Introduction
Thymoma is derived from thymic epithelial cells and
is one of the most common neoplasms in the anterior mediastinum
(1). The overall incidence of thymoma
is 0.15 cases per 100,000 individuals and the majority of the
patients with thymoma or thymic carcinoma are aged 40–60 years
(2,3).
The World Health Organisation (WHO) classification is based on
histological analysis of epithelial cell atypia and the degree of
infiltration of non-neoplastic lymphocytes (4). Although the great majority of these
tumors exhibit more conventional histological characteristics,
unusual types have also been described, such as sclerosing thymoma
(5). Spontaneous regression (SR) of
thymoma without therapy has been reported, although its incidence
is rare (6–8). This is the case report of a patient with
thymoma exhibiting SR and disappearance of the pleural
effusion.
Case report
A 30-year-old man was admitted to Toho University
Omori Medical Center with right chest pain and low-grade fever. The
patient was a never-smoker and had no medical history. On physical
examination, the temperature was 37.8°C and the respiratory sounds
were clear. A chest X-ray revealed a mass shadow in the right hilum
and a blunted right costophrenic angle. A chest X-ray obtained 3
months prior had shown minor expansion of the right mediastinum,
without any findings of right pleural effusion, but no additional
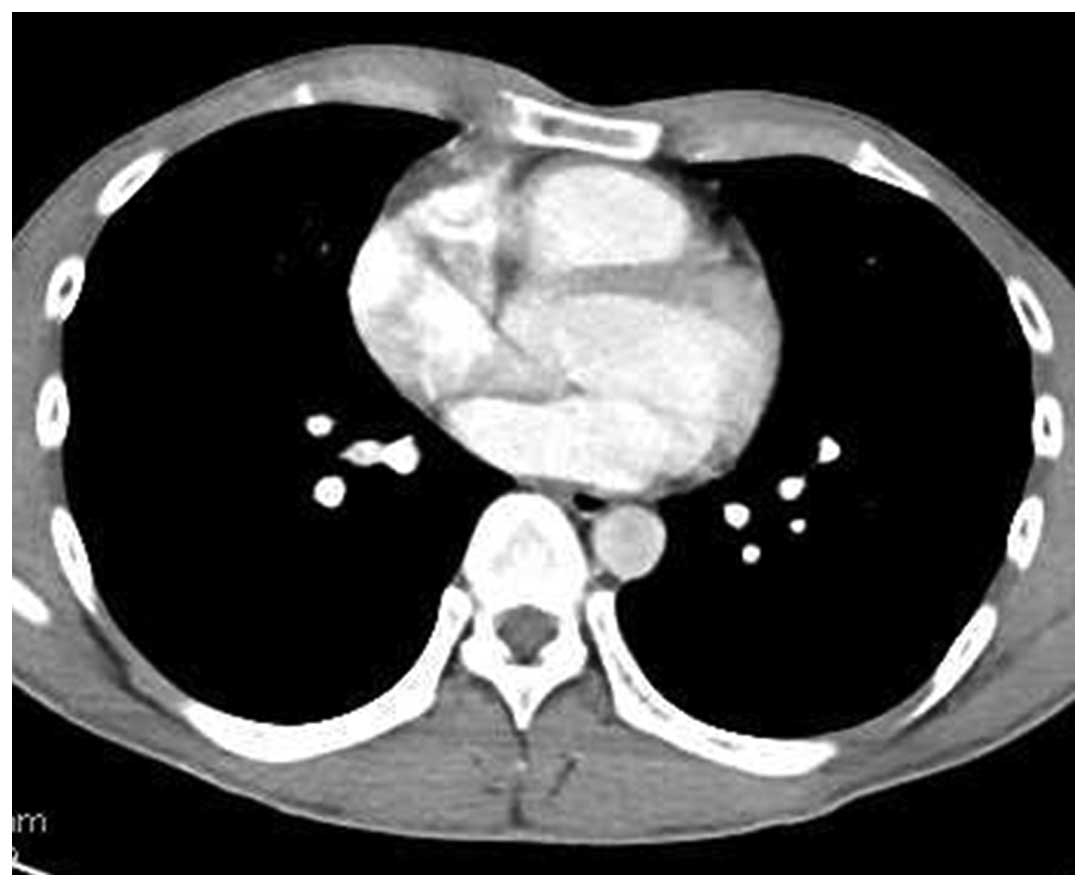
examinations were performed. A chest computed tomography (CT) scan
revealed an anterior mediastinal tumor sized 11.0×6.0×5.0 cm, with
a right pleural effusion (Fig. 1).
