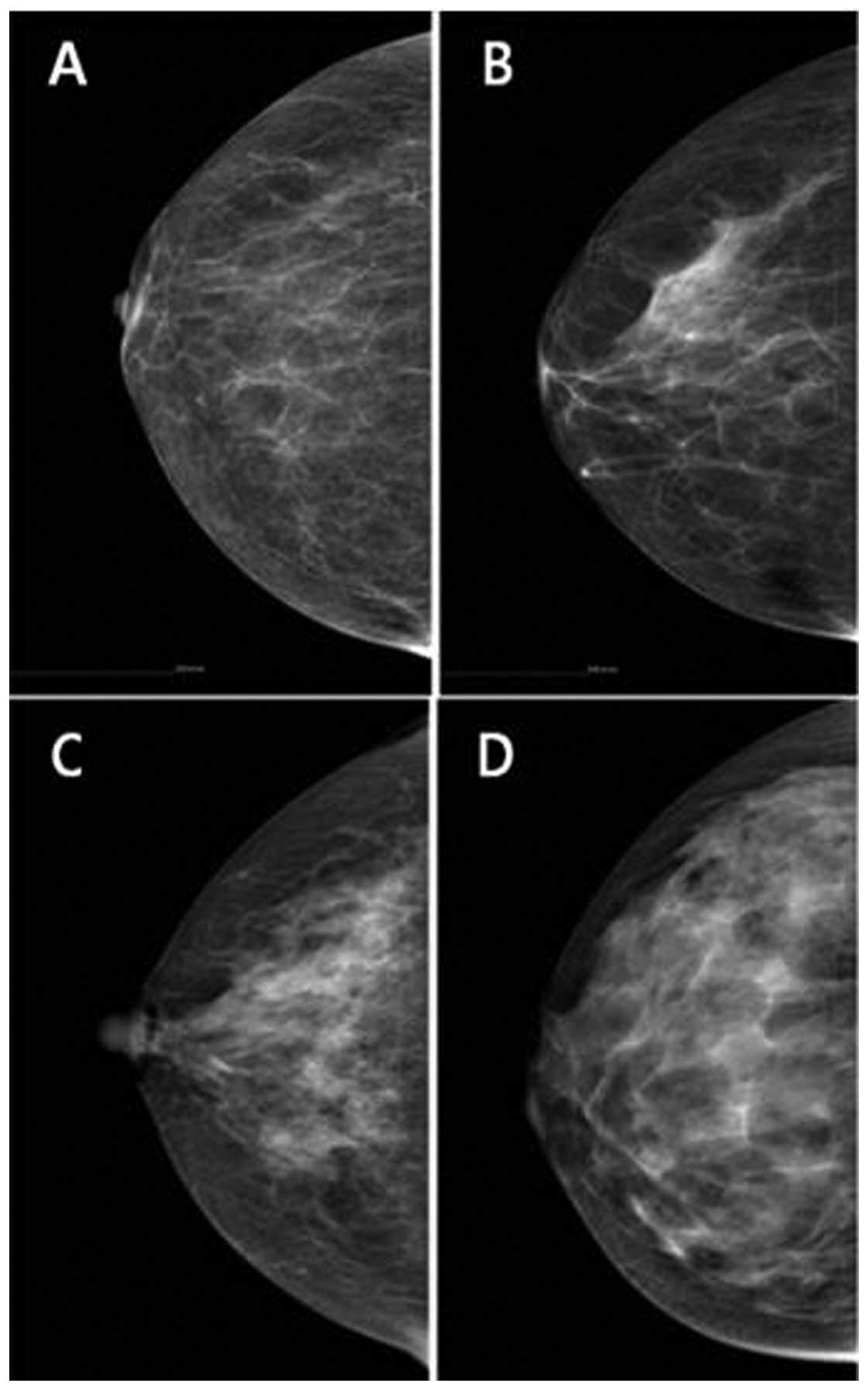
in the assessment of breast density by visual grading system. On
the basis of American College of Radiology Breast Imaging Reporting
and Data System (BI-RADS) breast composition, four density patterns
were designated as grades 1–4, with dense breast tissue graded as 3
and 4 (Fig. 2). The inter-observer
variability of the mammographic density was 0.679 and the
intra-observer variability was 0.786 and 0.703, respectively.
