Introduction
High-grade gliomas [HGG; grade III/IV according to
the World Health Organization (WHO) classification] are the most
common primary malignant brain tumors in adults, comprising >50%
of all cases (1). At present, the
standard therapy consists of maximal safe surgical resection
followed by local brain radiotherapy with concurrent and adjuvant
temozolomide (TMZ) chemotherapy (2,3). However,
despite aggressive treatment, the median overall survival (OS) of
glioblastoma multiforme (GBM) patients after diagnosis is only 14.6
months (2). Recurrence of HGG appears
to be unavoidable. The postoperative treatment for HGG was changed
from whole-brain radiation therapy (WBRT) plus chemotherapy with
carmustine, semustine and dacarbazine (4), to local brain radiotherapy plus TMZ
chemotherapy (2). As the irradiated
brain volume is associated with radiation neurotoxicity, target
delineation is crucial in radiation therapy for glioma.
The Radiation Therapy Oncology Group (RTOG) have
provided a protocol for the delineation of the clinical target
volume (CTV), including peritumoral edema, for the planning of
postoperative radiotherapy for HGG. Historical RTOG protocols,
including RTOG 83–02, 86–12 and 97–10, included peritumoral edema
in the CTV (5–7). Initial CTV is defined as the gross tumor
volume (GTV; postoperative residual tumor and cavity) plus
peritumoral edema with an additional 2-cm margin (radiation dose,
46 Gy); and boost CTV is defined as the GTV with an additional
2.5-cm margin (radiation dose, 60 Gy). The irradiated brain volume
is relatively large, according to the RTOG protocol. However, Chang
et al (8) argued that CTV
delineation using postoperative residual tumor and cavity plus a
2-cm margin, rather than intentionally including peritumoral edema,
did not appear to alter the central pattern of failure for patients
with GBM. Minniti et al (9)
and other European studies (2,10) also
concluded that a smaller CTV including the postoperative residual
tumor and cavity plus a 2-cm margin, compared with CTV expanded to
include the edema, reduced the volume of normal brain tissue
subjected to high-dose irradiation, without increasing the risk of
marginal recurrence, which was in accordance with the findings of
Chang et al (8).
There is currently no consensus regarding target
delineation for HGG, whereas the association between smaller HGG
target delineation and patterns of tumor recurrence has not been
extensively investigated in Asian populations. A smaller target
delineation protocol with a limited margins was adopted in our
institution. In the present study, the patterns of recurrence in 54
HGG patients following TMZ-based chemoradiation were investigated
with regards to their correlation with the reduced target
delineation protocol.
Patients and methods
Patients
The clinical data and serial magnetic resonance
images (MRI) of 54 patients with recurrent HGG were retrospectively
evaluated. Of the 54 patients, 33 were men and 21 were women. The
median age was 54 years (range, 22–77 years) and the median
Karnofsky performance status was 85 (range, 30–90). A total of 27
patients underwent gross total resection, 25 patients underwent
subtotal resection and 2 patients underwent biopsy only. A total of
37 patients were pathologically confirmed as having GBM and the
remaining 17 patients as having grade III anaplastic glioma
according to the WHO classification (anaplastic astrocytoma, n=10;
anaplastic oligodendroglioma, n=5; and anaplastic oligoastrocytoma,
n=2) between June 2011 and June 2014. All the patients had received
TMZ-based chemoradiation within 2–4 weeks after surgery, followed
by adjuvant TMZ chemotherapy. The clinicopathological
characteristics of the patients are listed in Table I.
 | Table I.Characteristics of patients with
recurrent high-grade glioma (n=54). |
Table I.
Characteristics of patients with
recurrent high-grade glioma (n=54).
| Characteristics | Patients, n (%) |
|---|
| Gender |
|
| Male | 33 (61.1) |
|
Female | 21 (38.9) |
| Type of surgery |
|
| Gross
total resection | 27 (50.0) |
| Subtotal
resection | 25 (46.3) |
| Biopsy
only | 2 (3.7) |
| Pathological
diagnosis |
|
|
Glioblastoma | 37 (68.5) |
|
Anaplastic astrocytoma | 10 (18.5) |
|
Anaplastic
oligodendroglioma | 5 (9.3) |
|
Anaplastic
oligoastrocytoma | 2 (3.7) |
| Age at diagnosis
(years) |
|
|
Median | 54 |
|
Range | 22–77 |
| Karnofsky performance
status |
|
|
Median | 85 |
|
Range | 30–90 |
Approval of the present retrospective analysis of
the patient data was obtained from the Ethics Committee of the
Second Affiliated Hospital of Zhejiang University School of
Medicine (Hangzhou, China).
