Introduction
Renal cell carcinoma (RCC) represents ~3% of all
adult cancers (1). Approximately 30%
of RCC patients have metastatic disease at the time of diagnosis,
and another 20–30% develop metastases after surgical treatment
(2). To date, no specific serum
biomarker has been shown to improve the predictive accuracy of the
current prognostic system for RCC; thus, preoperative prediction of
disease progression after surgery is difficult (3). Developing a specific molecular biomarker
to predict surgical outcome is crucial for elucidating the
mechanism underlying metastasis and recurrence in RCC, resulting in
discovery of novel therapeutic agents. The discovery and clinical
development of targeted agents have expanded treatment options in
metastatic RCC. However, metastatic RCC remains a lethal disease.
Complete response is rare and treatment with targeted agents
eventually fails in the majority of the patients (2,3).
Therefore, there is an urgent need for developing a prognostic tool
and a novel therapeutic agent for RCC.
The omega-3 fatty acids (FAs), including α-linolenic
acid (ALA), eicosapentaenoic acid (EPA) and docosahexaenoic acid
(DHA), are long-chain polyunsaturated FAs with the first double
bond on the third carbon from the methyl end of the chain. Omega-3
FAs are essential nutrients that cannot be synthesized in the body
and must be obtained from the diet.EPA and DHA are abundant in fish
oil (4) and fish oil supplements and
fatty fish, such as salmon and tuna, are particularly rich sources
of FAs, which are important dietary components for health
maintenance and disease prevention. Increased consumption of
omega-3 FAs has been shown to be associated with a lower incidence
of various types of cancer, including colon (5), breast (6,7) and
prostate cancer (6,7). Omega-3 FAs have been shown to exert a
variety of antitumor effects, such as antitumor angiogenesis
(8), induction of cancer cell
apoptosis (9), inhibition of tumor
invasion and metastasis (10,11), and attenuation of signaling pathways
(12). The antitumor effects of
omega-3 FAs have been suggested by clinical reports demonstrating
that higher intakes of EPA and DHA reduced the risk of mortality in
women treated for breast cancer (13,14). The
administration of DHA during anthracyclin-based chemotherapy
against metastatic breast cancer improved the outcome of
chemotherapy, suggesting that omega-3 FAs may be effective
adjuvants (15).
In the present study, we investiagted the serum DHA
level in RCC patients and evaluated the effect of DHA level on
pathological parameters and surgical outcome.
Patients and methods
Patients
A total of 112 patients who underwent surgical
treatment for RCC at the National Defense Medical College
(Tokorozawa, japan) between July, 2003 and April, 2009 were
included in this study. The characteristics of the patients
examined are summarized in Table I.
Cachexia is defined as a condition with weight loss and/or
hypoalbuminemia (≤3.8 mg/dl) and/or anorexia and malaise prior to
surgical treatment. Clinical staging was performed according to the
2009 TMN staging system, using computed tomography (CT) scans of
the chest, abdomen and pelvis. All tumor tissues were evaluated in
terms of pathological staging and histological grading according to
the TNM and the 2004 WHO classification of the renal tumors of the
adults (16). Disease progression was
defined as evidence of recurrence or metastasis on periodic CT of
the chest, abdomen and pelvis, or physical examinations. This study
was conducted following permission of the ethics committee of our
institute.
 | Table I.Patient characteristics prior to
surgical treatment. |
Table I.
Patient characteristics prior to
surgical treatment.