Statistical analysis
Data were processed using SPSS software for Windows,
version 12.0 (SPSS Inc., Chicago, IL, USA). The Chi-square test for
univariate analysis and the logistic regression analysis for
multivariate analysis were used to assess the correlation among
IGF-1R expression, mammographic breast density, clinicopathological
variables and breast cancer-related biomarkers. Cohen's Kappa test
was used to assess intra- and inter-observer variability in the
evaluation of mammographic breast density. Kaplan-Meier survival
curves were employed to evaluate OS and DFS. The Chi-square test
was used for univariate analysis and multivariate regression
analysis was performed using the Cox proportional hazards model,
with variables including mammographic breast density, expression of
IGF-1R, nuclear grade, histological grade, tumour size, lymph node
metastasis, ER, PR and HER-2 status, EGFR, CK 5/6 and Ki-67 for
survival analysis. P<0.05 was considered to indicate a
statistically significant difference.
Results
Correlation of clinicopathological
characteristics with IGF-1R expression and mammographic
density
The clinicopathological characteristics of the
patients and the correlation among IGF-1R expression, mammographic
breast density, clinicopathological variables and breast
cancer-related biomarkers are shown in Tables I and II.
 | Table I.Correlation of insulin-like growth
factor 1 receptor (IGF-1R) expression and mammographic breast
density with clinicopathological variables in primary breast
cancer. |
Table I.
Correlation of insulin-like growth
factor 1 receptor (IGF-1R) expression and mammographic breast
density with clinicopathological variables in primary breast
cancer.
|
|
| IGF-1R
expression | Dense breast
tissue |
|---|
|
|
|
|
|
|---|
|
|
| Low | High | Negative | Positive |
|
|---|
|
|
|
|
|
|
|---|
| Variables | Total (%) | No. (%) | No. (%) | P-value | No. (%) | No. (%) | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
| Median,
47 (range, 20–81) | 167 | 104 (62.3) | 63 (37.7) | 0.207 | 97 (58.1) | 70 (41.9) | 0.001 |
| Menopausal
status |
|
|
|
|
|
|
|
|
Premenopausal | 98 (58.7) | 59 (56.7) | 39 (61.9) | 0.338 | 50 (51.5) | 48 (68.6) | 0.889 |
|
Postmenopausal | 69 (41.3) | 45 (43.3) | 24 (38.1) |
| 47 (48.5) | 22 (31.4) |
|
| BMI |
|
|
|
|
|
|
|
|
<23 | 70 (41.9) | 44 (42.3) | 26 (41.3) | 0.312 | 33 (34.0) | 37 (52.9) | 0.093 |
|
≥23 | 97 (58.1) | 60 (57.7) | 37 (58.7) |
| 64 (66.0) | 33 (47.1) |
|
| Nuclear grade |
|
|
|
|
|
|
|
| 1 | 10 (6.0) | 6 (5.8) | 4 (6.3) | 0.147 | 6 (6.2) | 4 (5.7) | 0.218 |
| 2 | 99 (59.3) | 65 (62.5) | 34 (54.0) |
| 63 (64.9) | 36 (51.4) |
|
| 3 | 58 (34.7) | 33 (31.7) | 25 (39.7) |
| 28 (28.9) | 30 (42.9) |
|
| Histological
grade |
|
|
|
|
|
|
|
| 1 | 28 (16.8) | 18 (17.3) | 10 (15.9) | 0.357 | 23 (23.8) | 5 (7.1) | 0.045 |
| 2 | 88 (52.7) | 53 (51.0) | 35 (55.5) |
| 50 (51.5) | 38 (54.3) |
|
| 3 | 51 (30.5) | 33 (31.7) | 18 (28.6) |
| 24 (24.7) | 27 (38.6) |
|
| Tumor size |
|
|
|
|
|
|
|
| T1 | 66 (39.5) | 37 (35.6) | 29 (46.0) | 0.145 | 43 (44.3) | 23 (32.8) | 0.828 |
| T2 | 97 (58.1) | 65 (62.5) | 32 (50.8) |
| 52 (53.6) | 45 (64.3) |
|
| T3 | 4 (2.4) | 2 (1.9) | 2 (3.2) |
| 2 (2.1) | 2 (2.9) |
|
| Lymph node
metastasis |
|
|
|
|
|
|
|
| N0 | 92 (55.1) | 58 (55.7) | 34 (54.0) | 0.782 | 60 (61.9) | 32 (45.7) | 0.193 |