Radiotherapy and chemotherapy
Radiotherapy commenced within 2–4 weeks after
surgery. Patients were simulated and treated using a thermoplastic
mask for immobilization. The computed tomography (CT) scan obtained
at simulation was fused with available post-contrast T1-weighted
MRI and the treatment volume was contoured on the fused images. The
standard prescribed dose was 60 Gy (2 Gy per daily fraction from
Monday to Friday) over a period of 6 weeks. A 6-MV photon beam was
delivered by a Varian Trilogy (Varian Medical Systems, Palo Alto,
CA, USA) or Siemens Oncor (Siemens AG, Munich, Germany) linear
accelerator using a multileaf collimator. According to our
protocol, GTV was defined as the resection cavity and any residual
contrast-enhancing tumor on post-contrast T1-weighted MRI, ignoring
any edematous region. CTV1 was defined as GTV with an added 1-cm
margin and CTV2 as GTV with an added 2-cm margin. Peritumoral edema
was not intentionally included in the delineation of the CTV,
except for any edema existing within the added margin. A 3-mm
margin was applied to CTV1 and CTV2 to obtain planning target
volume (PTV)1 and PTV2, respectively. For intensity-modulated
radiotherapy (IMRT) planning, the dose prescribed for CTV2 was 54
Gy in 30 fractions and the dose for CTV1 was 60 Gy in 30 fractions
as a simultaneously integrated boost.
Concomitant chemotherapy consisted of TMZ at 75
mg/m2/day, administered 7 days per week from the first
day of radiotherapy. Adjuvant TMZ chemotherapy was performed for 4
weeks after the end of radiotherapy (administered over 5 days every
28 days for ≤6 cycles). The dose of TMZ was 150 mg/m2
for the first cycle and was increased to 200 mg/m2 from
the second cycle onwards if the chemotherapy was well-tolerated.
The dose was reduced or TMZ was suspended in patients with disease
progression or RTOG grade 3–4 toxicity.
MRI examination and assessment of
recurrence
Contrast-enhanced MRI of the brain was performed
prior to radiotherapy, between the end of radiotherapy and the
first cycle of adjuvant TMZ, and every 2 months thereafter or
according to the patient's neurological status. The MRI examination
protocol included axial T1- and T2-weighted images, as well as
axial, sagittal and coronal post-contrast T1-weighted images.
According to the current response assessment criteria of the
Neuro-Oncology Working Group (11),
radiological recurrence was defined as an increase of 25% or more
in the sum of the products of perpendicular diameters of enhancing
lesions (compared with baseline if no decrease), or appearance of
new lesions. Pseudoprogression in HGG patients often occurred
within 2–6 months after the completion of concomitant
chemoradiation, disappearing spontaneously within a few months
(12–14). Therefore, an asymptomatic increasing
lesion around or within the original tumor region, later resolving
or regressing, was considered as pseudoprogression (13,15,16), while
increasing contrast-enhancing lesions, which continued to progress
on serial MRI scans, were defined as tumor recurrence. Recurrence
was recorded at the time of the first MRI examination showing tumor
progression.
