Introduction
Radiation-induced cranial nerve palsy (RICNP) is a
severe long-term effect observed in patients treated with high-dose
radiation therapy (RT) for nasopharyngeal carcinoma, with an
incidence ranging between 3.7 and 30.9% in the literature (1–9).
Several studies have reported that the lower cranial
nerves (CNs) are more susceptible to radiation damage (1–3). RICNP
significantly compromises the quality of life: Damage of the
glossopharyngeal nerve (IX) causes loss of sensation in the pharynx
and decreased salivation; palsy of the vagus nerve (X) leads to
impaired parasympathetic functions of almost all organs; and palsy
of the hypoglossal nerve (XII) causes complete paralysis of the
ipsilateral side of the tongue.
The aim of this study was to present the detailed
clinical findings of two patients with RICNP following conventional
three-dimensional (3D) RT and IMRT, respectively, and to analyze
the IMRT cohort at risk (high radiation dose delivered to the upper
level 2 and 7b lymph node stations, where the nerves IX-XII pass
through), in order to assess the incidence of RICNP in IMRT.
Case reports
Case report 1 (3D-RT)
In June 1999, a 50-year-old male patient was
referred to our department for postoperative RT for a squamous cell
carcinoma of the right tonsil with unilateral lymph node
metastases, staged as pT3 (4.2 cm), pN2b (1/29, Rouvière node), M0,
R0 (minimal resection margin, 2 mm), G3.
The patient had previously undergone trans-cervical
oropharyngectomy with neck dissection of ipsilateral level 1–3
lymph nodes. Reconstruction of the defect was performed with a free
radialis flap.
RT planning was performed using a computed
tomography (CT)-based 3D conformal radiation technique. Adjuvant RT
was performed according to the following concomitant boost (CCB)
schedule: A first series with 20×1.8 to a total of 36 Gy using
laterally opposed photon beams, followed by spinal cord sparing
electrons to the dorsal lymphatic pathways combined with anterior
lateral opposed photon beam to a total of 50.4 Gy. The CCB was
performed with 9×1.5 Gy as a 2nd fraction/day, once/week.
Unfortunately, the electron isodose distribution is no longer
available, as the former treatment planning system has been