| N1 | 44 (26.3) | 29 (27.9) | 15 (23.8) |
| 23 (23.7) | 21 (30.0) |
|
| N2 | 20 (12.0) | 11 (10.6) | 9 (14.3) |
| 10 (10.3) | 10 (14.3) |
|
| N3 | 11 (6.6) | 6 (5.8) | 5 (7.9) |
| 4 (4.1) | 7 (10.0) |
|
| Subtype |
|
|
|
|
|
|
|
| Luminal
A | 86 (51.5) | 50 (48.1) | 36 (57.1) | 0.670 | 51 (52.6) | 35 (50.0) | 0.842 |
| Luminal
B | 21 (12.6) | 12 (11.5) | 9 (14.3) |
| 14 (14.4) | 7 (10.0) |
|
|
HER-2 | 24 (14.4) | 19 (18.3) | 5 (7.9 |
| 11 (11.3) | 13 (18.6) |
|
|
TNBC | 36 (21.5) | 23 (22.1) | 13 (20.7 |
| 21 (21.7) | 15 (21.4) |
|
| IGF-1R
expression |
|
|
|
|
|
|
|
| Low
(0,1) | 104 (62.3) | 104 (100.0) | 0 (0.0) |
| 68 (70.1) | 36 (51.4) | 0.021 |
| High
(2,3) | 63 (37.7) | 0 (0.0) | 63 (100.0) |
| 29 (29.9) | 34 (48.6) |
|
| Dense breast
tissue |
|
|
|
|
|
|
|
|
Negative | 97 (58.1) | 68 (65.4) | 29 (46.0) | 0.021 | 97 (100.0) | 0 (0.0) |
|
|
Positive | 70 (41.9) | 36 (34.6) | 34 (54.0) |
| 0 (0.0) | 70 (100.0) |
|
| Table II.Correlation of insulin-like growth
factor 1 receptor (IGF-1R) expression and mammographic breast
density with breast cancer-related biomarkers. |
Table II.
Correlation of insulin-like growth
factor 1 receptor (IGF-1R) expression and mammographic breast
density with breast cancer-related biomarkers.
|
|
| IGF-1R
expression | Dense breast
tissue |
|---|
|
|
|
|
|
|---|
|
|
| Low | High | Negative | Positive |
|
|---|
|
|
|
|
|
|
|---|
| Biomarkers | Total (%)
(n=167) | No. (%)
(n=104) | No. (%) (n=63) | P-value | No. (%) (n=97) | No. (%) (n=70) | P-value |
|---|
| ER |
|
|
|
|
|
|
|
|
Negative | 63 (37.7) | 44 (42.3) | 19 (30.2) | 0.301 | 34 (35.1) | 29 (41.4) | 0.855 |
|
Positive | 104 (62.3) | 60 (57.7) | 44 (69.8) |
| 63 (64.9) | 41 (58.6) |
|
| PR |
|
|
|
|
|
|
|
|
Negative | 95 (56.9) | 62 (59.6) | 33 (52.4) | 0.845 | 49 (50.5) | 46 (65.7) | 0.059 |
|
Positive | 72 (43.1) | 42 (40.4) | 30 (47.6) |
| 48 (49.5) | 24 (34.3) |
|
| HER-2 |
|
|
|
|
|
|
|
|
Negative | 122 (73.1) | 73 (70.2) | 49 (77.8) | 0.215 | 72 (74.2) | 50 (71.4) | 0.405 |
|
Positive | 45 (26.9) | 31 (29.8) | 14 (22.2) |
| 25 (25.8) | 20 (28.6) |
|
| EGFR |
|
|
|
|
|
|
|
|
Negative | 141 (84.4) | 86 (82.7) | 55 (87.3) | 0.980 | 83 (85.6) | 58 (82.9) | 0.958 |
|
Positive | 26 (15.6) | 18 (17.3) | 8 (12.7) |
| 14 (14.4) | 12 (17.1) |
|
| CK 5/6 |
|
|
|
|
|
|
|
|
Negative | 156 (93.4) | 97 (93.3) | 59 (93.7) | 0.812 | 90 (92.8) | 66 (94.3) | 0.194 |
|
Positive | 11 (6.6) | 7 (6.7) | 4 (6.3) |
| 7 (7.2) | 4 (5.7) |
|
| Ki-67 |
|
|
|
|
|
|
|
| Low,
<10% | 123 (73.7) | 72 (69.2) | 51 (81.0) | 0.160 | 73 (75.3) | 50 (71.4) | 0.947 |
| High,
≥10% | 44 (26.3) | 32 (30.8) | 12 (19.0) |
| 24 (24.7) | 20 (28.6) |
|
The density patterns on mammography were non-dense
breast tissue (grades 1 and 2) in 97 patients (58.1%) and dense
breast tissue in 70 patients (41.9%). The frequency of dense breast
tissue according to age was 100% (20–29 years), 70% (30–39 years),
40.3% (40–49 years), 43.8% (50–59 years), 10.6% (60–69 years) and
0% (70–89 years) (data not shown). Dense breast tissue was
significantly associated with age, body mass index (BMI),
menopausal status, histological grade and IGF-1R overexpression in
the univariate analysis and with age (P=0.001), histological grade
(P=0.045) and IGF-1R overexpression (P=0.021) in the multivariate
analysis (Tables I and II).