The laboratory analysis findings were normal, except for elevations
of the white blood cell count (11,000/µl), C-reactive protein (4.1
mg/dl) and serum cytokeratin fragment (CYFRA; 12.7 ng/ml, normal,
<2 ng/ml). Other tumor markers, including carcinoembryonic
antigen, α-fetoprotein, soluble interleukin-2 receptor, human
chorionic gonadotropin-β, and the anti-acetylcholine receptor
antibody, were within normal limits.
On the day of admission, thoracocentesis was
performed and 30 ml of yellowish, slightly bloody effusion were
obtained. The level of CYFRA in the pleural effusion was increased
to 143 ng/ml, the bacterial culture was negative and the
cytological examination revealed no malignant cells. The patient
exhibited no myasthenic symptoms, such as ptosis or muscle
weakness. On the first day after admission (6 days after the
initial CT), CT-guided needle biopsy (CTNB) was performed. the
chest CT prior to performing a CTNB revealed a mild regression of
the tumor (10.0×5.5×4.4 cm; reduction rate, 26.7%) with a marked
decrease of the pleural effusion volume, without additional
drainage (Fig. 2). The biopsied
specimen was mostly necrotic and the pathological diagnosis was not
definitive. Seven days later (13 days after the initial CT),
further regression was evident on CT (9.5×5.4×4.2 cm; reduction
rate, 34.7%) with disappearance of the pleural effusion.
At 35 days after the initial CT, the tumor had
shrunk to 8.0×3.6×3.0 cm (reduction rate, 73.8%) and the pleural
effusion had completely disappeared without treatment (Fig. 3). The serum CYFRA level had decreased
to 0.8 ng/ml. A non-steroidal drug was administered for the right
chest pain and fever. The patient's symptoms gradually disappeared
and the laboratory markers of inflammation decreased. Although the
mediastinal mass had shrunk without treatment, it did not
completely disappear (Table I). The
possibility of malignancy could not be excluded and the patient
underwent surgical resection 62 days after the initial CT. Magnetic
resonance imaging, 2 days prior to surgery, revealed a
high-intensity area in the left portion of the tumor, in
fat-suppressed T1- and T2-weighted images, suggesting a cystic
structure filled with considerable protein and serum (Fig. 4). The remaining portion of the tumor
exhibited a solid pattern, with a mildly hyperintense signal in
diffusion images and T2-weighted images. The tumor boundary was
relatively sharp, without any definitive findings suggesting
invasion.
 | Table I.Serial changes in the serum levels of
CYFRA and the size of the thymoma and volume of the pleural
effusion on chest CT. |
Table I.
Serial changes in the serum levels of
CYFRA and the size of the thymoma and volume of the pleural
effusion on chest CT.