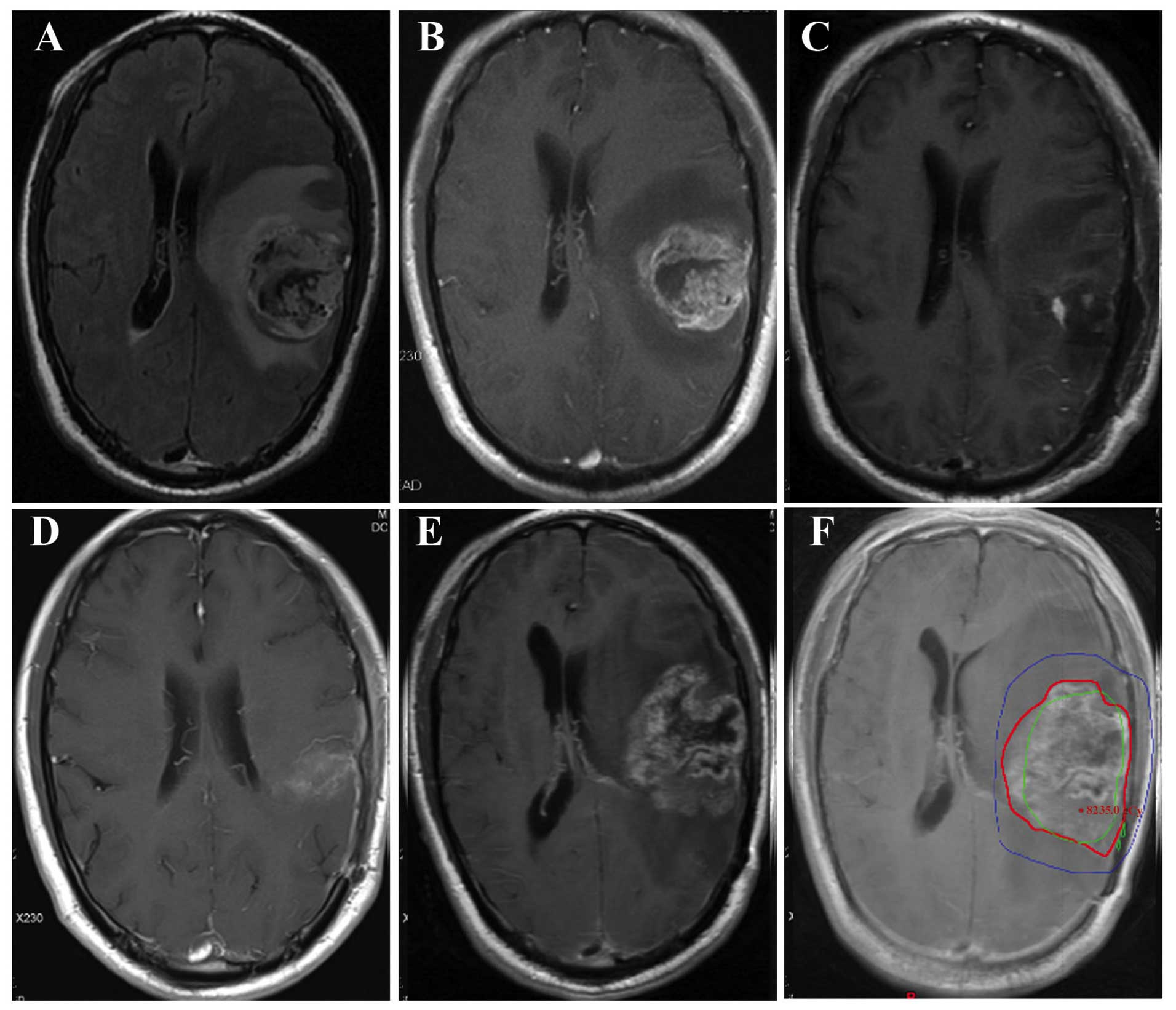
The axial post-contrast T1-weighted images first
showing tumor recurrence were imported into the Eclipse Treatment
Planning System (Varian Medical Systems) and fused with the
planning CT images with associated composite dose distribution. MRI
scans obtained immediately prior to and following recurrence were
carefully examined to identify the recurrent tumor. The recurrent
tumor was contoured and its volume (Vrecur) was
determined based on the CT and fused MRI data sets.
Vrecur was delineated without knowledge of the original
irradiation volumes, to reduce bias in volume delineation (Fig. 1), and was correlated with the 60-Gy
isodose line (IDL) in all patients with recurrence. The recurrence
patterns were classified as follows: Central recurrence, >95% of
the Vrecur inside the 60-Gy IDL; in-field recurrence,
80–95% of the Vrecur inside the 60-Gy IDL; marginal
recurrence, 20–80% of the Vrecur inside the 60-Gy IDL;
and distant recurrence, <20% of the Vrecur inside the
60-Gy IDL (8,17,18).
Cerebrospinal fluid dissemination (CSF-d) was considered as another
independent recurrence pattern.
