Introduction
Telomere activity is associated with malignant
potential in neoplasia (1). The
ability to maintain telomere length is a typical feature in
neoplasia and previous studies have revealed the robust expression
of telomerase reverse transcriptase (TERT) in numerous human
malignancies (2,3). Recurrent hot-spot mutations in the
TERT promoter were intitially reported in melanoma (4,5) and
subsequently in various tumor types, including primary nervous
system tumors (6). Two hot-spot
mutations, C228T and C250T, create novel binding sites for
E-twenty-six (ETS) transcription factors, resulting in a maximum 4-
to 5-fold increase in the induction of the TERT gene
(4,5).
Previous studies also demonstrated that TERT promoter
mutations occur in ~50% of SFTs of central nervous system (CNS)
origin (6). However, with the
exception of myxoid liposarcomas (MLSs), TERT promoter
mutations are relatively rare in soft tissue sarcomas, including
SFTs (7). Our previous study reported
that TERT promoter mutations are associated with poor
clinical outcomes in SFT in Japanese individuals (8). However, the tumor site-specific
frequency of TERT promoter mutations in our SFT cases
(8) appeared to be different from
previously reported values (6,7). These
findings prompted the present study to elucidate the potential role
of ethnic background in the possibly different frequencies of
TERT promoter mutations in bone and soft tissue
sarcomas.
In the present study, TERT promoter mutations
were examined in 180 cases of bone and soft tissue sarcomas to
elucidate its frequency in Japanese patients. It was demonstrated
that TERT promoter mutation rates in MLSs of Japanese
patients were lower compared with the reported values in German
patients.
Materials and methods
Sample preparation
The sarcoma tissue samples were collected from the
pathology records at the Pathology Division of Juntendo University
Hospital (Tokyo, Japan), which were surgically resected between
April 1990 and March 2010 at Juntendo University Hospital.
Diagnoses were made based on the standard histopathological
criteria in conjunction with immunohistochemical and molecular
analysis, according to the current World Health Organization
classification (9). In total, 180
cases of bone and soft tissue sarcomas were included in the present
study. Among these 180 cases, data regarding 40 SFT cases were from
our previous study (8). In addition,
3 cases of lipoblastoma and 5 cases of granular cell tumor of soft
tissue origin were also collected for comparison. The numbers and
types of bone and soft tissue tumors used in the present study are
summarized in Table I.
 | Table I.Examination TERT mutations of
bone and soft tissue tumors. |
Table I.
Examination TERT mutations of
bone and soft tissue tumors.
| Tumor type | TERT mutations
(no. cases) |
|---|
| Soft tissue
sarcomas |
|
| Myxoid
liposarcoma | 3
(13) |
| Well
differentiated liposarcoma | 0
(18) |
|
Myxofibrosarcoma | 0 (6) |
|
Pleomorphic undifferentiated
sarcoma | 1
(20) |
|
Leiomyosarcoma | 0
(19) |
|
Pleomorphic
leiomyosarcoma | 0 (5) |
|
Rhabdomyosarcoma | 0 (5) |
| Synovial
sarcoma | 0 (7) |
|
Dermatofibrosarcoma
protuberans | 0 (6) |
|
Ewing/primitive
neuroectodermal tumor | 0 (6) |
| Alveolar
soft part sarcoma | 0 (3) |
| Malignant
peripheral nerve sheath tumor | 0 (1) |
|
Extraskeletal myxoid
chondrosarcoma | 0 (1) |
| Clear
cell sarcoma | 0 (1) |
|
Endometrial stromal
sarcoma | 0 (1) |
| Malignant
granular cell tumor | 1 (2) |
| Solitary
fibrous tumor | 5
(40) |
|
Total | 10
(154) |
| Bone sarcomas |
|
|
Osteosarcoma | 0
(14) |
|
Chondrosarcoma | 0
(10) |
| Malignant
fibrous histiocytoma of bone | 0 (2) |
|
Total | 0
(26) |
| Benign tumors
(control) |
|
|
Lipoblastoma | 0 (3) |
| Granular
cell tumor | 0 (5) |
Ethics approval
This study was approved by the research Ethics
Committee of Juntendo University, School of Medicine (Tokyo,
Japan). Written informed consent was obtained from the
patients.
