Introduction
S-1, is an oral fluoropyrimidine anticancer agent
that was developed in Japan and was approved as an effective drug
for gastric cancer in 1999. This agent combines tegafur, a prodrug
of 5-Fluorouracil (5-FU), with gimeracil, a reversible antagonist
of the rate-limiting enzyme in the 5-FU degradation pathway and
oteracil potassium, a reversible inhibitor of the phosphoenzyme of
5-FU that reduces gastric toxicity, in order to increase the
concentration of 5-FU in the blood, thereby enhancing antitumor
efficacy but reducing gastric toxicity that typically occurs with
increased concentrations (1). The
response rates for single-agent S-1 in advanced recurrent gastric
cancer were 53.6% (15/28) and 44.6% (45/101) in an early phase II
and late phase II trial, respectively. S-1 has been widely used as
first-line treatment for gastric cancer and has the highest
response rate among anticancer drugs indicated for gastric cancer
(2–5).
In 2006, the results of an interim analysis of a
clinical trial in patients undergoing resection for gastric cancer,
namely the Adjuvant Chemotherapy Trial of S-1 for Gastric Cancer
(ACTS-GC), were presented in order to report the benefits of
S-1-based adjuvant chemotherapy following surgery in gastric cancer
(6). This study was conducted using a
4-week administration schedule for S-1 followed by a 2-week rest
period in patients with stage II (excluding T1), IIIA or IIIB
gastric cancer who underwent curative R0 or R1 resection with no
residual tumor by standard gastric cancer surgery (D2 lymph node
dissection). In the group where the treatment regimen was
administration of S-1 for 4 weeks followed by 2 weeks of rest,
which was continued for 1 year, the risk of death was reduced by
32% and The survival rates at 3 years POST-surgery were 70.1 and
80.5% in the surgery-alone and S-1 groups, respectively,
demonstrating a survival benefit with S-1 treatment. With the most
frequent ≥Grade 3 adverse event being anorexia at 5.7%,
postoperative adjuvant chemotherapy with S-1 has become the
standard treatment for patients with stage II or III gastric cancer
undergoing curative resection. However, compliance to the S-1
treatment is far from ideal, with 87.4% of the patients compliant
at 3 months, 77.9% at 6 months, 70.8% at 9 months and 65.8% at 12
months. Studies investigating alternative dosing regimens to fully
exploit the efficacy of S-1 while reducing adverse reactions are
required.
A feasibility study of S-1 as postoperative adjuvant
chemotherapy using a 2-week administration regimen followed by a
1-week rest period was previously conducted in locally advanced
squamous cell carcinoma of the head and neck (SCCHN) in order to
increase the compliance to the S-1 therapy. In that study,
treatment of scchn with S-1 was continued for 6 months as a 2-week
administration/1-week rest (2-week/1-week) regimen or a 4-week
administration/2-week rest (4-week/2-week) regimen. The treatment
completion rate was reported to be 40 and 29.4%, the ratio of S-1
relative cumulative dose 54.9 and 34.3% and the frequency of ≥Grade
3 adverse events 8 and 17.6% for the 2-week/1-week and
4-week/2-week regimens, respectively (7). These results suggested that the
reduction of adverse events by using the 2-week/1-week regimen
exerted a significant positive effect on the completion rate of S-1
treatment. However, no distinct evidence associated with the
efficacy of the 2-week/1-week regimen as postoperative adjuvant
chemotherapy in gastric cancer has been reported.
We conducted a multicenter, randomized clinical
trial to investigate the completion rate of treatment using the
4-week/2-week regimen and the 2-week/1-week regimen as
postoperative adjuvant chemotherapy with S-1 in order to establish
a safer postoperative adjuvant chemotherapy regimen while achieving
higher treatment compliance in gastric cancer patients.
Patients and methods
Patients
Among The patients who underwent R0 or R1 surgical
resection for stage II (excluding T1), IIIA or IIIB gastric cancer
between May, 2008 and February, 2010, 47 patients were enrolled in
this study.