Follow-up
The follow-up time was calculated from the date of
pathological diagnosis. OS was calculated using the Kaplan-Meier
survival analysis and was defined as the time from the day of
pathological diagnosis until death or the last follow-up. The time
to recurrence was defined from the day of pathological diagnosis
until disease recurrence. Statistical analysis was performed with
the Statistical Package for Social Sciences, version 19.0 (IBM
Corp., Armonk, NY, USA).
Results
Patient survival
The median follow-up time was 14 months. For GBM
cases, the median OS was 13.0 months [95% confidence interval (CI):
13.4–23.5 months] and the 1-year and 2-year OS rates were 70.3 and
18.9%, respectively. The median progression-free survival (PFS) was
9.0 months (95% CI: 7.6–16.6 months) and the 1-year and 2-year PFS
rates were 29.7 and 8.1%, respectively.
For anaplastic glioma cases, the median OS was 17.0
months (95% CI: 13.5–22.2 months) and the 1-year and 2-year OS
rates were 82.4 and 17.6%, respectively. The median PFS was 12.0
months (95% CI: 9.8–17.0 months) and the 1-year and 2-year PFS
rates were 47.1 and 11.8%, respectively.
Recurrence patterns
As shown in Table II,
34 patients (63.0%) developed central recurrence at a median
interval of 11 months after pathological confirmation (range, 2–30
months), 8 patients (14.8%) developed in-field recurrence at a
median interval of 9 months (range, 3–11 months), 2 patients (3.7%)
developed marginal recurrence at 2 and 58 months, 2 patients (3.7%)
developed distant recurrence at 2 and 35 months, and 11 patients
(20.4%) developed CSF-d at a median interval of 10 months (range,
5–58 months), 2 of whom developed central recurrence, with 1
patient simultaneously developing marginal recurrence. A
representative case of GBM recurrence is presented in Fig. 1.
| Table II.Recurrence patterns and time to
recurrence in patients with high-grade glioma. |
Table II.
Recurrence patterns and time to
recurrence in patients with high-grade glioma.
| Recurrence
pattern | Patients, n (%) | Time to recurrence
(months), median (range) | Recurrence rate at 1
year (%) | Recurrence rate at 2
years (%) |
|---|
| Central
recurrence | 34 (63.0) | 11 (2–30) | 56 | 94 |
| In-field
recurrence | 8 (14.8) | 9
(3–11) | 100 | 100 |
| Marginal
recurrence | 2 (3.7) | 30 (2–58) | 50 | 50 |
| Distant
recurrence | 2 (3.7) | 19 (2–35) | 50 | 50 |
| CSF-d | 11 (20.4) | 10 (5–58) | 55 | 82 |
Of the 11 patients who developed CSF-d, 1 patient
developed lesions on the leptomeninges of the brainstem, cervical,
thoracic and lumbar spine, and a total of 15 lesions were detected
in the other 10 cases: In the ependyma of the ipsilateral lateral
ventricle (n=6, 40.0%), in the ependyma of the contralateral
lateral ventricle (n=3, 20.0%), in the lateral cleft pool (n=3,
20.0%; 1 ipsilateral and 2 contralateral lesions) and in the
interpeduncular cistern, fourth ventricle and contralateral
pontocerebellar trigone, respectively (n=1 each, 20%).
Discussion
A smaller target delineation protocol with a limited
margin was used in the present study for TMZ-based chemoradiation
therapy in patients with HGG. Local recurrence (central and
in-field recurrence) was found to be the major recurrence pattern,
while only 2 patients (3.7%) developed marginal recurrence.
The volume of the brain subjected to irradiation is
considered to be a major factor associated with the development of
neurotoxicity, including cognitive decline and radionecrosis.
Reduction of the irradiated volume is crucial in HGG radiotherapy,
since smaller irradiation volumes may reduce radiation-associated
adverse effects. As the prognosis of HGG remains poor, quality of
life is an important consideration for patients receiving TMZ-based
chemoradiotherapy.
Before the 1980s, postoperative WBRT was used for
HGG treatment (19–21). An early study by Wallner et al
(22) reported that ~80% of GBM and
anaplastic astrocytoma recurrences after WBRT occurred within 2 cm
of the original pre-operative tumor (22). The results of the Brain Tumor
Cooperative Trial 8001 showed that partial brain radiotherapy was
as effective as WBRT (23). These
important studies provided evidence for the effectiveness of
partial-brain radiation therapy for GBM and anaplastic
astrocytoma.