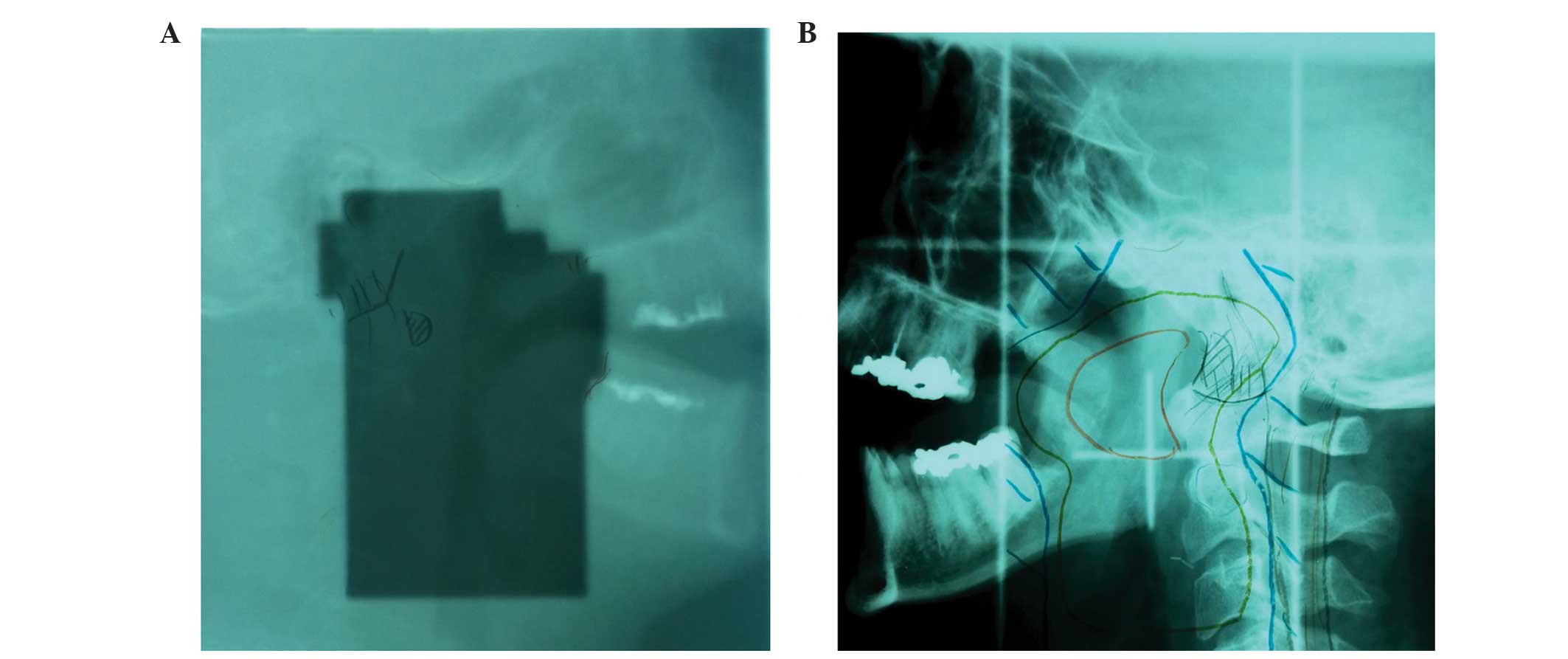
replaced by other systems. In an attempt to reconstruct the dose to
the nerve region of interest (ROI) in this patient based on hard
copy printouts from 1999, bilateral high-dose exposure was
documented, as the primary lesion extended to both sides and there
was significant nodal disease. The XII nerve was bilaterally
exposed to the tumor dose, except for the most cranial aspect (2–3
cm from the hypoglossal canal), which was exposed to a lower dose
(~50–55 Gy), which is usually well tolerated (Fig. 1). The patient underwent regular
follow-up (FU) at our joint Otorhinolaryngology clinic (S.S., G.H.)
until July, 2000. Late term tolerance to treatment has been good
thus far, apart from a velopalatal insufficiency due to extensive
palatal resection with consequent altered speech. Velopalatal
reconstructive surgery was performed in July, 2000.
In May, 2011, the patient developed swallowing
disturbances due to impaired tongue and laryngeal movement.
Sufficient nutrition was ensured through a feeding tube. In June,
2011 the patient underwent transcervical cricomyotomy to reduce the
resistance to swallowing, which achieved a minor improvement. At
that time, bilateral XII nerve palsy was diagnosed. Centrally
located causes, such as amyotrophic lateral sclerosis, were
excluded. Following re-evaluation of the RT fields, XII nerve palsy
was hypothesized to be a side effect of the bilateral irradiation
12 years prior.
Further extensive neurological and radiological
investigations were performed to differentiate between RT-induced
damage vs. other causes, which revealed an overall decreased motor
neuron activity affecting other nerves, including the tibial and
median nerves; to a certain extent, the progressive severe symptoms
were considered to reflect the coexistence of radiation-related and
independent neuronal disorders. However, in August, 2014, the
patient was diagnosed with bilateral X nerve paresis with nocturnal
stridor, feeding tube dependency and almost completely paralyzed
tongue muscles, which supported the radiogenic etiology of the
symptoms. To date, the patient remains tumor-free (September,
2014).