| Characteristics | No. | % |
|---|
| Age, years |
|
|
| Mean
(median) | 61.2 (63) |
|
|
Range | 36–82 |
|
| Gender |
|
|
|
Male | 88 | 78.57 |
|
Female | 24 | 21.43 |
| pT stage |
|
|
| T1a | 50 | 44.64 |
| T1b | 31 | 27.68 |
| T2a | 10 | 8.93 |
| T2b | 2 | 1.79 |
| T3a | 6 | 5.36 |
| T3b | 12 | 10.71 |
| T3c | 0 | 0.00 |
| T4 | 1 | 0.89 |
| N stage |
|
|
| N0 | 111 | 99.11 |
| N1 | 1 | 0.89 |
| M stage |
|
|
| M0 | 97 | 86.61 |
| M1 | 15 | 13.39 |
| Histological
subtype |
|
|
| Clear
cell | 105 | 93.75 |
|
Chromophobe | 4 | 3.57 |
|
Papillary | 3 | 2.68 |
| Treatment |
|
|
|
Radical | 97 | 86.61 |
|
Partial | 15 | 13.39 |
Serum FA profile
The levels and distribution profile of FAs in serum
samples collected in the morning of the day of operation were
measured by a transesterification method described previously
(17). In brief, FA methyl esters
were chromatographed on a 30×0.25 mm internal diameter DB-23 column
(J&W Scientific, Santa Clara, CA, USA), with a film thickness
of 0.25 mm and a cyanopropyl/polysiloxane phase. Analysis was
performed on a Dani 3800 GC programmed temperature vaporizer system
(the injector temperature was raised from 50 to 250°C within 9–50
sec) equipped with a flame ionization detector (detector
temperature, 260°C) and a Shimadzu C-R1B integration unit (all from
Shimadzu, Kyoto, Japan). The carrier gas was helium, flowing at 3
ml/min. The injected sample volume was 1 ml and the split rate was
1:10 (solvent split). The column temperature was increased from 130
to 240°C at 2°C/min. The peak quantification was based on peak area
comparison with the internal standard (17:0,100 mg). the
concentration of DHA as well as the proportion of DHA as a
percentage of the total FA content were indicated. We examined the
proportion as well as the concentration of the serum DHA in
preoperative patients, as both have been shown to be significant
predictors in patients with breast cancer or neuroblastoma
(15,18).
Statistical analysis
The results are expressed as mean value ± standard
error for three independent experiments. The Mann-Whitney U test
was used to compare the serum levels of the FA profile in different
groups. Cancer-specific survival was evaluated by the Kaplan-Meier
method, and survival differences were compared using the log-rank
test. Univariate and multivariate Cox proportional hazards models
were used to assess the effect of independent predictors on
time-to-event outcomes. P-values <0.05 were considered to
indicate statistically significant differences.
Results
Preoperative FA levels and
clinicopathological characteristics
The patient characteristics are summarised in
Table I. Of the 112 patients, 81
presented with locally confined disease (T1–2), while 31 presented
with locally advanced disease (T3–4). Of the 112 patients, 97 had
no metastasis (M0), whereas 15 presented with metastasis (M1).
Radical nephrectomy was performed in 97 cases and partial
nephrectomy was performed in 15 cases. We first analyzed the
associations between clinicopathological parameters and the serum
level of omega-3 FAs in serum FA composition (Table II). The mean level of ALA in patients
with T1–2 disease was significantly higher compared with that in
patients with T3–4 disease (P=0.02). The mean level of DHA in
patients without any metastasis (N0M0) was significantly higher
compared with that in patients with metastatic disease (N+ and/or
M+, P=0.047).
| Table II.Association between serum omega-3 FA
levels and pathological parameters. |
Table II.
Association between serum omega-3 FA
levels and pathological parameters.