To date, there is no consensus regarding the optimal
radiation volume for HGG. For example, according to the RTOG
guidelines for target delineation, the radiation volume is
significantly larger compared with that determined following the
European Organization for Research and Treatment of Cancer (EORTC)
guidelines (2,10). When considering reducing the
irradiation volume, the risk of geographic tumor miss should also
be considered. In such cases, the rate of marginal tumor recurrence
is an important index.
In a study by Milano et al (24), the RTOG guidelines for target
delineation were followed: Initial CTV was defined as peritumoral
edema with an added margin of 2 cm and a prescribed radiation dose
of 46–50 Gy, whereas boost CTV was defined as the GTV plus a
2–2.5-cm margin, with a prescribed radiation dose of 60 Gy. The
irradiated brain volume determined by these guidelines is
relatively large. Among the 39 cases with recurrence, as regards
the pattern of first recurrence, in-field recurrence occurred in
92%, marginal recurrence in 15% and distant recurrence in 13% of
the patients. A limited margin was used by McDonald et al
(25), who added a median margin of
0.7 cm to postoperative edema (T2 abnormality) to create the
initial CTV, followed by addition of a geometric 0.3- or 0.5-cm
margin to create the initial PTV. To delineate boost CTV, a 0.5-cm
margin was most commonly added to the GTV; boost PTV was calculated
by adding a further 0.3- or 0.5-cm geometric margin, and received a
dose of 60 Gy. On average, the treated boost PTV (median, 140
cm3) was 70% smaller compared with the boost PTV with a
2.5-cm margin (median, 477 cm3). Of the 41 patients with
GBM recurrence, 38 (93%) had central or in-field recurrence, 2 (5%)
had marginal recurrence and 1 (2%) had distant recurrence. A boost
PTV margin of ≤1 cm did not appear to increase the risk of marginal
recurrence.
Further reduction of radiation volume may be
possible for GBM treatment. Chang et al (8) investigated 48 cases of postoperative GBM
who were treated at the MD Anderson Cancer Center. GTV was defined
as the postoperative enhancing tumor and resection cavity; initial
CTV was defined as GTV plus a 2-cm margin, and boost CTV was
defined as the GTV plus 0.5 cm. A 5-mm margin was added to the
initial CTV and boost CTV to create the initial PTV and boost PTV,
respectively, which received 50 and 60 Gy, respectively. A total of
43 patients were found to have central or in-field recurrence, 2
had distant recurrence and 3 (6.25%) had marginal recurrence. The
authors concluded that CTV delineation using the postoperative
residual tumor and cavity plus a 2-cm margin, rather than
intentionally including peritumoral edema, resulted in a smaller
brain volume being irradiated compared with the corresponding
theoretical RTOG protocol, but did not appear to alter the central
pattern of treatment failure for patients with GBM (8).
According to recent EORTC randomized trials, Minniti
et al (9) determined the CTV
as the residual tumor and resection cavity plus a 2-cm margin. The
CTV was expanded by 0.3 cm to create the PTV to compensate for
variability in treatment setup and patient motion, and a dose of 60
Gy was delivered in 30 2-Gy fractions over a period of 6 weeks. For
each patient, a theoretical plan based on the addition of
postoperative edema plus a 2-cm margin according to the RTOG
guidelines was created and the patterns of failure were also
evaluated. Central and in-field recurrence was observed in 85,
marginal recurrence in 6 and distant recurrence in 14 patients. The
patterns of failure were similar to those previously reported
(24); however, the median brain
volume subjected to high doses of radiation in the study by Minniti
et al (9) was significantly
smaller according to the EORTC compared with the RTOG guidelines.
The authors concluded that a smaller CTV, including the
postoperative residual tumor and cavity plus a 2-cm margin, as
compared with CTV expanded to include the edema, reduced the volume
of normal brain subjected to high doses of radiation, while not
increasing the risk of marginal recurrence.