Care report 2 (IMRT)
A 46-year-old patient underwent definitive SIB-IMRT
with 30×2.2 Gy/fraction (66 Gy mean dose) for a left-sided cT1cN1
base of tongue carcinoma. Six years later he was diagnosed with an
ipsilateral brachial plexopathy, which was due to a disc herniation
C3/4 and C5/6, and a left XII nerve RICNP grade 2–3, for which
other etiology with the exception of RT was excluded. The 2.2 Gy/f
SIB-IMRT schedule was used for several other patients in the
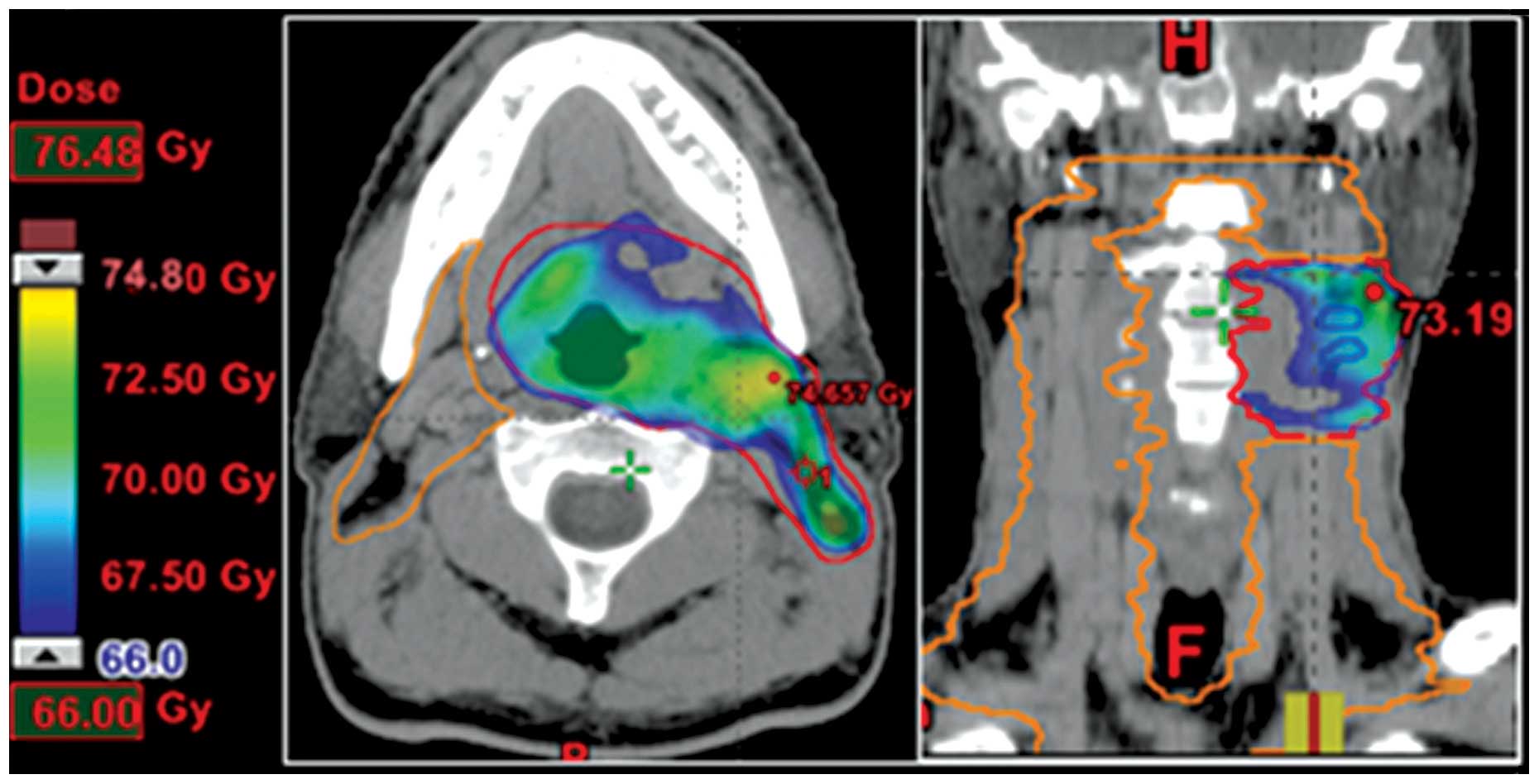
initial IMRT implementation phase. The Dmax point dose in this
patient was 74 Gy (Fig. 3). Two years
later, the patient succumbed to an aggressive NHL, and therefore,
no further RICNP FU is available.
IMRT cohort
In order to assess the incidence of RICNP in the
IMRT era, we identified patients at risk treated in our department
with normofractionated/slightly hypofractionated (2.0/2.11/2.2
Gy/f) IMRT between January, 2002 and December, 2012. All the
patients were irradiated with 6-MV photons, with 66–70 Gy, 5
days/week, using simultaneous-integrated boost IMRT as previously
described (10). The inclusion
criteria were as follows: Patients with locoregionally controlled
disease who received >65 Gy to the lower CN region with a FU of
at least 24 months. These criteria were met by 151 patients treated
with definitive IMRT, with or without additional chemotherapy.
Focus was on the lower CNs, as they are the CNs most exposed to
high radiation dose. The patient characteristics are summarized in
Table I.
 | Table I.Patient and treatment parameters. |
Table I.