Treatment schedule
The patients were randomly assigned to arm A
(4-week/2-week treatment regimen arm; N=25); and arm B
(2-week/1-week treatment regimen arm; N=22), with the goal of
administering S-1 for 1 year. In arm A (4-week/2-week arm), S-1 was
orally administered twice a day (after breakfast and dinner) for 28
consecutive days, followed by a 14-day rest period, as a 6-week (42
days) course for a total of 1 year. In arm B (2-week/1-week arm),
S-1 was orally administered twice a day (after breakfast and
dinner) for 14 consecutive days, followed by a 7-day rest period as
a 3-week (21 days) course for a total of 1 year (Fig. 1). The initial dose of S-1 was
determined based on The estimated creatinine clearance calculated
using the Cockcroft-Gault formula and using age, body weight and
serum creatinine at baseline and body surface area. Patients with a
body surface area of <1.25 m2 received 80 mg daily;
those with a body surface area of 1.25 m2 to <1.5
m2 received 100 mg daily; and those with a body surface
area of ≥1.5 m2 received 120 mg daily.
Toxicity
In the event of toxicity [National Cancer Institute
Common Toxicity Criteria (NCI-CTC) version 3.0], the following
treatment delays and dose reductions were planned: S-1
administration on day 1 in subsequent cycles was delayed when there
was a leukocyte count <2,000/mm3; neutrophil count
<1,000/mm3; platelet count <75,000/mm3;
aspartate aminotransferase (AST) and alanine aminotransferase (ALT)
levels >150 IU/l; and serum creatinine >1.5 mg/dl. If these
toxicities exhibited a causal relationship with S-1, or in cases
with creatinine clearance ≥50 to <80 ml/min prior to the
initiation of a new course, the daily dose of S-1 was reduced from
120–100 mg, from 100–80 mg or from 80–50 mg twice daily, but the
minimal daily dose was maintained at 40 mg twice daily. Treatment
was continued until disease progression, unacceptable toxicity,
patient refusal or physician decision.
Inclusion criteria
The eligibility criteria for patient enrollment were
as follows: i) Patients who had pathologically confirmed gastric
cancer; ii) patients who underwent R0 or R1 surgical resection with
D2 or more extended lymph node dissection; iii) patients with stage
II (excluding T1), IIIA or IIIB gastric cancer based on
comprehensive findings; iv) patients aged 20–75 years at
enrollment; v) patients who had not undergone pretreatment other
than surgical treatment (radiological, chemical and/or hormonal
therapy); vi) patients who were able to tolerate oral
administration within 6 weeks after surgery; vii) patients who had
no severe postoperative complications and met the following
criteria for postoperative laboratory parameters: white blood cell
count ≥4,000/mm3 and <12,000/mm3;
neutrophil count ≥2,000/mm3; platelet count
≥10×104/mm3; hemoglobin ≥9.0 g/dl; total
bilirubin ≤1.5 mg/dl; AST (SGOT) and ALT (SGPT) <100 IU/l; serum
creatinine ≤upper limit of the institutional standard; creatinine
clearance based on the Cockcroft-Gault formula ≥50 ml/min; and
viii) patients who provided written informed consent.
Exclusion criteria
The exclusion criteria were as follows: i) Patients
with simultaneous or metachronous double/multiple cancers; ii)
patients with contraindications to S-1 treatment; iii) patients
requiring use of flucytosine, phenytoin and warfarin potassium; iv)
patients with a history of ≥Grade 3 drug allergy; v) patients with
severe complication(s), such as intestinal paresis, ileus,
interstitial pneumonia or pulmonary fibrosis, uncontrolled
diabetes, heart, renal and/or hepatic failure; vi) patients with
diarrhea; vii) pregnant women, lactating women and women intending
to become pregnant; viii) men who intend to reproduce; ix) human
immunodeficiency virus-positive patients; and x) patients who were
considered by the investigator or subinvestigator to be unsuitable
for this study.