| Parameters | No. | n-3 PUFA (%) | P-value | ALA (%) | P-value | EPA (%) | P-value | DHA (%) | P-value |
|---|
| Gender |
|
|
0.093 |
| 0.248 |
| 0.046 |
| 0.274 |
| Male | 88 | 6.84±0.22 |
| 0.71±0.02 |
| 2.17±0.10 |
| 3.95±0.14 |
|
|
Female | 24 | 6.02±0.43 |
| 0.66±0.04 |
| 1.74±0.19 |
| 3.62±0.26 |
|
| ECOG PS |
|
| 0.258 |
| 0.323 |
| 0.335 |
| 0.324 |
| 0–1 | 106 | 6.71±0.21 |
| 0.71±0.02 |
| 2.10±0.09 |
| 3.91±0.13 |
|
|
>2 |
6 | 5.70±0.86 |
| 0.62±0.08 |
| 1.71±0.39 |
| 3.37±0.53 |
|
| BMI, kg/m2 |
|
| 0.639 |
| 0.285 |
| 0.288 |
| 0.886 |
|
<23 | 59 | 6.75±0.28 |
| 0.68±0.03 |
| 2.17±0.13 |
| 3.89±0.17 |
|
|
>23 | 53 | 6.56±0.29 |
| 0.72±0.03 |
| 1.98±0.13 |
| 3.86±0.18 |
|
| Cachexia |
|
| 0.345 |
| 0.159 |
| 0.649 |
| 0.325 |
|
Absent | 103 | 6.71±0.21 |
| 0.71±0.02 |
| 2.09±0.09 |
| 3.91±0.13 |
|
|
Present |
9 | 6.02±0.71 |
| 0.61±0.07 |
| 1.94±0.32 |
| 3.47±0.43 |
|
| T stage |
|
| 0.383 |
| 0.02 |
| 0.783 |
| 0.383 |
|
T1–2 | 93 | 6.74±0.22 |
| 0.72±0.02 |
| 2.09±0.10 |
| 3.93±0.13 |
|
|
T3–4 | 19 | 6.27±0.49 |
| 0.61±0.04 |
| 2.02±0.22 |
| 3.64±0.29 |
|
| Tumor necrosis |
|
| 0.121 |
| 0.087 |
| 0.246 |
| 0.157 |
|
Negative | 74 | 6.88±0.25 |
| 0.72±0.02 |
| 2.16±0.11 |
| 4.00±0.15 |
|
|
Positive | 38 | 6.22±0.34 |
| 0.66±0.03 |
| 1.93±0.16 |
| 3.64±0.21 |
|
| Metastasis |
|
| 0.074 |
| 0.798 |
| 0.222 |
| 0.047 |
|
N0M0 | 97 | 6.80±0.21 |
| 0.70±0.02 |
| 2.13±0.09 |
| 3.97±0.13 |
|
| N+
and/or M+ | 15 | 5.75±0.54 |
| 0.69±0.05 |
| 1.79±0.25 |
| 3.26±0.33 |
|
| Grade |
|
| 0.374 |
| 0.537 |
| 0.494 |
| 0.392 |
|
G1–2 | 72 | 6.79±0.25 |
| 0.71±0.02 |
| 2.13±0.11 |
| 3.95±0.15 |
|
| G3 | 40 | 6.42±0.34 |
| 0.69±0.03 |
| 1.99±0.15 |
| 3.74±0.20 |
|
| Venous
invasion |
|
| 0.164 |
| 0.126 |
| 0.372 |
| 0.167 |
|
Negative | 65 | 6.89±0.26 |
| 0.73±0.02 |
| 2.15±0.12 |
| 4.02±0.16 |
|
|
Positive | 47 | 6.33±0.31 |
| 0.67±0.03 |
| 1.99±0.14 |
| 3.68±0.19 |
|
| Histology |
|
| 0.419 |
| 0.924 |
| 0.691 |
| 0.309 |
| Clear