Mutational analysis of the TERT
promoter
The genomic DNA was extracted from each
formalin-fixed, paraffin-embedded tissue block. When isolating DNA,
the most representative tissue blocks, containing the maximum
percentage of tumor tissue were selected. The surrounding
non-tumoral tissues were manually removed by dissection to enrich
the percentage of tumor cells. The TERT promoter region
mutations were examined using polymerase chain reaction (PCR),
followed by direct sequencing with previously described primer
pairs (6). The AccuPrime™ GC-rich DNA
polymerase kit (Thermo Fisher Scientific, Inc., Waltham, MA, USA)
was used for PCR. The PCR products were electrophoresed in a 2%
agarose gel and were recovered using the QIAquick Gel Extraction
kit (Qiagen, Hilden, Germany). Isolated PCR products were
subsequently sequenced using a capillary sequencing machine 202
(3730xl Genetic Analyzer; Applied Biosystems) in the sense and
antisense directions, and were analyzed by Sequencing Analysis
V3.5.1 software (Applied Biosystems; Thermo Fisher Scientific,
Inc.). Once mutations were detected, the corresponding non-tumoral
DNA were also extracted to confirm the obtained mutations as
tumor-specific mutations.
Results
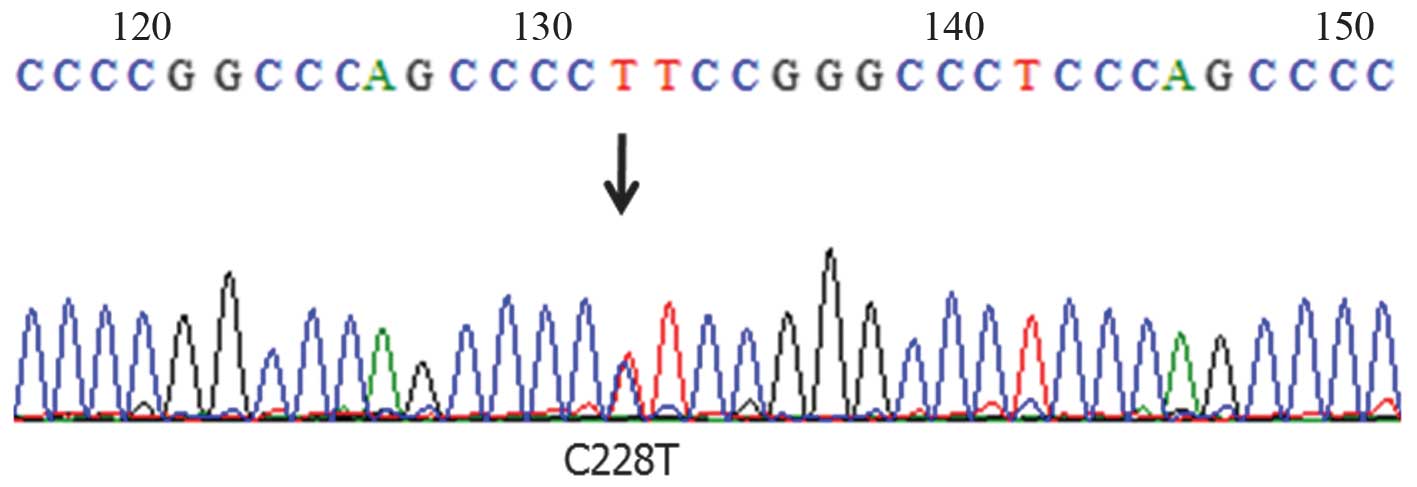
TERT promoter region mutations were
identified in 10 cases [5 SFTs, 3 MLSs (Fig. 1), 1 pleomorphic sarcoma and 1
malignant granular cell tumor]. These mutations were confirmed as
tumor-specific mutations. The clinicopathological data of cases
with TERT promoter mutations are summarized in Table II. All mutations were C228T. The
frequencies of TERT promoter mutation in MLS and pleomorphic
undifferentiated sarcoma were 23.1 (3/13) and 5% (1/20),
respectively. It was demonstrated that 2/3 MLSs with a TERT
promoter mutation contained areas with a round-cell component. It
was recently reported that TERT promoter mutations were
associated with an adverse clinical course in SFTs (8), therefore, the prognostic impact of
TERT promoter mutations in these tumors was also assessed.
However, 4/5 patients with TERT-mutated tumors experienced
no local recurrence or distant metastasis. Only 1 patient with
TERT-mutated pleomorphic sarcoma experienced lung metastasis
46 months following the wide resection of the tumor and
subsequently underwent a resection of the metastasized tumor. This
patient survived and currently exhibits no evidence of the disease.
Furthermore, TERT promoter mutations were detected in 1/2
patients with malignant granular cell tumor, although it was not
observed in any of 5 granular cell tumors.
| Table II.Clinical information of tumors with
TERT mutations. |
Table II.