IGF-1R expression was scored as 0 in 34 patients
(20.4%), 1 in 70 patients (41.9%), 2 in 60 patients (35.9%) and 3
in 3 patients (1.8%). The frequency of IGF-1R overexpression
according to age was 0% (20–29 years), 34.5% (30–39 years), 45.2%
(40–49 years), 37.8% (50–59 years), 31.6% (60–69 years), 16.7%
(70–79 years) and 0% (80–89 years) (data not shown). IGF-1R
overexpression was significantly associated with dense breast
tissue at ages >40 years (P=0.002). Overexpression of IGF-1R was
identified in 63 patients (37.7%), but exhibited no correlation
with any clinicopathological parameters, such as age, BMI, primary
tumour size, nuclear grade, histological grade, lymph node
metastasis, ER, PR, HER-2, EGFR and Ki-67 (Tables I and II).
ER expression (P=0.010, odds ratio=0.516) was
associated with DFS and nuclear grade (P=0.029, odds ratio=0.068),
histologic grade (P=0.019, odds ratio=16.318), lymph node
metastasis (P=0.014, odds ratio=3.140) and ER expression (P=0.016,
odds ratio=0.041) were associated with OS (Table III). There was no significant
difference in OS and DFS between dense and non-dense breast tissue
(Fig. 3). IGF-1R overexpression in
breast cancer in premenopausal women was associated with HER-2
positivity (P~0.016) and worse DFS (P=0.0414) (Fig. 4).
| Table III.Cox's proportional hazards regression
models for overall survival (OS) and disease-free survival
(DFS). |
Table III.
Cox's proportional hazards regression
models for overall survival (OS) and disease-free survival
(DFS).
|
|
| OS | DFS |
|---|
|
|
|
|
|
|---|
| Variables | No. | RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| Dense breast
tissue |
|
|
|
|
|
|
|
|
Negative | 97 | 0.647 | 0.138–3.424 | 0.647 | 1.175 | 0.816–1.692 | 0.387 |
|
Positive | 70 |
|
|
|
|
|
|
| Nuclear grade |
|
|
|
|
|
|
|
| 1 | 10 | 0.068 | 0.006–0.759 | 0.029 | 1.086 | 0.694–1.699 | 0.719 |
| 2 | 99 |
|
|
|
|
|
|
| 3 | 58 |
|
|
|
|
|
|
| HistologicAL
grade |
|
|
|
|
|
|
|
| 1 | 28 | 16.318 | 1.571–169.479 | 0.019 | 0.774 | 0.539–1.113 | 0.167 |
| 2 | 88 |
|
|
|
|
|
|
| 3 | 51 |
|
|
|
|
|
|
| Tumor size |
|
|
|
|
|
|
|
| T1 | 66 | 0.327 | 0.327–6.331 | 0.630 | 0.799 | 0.571–1.117 | 0.190 |
| T2 | 97 |
|
|
|
|
|
|
| T3 | 4 |
|
|
|
|
|
|
| LN metastasis |
|
|
|
|
|
|
|
| N0 | 92 | 3.140 | 1.255–7.857 | 0.014 | 1.218 | 0.986–1.505 | 0.068 |
| N1 | 44 |
|
|
|
|
|
|
| N2 | 20 |
|
|
|
|
|
|
| N3 | 11 |
|
|
|
|
|
|
| ER |
|
|
|
|
|
|
|
|
Negative | 63 | 0.041 | 0.003–0.549 | 0.016 | 0.516 | 0.312–0.854 | 0.010 |
|
Positive | 104 |
|
|
|
|
|
|
| PR |
|
|
|
|
|
|
|
|
Negative | 95 | 6.908 | 0.552–86.498 | 0.134 | 0.820 | 0.526–1.277 | 0.379 |
|
Positive | 72 |
|
|
|
|
|
|
| HER-2 |
|
|
|
|
|
|
|
|
Negative | 122 | 0.940 | 0.177–4.995 | 0.940 | 0.882 | 0.581–1.340 | 0.557 |
|
Positive | 45 |
|
|
|
|
|
|
| EGFR |
|
|
|
|
|
|
|
|
Negative | 141 | 0.000 | 0.000 | 0.983 | 0.663 | 0.382–1.151 | 0.144 |
|
Positive | 26 |
|
|
|
|
|
|
| CK 5/6 |
|
|
|
|
|
|
|
|
Negative | 156 | 0.001 | 0.000 | 0.993 | 1.476 | 0.672–3.242 | 0.333 |
|
Positive | 11 |
|
|
|
|
|
|
| Ki-67, % |
|
|
|
|
|
|
|
| Low
(<10) | 123 | 7.922 | 0.460–136.514 | 0.154 | 1.345 | 0.891–2.030 | 0.158 |
| High
(≥10) | 44 |
|
|
|
|
|
|
| IGF-1R |
|
|
|
|
|
|
|
| Low
(0,1) | 104 | 1.093 | 0.176–6.795 | 0.924 | 0.928 | 0.637–1.353 | 0.698 |
| High
(2,3) | 63 |
|
|
|
|
|
|
Discussion
The earlier detection rate of breast cancer is
continuously increasing, as a result of the growing public interest
in breast cancer and the wider application of selective
mammographic screening. However, increased breast density makes it
more difficult to detect tumours in women exhibiting dense breast
tissue on mammography; in addition, the presence of dense breast