Patient and treatment parameters.
| Parameters | Values |
|---|
| Patients, no. | 151 |
| Cervical sides at
risk, no. | 188 |
| Primary tumor
location, no. |
|
|
Oropharynx | 75 |
|
Nasopharynx | 27 |
|
Hypopharynx | 30 |
|
Supraglottic area | 11 |
| Oral
cavity | 4 |
|
Glottic | 3 |
| Unknown
primary | 1 |
| Gender ratio
(female:male) | 1:3.5 |
| Mean age, years
(range) | 58 (16–84) |
| Follow-up, months
mean/median (range) | 71/68 (27–145) |
| T stage, % |
|
| 1 | 11 |
| 2 | 24 |
| 3 | 25 |
| 4 | 39 |
| Unknown
primary | 1 |
| N stage, % |
|
| 0 | 6 |
| 1–2b | 58 |
| 2c | 29 |
| 3 | 7 |
| Systemic therapy,
no. | 82 |
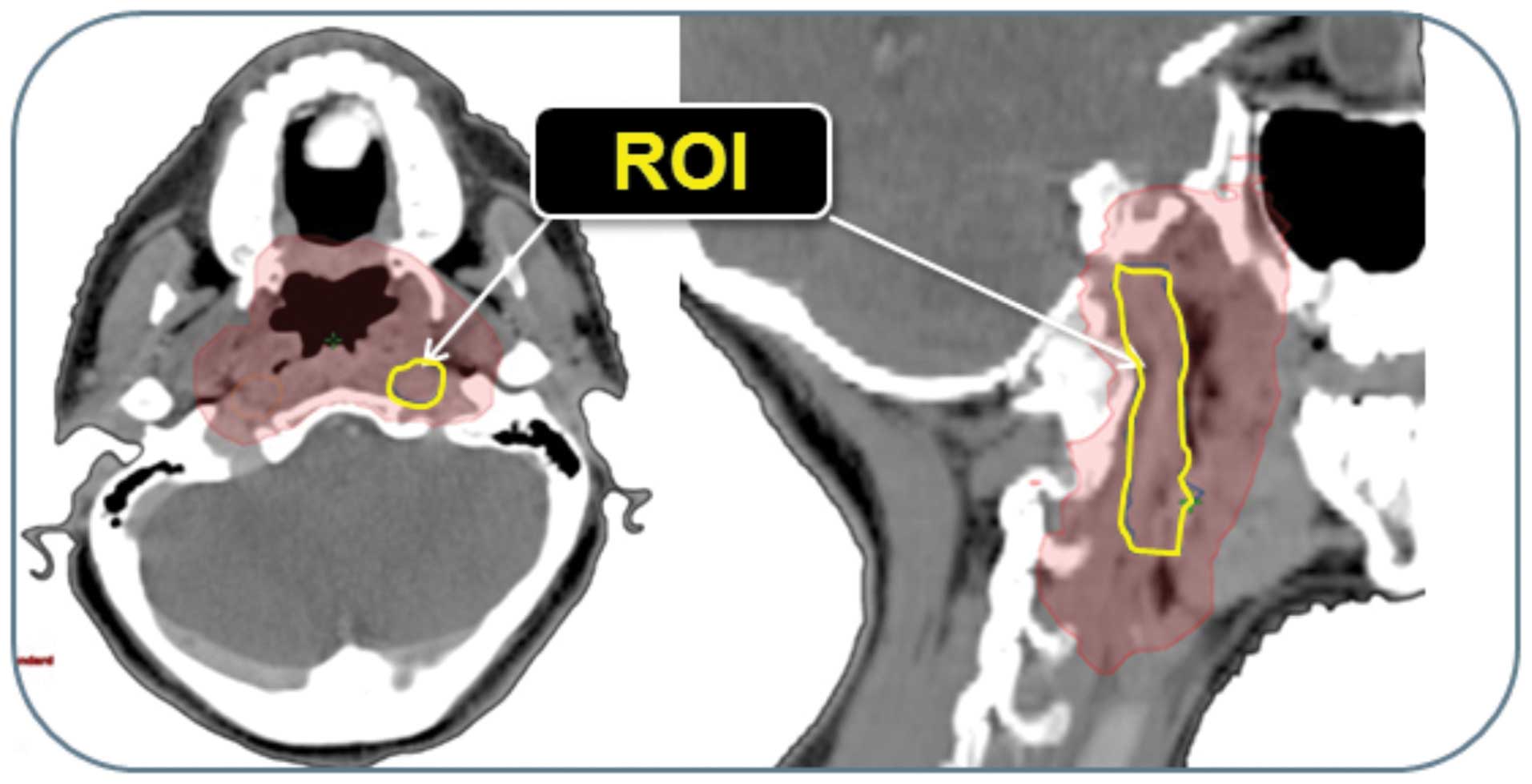
The corresponding anatomic ROI was retrospectively
contoured in the planning CT by B.Y. and reviewed by C.G. (Fig. 2). The anatomic ROI was drawn from the
base of the skull through the carotid sheath above the hyoid bone,
where the CNs IX-XII are located between the internal jugular vein
and internal carotid artery down to the thyroid cartilage, which is
approximately in the upper border of C4 (11). The space in the level of 2nd and 3rd
cervical vertebrae included the common carotid artery inferiorly
and internal carotid artery superiorly, internal jugular vein and
the IX, X, XI and XII cranial nerves. Due to the limited resolution
of the planning CT, it was not possible to draw each of the lower
CNs separately.