cell | 105 | 6.62±0.21 |
| 0.70±0.02 |
| 2.07±0.09 |
| 3.84±0.13 |
|
|
Others |
7 | 7.29±0.80 |
| 0.71±0.08 |
| 2.22±0.36 |
| 4.36±0.49 |
|
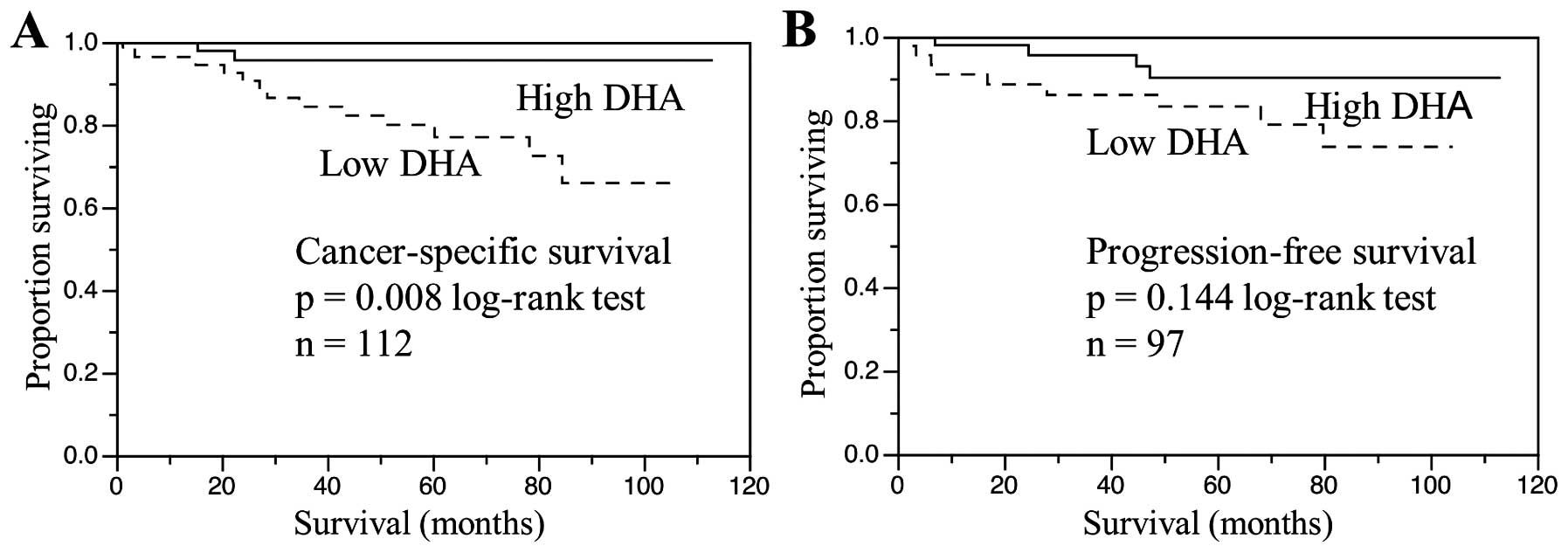
Preoperative serum DHA levels and
clinical outcome
Cancer-specific survival for patients stratified by
preoperative serum DHA level is shown in Fig. 1. The 112 patients were divided into
two groups depending on whether their DHA levels were above or
below the median value and a survival curve for each group was
generated. The cancer-specific survival of patients with a serum
DHA level below the median value was significantly shorter compared
with that in patients with a DHA level above the median value
(P=0.008; Fig. 1A). The effect of DHA
level on the progression-free survival of the 97 patients without
metastasis was evaluated by dividing the patients into two groups
depending on whether their DHA levels were above or below the
median value and a survival curve for each group was generated. The
progression-free survival of patients with a serum DHA level below
the median value was shorter compared with that in patients with a
serum DHA level above the median value; however, the difference was
not significant (P=0.144; Fig. 1B).
Other factors shown by univariate analysis to be predictive of
shortened cancer-specific survival were cachexia (P<0.0001),
more advanced tumor stage (pT3–4; P=0.0003), presence of tumor
necrosis (P=0.002), higher tumor grade (grade 3; P=0.0032),
presence of metastasis (N+ and/or M+; P<0.0001, Table III) and low DHA level (P=0.0051).
However, the multivariate Cox proportional hazards analysis of
these significant prognostic factors revealed that cachexia
(P=0.014), metastasis (P=0.023) and low DHA level (P=0.033) were
independent predictors of shortened cancer-specific survival
(Table III).
| Table III.Risk factors for cancer-specific
survival by univariate and multivariate analyses of Cox
proportional hazards model. |
Table III.