Clinical information of tumors with
TERT mutations.
| Case | Age/sex | Location | Diagnosis | Mutation | Treatment | Prognosis |
|---|
| 96 | 47/F | R. lower leg | Myxoid liposarcoma
with RC | C228T | CTx+WR+CTx | NED (58 mos) |
| 276 | 58/M | R. thigh | Malignant granular
cell tumor | C228T | WR | NED (72 mos) |
| 278 | 60/M | R. thigh | Pleomorphic
sarcoma | C228T | WR | Lung metastasis (46
mos) |
|
|
|
|
|
|
| Alive with NED (103
mos) |
| 280 | 56/M | R. thigh | Myxoid
liposarcoma | C228T | WR+RTx | NED (61 mos) |
| 370 | 43/M | L. thigh | Myxoid liposarcoma
with RC | C228T | WR+CTx | NED (43 mos) |
Other mutations neighboring the hot-spots were also
noted in 3 cases, C229T in a case of synovial sarcoma, C230T in a
case of myxofibrosarcoma and C232T in a case of Ewing/primitive
neuroectodermal tumor, however, these mutations generated no
consensus binding sites for ETS transcription factors within the
TERT promoter region (10).
Discussion
Telomeres are extended by the protein complex,
telomerase, in which the enzyme TERT exerts a pivotal role
(11). TERT promoter hot-spot
mutations recently emerged as an underlying mechanism of TERT
upregulation in certain human cancer types. In SFTs of the CNS,
TERT promoter mutations were identified in 50% of cases
(6). However, in our previous study,
TERT promoter mutations were detected in 5/40 SFTs (12.5%,
0/6 of CNS origin, 2/25 of pleural/lung origin and 3/9 of soft
tissue origin (8). However, another
previous study reported that TERT promoter mutations were
observed in 4/31 (13%) SFTs of soft tissue origin (7). These findings appear to be at odds and
prompted the present study to investigate if a difference in ethnic
background may contribute to this discrepancy. In the present
study, a TERT promoter mutation in MLS was detected in 3/13
cases (23.1%), which is lower compared with a previously reported
value of 74% in this tumor type (7).
The sensitivity of the examination may affect the lower frequency
of TERT promoter mutation, however, the present study
attempted to enrich the quantities of tumor cells during DNA
isolation. These findings supported the present hypothesis that
ethnic differences may affect the frequency of TERT promoter
mutations.
In the present study, 2/3 MLSs with TERT
promoter mutations contained a round-cell component, however, there
was no association between TERT promoter mutation and the
presence of a round-cell component, consistent with previous
findings (7).
Lipoblastoma is a benign lipogenic tumor arising in
infants and younger children. The histology of lipoblastoma
overlaps with other lipomatous tumors, including MLSs, therefore,
the frequency of TERT promoter mutations was assessed in
lipoblastomas. However, 0/3 cases of this tumor type harbored a
TERT promoter mutation.
Granular cell tumor is a benign Schwann cell lesion
and typically occurs in the skin and subcutis. The clinical and
morphological criteria for malignant granular cell tumor is well
described (12). In the present
study, 2 cases of malignant granular cell tumors were included. The
clinical course in one was previously reported in detail (13), although it was the other case, which
harbored the TERT promoter mutation. Genetic alterations in
malignant granular cell tumors remain to be described in detail,
however, it has been reported that a malignant granular cell tumor
is characterized by a gain of chromosome 10 and a loss of p16
(14). Another previous report shows
that malignant granular cell tumors share certain cytogenetic
abnormalities with malignant peripheral nerve sheath tumors
(MPNSTs), leading to the hypothesis that they may represent
histogenetically associated lesions (15). The present study identified a
TERT promoter mutation in 1/2 malignant granular cell tumor
cases, however, not in a sporadic MPNST case. A previous study
demonstrated that the TERT promoter mutation is also rare in
sporadic MPNSTs and absent in neurofibromatosis type 1-associated
MPNSTs (16), although another
previous study revealed that TERT promoter hot-spot
mutations were observed in 6% of MPNSTs (7). The present study cannot comment on the
hypothesis of histogenetic similarity between malignant granular
cell tumors and MPNSTs, since the present study included only a few
cases of these tumor types. However, although malignant granular
cell tumors are relatively rare, it is of interest to further
investigate the frequency of TERT promoter mutations in
malignant granular cell tumors to elucidate the association between
TERT promoter mutations and the malignant behavior of this
tumor. TERT promoter mutations in this tumor type may be in
part driven by its presence in the dermal or subcutaneous
localization, since this type of C to T alteration is a ultraviolet
signature mutation, and TERT promoter mutations are
frequently observed in atypical fibroxanthomas and pleomorphic
dermal sarcomas (17).
In conclusion, the present study revealed the first
case, to the best of our knowledge, of malignant granular cell
tumor with a TERT promoter mutation and demonstrated that
the frequency of TERT promoter mutations in MLSs of Japanese
patients is lower compared with that reported in German
patients.
Acknowledgements
The present study was supported, in part, by a
Grant-in-Aid for General Scientific Research from the Ministry of
Education, Science, Sports and Culture, Tokyo, Japan (grant no.
26670286).