The classification of pathological stage for
resected tumors was based on the Japanese classification of gastric
carcinoma (8).
Approval for implementing this study was obtained
from The Institutional Review Boards of Okayama University and
Kawasaki Medical School. Written informed consent was provided from
all the participating subjects.
Statistical methods
The primary endpoint was the treatment completion
rate in stage II and III gastric cancer treated with the
4-week/2-week or 2-week/1-week regimen of S-1 as adjuvant
chemotherapy. The sample size was estimated to be 57 to correctly
select a better treatment with probability (P=0.95) based on the
expectation that a 15% difference would be observed in the
treatment completion rate between the two arms. Taking ineligible
patients into account, the sample size was set at 60 for each arm.
Safety (NCI-CTC version 3.0), relapse-free survival and overall
survival were observed as secondary endpoints. Completion rate was
calculated by dividing the number of patients who continued
treatment by the total number of patients. The relapse-free
survival was defined as the time from the date of registration to
the date of confirmed recurrence or death from any cause, rather
than the date of treatment discontinuation. The overall survival
was defined as the time interval from the date of registration to
the date of death from any cause. Survival curves were estimated
using the Kaplan-Meier method and differences were analyzed using
the stratified log-rank test.
Results
Patient characteristics
Enrollment in this study was completed at the end of
February, 2010. The baseline characteristics of the patients are
summarized in Table I. There was no