Risk factors for cancer-specific
survival by univariate and multivariate analyses of Cox
proportional hazards model.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | P-value | P-value | HR | 95% CI |
|---|
| Cachexia
(positive) | <0.0001 | 0.014 | 6.29 | 1.48–28.37 |
| T stage (T3–4) |
0.0003 | 0.21 | 2.52 | 0.58–10.35 |
| Tumor necrosis
(positive) | 0.002 | 0.644 | 1.46 | 0.29–7.45 |
| Grade (G3) |
0.0032 | 0.981 | 1.02 | 0.16–6.39 |
| Metastasis (N+
and/or M+) | <0.0001 | 0.023 | 4.71 | 1.23–23.76 |
| DHA level (lower
than median) |
0.0051 | 0.033 | 4.43 | 1.11–30.25 |
Discussion
Using the cox proportional hazards model, we
demonstrated that the preoperative low DHA level was one of the
independent predictors of shortened cancer-specific survival in RCC
patients who underwent surgical treatment. Furthermore, the DHA
level in patients with metastatic disease was found to be
significantly lower compared with that in patients without
metastatic disease. To the best of our knowledge, this is the first
report showing a association between serum DHA levels and
pathological parameters and clinical outcome following surgical
treatment in patients with RCC.
Although it has not been elucidated whether the low
preoperative DHA level is a reason or a consequence of metastatic
disease, resulting in poor cancer-specific survival, there is
accumulating evidence indicating that DHA inhibits carcinogenesis
(4), inflammation (19), angiogenesis (8) and metastasis (10) in animal and in vitro studies.
It has been reported that serum levels of omega-3 FAs in patients
with pancreatic cancer, lung cancer, or NHL are lower compared with
those in healthy controls (20,21).
Moreover, pancreatic cancer or NHL patients with more advanced
clinical stages have lower levels of serum omega-3 FAs (21,22). In
our study, there was a significant association between the presence
of metastasis and decreased serum DHA level. DHA has been shown to
reduce metastasis in animal experimental models (10,11). DHA
has been shown to prevent the migration and invasion of human
MDA-MB-231 mammary cancer cells in vitro, and a DHA-rich
fish oil diet prevents bone metastasis from breast cancer by
reducing the expression of CD44, which has been identified as a
molecular signature of cancer stem cells (10). A recent study has demonstrated that
DHA inhibited vascular endothelial growth factor (VEGF)- and
fibroblast growth factor-2-induced angiogenesis, and suppressed
primary tumor growth and metastasis in the Lewis lung carcinoma
mouse model (11). These studies
raise the possibility that reduced DHA level may lead to
progression of metastasis in patients with RCC, or that increased
DHA level may lead to suppression of metastasis.
The effect of DHA on tumor angiogenesis is pivotal,
since the hypervascularity, sustained by tumor angiogenesis, is a
hallmark of RCC. Current advances in the treatment of metastatic
RCC, supported by a better understanding of the RCC biology, are
focused on anti-angiogenesis. Although metastasis remains poorly
understood, angiogenesis is crucial for the metastatic process.
During metastatic dissemination, a cancer cell develops from the
proximal tubules and promotes angiogenesis to feed itself and to
enter the microvasculature. A cancer cell that survived the immune
system translocates through the bloodstream to the microvessels of
distant tissues, exits the bloodstream and colonizes in the distant
tissues, where angiogenesis is promoted to feed colonized tumor
cells and help them proliferate. Hypervascularity is prominent in
both primary and metastatic lesions on enhanced CT. RCCs tend to
spread either by direct invasion through the renal capsule into the
perinephric fat, or by direct extension into the renal vein.
Staging of RCC takes into account the presence of renal vein
involvement and the prognosis of T3 disease with the presence of
renal vein involvement is worse compared with that of T2 disease
(23). Angiogenesis is a hallmark of
the RCC biology and DHA possesses a variety of anti-angiogenic
properties. First, n-3 FAs, including DHA, inhibit the biosynthesis
of arachidonic acid-derived eicosanoids, which have
pro-inflammatory properties, to promote tumor angiogenesis
(4). Eicosanoids produced from n-6
FAs (arachidonic acid) stimulate inflammation and tumor
angiogenesis, while eicosanoids produced from n-3 FAs, such as EPA
and DHA, are anti-inflammatory and do not stimulate angiogenesis.
Second, epoxy metabolites of DHA, which are lipid mediators
produced by cytochrome P450 epoxygenases, inhibit angiogenesis and
metastasis (11). Finally, it was
suggested that n-3 FAs exert potent anti-angiogenic effects by
inhibiting the production of angiogenic mediators, such as VEGF,
platelet-derived growth factor, platelet-derived endothelial growth
factor, cyclo-oxygenase 2, prostaglandin E2, nitric oxide, nuclear
factor κB, matrix metalloproteinases and β-catenin (8).
