Introduction
Low-grade glioma (LGG) is often encountered in
relatively young individuals, including women of childbearing age.
Advances in the therapeutic management of LGG during the last
decade and improvements in its prognosis are expected to assist
young women with LGG in becoming pregnant. A number of case series
are found in the literature describing pregnant women with LGG,
either detected prior to pregnancy or newly diagnosed during
pregnancy (1–10). In either case, its management is a
particularly challenging situation since i) anti-tumor therapy is
required, although the impact on the fetus or the pregnancy would
require consideration or ii) the pregnancy would have to be
discontinued, depending on the severity of the disease and the
gestational age (10). Once a
pregnancy with LGG is identified, patients, families, and
neurosurgeons must recognize that they will encounter numerous
difficult decisions at each stage of the pregnancy.
The association between the behavior of the glioma
and the pregnancy remains to be elucidated. Several previous
studies have reported that the velocity of the diametric expansion
of LGG increases during pregnancy (8)
and that this acceleration may depend on multiple factors,
including hormonal factors (11),
growth factors (12), and hemodynamic
changes (1,13), associated with pregnancy.
Pilocytic astrocytoma (PA) is typically a
slow-growing astrocytoma and is therefore, considered the ‘most
benign’ of all the astrocytomas. It occurs predominantly in
childhood and adolescence (14).
Growth of PA during pregnancy is rarely reported. The present study
reported a case in which PA growth occurred and urgent resection
was required during pregnancy. The behavior of the glioma is
focussed on during the pregnancy.
Case report
A 30-year-old pregnant woman with a history of a
brainstem tumor, which developed around the dorsal midbrain,
spreading from the third to fourth ventricle was included in the
present study. Although the tumor had remained pathologically
undiagnosed, despite a biopsy at a previous medical institution,
the patient received γ-knife therapy and ventriculoperitoneal shunt
(VPS) placement at 13 years of age. The tumor remained stable
following radiosurgery and the patient had undergone several VPS
revisions for shunt malfunction during adolescence.
At 29-years-old, the patient became pregnant for the
first time. Owing to her history of the brainstem tumor and VPS
placement, she was referred to our institution at that time. She
developed an eye movement disorder during the third trimester of
the pregnancy, which suggested shunt malfunction due to the
increased intra-abdominal pressure caused by the gravid uterus. The
patient underwent a cesarean delivery (CS) and an external
ventricle drain at 36 weeks of gestation under epidural anesthesia.
Due to the patient's desire to bear more children in the future, an
endoscopic third ventriculostomy (ETV) and to withdraw from VPS
placement was planned. Therefore, two weeks following delivery, the
patient underwent an ETV and an endoscopic biopsy of the residual
tumor in the third ventricle. No pathological confirmation of
disease was detected across several specimens. The ETV was highly
effective and the VPS was removed, as planned. The post-operative
course was uneventful and the patient was discharged from hospital
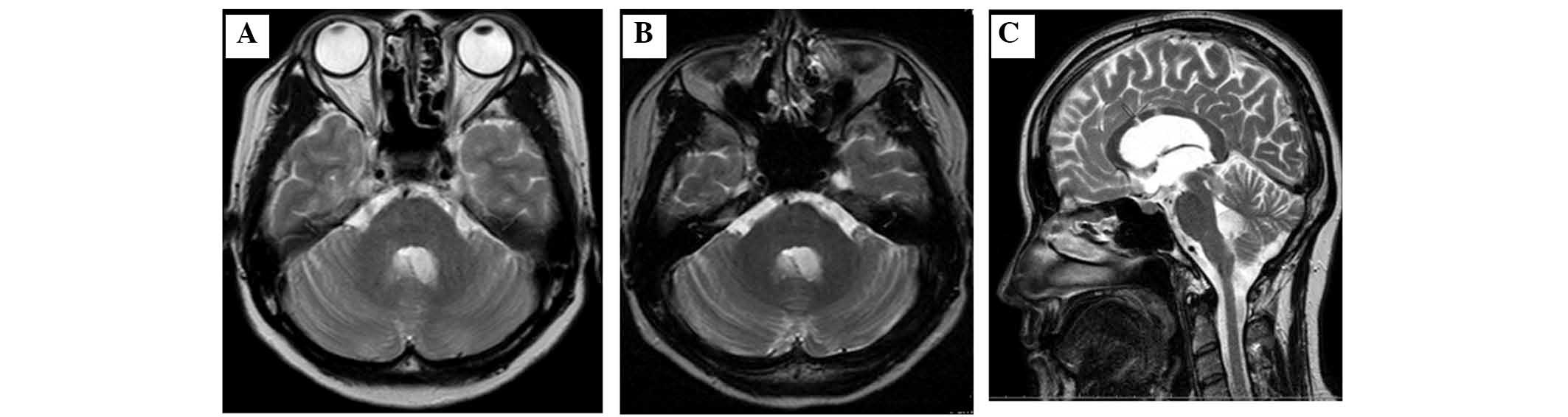
with a healthy son. Notably, no significant changes in the behavior
of the brain tumor was observed during the first pregnancy
(Fig. 1).