| Time points | Day | Size, mm | Reduction rate,
% | Pleural effusion | CYFRA, ng/ml |
|---|
| At first visit | 0 | 110×60×50 | – | + | 12.7 |
| At CTNB | 6 | 100×55×44 | 26.7 | + | – |
| After CTNB (7
days) | 13 | 95×54×42 | 34.7 | – | – |
| After CTNB (1
month) | 35 | 80×36×30 | 73.8 | – | 0.8 |
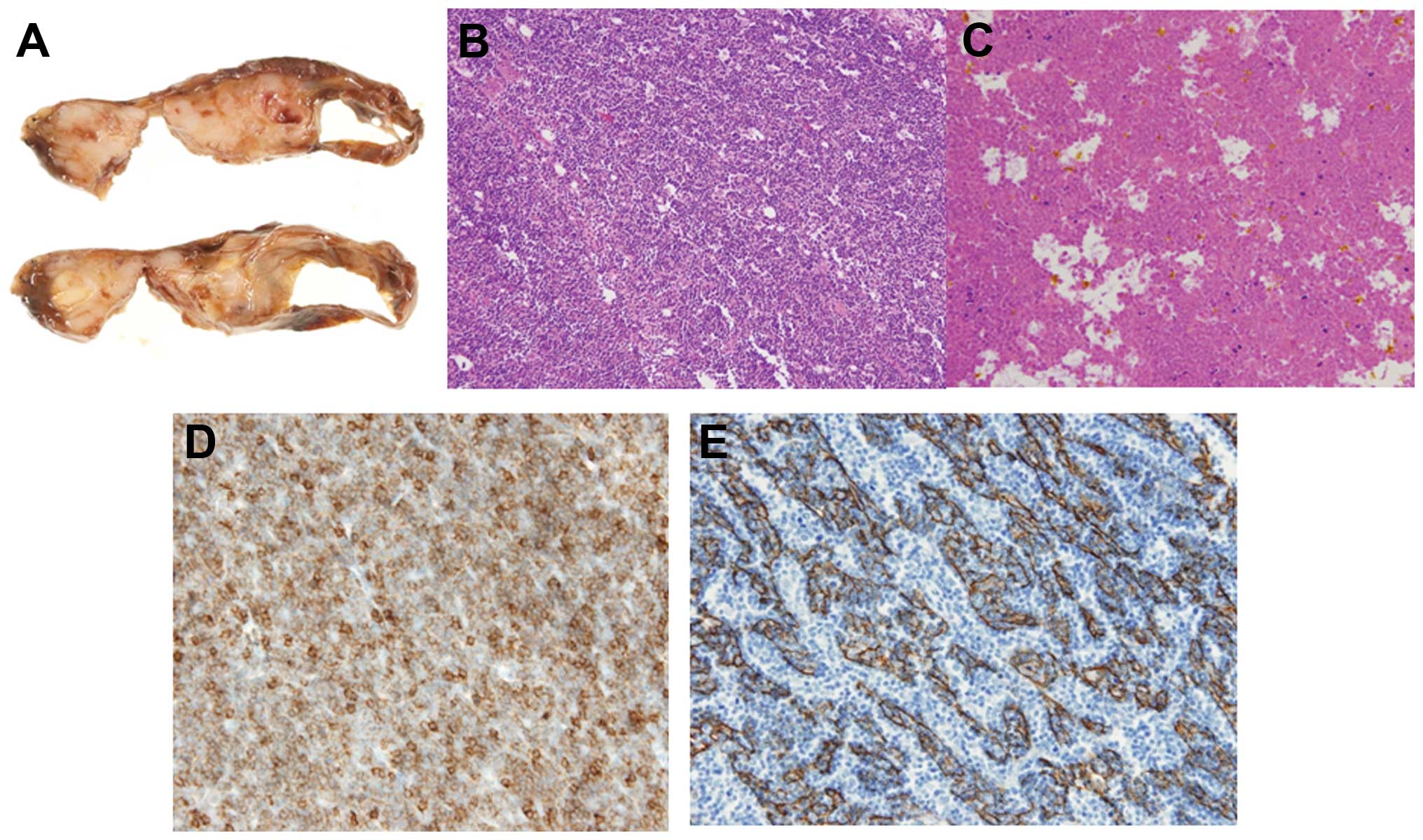
The mediastinal mass adhered densely to the upper
lobe of the right lung and thymectomy and partial resection of the
right upper lobe were performed. The mediastinal mass was composed
of a solid part and cystic space (Fig.
5A). In the solid part, there was epithelial cell proliferation
admixed with a large number of lymphocytes, which was compatible
with who type B2 thymoma (Fig. 5B).
The tumor displayed coagulation necrosis and fibrosis, with foamy
cell aggregations and cholesterol crystals (Fig. 5C). Microscopic transcapsular invasion
was present (Masaoka classification, stage II). By contrast, the
cystic wall was lined by a flattened epithelium including a small
number of goblet cells. Thymic tissue with Hassall's corpuscles was
attached to the thin-walled cyst, which was consistent with a
thymic cyst. On immunohistochemical staining (Fig. 5D and E), the tumor was strongly
positive for cytokeratin. The postoperative course was uneventful
and the patient remains recurrence-free at 1 year after
surgery.