All the patients were followed up on a weekly basis
during the RT period by a radiation oncologist. Regular FU visits
were conducted in our joint clinic (Department of
Otorhinolaryngology, Head and Neck Surgery, University Hospital of
Zurich) and, in part, at a private clinic. The institutional
standards for patient assessment included physical examination and
flexible fiberoptic endoscopy every ~2 months during the first year
of FU, every 3 months during the second and third years and every 6
months during the fourth and fifth years. In case of suspicious
findings or clinical symptoms, further investigations were
performed, including magnetic resonance imaging, positron emission
tomography-CT, or fine-needle aspirations. Clinical examination to
diagnose or exclude RICNP was routinely performed, based on
clinical history and physical examination in our
Otorhinolaryngology joint clinic. As CNP is a clinical disorder
with distinct subjective symptoms, affected patients were reliably
diagnosed during the regular FU visits; undetected cases were
unlikely in the assessed cohort undergoing regular FU.
Systemic chemotherapy was administered in
combination with IMRT when indicated [cisplatin weekly 40
mg/m2 (82%) and/or cetuximab 400 mg/m2
loading dose followed by 250 mg/m2 weekly during RT,
according to Bonner et al (12)]. To date, one of 151 patients in the
IMRT cohort has developed lower CNP after 6 years post IMRT (see
Case report 2). The overall survival of the IMRT cohort is depicted
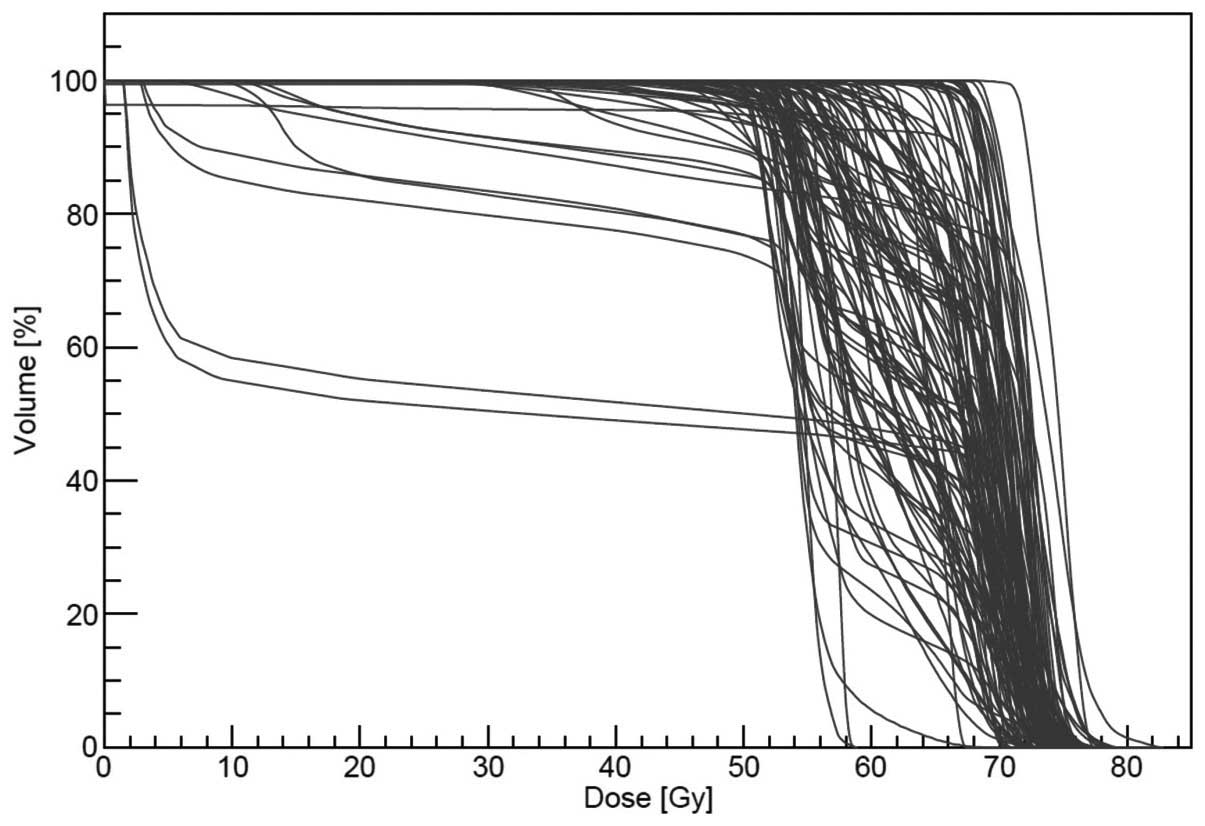
in Fig. 4. A total of 114 patients
with unilateral and 37 patients with bilateral exposure [total:
114+(2×37)=188 ROIs in 151 individuals] were included in this
analysis. The dose-volume histograms of all 188 ROIs are shown in
Fig. 5. The absolute volumes of the
ROIs were mean/median 9.4/9.3 cc (range, 5.5–14.5 cc). The mean
dose was 65.45 Gy (range, 46.26–75.42 Gy) and the mean maximum dose
was 75.42 Gy (range, 59.7–108.13 Gy). A total of 55, 37 and 8% of
the patients were followed up for 5, 7 and 10 years, respectively.