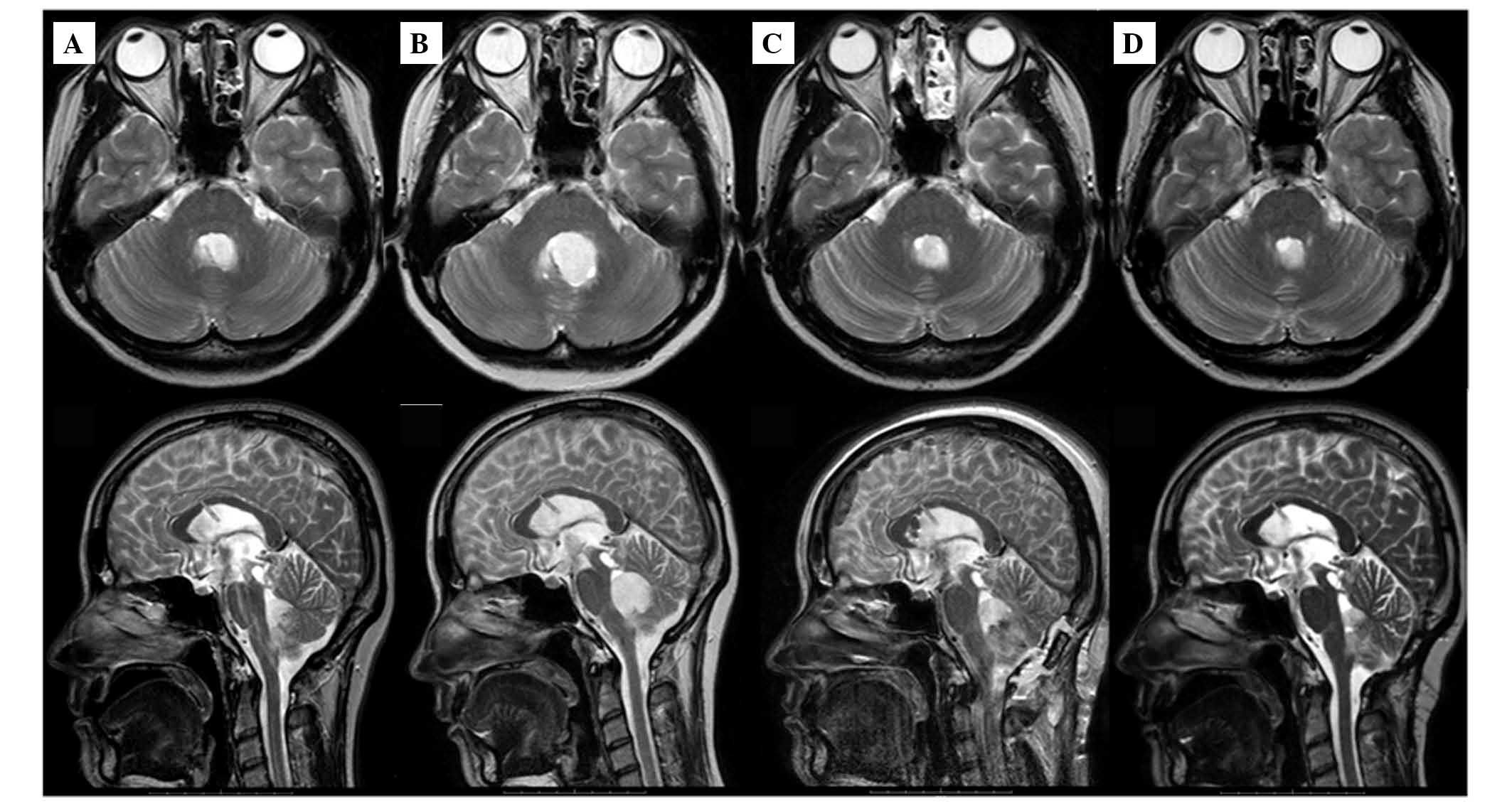
One year later, the patient became pregnant for the
second time, the patient was 30-years-old. The tumor remained
stable during the first trimester (Fig.