tissue per se is known to be associated with an increased
risk of breast cancer. It was reported that alternative hormonal
therapy, particularly estrogen-progestin complex therapy, increased
the frequency of dense breast tissue and, thus, the risk of breast
cancer (19). The administration of
hormonal inhibitors, such as tamoxifen, decreased the recurrence
rates of breast cancer as well as breast tissue density, further
suggesting that increased breast tissue density constitutes a risk
factor for breast cancer (20).
In this study, the BI-RADS classification, which is
widely in use today, was adopted for analyzing mammographic
density. Although this is a semi-quantitative method, rather than a
quantitative measurement, similar to the computer-assisted breast
density assessment, it has been found to be close to a quantitative
method, exhibiting high consistency rates in terms of intra- and
inter-observer variability. According to comparative studies on
different mammographic readings, no significant difference was
found between the BI-RADS-based group and the other group using
computer-based calculation of absolute areas in terms of several
clinicopathological factors (21,22). In
view of mammographic timing, screening at a certain point in time
during the menstrual cycle possibly ensures a more accurate
measurement of density; however, in the majority of the cases,
density does not vary significantly depending on different points
of time during the menstrual cycle. The reason for reading the
tumour-free parts is to avoid having the reading affected by the
radio-opacity of most tumours. Assessing the density of one breast
only instead of both sides may lower the accuracy of the density
measurement, although the high consistency in density between the
two breasts prevents against wrongful density classification
(4,23).
The univariate analysis identified factors such as
age, BMI, menopausal status and histological grade as relevant to
dense breast tissue, whereas the multivariate analysis demonstrated
the relevance of age and histological grade. In this study, the
univariate analysis demonstrated that dense breast tissue was a
more frequent finding in pre- rather than postmenopausal women,
whereas the multivariate analysis found no such relevance,
suggesting that age rather than menopausal status is more
significant. In terms of BMI, the univariate analysis identified an
inverse correlation between increased BMI and frequency of dense
breast tissue, whereas the multivariate analysis demonstrated no
significant correlation. Age was found to be inversely correlated
with dense breast tissue. In an autopsy study by Li et al
(24), density was found to be high
when cell nuclei occupied large areas, whereas nuclear grade was
nots found to be associated with dense breast tissue in the present
study. However, histological grade was found to be related to
increased breast tissue density, which requires further
investigation. It was reported that ER-positive compared to
negative tumours were more frequently associated with dense breast
tissue. By contrast, breast tissue density was not associated with
the expression of ER in the present study, which is consistent with
the findings of with Ghosh et al (22). This study reported that the
overexpression of IGF-1R may be significantly associated with dense
breast tissue on mammography.
IGF-1 in the blood is considered to be an important
factor affecting breast tissue density. Anti-estrogens administered
to patients with high IGF-1 in the blood reduced IGF-1 levels and
breast tissue density, indicating that IGF-1 affects breast density
(25,26). The concentration of IGF-1 in the
blood, as well as breast density, is known to decrease with age.