significant difference in any characteristic between the two arms.
Subsequently, an analysis of data was initiated to evaluate the
completion rates of treatment.
 | Table I.Baseline characteristics of the
patients. |
Table I.
Baseline characteristics of the
patients.
| Characteristics | Arm Aa (n=25) | Arm Bb (n=21) |
|---|
| Age, year |
|
|
|
Median | 65 | 61 |
|
Range | 43–73 | 46–80 |
| Gender (%) |
|
|
| Male | 19 (76.0) | 17 (80.9) |
|
Female | 6 (24.0) | 4 (19.1) |
| Depth of tumor
invasion (%) |
|
|
| T1 | 0 (0) | 0 (0) |
| T2 | 14 (56.0) | 11 (52.4) |
| T3 | 11 (44.0) | 10 (47.6) |
| T4 | 0 (0) | 0 (0) |
| Lymph node metastasis
(%) |
|
|
| N0 | 4 (16.0) | 3 (14.3) |
| N1 | 11 (44.0) | 11 (52.4) |
| N2 | 10 (40.0) | 7 (33.3) |
| N3 | 0 (0) | 0 (0) |
| Pathological stage
(%) |
|
|
| II | 10 (40.0) | 10 (47.6) |
| IIIA | 9 (36.0) | 8 (38.1) |
| IIIB | 6 (24.0) | 3 (14.3) |
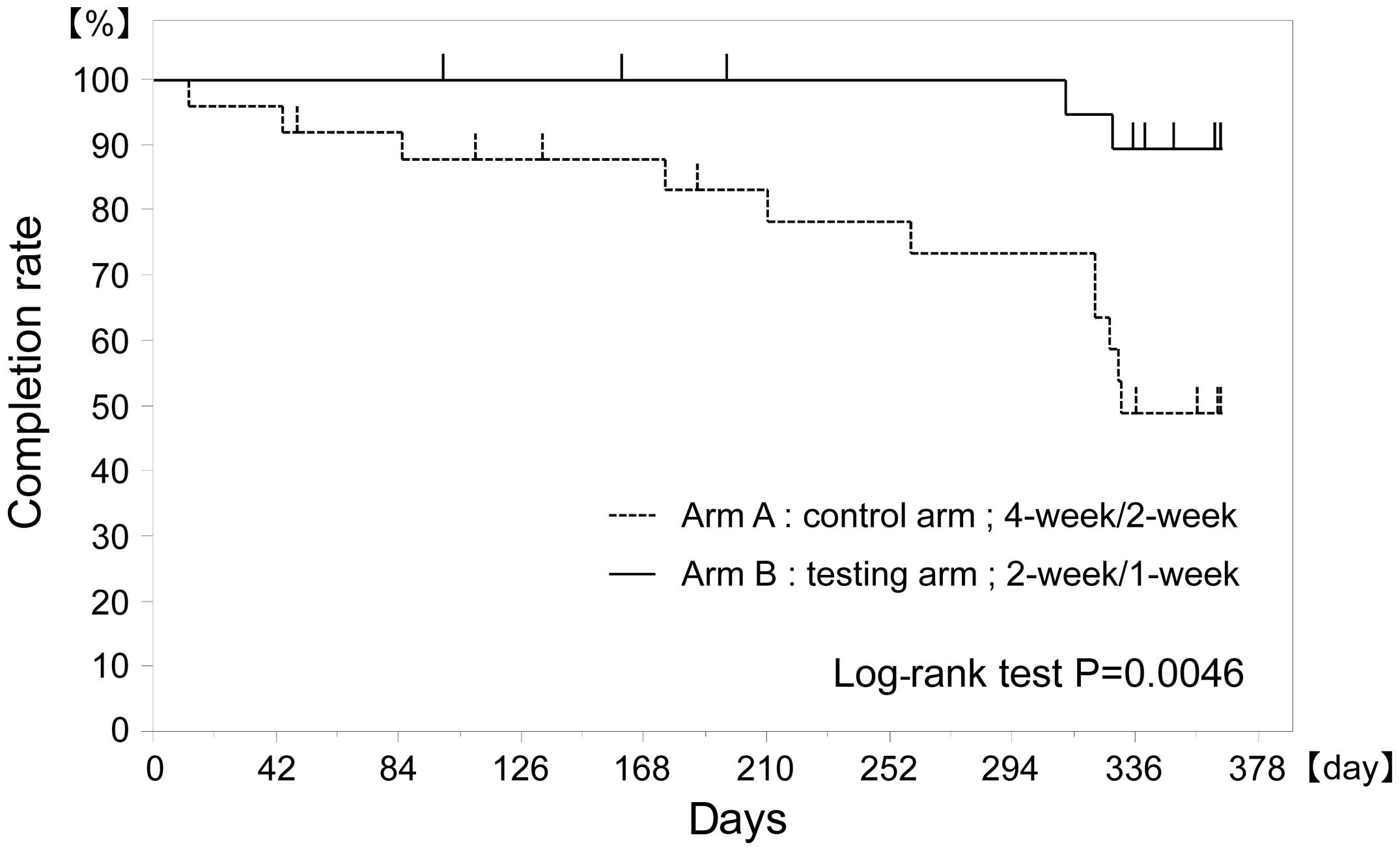
Treatment continuation rates
The treatment continuation rates for S-1 were 88 and
100% at 3 months, 83 and 100% at 6 months and 49 and 89% at 12
months after the initiation of S-1 treatment for the 4-week/2-week
and the 2-week/1-week arms, respectively, with the 2-week/1-week
arm being superior to the 4-week/2-week arm (P=0.0046) (Fig. 2, Table
II).
| Table II.Compliance/feasibility of each
treatment arm. |
Table II.
Compliance/feasibility of each
treatment arm.
| Variables | Arm Aa (n=25) | Arm Bb (n=21) |
|---|
| Protocol treatment
completion rate (%) |
|
|
| 3
month | 88 | 100 |
| 6
months | 83 | 100 |
| 9
months | 73 | 100 |
| 12
months | 49 | 89 |
| Relative dose
intensity (%) | 70.0 | 83.8 |
Adverse events
Adverse events were analyzed for all The patients.