Discussion
SR has been reported in various types of cancer,
although it is considered unusual (9). Cole (9,10) reported
that immunological reactions play an important role in this rare
event (10) and SR of tumors may be
caused by necrosis and rupture (9).
SR in mediastinal tumors has been reported in renal cell carcinoma,
malignant melanoma and neuroblastoma (9). However, SR of thymoma is rare (6–8). Moran and
suster (1) reported 25 cases of
thymoma with prominent hemorrhagic and necrotic changes, without a
detailed description of tumor regression.
Thymoma is generally asymptomatic (1) and the majority of the patients with
thymoma commonly present with an abnormal chest shadow, while 15%
of the cases with thymoma are associated with myasthenia gravis
(11). By contrast, all the reported
patients with SR of thymoma have presented with symptoms, such as
fever or chest pain (Table II).
These symptoms may be associated with rapid tumor enlargement prior
to regression, as was the case in our patient. One possible cause
of the rapid enlargement of thymoma prior to regression has been
reported to be disruption of the vascular supply and necrosis and
an inflammatory reaction resulting in pleural effusion (6). All the patients with sr of thymoma
presented with pleural effusion (Table
II), supporting this hypothesis. In the present case, the tumor
included prominent degenerative and necrotic areas, which was
consistent with previous reports (Table
II). Kuo (12) reported that a
hemorrhagic and necrotic thymoma may develop into a sclerosing
thymoma, due to the absorption of the hemorrhagic and necrotic
components. Clinical findings such as fever, chest pain and
elevation of serum levels of inflammatory markers are consistent
with massive necrosis (12). The
cause, mechanism and trigger of regression, as well as the cause of
necrosis, have not been clearly determined and remain a hypothesis.
Rapid tumor growth may lead to increased internal pressure,
resulting in massive necrosis and subsequent tumor regression. In
some patients, non-steroidal anti-inflammatory drugs were
administered for subjective symptoms. Thymoma regression during
corticosteroid treatment has been reported (4) and may be associated with stress and
increased steroid levels. Some cases are believed to be caused by
vascular insufficiency and thrombus formation (8), which was not observed in our
patient.
| Table II.Reported cases of SR of thymoma. |
Table II.
Reported cases of SR of thymoma.
|
|
|
|
| Symptoms |
| Pathological
findings |
|
|
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| No. | Author | Age, years | Gender | Chest pain | Fever | Masaoka stage | Necrosis | WHO type | Size before SR,
mm | Pleural effusion | CYFRA, ng/ml | Size after SR,
mm | Reduction rate,
% | Duration of SR | Refs. |
|---|
| 1 | Okagawa et
al | 31 | F | + | + | II | + | B2 | 60×55×50 | + | ND | 45×40×30 | 67.3 | 3 weeks | (7) |
| 2 | Yutaka et
al | 47 | M | + | ND | I | + | B3 | 80×70×60 | + | 40 | 60×30×20 | 89.3 | 1 month | (6) |
| 3 | Fukui et
al | 43 | F | + | ND | II | + | B2 | 34×34×27 | + | ND | 14×12×8 | 95.7 | 1.5 months | (8) |
| 4 | Fukui et
al | 32 | F | + | + | IV | + | B2 | 100×95×79 | + | ND | 73×69×49 | 63.1 | 1 week | (8) |
| 5 | Present case | 30 | M | + | + | II | + | B2 | 110×60×50 | + | 12.7 | 80×36×30 | 73.8 | 1 month | – |
Elevation of CYFRA in the pleural effusion was
prominent in the present case, suggesting that the origin of CYFRA
may be the epithelial cells of the thymoma. CYFRA has been reported
to be a sensitive and specific marker for squamous cell lung
cancer, through detecting a fragment of the cytokeratin-19, which
is a subunit of the cytokeratin intermediate filament expressed in
simple epithelia and their malignant counterparts (13). In the present case, the level of CYFRA
was increased in the serum and pleural effusion, which had not been
previously reported (Table II). The
increased CYFRA levels may be attributed by a collapse of tumor
cells and increased cytokeratin fragment modification by
intracellular activated protease (14).