It is also possible that the low DHA level is the
result of metastasis or poor cancer-specific survival, resulting in
cancer cachexia, which is one of the most common paraneoplastic
syndromes associated with RCC. Cachexia is a complex metabolic
syndrome associated with underlying illness and characterized by
loss of muscle, with or without loss of fat mass (24). Anorexia, inflammation, insulin
resistance and increased muscle protein breakdown are the most
prominent clinical characteristics of cachexia. DHA is an essential
nutrient that cannot be synthesized in the body and must be
obtained from the diet. The decreased DHA level in patients with
metastasis in this study may be the result of cancer cachexia
accompanied by anorexia or lipid metabolism changes, similar to
those described in patients with pancreatic cancer (22).
This study has several limitations. First, it was a
case-control study including only 112 patients; thus, our results
require confirmation by a large randomized control prospective
trial. Second, the mechanism underlying the association between low
DHA level and metastatic disease or poor cancer-specific survival
was not elucidated in this study. We are currently investigating
the antitumor effects of DHA, such as antitumor migration and
invasion or anti-angiogenesis, to determine whether low DHA level
is a causative factor in metastatic disease and shortened
cancer-specific survival. However, even with these limitations, our
study strongly suggests that DHA may be a useful biomarker to
predict prognosis of patients with RCC.
In conclusion, we herein demonstrated that the serum
DHA levels in RCC patients with metastasis were lower compared with
those in patients without metastasis. In addition, low serum DHA
level was an independent predictor of shortened cancer-specific
survival in a multivariate Cox proportional hazard model. Our
results suggest that the serum DHA level may be a useful biomarker
to predict prognosis in patients with RCC and personalize follow-up
strategy.
References
|
1
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J,
Murray T and Thun MJ: Cancer statistics, 2008. CA Cancer J Clin.
58:71–96. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bukowski RM: Prognostic factors for
survival in metastatic renal cell carcinoma: Update 2008. Cancer.
115(Suppl 10): S2273–S2281. 2009. View Article : Google Scholar
|
|
3
|
Sonpavde G and Choueiri TK: Biomarkers:
The next therapeutic hurdle in metastatic renal cell carcinoma. Br
J Cancer. 107:1009–1016. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Larsson SC, Kumlin M, Ingelman-Sundberg M
and Wolk A: Dietary long-chain n-3 fatty acids for the prevention
of cancer: A review of potential mechanisms. Am J Clin Nutr.
79:935–945. 2004.PubMed/NCBI
|
|
5
|
Sasazuki S, Inoue M, Iwasaki M, Sawada N,
Shimazu T, Yamaji T, Takachi R and Tsugane S: Japan Public Health
Center-Based Prospective Study Group: Intake of n-3 and n-6
polyunsaturated fatty acids and development of colorectal cancer by
subsite: Japan Public Health Center-based prospective study. Int J
Cancer. 129:1718–1729. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Terry PD, Rohan TE and Wolk A: Intakes of
fish and marine fatty acids and the risks of cancers of the breast
and prostate and of other hormone-related cancers: A review of the
epidemiologic evidence. Am J Clin Nutr. 77:532–543. 2003.PubMed/NCBI
|
|
7
|
Sonoda T, Nagata Y, Mori M, Miyanaga N,
Takashima N, Okumura K, Goto K, Naito S, Fujimoto K, Hirao Y, et
al: A case-control study of diet and prostate cancer in Japan:
Possible protective effect of traditional Japanese diet. Cancer
Sci. 95:238–242. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Spencer L, Mann C, Metcalfe M, Webb M,
Pollard C, Spencer D, Berry D, Steward W and Dennison A: The effect
of omega-3 FAs on tumour angiogenesis and their therapeutic
potential. Eur J Cancer. 45:2077–2086. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Serini S, Fasano E, Piccioni E, Monego G,
Cittadini AR, Celleno L, Ranelletti FO and Calviello G: DHA induces
apoptosis and differentiation in human melanoma cells in vitro:
Involvement of HuR-mediated COX-2 mRNA stabilization and
beta-catenin nuclear translocation. Carcinogenesis. 33:164–173.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mandal CC, Ghosh-Choudhury T, Yoneda T,
Choudhury GG and Ghosh-Choudhury N: Fish oil prevents breast cancer
cell metastasis to bone. Biochem Biophys Res Commun. 402:602–607.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang G, Panigrahy D, Mahakian LM, Yang J,
Liu JY, Lee Stephen KS, Wettersten HI, Ulu A, Hu X, Tam S, et al:
Epoxy metabolites of docosahexaenoic acid (DHA) inhibit
angiogenesis, tumor growth, and metastasis. Proc Natl Acad Sci USA.