The frequency of adverse events was 92 and 77.3% for the
4-week/2-week and 2-week/1-week arms, respectively. Grade 3 adverse
events included anorexia (8.0 and 0%), nausea (4.0 and 0%),
vomiting (4.0 and 0%), fatigue (8.0 and 0%), pigmentation (0 and
4.8%), diarrhea (4.0 and 0%), decreased hemoglobin concentration
(4.0 and 4.8%), hand-foot syndrome (4.0 and 0%) and hypoalbuminemia
(4.0 and 0%), with a tendency toward lower rates observed in the
2-week/1-week arm. No ≥grade 4 adverse events were observed in
either arm (Table III).
| Table III.Adverse events in each treatment
arm. |
Table III.
Adverse events in each treatment
arm.
|
| Arm Aa (n=25) | Arm Ba (n=25) |
|---|
|
|
|
|
|---|
| Adverse events | All grades (%) | ≥Grades 3 (%) | All grades (%) | ≥Grades 3 (%) |
|---|
| Leukopenia | 6 (24.0) | 0 (0.0) | 8 (38.1) | 0 (0.0) |
| Neutropenia | 10 (40.0) | 0 (0.0) | 10 (47.6) | 0 (0.0) |
|
Thrombocytopenia | 5 (20.0) | 0 (0.0) | 2 (9.5) | 0 (0.0) |
| Anemia | 11 (44.0) | 1 (4.0) | 9 (42.9) | 1 (4.8) |
|
Hypoalbuminemia | 1 (4.0) | 1 (4.0) | 0 (0.0) | 0 (0.0) |
| AST | 2 (8.0) | 0 (0.0) | 5 (23.8) | 0 (0.0) |
| ALT | 3 (12.0) | 0 (0.0) | 4 (19.0) | 0 (0.0) |
| Total
bilirubin | 3 (12.0) | 0 (0.0) | 2 (9.5) | 0 (0.0) |
| Oral mucositis | 8 (32.0) | 0 (0.0) | 3 (14.3) | 0 (0.0) |
| Anorexia | 11 (44.0) | 2 (8.0) | 10 (47.6) | 0 (0.0) |
| Nausea | 10 (40.0) | 1 (4.0) | 5 (23.8) | 0 (0.0) |
| Vomiting | 2 (8.0) | 1 (4.0) | 2 (9.5) | 0 (0.0) |
| Rash | 5 (20.0) | 0 (0.0) | 4 (19.0) | 0 (0.0) |
| Fatigue | 14 (56.0) | 2 (8.0) | 7 (33.3) | 0 (0.0) |
| Pigmentation | 12 (48.0) | 0 (0.0) | 10 (47.6) | 1 (4.8) |
| Diarrhea | 11 (44.0) | 1 (4.0) | 5 (23.8) | 0 (0.0) |
| Water eyes | 1 (4.0) | 0 (0.0) | 2 (9.5) | 0 (0.0) |
| Hand-foot
syndrome | 1 (4.0) | 1 (4.0) | 1 (4.8) | 0 (0.0) |
| Dysphasia | 1 (4.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Hematuria | 1 (4.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Discussion
For the treatment of gastric cancer, which has a
high incidence among Japanese individuals, curative surgery is the
optimal therapeutic approach. Although a wide variety of
postoperative adjuvant chemotherapy options for gastric cancer have
been investigated in order to improve The outcome of surgery, S-1
has become the standard adjuvant chemotherapy following gastric
cancer surgery in Japan, based on the results of the ACTS-GC study.
However, compliance to S-1 treatment was not satisfactory in the
ACTS-GC study and an improvement in compliance remains an issue
that must be addressed.