2A). However, she presented with nausea and headache 5 months
into the pregnancy. Magnetic resonance imaging (MRI) of the head
revealed rapid tumor growth in the fourth ventricle and cerebellum
(Fig. 2B), which necessitated an
urgent resection. At the 25-week gestation point, abortion is
prohibited. As fetal maturity was not sufficient to proceed with
the delivery, tumor resection was performed with the patient under
general anesthesia, thereby allowing the pregnancy to continue. As
the tumor had infiltrated the dorsal brainstem, a partial resection
was performed (Fig. 2C). The fetal
heart rate was monitored and a good fetal condition was maintained
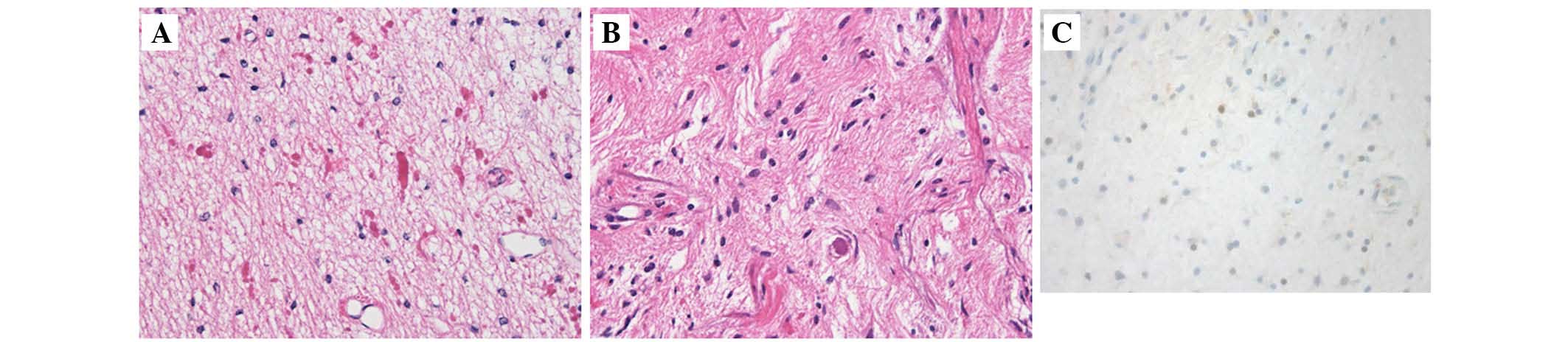
during the operation. Histological examination revealed a World
Health Organization grade I PA, with moderate cellularity exhibited
by a number of compacted bipolar cells with Rosenthal fibers and
eosinophilic granular bodies (Fig. 3A and
B). Immunostaining for progesterone receptor expression
revealed focal staining in the tumor (Fig. 3C). The patient had an uneventful
recovery and was discharged 2 weeks after the operation. At week 37
of the pregnancy, the patient delivered a healthy daughter by CS.
No complementary treatment was administered. The patient exhibited
no relapse of tumor growth during the perinatal period. By
contrast, the follow-up MRIs revealed a significantly decreased
tumor volume by up to ~50% in just 7 months following delivery
(Figs. 2D and 4).