110:6530–6535. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rogers KR, Kikawa KD, Mouradian M,
Hernandez K, McKinnon KM, Ahwah SM and Pardini RS: Docosahexaenoic
acid alters epidermal growth factor receptor-related signaling by
disrupting its lipid raft association. Carcinogenesis.
31:1523–1530. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Patterson RE, Flatt SW, Newman VA,
Natarajan L, Rock CL, Thomson CA, Caan BJ, Parker BA and Pierce JP:
Marine fatty acid intake is associated with breast cancer
prognosis. J Nutr. 141:201–206. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Vaughan VC, Hassing MR and Lewandowski PA:
Marine polyunsaturated fatty acids and cancer therapy. Br J Cancer.
108:486–492. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bougnoux P, Hajjaji N, Ferrasson MN,
Giraudeau B, Couet C and Le Floch O: Improving outcome of
chemotherapy of metastatic breast cancer by docosahexaenoic acid: A
phase II trial. Br J Cancer. 101:1978–1985. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lopez-Beltran A, Scarpelli M, Montironi R
and Kirkali Z: 2004 WHO classification of the renal tumors of the
adults. Eur Urol. 49:798–805. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sattler W, Puhl H, Hayn M, Kostner GM and
Esterbauer H: Determination of fatty acids in the main lipoprotein
classes by capillary gas chromatography: BF3/methanol
transesterification of lyophilized samples instead of Folch
extraction gives higher yields. Anal Biochem. 198:184–190. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gleissman H, Segerström L, Hamberg M,
Ponthan F, Lindskog M, Johnsen JI and Kogner P: Omega-3 fatty acid
supplementation delays the progression of neuroblastoma in vivo.
Int J Cancer. 128:1703–1711. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Surette ME: The science behind dietary
omega-3 fatty acids. CMAJ. 178:177–180. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zuijdgeest-van Leeuwen SD, van der Heijden
MS, Rietveld T, van den Berg JW, Tilanus HW, Burgers JA, Wilson JH
and Dagnelie PC: Fatty acid composition of plasma lipids in
patients with pancreatic, lung and oesophageal cancer in comparison
with healthy subjects. Clin Nutr. 21:225–230. 2002. View Article : Google Scholar
|
|
21
|
Cvetković Z, Vucić V, Cvetković B,
Petrović M, Ristić-Medić D, Tepsić J and Glibetić M: Abnormal fatty
acid distribution of the serum phospholipids of patients with
non-Hodgkin lymphoma. Ann Hematol. 89:775–782. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Macášek J, Vecka M, Žák A, Urbánek M,
Krechler T, Petruželka L, Staňková B and Zeman M: Plasma fatty acid
composition in patients with pancreatic cancer: Correlations to
clinical parameters. Nutr Cancer. 64:946–955. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kim SP, Alt AL, Weight CJ, Costello BA,
Cheville JC, Lohse C, Allmer C and Leibovich BC: Independent
validation of the 2010 American Joint Committee on Cancer TNM
classification for renal cell carcinoma: Results from a large,
single institution cohort. J Urol. 185:2035–2039. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ebadi M and Mazurak VC: Evidence and
mechanisms of fat depletion in cancer. Nutrients. 6:5280–5297.
2014. View Article : Google Scholar : PubMed/NCBI
|