In the present study, an even smaller CTV, defined
as the enhanced residual tumor and cavity plus a 1-cm margin, was
introduced as routine treatment and a simultaneously integrated
boost IMRT was performed. The recurrence patterns were similar to
those reported by Minniti et al (9) and other European studies (2,10), with
only 2 patients (3.7%) developing marginal recurrence. The median
OS and PFS were 13 and 9.0 months, respectively, which were similar
to those reported by several prospective studies (2,9,26). As the rate of marginal recurrence was
low, it appears that the smaller irradiated volume used in the
present study was appropriate. However, clinical trials
investigating smaller irradiation volumes in GBM are required to
validate our findings.
Acknowledgements
The authors would like to thank all colleagues at
the Department of Radiation Oncology (The Second Affiliated
Hospital, Zhejiang University School of Medicine, Hangzhou, China)
for their cooperation. Financial support was received from the
National Natural Science Foundation of China (grant nos. 81071823
and 81572952).
References
|
1
|
Mirimanoff R-O: High-grade gliomas:
Reality and hopes. Chin J Cancer. 33:1–3. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stupp R, Mason WP, Van Den Bent MJ, Weller
M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn
U, et al: Radiotherapy plus concomitant and adjuvant temozolomide
for glioblastoma. N Engl J Med. 352:987–996. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stupp R, Hegi ME, Mason WP, van den Bent
MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B,
Belanger K, et al: Effects of radiotherapy with concomitant and
adjuvant temozolomide versus radiotherapy alone on survival in
glioblastoma in a randomised phase III study: 5-year analysis of
the EORTC-NCIC trial. Lancet Oncol. 10:459–466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chang C, Horton J, Schoenfeld D, Salazer
O, Perez-Tamayo R, Kramer S, Weinstein A, Nelson J and Tsukada Y:
Comparison of postoperative radiotherapy and combined postoperative
radiotherapy and chemotherapy in the multidisciplinary management
of malignant gliomas. A joint Radiation Therapy Oncology Group and
Eastern Cooperative Oncology Group study. Cancer. 52:997–1007.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nelson DF, Curran WJ Jr, Scott C, Nelson
JS, Weinstein AS, Ahmad K, Constine LS, Murray K, Powlis WD,
Mohiuddin M, et al: Hyperfractionated radiation therapy and
bis-chlorethyl nitrosourea in the treatment of malignant glioma -
possible advantage observed at 72.0 Gy in 1.2 Gy B.I.D. fractions:
Report of the Radiation Therapy Oncology Group protocol 8302. Int J
Radiat Oncol Biol Phys. 25:193–207. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Urtasun RC, Kinsella TJ, Farnan N, DelRowe
JD, Lester SG and Fulton DS: Survival improvement in anaplastic
astrocytoma, combining external radiation with halogenated
pyrimidines: Final report of RTOG 86-12, phase I–II study. Int J
Radiat Oncol Biol Phys. 36:1163–1167. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Colman H, Berkey BA, Maor MH, Groves MD,
Schultz CJ, Vermeulen S, Nelson DF, Mehta MP and Yung WK: Radiation
Therapy Oncology Group: Phase II Radiation Therapy Oncology Group
trial of conventional radiation therapy followed by treatment with
recombinant interferon-beta for supratentorial glioblastoma:
Results of RTOG 9710. Int J Radiat Oncol Biol Phys. 66:818–824.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chang EL, Akyurek S, Avalos T, Rebueno N,
Spicer C, Garcia J, Famiglietti R, Allen PK, Chao KC, Mahajan A, et
al: Evaluation of peritumoral edema in the delineation of
radiotherapy clinical target volumes for glioblastoma. Int J Radiat
Oncol Biol Phys. 68:144–150. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Minniti G, Amelio D, Amichetti M, Salvati
M, Muni R, Bozzao A, Lanzetta G, Scarpino S, Arcella A and Enrici
RM: Patterns of failure and comparison of different target volume
delineations in patients with glioblastoma treated with conformal
radiotherapy plus concomitant and adjuvant temozolomide. Radiother
Oncol. 97:377–381. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Brandes AA, Stupp R, Hau P, Lacombe D,
Gorlia T, Tosoni A, Mirimanoff RO, Kros JM and van den Bent MJ:
EORTC study 26041–22041: Phase I/II study on concomitant and
adjuvant temozolomide (TMZ) and radiotherapy (RT) with
PTK787/ZK222584 (PTK/ZK) in newly diagnosed glioblastoma. Eur J
Cancer. 46:348–354. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wen PY, Macdonald DR, Reardon DA,
Cloughesy TF, Sorensen AG, Galanis E, DeGroot J, Wick W, Gilbert
MR, Lassman AB, et al: Updated response assessment criteria for
high-grade gliomas: Response assessment in Neuro-Oncology Working
Group. J Clin Oncol. 28:1963–1972. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
de Wit MC, de Bruin HG, Eijkenboom W,
Sillevis Smitt PA and van den Bent MJ: Immediate post-radiotherapy
changes in malignant glioma can mimic tumor progression. Neurology.