The 4-week administration of S-1 followed by a
2-week rest regimen has been established as the standard regimen
for S-1 therapy. Results from a post-marketing survey on 4,177
patients with advanced recurrent gastric cancer demonstrated that
the rate of toxicity for the 4-week/2-week regimen was 74.3% and
the rate of ≥Grade 3 adverse events was 25%. In addition, in 3,801
patients assessed for the efficacy analysis, benefits with the
4-week/2-week regimen were observed, with a median survival time of
8.3 months and a 1-year survival rate of 33.3% (95% confidence
interval: 31.8–34.9) (9). However,
since the 2-week/1-week regimen is considered to be acceptable in
terms of relative dose intensity over a treatment period similar to
the usual treatment schedule (4-week/2-week) and since there are
reports that antitumor efficacy, adverse reactions and prolongation
of the treatment period are not superior compared to the
conventional S-1 treatment schedule (4-week/2-week) in advanced
recurrent gastric cancer, this regimen does not have a solid
reputation (10,11).
The 2-week/1-week regimen investigated in this study
exhibited better feasibility and a higher treatment completion rate
compared to the standard 4-week/2-week regimen. If the
2-week/1-week regimen is associated with a better relapse-free
survival and overall survival, this treatment may be a safe
treatment option, with a higher completion rate.
The association between the dosing interval of
fluoropyrimidine anticancer drugs and antitumor efficacy and
adverse reactions has been extensively investigated. Originally,
the known cell cycle of tumor cells is longer (5–7 days) compared
to that of normal cells, such as bone marrow and gastrointestinal
mucosal cells (~0.5–2 days) (12,13).
Shirasaka et al (14) reported
that normal cells may be rescued by interrupting the administration
of fluoropyrimidine anticancer drugs every 24 h, exploiting the
difference in cell cycles between normal and tumor cells. In an
alternate-day treatment regimen based on the abovementioned theory,
normal cells may have a rest every other day, while tumor cells
have no rest due to their longer doubling time, suggesting that The
cytotoxic effect on tumor cells is equal to or more potent than on
normal cells. Arai et al (15)
conducted an alternate-day treatment schedule with S-1 in 36
gastric cancer patients and reported that these patients exhibited
adequate blood 5-FU concentrations at 2 h after administration and
experienced a reduced frequency of adverse events, with adequate
clinical efficacy.
Recently, the benefits of combination treatments
with S-1/cisplatin or S-1/docetaxel as adjuvant chemotherapy
following surgery in stage III gastric cancer were reported.
Takahari et al (16)
investigated the benefits of postoperative adjuvant chemotherapy
using the S-1/cisplatin combination in stage III gastric cancer and
reported excellent outcomes with relapse-free and overall survival
rates at 74.1 and 84.5%, respectively, at 3 years. In addition,
Fujitani et al (17)
investigated postoperative adjuvant chemotherapy with the
S-1/docetaxel combination in stage III gastric cancer and reported
results that relapse-free and overall survival rates were 66.2 and
78.4%, respectively, at 3 years. However, these aggressive
postoperative adjuvant chemotherapies may be associated with low
tolerability, as the completion rates for the treatment courses
were 72% for 3 courses of S-1/cisplatin and 79.2% for 4 courses of
S-1/docetaxel. The development of safer adjuvant chemotherapy
regimens of satisfactory efficacy and tolerability are expected in
future studies.
In conclusion, the completion of treatment using the
4-week administration followed by a 2-week rest or the 2-week
administration followed by a 1-week rest regimen of S-1 as
postoperative adjuvant chemotherapy was investigated in a
multicenter, randomized clinical trial in order to establish a safe
postoperative adjuvant chemotherapy regimen for gastric cancer,
with a higher treatment completion rate. The 2-week/1-week regimen
was associated with a higher completion rate compared to the
4-week/2-week regimen, with an acceptable frequency of adverse
events. If future analyses reveal acceptable relapse-free survival
and overall survival rates for the 2-week/1-week regimen, this is
expected to be a safer treatment option with a higher completion
rate.
References
|
1
|
Shirasaka T, Shimamato Y, Ohshimo H,
Yamaguchi M, Kato T, Yonekura K and Fukushima M: Development of a
novel form of an oral 5-fluorouracil derivative (S-1) directed to
the potentiation of the tumor selective cytotoxicity of
5-fluorouracil by two biochemical modulators. Anticancer Drugs.