The mean/median duration of FU of the entire cohort was 71/68
months (range, 27–145 months).
Discussion
The presented case with bilateral CN XII palsy due
to radiation exposure in the pre-IMRT era prompted us to analyze
our IMRT cohort at risk. There was one (1) RICNP case among 151 assessed patients
treated with definitive IMRT in our institution, after a mean FU of
71 months.
There were certain limitations to this analysis,
mainly due to its retrospective approach and the relatively short
observation time.
A crucial point when evaluating RICNP rates is the
duration of observation of the assessed cohorts, as the risk for
such events changes with longer FU. For RT-induced brachial
plexopathy, the risk was found to be constant over a considerable
portion of breast cancer patients life (13). Johansson et al (14) retrospectively analyzed the latency for
RT-induced neuropathy in breast cancer patients and found that the
incidence at 5 years did not represent the full spectrum of
injuries.
Over the last few years, certain study groups
published results focusing on RICNP in patients with nasopharyngeal
(1–4,15) and
oropharyngeal cancer (16). In those
reports, the rate of RICNP ranges between 3.7 and 30.9% (Table II). As summarized in Table II, the techniques and doses of RT and
the frequency of chemotherapy application exhibited significant
variations, which may be responsible for the wide range of RICNP
incidence. The median FU time in the aforementioned studies ranged
between 7.5 and 11.4 years. Rong et al (1) reported a mean latency for RICNP of 5.85
years. Kong et al (2)
demonstrated that, among all patients who developed RICNP, ~10%
developed RICNP during every 5 years. The cumulative incidence for
lower RICNP was 5.7, 17.4, 27.1 and 37.3% at 5, 10, 15 and 20
years, respectively. Another study group focusing on XII CNP
reported the development of RICNP in 8 of the 17 affected patients
within the first 50 months following RT completion (4).
| Table II.Selected studies on head and neck
cancer patients with RICNP. |
Table II.