However, dense breast tissue becomes less frequent with age, while
the incidence of breast cancer gradually increases, indicating that
other factors may be involved. To assess the relevance to breast
tissue density more accurately, it is crucial to investigate the
expression of IGF-1R in tissues in lieu of IGF-1 in the blood, on
which no study results have been reported thus far. The
concentration of IGF-1 in the blood is known to decrease with age,
whereas IGF-1R overexpression in this study was found to increase
up to the age of 40 years and decrease thereafter, indicating
differences from the expression in actual cancer tissues. As
regards age, IGF-1R overexpression was found in women in their 4th
and 5th decades of life, which represents a similar distribution in
the age groups prone to breast cancer among Korean women. The
present study found that the overexpression of IGF-1R in the breast
cancer tissues of women aged ≥40 years was associated with the
presence of dense breast tissue on mammography. Based on this
finding, IGF-1R overexpression appears to play an important role in
breast cancer patients with dense breast tissue. Based on reports
that IGF-1 and IGF-1R expression varies across ethnic groups,
ethnicity-based correlations between dense breast tissue and IGF-1R
overexpression should be investigated, in order to elucidate the
effect of IGF-1R overexpression on breast cancer patients with
dense breast tissue (27,28).
IGF-1R is associated with several types of cancer,
including breast and prostate cancer. The signaling stages of
IGF-1R are crucial for the normal development of mammary tissues
and play an important role in mitosis and anti-apoptosis. The
self-phosphorylation of IGF-1R, the phosphorylation of insulin
receptor substrates (IRS) 1–4 by tyrosine kinase and the activation
of phosphoinositide 3-kinase (PI3K)/Akt/mammalian target of
rapamycin (mTOR) signaling system play important roles in the
differentiation and survival of tumour cells (29). To determine IGF-1R expression and the
mechanism underlying its effects, it is necessary to examine the
IRS that function as a signaling system of IGF-1R, SHC (leading to
Ras/Raf/mitogen activated protein kinase cascade) and PI3K, along
with the expression of downstream signaling molecules, such as
mTOR, activated by PI3K. Recently, IGF-1R overexpression was
reported to contribute to resistance to tamoxifen, chemotherapy,
Herceptin and radiotherapy. Therefore, it is necessary to predict
the resistance to treatment of a mammographically dense breast and
investigate the administration of agents to manage resistant cases
(30,31).
As regards the expression of IGF-1R as a prognostic
factor, Kim et al (17)
reported that, in Korean breast cancer patients, IGF-1R expression
was associated with high DFS (P=0.026) and 5-year survival rates
(P=0.019), which were favourable prognostic factors. This finding
was attributable to the correlation of IGF-1R overexpression to
ER-positive and HER-2-negative tumours, which was considered as a
good prognostic factor. By contrast, the present study found no
correlation with ER status (12).
Similar to the results of Shimizu et al (15) there was no observed correlation with
age, tumour size, lymph node metastasis, histological grade,
hormone receptor status and OS rates in this study. The present
study found no factors associated with the relevance between
IGF-1R, clinicopathological characteristics and biomarkers, in
agreement with the results of Taunk et al (32), who reported that, in a group without
lymph node metastasis, IGF-1R overexpression was associated with
low survival rates. By contrast, the present study found no effect
of IGF-1R overexpression on OS rates, irrespective of lymph node
metastasis.
The overexpression of IGF-1R in premenopausal women
was found to be relevant to HER-2 positivity with low DFS,
indicating that IGF-1R overexpression in premenopausal women may
represent an unfavorable prognostic factor. In the subgroup
analysis based on the overexpression of IGF-1R and the
presence/absence of dense breast tissue, the concomitant occurrence
of IGF-1R overexpression and dense breast tissue in premenopausal
women was associated with a lower DFS (P=0.0154) and may be
considered as an unfavorable prognostic factor compared to those
with no such concomitant characteristics. Several recent studies
reported IGF-1R overexpression to be an unfavorable prognostic
factor, but the results were inconsistent, which warrants further
investigation (15,17,18,32,33).