References
|
1
|
Landa I, Ganly I, Chan TA, Mitsutake N,
Matsuse M, Ibrahimpasic T, Ghossein RA and Fagin JA: Frequent
somatic TERT promoter mutations in thyroid cancer: higher
prevalence in advanced forms of the disease. J Clin Endocrinol
Metab. 98:E1562–E1566. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shay JW and Bacchetti S: A survey of
telomerase activity in human cancer. Eur J Cancer. 33:787–791.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ulaner GA, Hoffman AR, Otero J, Huang HY,
Zhao Z, Mazumdar M, Gorlick R, Meyers P, Healey JH and Ladanyi M:
Divergent patterns of telomere maintenance mechanisms among human
sarcomas: Sharply contrasting prevalence of the alternative
lengthening of telomeres mechanism in Ewing's sarcomas and
osteosarcomas. Genes Chromosomes Cancer. 41:155–162. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Horn S, Figl A, Rachakonda PS, Fischer C,
Sucker A, Gast A, Kadel S, Moll I, Nagore E, Hemminki K, et al:
TERT promoter mutations in familial and sporadic melanoma. Science.
339:959–961. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Huang FW, Hodis E, Xu MJ, Kryukov GV, Chin
L and Garraway LA: Highly recurrent TERT promoter mutations in
human melanoma. Science. 339:957–959. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Koelsche C, Sahm F, Capper D, Reuss D,
Sturm D, Jones DT, Kool M, Northcott PA, Wiestler B, Böhmer K, et
al: Distribution of TERT promoter mutations in pediatric and adult
tumors of the nervous system. Acta Neuropathol. 126:907–915. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Koelsche C, Renner M, Hartmann W, Brandt
R, Lehner B, Waldburger N, Alldinger I, Schmitt T, Egerer G, Penzel
R, et al: TERT promoter hotspot mutations are recurrent in myxoid
liposarcomas but rare in other soft tissue sarcoma entities. J Exp
Clin Cancer Res. 33:332014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Akaike K, Kurisaki-Arakawa A, Hara K,
Suehara Y, Takagi T, Mitani K, Kaneko K, Yao T and Saito T:
Distinct clinicopathological features of NAB2-STAT6 fusion gene
variants in solitary fibrous tumor with emphasis on the acquisition
of highly malignant potential. Hum Pathol. 46:347–356. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
World Health Organization (WHO)
Classification of Tumours of Soft Tissue. Fletcher CDM, Bridge JA,
Hogendoorn PCW and Mertens F: World Health Organization
International Agency for Research on Cancer. IARC Press. 2013.
|
|
10
|
Borah S, Xi L, Zaug AJ, Powell NM, Dancik
GM, Cohen SB, Costello JC, Theodorescu D and Cech TR: Cancer. TERT
promoter mutations and telomerase reactivation in urothelial
cancer. Science. 347:1006–1010. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Xu L, Li S and Stohr BA: The role of
telomere biology in cancer. Annu Rev Pathol. 8:49–78. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fanburg-Smith JC, Meis-Kindblom JM, Fante
R and Kindblom LG: Malignant granular cell tumor of soft tissue:
Diagnostic criteria and clinicopathologic correlation. Am J Surg
Pathol. 22:779–794. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Saito T, Mitomi H, Torigoe T, Takagi T,
Suehara Y, Okubo T, Kaneko K and Yao T: Malignant granular cell
tumor with an unusually long clinical course: An autopsy case with
review of literature. J Cancer Sci Ther. 4:260–263. 2012.
View Article : Google Scholar
|
|
14
|
Papachristou DJ, Palekar A, Surti U,
Cieply K, McGough RL and Rao UN: Malignant granular cell tumor of
the ulnar nerve with novel cytogenetic and molecular genetic
findings. Cancer Genet Cytogenet. 191:46–50. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Di Tommaso L, Magrini E, Consales A, Poppi
M, Pasquinelli G, Dorji T, Benedetti G and Baccarini P: Malignant
granular cell tumor of the lateral femoral cutaneous nerve: Report
of a case with cytogenetic analysis. Hum Pathol. 33:1237–1240.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dubbink HJ, Bakels H, Post E, Zwarthoff EC
and Verdijk RM: TERT promoter mutations and BRAF mutations are rare
in sporadic, and TERT promoter mutations are absent in NF1-related
malignant peripheral nerve sheath tumors. J Neurooncol.
120:267–272. 2104. View Article : Google Scholar
|
|
17
|
Griewank KG, Schilling B, Murali R,
Bielefeld N, Schwamborn M, Sucker A, Zimmer L, Hillen U, Schaller
J, Brenn T, et al: TERT promoter mutations are frequent in atypical
fibroxanthomas and pleomorphic dermal sarcomas. Mod Pathol.
27:502–508. 2014. View Article : Google Scholar : PubMed/NCBI
|