Selected studies on head and neck
cancer patients with RICNP.
| Authors (year) | Country | RT time period | Tumor side | No. of patients | RT technique | Total dose | CTX (%) | Median FU
(years) | RICNP (%) | Most frequently
affected CNs | (Refs.) |
|---|
| Sanguineti et
al (1997) | USA | 1954–1992 | NPC | 378 | 2D | 58–76 Gya | 0.0 | 10 | 8.0 | NA | (8) |
| Lin et
al(2002) | China | Since 1968 | NPC | NA | 2D | 70–79.2
Gya | NA | NA | 19 patients collected
from a large sample - no quantitative analysis | XIIb | (15) |
| King et
al(1998) | China | Prior to 1995 | NPC | 387 | 2D | >66
Gya | NA | for patients with
RICNP: 3 | 4.3 | XII only | (4) |
| Sumitsawan et
al (2009) | Thailand | 2003–2005 | NPC | 200 | NA | 69 Gya | 72.5 | NA | 6.5 | NA | (9) |
| Luk et
al(2013) | China | 1998–2007 | NPC | 965 | 3DCRT 73.4% IMRT
26.6% | 66–70 Gya | NA | 8.9 | 3.7 | XIIb | (3) |
| Huang et al
(2013) | USA | 2000–2005 | OPC | 3 | 3DRT, IMRT | 70.4–75.88
Gya | 66.6 | 8–13 | 100.0 | X, XI, XII | (16) |
| Rong et al
(2012) | China | 1994–2006 | NPC | 328 | 2-D | 60–80
Gya | NA | 11.3 | 21.9 | Lower
CNb | (1) |
| Kong et al
(2011) | China,
Singapore | 1962–1995 | NPC | 317 |
2D/60Co/BT boost | 71 Gy (90.5%
conventional, 9.5% hyperfract.) | 14.2 | 11.4 | 30.9 | Lower
CNb | (2) |
| He et al
(2012) | China | 1995–2002 | NPC | 158 |
2D/60Co | 78 hyperfract. | 0.0 | 7.5 | 11.0 | XIIb | (5) |
| Bakst et al
(2011) | USA | 2002–2007 | NPC | 25 | IMRT | 70.2 Gy
hypofract. | 100.0 | 2.75 | 4.0 | XII only | (6) |
| Fua et al
(2007) | Malaysia | 2004–2008 | NPC | 176 | 3DCRT | 66–70
Gya | 16.5 | 5 | 2.5 | NA | (7) |
| Present study | Switzerland | 2002–2012 | All | 188 necks | SIB-IMRT | >65
Gya | 82.0 | 5.9 | 0.5 | XII |
|
| Total |
|
|
| 2,479 |
|
|
| Mean: 7.3 | Mean: 9.7 |
|
|
Several risk factors for RICNP have been described:
Kong et al (2) identified
initial CNP at diagnosis, chemotherapy, total radiation dose and
upper neck fibrosis as independent risk factors for developing
RICNP. Luk et al (3) also
found CNP at diagnosis to be a prognostic factor. In our cohort,
82% of the patients received systemic therapy and none of the
included patients presented with CNP prior to treatment initiation.
The majority of the studies on RICNP included patients prior to the
availability of IMRT (Table II).
IMRT is known to improve the therapeutic ratio and/or treatment
tolerance in patients with head and neck cancer (17,18) by
facilitating sparing of normal tissue. In a prospective trial
analyzing hypofractionated IMRT with chemotherapy for
nasopharyngeal cancer, Bakst et al (6) only reported 4% RICNP.
In conclusion, our results and the general knowledge
of the tissue sparing ability of IMRT indicate that modern RT
techniques may affect the incidence of RICNP by exposing shorter
parts of the nerves to high radiation doses and by causing less
extensive muscle and soft tissue fibrosis close to the CNs, which
was also considered to be partly responsible for the pathogenesis
of RICNP. Applying IMRT, physicians must bear in mind that ‘hot
spots’ in CN regions must be avoided (11). Hypofractctionation >2.11 Gy/f may
result in a higher risk for RICNP due to hot spots. RT-induced
nerve damage is known for a potentially long latency till clinical
appearance (19).
Modulated tissue-sparing RT techniques may have the
potential to reduce the incidence of RICNP. Longer FU is required
to support this hypothesis.
References
|
1
|
Rong X, Tang Y, Chen M, Lu K and Peng Y:
Radiation-induced cranial neuropathy in patients with
nasopharyngeal carcinoma A follow-up study. Strahlenther Onkol.