7:548–557. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sugimachi K, Maehara Y, Horikoshi N,
Shimada Y, Sakata Y, Mitachi Y and Taguchi T: An early phase II
study of oral S-1, a newly developed 5-fluorouracil derivative for
advanced and recurrent gastrointestinal cancers. The S-1
Gastrointestinal Cancer Study Group. Oncology. 57:202–210. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sakata Y, Ohtsu A, Horikoshi N, Sugimachi
K, Mitachi Y and Taguchi T: Late phase II study of novel oral
fluoropyrimidine anticancer drug S-1 (1 M tegafur-0.4 M gimestat-1
M otastat potassium) in advanced gastric cancer patients. Eur J
Cancer. 34:1715–1720. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Koizumi W, Kurihara M, Nakano S and
Hasegawa K: Phase II study of S-1, a novel oral derivative of
5-fluorouracil, in advanced gastric cancer. For the S-1 Cooperative
Gastric Cancer Study Group. Oncology. 58:191–197. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Maehara Y: S-1 in gastric cancer: a
comprehensive review. Gastric Cancer. 6 (Suppl 1):2–8. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sakuramoto S, Sasako M, Yamaguchi T, et
al: Adjuvant chemotherapy for gastric cancer with S-1, an oral
fluoropyrimidine. N Engl J Med. 357:1810–1820. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tsukuda M, Kida A, Fujii M, et al:
Randomized scheduling feasibility study of S-1 for adjuvant
chemotherapy in advanced head and neck cancer. Br J Cancer.
93:884–889. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Japanese Gastric Cancer Association, .
Japanese classification of gastric carcinoma - 2nd English edition.
Gastric Cancer. 1:10–24. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nagashima F, Ohtsu A, Yoshida S and Ito K:
Japanese nationwide post-marketing survey of S-1 in patients with
advanced gastric cancer. Gastric Cancer. 8:6–11. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Imamura H, Furukawa H, Kishimoto T, et al:
Phase II study of 2-week S-1 administration followed by 1-week rest
for gastric cancer. Hepatogastroenterology. 54:2167–2171.
2007.PubMed/NCBI
|
|
11
|
Kimura Y, Kikkawa N, Iijima S, et al: A
new regimen for S-1 therapy aiming at adverse reaction mitigation
and prolonged medication by introducing a 1-week drug-free interval
after each 2-week dosing session: efficacy and feasibility in
clinical practice. Gastric Cancer. 6 (Suppl 1):34–39. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lipkin M, Sherlock P and Bell B: Cell
proliferation kinetics in the gastrointestinal tract of man. II.
Cell renewal in stomach, ileum, colon, and rectum.
Gastroenterology. 45:721–729. 1963.PubMed/NCBI
|
|
13
|
Clarkson B, Ota K, Ohkita T and O'Connor
A: Kinetics of proliferation of cancer cells in neoplastic
effusions in man. Cancer. 18:1189–1213. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shirasaka T: Conceptual changes in cancer
chemotherapy - biochemical modulation of 5-FU from bench to clinic.
Cancer & Chemotherapy. 27 (Suppl 2):193–205. 2000.
|
|
15
|
Arai W, Hosoya Y, Hyodo M, et al:
Alternate-day oral therapy with TS-1 for advanced gastric cancer.
Int J Clin Oncol. 9:143–148. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Takahari D, Hamaguchi T, Yoshimura K, et
al: Survival analysis of adjuvant chemotherapy with S-1 plus
cisplatin for stage III gastric cancer. Gastric Cancer. 17:383–386.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fujitani K, Tamura S, Kimura Y, et al:
Three-year outcomes of a phase II study of adjuvant chemotherapy
with S-1 plus docetaxel for stage III gastric cancer after curative
D2 gastrectomy. Gastric Cancer. 17:348–353. 2014. View Article : Google Scholar : PubMed/NCBI
|