63:535–537. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Taal W, Brandsma D, de Bruin HG, Bromberg
JE, Swaak-Kragten AT, Smitt PA, van Ews CA and van den Bent MJ:
Incidence of early pseudo-progression in a cohort of malignant
glioma patients treated with chemoirradiation with temozolomide.
Cancer. 113:405–410. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chaskis C, Neyns B, Michotte A, De Ridder
M and Everaert H: Pseudoprogression after radiotherapy with
concurrent temozolomide for high-grade glioma: Clinical
observations and working recommendations. Surg Neurol. 72:423–428.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Brandes AA, Franceschi E, Tosoni A, Blatt
V, Pession A, Tallini G, Bertorelle R, Bartolini S, Calbucci F,
Andreoli A, Frezza G, Leonardi M, Spagnolli F and Ermani M: MGMT
promoter methylation status can predict the incidence and outcome
of pseudoprogression after concomitant radiochemotherapy in newly
diagnosed glioblastoma patients. J Clin Oncol. 26:2192–2197. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brandsma D, Stalpers L, Taal W, Sminia P
and van den Bent MJ: Clinical features, mechanisms, and management
of pseudoprogression in malignant gliomas. Lancet Oncol. 9:453–461.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee SW, Fraass BA, Marsh LH, Herbort K,
Gebarski SS, Martel MK, Radany EH, Lichter AS and Sandler HM:
Patterns of failure following high-dose 3-D conformal radiotherapy
for high-grade astrocytomas: A quantitative dosimetric study. Int J
Radiat Oncol Biol Phys. 43:79–88. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chan JL, Lee SW, Fraass BA, Normolle DP,
Greenberg HS, Junck LR, Gebarski SS and Sandler HM: Survival and
failure patterns of high-grade gliomas after three-dimensional
conformal radiotherapy. J Clin Oncol. 20:1635–1642. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Andersen AP: Postoperative irradiation of
glioblastomas. Results in a randomized series. Acta Radiol Oncol
Radiat Phys Biol. 17:475–484. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Walker MD, Alexander E Jr, Hunt WE,
MacCarty CS, et al: Evaluation of BCNU and/or radiotherapy in the
treatment of anaplastic gliomas. A cooperative clinical trial. J
Neurosurg. 49:333–343. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shapiro WR and Young DF: Treatment of
malignant glioma. A controlled study of chemotherapy and
irradiation. Arch Neurol. 33:494–500. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wallner KE, Galicich JH, Krol G, Arbit E
and Malkin MG: Patterns of failure following treatment for
glioblastoma multiforme and anaplastic astrocytoma. Int J Radiat
Oncol Biol Phys. 16:1405–1409. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shapiro WR, Green SB, Burger PC, et al:
Randomized trial of three chemotherapy regimens and two
radiotherapy regimens and two radiotherapy regimens in
postoperative treatment of malignant glioma. Brain Tumor
Cooperative Group Trial 8001. J Neurosurg. 71:1–9. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Milano MT, Okunieff P, Donatello RS,
Mohile NA, Sul J, Walter KA and Korones DN: Patterns and timing of
recurrence after temozolomide-based chemoradiation for
glioblastoma. Int J Radiat Oncol Biol Phys. 78:1147–1155. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
McDonald MW, Shu H-KG, Curran WJ and
Crocker IR: Pattern of failure after limited margin radiotherapy
and temozolomide for glioblastoma. Int J Radiat Oncol Biol Phys.
79:130–136. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sherriff J, Tamangani J, Senthil L,
Cruickshank G, Spooner D, Jones B, Brookes C and Sanghera P:
Patterns of relapse in glioblastoma multiforme following
concomitant chemoradiotherapy with temozolomide. Br J Radiol.
86:201204142013. View Article : Google Scholar : PubMed/NCBI
|