ER (P=0.010) was the factor found to affect patients' DFS rate,
whereas nuclear grade (P=0.029), histological grade (P=0.019), ER
(P=0.016) and lymph node metastasis (P=0.014) were associated with
OS, which is in agreement with the common prognostic factors of
breast cancer. Survival rates did not vary according to tumour
subtypes. The present study investigated the frequency of IGF-1R
overexpression in breast cancer tissues and the frequency of
mammographic dense breast tissue, in order to analyze the
correlations between the two. Further studies are required
investigating IGF-1R expression in reference to density of normal
breast tissues as well as cancer tissues, in order to elucidate the
effect of IGF-1R on breast density.
In conclusion, IGF-1R expression in breast cancer
tissue was found to be significantly associated with mammographic
breast density in patients aged >40 years. It Appears that
IGF-1R expression in breast cancer plays an important role in cases
with dense breast tissue. In premenopausal women, IGF-1R
overexpression in breast cancer tissue was significantly associated
with HER-2 positivity and poor DFS. However, IGF-1R overexpression
in this study exhibited no correlation with other
clinicopathological parameters. Dense breast tissue was found to be
associated with age and histological grade. There was no difference
in DFS and OS according to breast density.
References
|
1
|
Couzin J: Breast cancer. Dissecting a
hidden breast cancer risk. Science. 309:1664–1666. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ursin G, Ma H, Wu AH, Bernstein L, Salane
M, Parisky YR, Astrahan M, Siozon CC and Pike MC: Mammographic
density and breast cancer in three ethnic groups. Cancer Epidemiol
Biomarkers Prev. 12:332–338. 2003.PubMed/NCBI
|
|
3
|
Maskarinec G, Pagano I, Lurie G, Wilkens
LR and Kolonel LN: Mammographic density and breast cancer risk: The
multiethnic cohort study. Am J Epidemiol. 162:743–752. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Diorio C, Pollak M, Byrne C, Mâsse B,
Hébert-Croteau N, Yaffe M, Coté G, Bérubé S, Morin C and Brisson J:
Insulin-like growth factor-I, IGF-binding protein-3, and
mammographic breast density. Cancer Epidemiol Biomarkers Prev.
14:1065–1073. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bremnes Y, Ursin G, Bjurstam N, Rinaldi S,
Kaaks R and Gram IT: Insulin-like growth factor and mammographic
density in postmenopausal Norwegian women. Cancer Epidemiol
Biomarkers Prev. 16:57–62. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Grimberg A and Cohen P: Role of
insulin-like growth factors and their binding proteins in growth
control and carcinogenesis. J Cell Physiol. 183:1–9. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Guo YP, Martin LJ, Hanna W, Banerjee D,
Miller N, Fishell E, Khokha R and Boyd NF: Growth factors and
stromal matrix proteins associated with mammographic densities.
Cancer Epidemiol Biomarkers Prev. 10:243–248. 2001.PubMed/NCBI
|
|
8
|
Sarfstein R, Maor S, Reizner N,
Abramovitch S and Werner H: Transcriptional regulation of the
insulin-like growth factor-I receptor gene in breast cancer. Mol
Cell Endocrinol. 252:241–246. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Miller BS and Yee D: Type I insulin-like
growth factor receptor as a therapeutic target in cancer. Cancer
Res. 65:10123–10127. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hartog H, Wesseling J, Boezen HM and van
der Graaf WT: The insulin-like growth factor 1 receptor in cancer:
Old focus, new future. Eur J Cancer. 43:1895–1904. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Happerfield LC, Miles DW, Barnes DM,
Thomsen LL, Smith P and Hanby A: The localization of the
insulin-like growth factor receptor 1 (IGFR-1) in benign and
malignant breast tissue. J Pathol. 183:412–417. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bhargava R, Beriwal S, McManus K and Dabbs
DJ: Insulin-like growth factor receptor-1 (IGF-1R) expression in
normal breast, proliferative breast lesions, and breast carcinoma.
Appl Immunohistochem Mol Morphol. 19:218–225. 2011.PubMed/NCBI
|
|
13
|
Ouban A, Muraca P, Yeatman T and Coppola
D: Expression and distribution of insulin-like growth factor-1
receptor in human carcinomas. Hum Pathol. 34:803–808. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yanochko GM and Eckhart W: Type I
insulin-like growth factor receptor over-expression induces
proliferation and anti-apoptotic signaling in a three-dimensional
culture model of breast epithelial cells. Breast Cancer Res.
8:R182006. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Shimizu C, Hasegawa T, Tani Y, Takahashi
F, Takeuchi M, Watanabe T, Ando M, Katsumata N and Fujiwara Y:
Expression of insulin-like growth factor 1 receptor in primary
breast cancer: Immunohistochemical analysis. Hum Pathol.