188:282–286. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kong L, Lu JJ, Liss AL, Hu C, Guo X, Wu Y
and Zhang Y: Radiation-induced cranial nerve palsy: A
cross-sectional study of nasopharyngeal cancer patients after
definitive radiotherapy. Int J Radiat Oncol Biol Phys.
79:1421–1427. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Luk YS, Shum JS, Sze HC, Chan LL, Ng WT
and Lee AW: Predictive factors and radiological features of
radiation-induced cranial nerve palsy in patients with
nasopharyngeal carcinoma following radical radiotherapy. Oral
Oncol. 49:49–54. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
King AD, Leung SF, Teo P, Lam WW, Chan YL
and Metreweli C: Hypoglossal nerve palsy in nasopharyngeal
carcinoma. Head Neck. 21:614–619. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
He X, Ye M, Guo X, Pan Z, Zhang Z, He S
and Liu T: Treatment outcome of patients with stages I-II
nasopharyngeal carcinoma after late course accelerated
hyperfractionation radiotherapy alone. Oral Oncol. 48:1058–1063.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bakst RL, Lee N, Pfister DG, Zelefsky MJ,
Hunt MA, Kraus DH and Wolden SL: Hypofractionated dose-painting
intensity modulated radiation therapy with chemotherapy for
nasopharyngeal carcinoma: A prospective trial. Int J Radiat Oncol
Biol Phys. 80:148–153. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fua TF, Corry J, Milner AD, Cramb J,
Walsham SF and Peters LJ: Intensity-modulated radiotherapy for
nasopharyngeal carcinoma: Clinical correlation of dose to the
pharyngo-esophageal axis and dysphagia. Int J Radiat Oncol Biol
Phys. 67:976–981. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sanguineti G, Geara FB, Garden AS, Tucker
SL, Ang KK, Morrison WH and Peters LJ: Carcinoma of the nasopharynx
treated by radiotherapy alone: Determinants of local and regional
control. Int J Radiat Oncol Biol Phys. 37:985–996. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sumitsawan Y, Chaiyasate S, Chitapanarux
I, Anansuthiwara M, Roongrotwattanasiri K, Vaseenon V and Tooncam
H: !Late complications of radiotherapy for nasopharyngeal
carcinoma. Auris Nasus Larynx. 36:205–209. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Peponi E, Glanzmann C, Kunz G, Renner C,
Tomuschat K and Studer G: Simultaneous integrated boost
intensity-modulated radiotherapy (SIB IMRT) in nasopharyngeal
cancer. Strahlenther Onkol. 186:135–142. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mourad WF, Young BM, Young R, et al:
Clinical validation and applications for CT-based atlas for
contouring the lower cranial nerves for head and neck cancer
radiation therapy. Oral Oncol. 49:956–963. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bonner JA, Harari PM, Giralt J, et al:
Radiotherapy plus cetuximab for squamous-cell carcinoma of the head
and neck. N Engl J Med. 354:567–578. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bajrovic A, Rades D, Fehlauer F, Tribius
S, Hoeller U, Rudat V, Jung H and Alberti W: Is there a life-long
risk of brachial plexopathy after radiotherapy of supraclavicular
lymph nodes in breast cancer patients? Radiother Oncol. 71:297–301.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Johansson S, Svensson H and Denekamp J:
Dose response and latency for radiation-induced fibrosis, edema,
and neuropathy in breast cancer patients. Int J Radiat Oncol Biol
Phys. 52:1207–1219. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lin YS, Jen YM and Lin JC:
Radiation-related cranial nerve palsy in patients with
nasopharyngeal carcinoma. Cancer. 95:404–409. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Huang AT, Song S, Dominguez LM, Nguyen J,
Goldman RA and Reiter ER: Delayed lower cranial neuropathies
following primary radiotherapy for oropharyngeal squamous cell
carcinoma. Laryngoscope. 123:1207–1209. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
May JT, Rao N, Sabater RD, et al:
Intensity-modulated radiation therapy as primary treatment for
oropharyngeal squamous cell carcinoma. Head Neck. 35:1796–1800.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Studer G, Linsenmeier C, Riesterer O, et
al: Late term tolerance in head neck cancer patients irradiated in
the IMRT era. Radiat Oncol. 8:2592013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Studer G, Stocker DN, Loewenich KF and
Glanzmann C: 40/42Gy in 13 fractions: a safe dose for the brachial
plexus. J Nucl Med Radiat Ther. 5:1682014.
|