Discussion
Glioma during pregnancy is a rare occurrence. The
incidence of malignant brain tumors in pregnancy is 3.6 per million
live births (15), and its management
is often quite difficult. The treatment of glioma during pregnancy
is complex as it may be associated with adverse effects on the
fetus. If fetal pulmonary maturity has been attained, delivery
prior to neurosurgery is preferable (16). Prompt therapy in parallel with the
pregnancy appears to be more actively required in patients with
high-grade glioma (HGG) or newly diagnosed symptomatic LGG during
pregnancy compared with in patients with known LGG (kLGG) prior to
pregnancy (2–6,9). LGG is a
slow-growing tumor and the majority of pregnant women with kLGG
give birth as planned and are less likely to receive any urgent
therapy during pregnancy (7,8,10).
Therefore, operative treatment during pregnancy for kLGG is
extremely rare. However, there are, of course, exceptions to the
clinical course of the disease. In a case series by Zwinkels et
al (10), two pregnant women with
kLGG received therapeutic abortions during the first trimester as a
result of rapid tumor progression and subsequent tumor resection
was performed (10). Daras et
al (17) reported three cases of
kLGG, which demonstrated neurological deterioration during
pregnancy or puerperium due to malignant transformation of LGG to
HGG. Of these, one patient underwent a tumor resection at 24 weeks
of gestation during her pregnancy and the other two received
radiation and chemotherapy following the gestation period. In the
present case, no option was available other than urgent surgical
treatment and the continuation of the pregnancy as the patient
presented with neurological deterioration associated with tumor
growth and fetal maturity had not been achieved.
PA is a circumscribed, slow-growing, benign
astrocytoma that occurs predominantly in childhood and adolescence
(14). Despite an extensive
literature search, only one report of a PA associated with
pregnancy exists and it had required tumor resection (6). The PA in this case was newly diagnosed
during pregnancy and surgery was performed shortly after delivery
(6). By contrast, the PA in our case
was observed carefully for 17 years and the tumor volume remained
stable until the patient's second pregnancy. Despite careful
observation, rapid tumor growth occurred during the second
pregnancy and tumor resection was performed during the pregnancy.
Although tumor growth of PA during pregnancy is extremely rare,
neurosurgeons should maintain careful observation when young women
with PAs are considering becoming pregnant.
The mechanism by which pregnancy affects glioma has
remained unclear. Pregnancy leads to major changes in the levels of
pregnancy hormones. Progesterone levels are dramatically elevated
during a pregnancy, particularly during the later stages (18). Gonzalez-Aguero et al (11) reported that progesterone induces cell
growth in human astrocytomas (11).
Khalid et al (19) suggested
that progesterone receptors may be involved in the growth of
astrocytic tumors (19). In the
present case, immunostaining for the expression of progesterone
receptor revealed focal staining in the tumor. Symptomatic
appearance in our patient began at 5 months into the pregnancy, and
the tumor volume significantly decreased following delivery. It is
possible that changes in progesterone levels induced progesterone
receptor activation and affected tumor growth and regression in our
patient.
In conclusion, the present study reported a case of
PA, which exhibited progression and required urgent neurosurgical
treatment during the patient's second pregnancy. While this was an
extremely rare event, the changes in progesterone levels during
pregnancy may have induced progesterone receptor activation and
affected tumor growth. Neurosurgeons and obstetricians should
recognize the possibility of tumor progression during each
pregnancy and the necessity of close neurological follow-up with
repeated MRIs and obstetrical monitoring, even if the histological
type is not typically malignant and no observable tumor growth
occurs during previous pregnancies. The present study is an
important clinical case of a brain tumor during pregnancy, which
gives cause for alarm.
References
|
1
|
Blumenthal DT, Parreño MG, Batten J and
Chamberlain MC: Management of malignant gliomas during pregnancy: A
case series. Cancer. 113:3349–3354. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cohen-Gadol AA, Friedman JA, Friedman JD,
Tubbs RS, Munis JR and Meyer FB: Neurosurgical management of
intracranial lesions in the pregnant patient: A 36-year
institutional experience and review of the literature. J Neurosurg.