35:1537–1542. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chong YM, Williams SL, Elkak A, Sharma AK
and Mokbel K: Insulin-like growth factor 1 (IGF-1) and its receptor
mRNA levels in breast cancer and adjacent non-neoplastic tissue.
Anticancer Res. 26:167–173. 2006.PubMed/NCBI
|
|
17
|
Kim JH, Cho YH, Park YL, Sohn JH and Kim
HS: Prognostic significance of insulin growth factor-I receptor and
insulin growth factor binding protein-3 expression in primary
breast cancer. Oncol Rep. 23:989–995. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Creighton CJ, Casa A, Lazard Z, Huang S,
Tsimelzon A, Hilsenbeck SG, Osborne CK and Lee AV: Insulin-like
growth factor-I activates gene transcription programs strongly
associated with poor breast cancer prognosis. J Clin Oncol.
26:4078–4085. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bock K, Hadji P, Duda VF, Jackisch C and
Wagner U: Mammographic breast density and breast cancer risk during
HRT. Zentralbl Gynakol. 127:217–221. 2005.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Martin LJ, Minkin S and Boyd NF: Hormone
therapy, mammographic density, and breast cancer risk. Maturitas.
64:20–26. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ding J, Warren R, Girling A, Thompson D
and Easton D: Mammographic density, estrogen receptor status and
other breast cancer tumor characteristics. Breast J. 16:279–289.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ghosh K, Brandt KR, Sellers TA, Reynolds
C, Scott CG, Maloney SD, Carston MJ, Pankratz VS and Vachon CM:
Association of mammographic density with the pathology of
subsequent breast cancer among postmenopausal women. Cancer
Epidemiol Biomarkers Prev. 17:872–879. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Harvey JA and Bovbjerg VE: Quantitative
assessment of mammographic breast density: Relationship with breast
cancer risk. Radiology. 230:29–41. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li T, Sun L, Miller N, Nicklee T, Woo J,
Hulse-Smith L, Tsao MS, Khokha R, Martin L and Boyd N: The
association of measured breast tissue characteristics with
mammographic density and other risk factors for breast cancer.
Cancer Epidemiol Biomarkers Prev. 14:343–349. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pollak M: IGF-I physiology and breast
cancer. Recent Results Cancer Res. 152:63–70. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Meggiorini ML, Labi L, Vestri AR, Porfiri
LM, Savelli S and De Felice C: Tamoxifen in women with breast
cancer and mammographic density. Eur J Gynaecol Oncol. 29:598–601.
2008.PubMed/NCBI
|
|
27
|
Pinheiro SP, Holmes MD, Pollak MN,
Barbieri RL and Hankinson SE: Racial differences in premenopausal
endogenous hormones. Cancer Epidemiol Biomarkers Prev.
14:2147–2153. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kalla Singh S, Tan QW, Brito C, De León M
and De León D: Insulin-like growth factors I and II receptors in
the breast cancer survival disparity among African-American women.
Growth Horm IGF Res. 20:245–254. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Rozengurt E, Sinnett-Smith J and Kisfalvi
K: Crosstalk between insulin/insulin-like growth factor-1 receptors
and G protein-coupled receptor signaling systems: A novel target
for the antidiabetic drug metformin in pancreatic cancer. Clin
Cancer Res. 16:2505–2511. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nahta R, Yuan LX, Zhang B, Kobayashi R and
Esteva FJ: Insulin-like growth factor-I receptor/human epidermal
growth factor receptor 2 heterodimerization contributes to
trastuzumab resistance of breast cancer cells. Cancer Res.
65:11118–11128. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chong K, Subramanian A, Sharma A and
Mokbel K: Measuring IGF-1, ER-α and EGFR expression can predict
tamoxifen-resistance in ER-positive breast cancer. Anticancer Res.
31:23–32. 2011.PubMed/NCBI
|
|
32
|
Taunk NK, Goyal S, Moran MS, Yang Q,
Parikh R and Haffty BG: Prognostic significance of IGF-1R
expression in patients treated with breast-conserving surgery and
radiation therapy. Radiother Oncol. 96:204–208. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kostopoulos I, Arapantoni-Dadioti P, Gogas
H, et al: Evaluation of the prognostic value of HER-2 and VEGF in
breast cancer patients participating in a randomized study with
dose-dense sequential adjuvant chemotherapy. Breast Cancer Res
Treat. 96:251–261. 2006. View Article : Google Scholar : PubMed/NCBI
|