Cytokeratin is one of the intermediate filament
proteins from the cytoskeleton of epithelial cells (15) and the results of cytokeratin staining
in this case also suggests that elevation of CYFRA is caused by the
thymoma. Originally, CYFRA was used in the diagnosis, assessment of
therapeutic effectiveness and evaluation of prognosis in cancers
such as squamous cell carcinoma (16). Additionally, the present case
demonstrated that CYFRA may be useful for the evaluation of thymoma
with extensive necrosis. The serum CYFRA levels decreased without
treatment in our patient, possibly reflecting the decreased tumor
volume or massive necrotic reaction.
We herein report a case of SR of thymoma. Although
the frequency of this event is low, SR does not exclude malignancy
and surgical intervention should be considered for the residual
lesion.
References
|
1
|
Moran MD and Suster S: Thymoma with
prominent cystic and hemorrhagic changes and areas of necrosis and
infarction: A clinicopathologic study of 25 cases. Am J Surg
Pathol. 25:1086–1090. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Engels EA and Pfeiffer RM: Malignant
thymoma in the United States: Demographic patterns in incidence and
associations with subsequent malignancies. Int J Cancer.
105:546–551. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schmidt-Wolf IG, Rockstroh JK, Schüller H,
et al: Malignant thymoma: Current status of classification and
multimodality treatment. Ann Hematol. 82:69–76. 2003.PubMed/NCBI
|
|
4
|
Barratt S, Puthucheary ZA and Plummeridge
M: Complete regression of a thymoma to glucocorticoids, commenced
for palliation of symptoms. Eur J Cardiothorac Surg. 31:1142–1143.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moran CA and Suster S: ‘Ancient’
(sclerosing) thymomas: A clinicopathologic study of 10 cases. Am J
Clin Pathol. 121:867–871. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yutaka Y, Omasa M, Shikuma K, Okuda M and
Taki T: Spontaneous regression of an invasive thymoma. Gen Thorac
Cardiovasc Surg. 57:272–274. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Okagawa T, Uchida T and Suyama M: Thymoma
with spontaneous regression and disappearance of pleural effusion.
Gen Thorac Cardiovasc Surg. 55:515–517. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fukui T, Taniguchi T, Kawaguchi K and
Yokoi K: Spontaneous regression of thymic epithelial tumours.
Interact Cardiovasc Thorac Surg. 18:399–401. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cole WH: Spontaneous regression of cancer:
The metabolic triumph of the host? Ann NY Acad Sci. 230:111–141.
1974. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cole WH: Efforts to explain spontaneous
regression of cancer. J Surg Oncol. 17:201–209. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Romi F: Thymoma in myasthenia gravis: From
diagnosis to treatment. Autoimmune Dis. 2011:4745122011.PubMed/NCBI
|
|
12
|
Kuo T: Sclerosing thymoma - a possible
phenomenon of regression. Histopathology. 25:289–291. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pujol JL, Grenier J, Daurès JP, Daver A,
Pujol H and Michel FB: Serum fragment of cytokeratin subunit 19
measured by CYFRA 21-1 immunoradiometric assay as a marker of lung
cancer. Cancer Res. 53:61–66. 1993.PubMed/NCBI
|
|
14
|
Morita T, Kikuchi T, Hashimoto S,
Kobayashi Y and Tokue A: Cytokeratin-19 fragment (CYFRA 21-1) in
bladder cancer. Eur Urol. 32:237–244. 1997.PubMed/NCBI
|
|
15
|
Hsu JD, Yao CC, Lee MY, et al: True
cytokeratin 8/18 immunohistochemistry is of no use in
distinguishing between primary endocervical and endometrial
adenocarcinomas in a tissue microarray study. Int J Gynecol Pathol.
29:282–289. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rastel D, Ramaioli A, Cornillie F and
Thirion B: CYFRA 21-1, a sensitive and specific new tumour marker
for squamous cell lung cancer. Report of the first European
multicentre evaluation. CYFRA 21-1 Multicentre Study Group. Eur J
Cancer. 30A:601–606. 1994. View Article : Google Scholar : PubMed/NCBI
|