111:1150–1157. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Isla A, Alvarez F, Gonzalez A,
García-Grande A, Perez-Alvarez M and García-Blazquez M: Brain tumor
and pregnancy. Obstet Gynecol. 89:19–23. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Johnson N, Sermer M, Lausman A and Maxwell
C: Obstetric outcomes of women with intracranial neoplasms. Int J
Gynaecol Obstet. 105:56–59. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lynch JC, Gouvêa F, Emmerich JC,
Kokinovrachos G, Pereira C, Welling L and Kislanov S: Management
strategy for brain tumour diagnosed during pregnancy. Br J
Neurosurg. 25:225–230. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nishio S, Morioka T, Suzuki S, Takeshita
I, Ikezaki K, Fukui M and Nakano H: Primary brain tumours
manifesting during pregnancy: Presentation of six cases and a
review of the literature. J Clin Neurosci. 3:334–337. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pallud J, Duffau H, Razak RA,
Barbarino-Monnier P, Capelle L, Fontaine D, Frenay M, Guillet-May
F, Mandonnet E and Taillandier L: Influence of pregnancy in the
behavior of diffuse gliomas: Clinical cases of a French glioma
study group. J Neurol. 256:2014–2020. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pallud J, Mandonnet E, Deroulers C,
Fontaine D, Badoual M, Capelle L, Guillet-May F, Page P, Peruzzi P
and Jouanneau E: Pregnancy increases the growth rates of World
Health Organization grade II gliomas. Ann Neurol. 67:398–404.
2010.PubMed/NCBI
|
|
9
|
Sneed PK, Albright NW, Wara WM, Prados MD
and Wilson CB: Fetal dose estimates for radiotherapy of brain
tumors during pregnancy. Int J Radiat Oncol Biol Phys. 32:823–830.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zwinkels H, Dörr J, Kloet F, Taphoorn MJ
and Vecht CJ: Pregnancy in women with gliomas: A case-series and
review of the literature. J Neurooncol. 115:293–301. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
González-Agüero G, Gutiérrez AA,
González-Espinosa D, Solano JD, Morales R, González-Arenas A,
Cabrera-Muñoz E and Camacho-Arroyo I: Progesterone effects on cell
growth of U373 and D54 human astrocytoma cell lines. Endocrine.
32:129–135. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schlenska-Lange A, Knüpfer H, Lange TJ,
Kiess W and Knüpfer M: Cell proliferation and migration in
glioblastoma multiforme cell lines are influenced by insulin-like
growth factor I in vitro. Anticancer Res. 28:1055–1060.
2008.PubMed/NCBI
|
|
13
|
Ducray F, Colin P, Cartalat-Carel S,
Pelissou-Guyotat I, Mahla K, Audra P, Gaucherand P, Honnorat J and
Trouillas P: Management of malignant gliomas diagnosed during
pregnancy. Rev Neurol (Paris). 162:322–329. 2006.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Huang H, Hara A, Homma T, Yonekawa Y and
Ohgaki H: Altered expression of immune defense genes in pilocytic
astrocytomas. J Neuropathol Exp Neurol. 64:891–901. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Haas JF, Jänisch W and Staneczek W: Newly
diagnosed primary intracranial neoplasms in pregnant women: A
population-based assessment. J Neurol Neurosurg Psychiatry.
49:874–880. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tewari KS, Cappuccini F, Asrat T, Flamm
BL, Carpenter SE, Disaia PJ and Quilligan EJ: Obstetric emergencies
precipitated by malignant brain tumors. Am J Obstet Gynecol.
182:1215–1221. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Daras M, Cone C and Peters KB: Tumor
progression and transformation of low-grade glial tumors associated
with pregnancy. J Neurooncol. 116:113–117. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li R, Scanlon KS and Serdula MK: The
validity and reliability of maternal recall of breastfeeding
practice. Nutr Rev. 63:103–110. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Khalid H, Shibata S, Kishikawa M, Yasunaga
A, Iseki M and Hiura T: Immunohistochemical analysis of
progesterone receptor and Ki-67 labeling index in astrocytic
tumors. Cancer. 80:2133–2140. 1997. View Article : Google Scholar : PubMed/NCBI
|