Introduction
Lung cancer is the leading cause of cancer-related
mortality worldwide (1). More than
80% of all lung cancers are non-small-cell lung cancers (NSCLCs)
(2). Platinum-based chemotherapy has
been widely accepted as the standard treatment for advanced NSCLC
(3) and is appropriate for several
patients with lung cancer. However, the use of traditional
chemotherapeutic agents, such as platinum, has reached a
therapeutic plateau.
Erlotinib, an epidermal growth factor receptor
(EGFR) tyrosine kinase inhibitor (TKI), is an effective standard
second-line treatment for NSCLC, regardless of EGFR mutation
status (4–8). In a previous phase III study (BR.21),
erlotinib prolonged overall survival (OS) and progression-free
survival (PFS) compared with placebo when used as second- or
third-line treatment of NSCLC; the OS was 6.7 and 4.7 months
[hazard ratio (HR)=0.61; P<0.001) and the PFS was 2.2 and 1.8
months (HR=0.70; P<0.001) in the erlotinib and placebo groups,
respectively (4). According to
certain reports, erlotinib may also be effective in Japanese
patients with previously treated NSCLC, irrespective of their
EGFR mutation status (7,8).
However, driver oncogene-targeted therapy has met with great
success (9–12) and EGFR-TKIs are generally more
effective in patients with EGFR mutation-positive NSCLC.
Approximately 35–50% of the NSCLCs in East Asian patients harbor
EGFR mutations, which is higher compared with the percentage
in Western populations (13,14). To accurately interpret the results of
clinical trials, the proportion of patients with EGFR
mutation-positive tumors should be taken into account.
Owing to the growing size of the aging population,
the number of elderly patients with NSCLC is increasing (15). Although several clinical trials have
demonstrated that EGFR-TKIs are safe and effective, the safety and
efficacy of these drugs specifically in elderly patients remains
unclear. Evaluation of these drugs in such patients is necessary
given the complications, organ dysfunction and metabolic changes
that may accompany aging (16,17). A
phase II trial of elderly NSCLC patients receiving erlotinib as
second- or third-line treatment was performed by the Keio Lung
Oncology Group (KLOG001). This trial included EGFR
mutation-positive as well as EGFR mutation-negative tumors
and was registered at the UMIN-CTR (study ID: UMIN000001873).
Patients and methods
Patient eligibility
Patients eligible for this study were aged ≥70 years
and had confirmed stage III or IV or postoperative recurrent NSCLC.
The patients were previously treated with 1 or 2 chemotherapy
regimens that did not include EGFR-TKIs and had at least one
measurable lesion according to the Response Evaluation Criteria in
Solid Tumors (RECIST), version 1.1 (https://www.eortc.be/Recist/documents/RECISTGuidelines.pdf).
Additional inclusion criteria were Eastern Cooperative Oncology
Group (ECOG) performance status (PS) 0–2, life expectancy >3
months and adequate organ function. The main exclusion criteria
were major surgery ≤4 weeks, thoracic radiation therapy ≤2 weeks,
or chemotherapy ≤4 weeks prior to the trial, and the presence of
active double cancer, active infection, interstitial lung disease,
symptomatic brain metastasis, or severe comorbidities. This study
was approved by the Institutional Review Board at Keio University
School of Medicine. All the patients provided written informed
consent.
Study design and treatment
This study was a single-arm multi-center phase II
trial of second- or third-line erlotinib treatment in elderly
patients with NSCLC. The primary endpoint was overall response rate
(ORR) and the secondary endpoints were PFS, OS and toxicity. The
estimated minimum sample size was 38, with an α error of 0.05
(one-sided) and a β error of 0.2. The threshold ORR was 10%
(4,18) and the expected ORR was 25% (19). Assuming that ~5% of patients would
not qualify, 40 patients were enrolled. Patients received erlotinib
at 150 mg/day until the disease progressed, unacceptable toxicity
developed despite dose reduction, or further treatment was refused.
If grade 3 or 4 adverse events (AEs) occurred, treatment was
withheld for up to 14 days and the dose was reduced. Two dose
reductions were permitted per patient (first reduction to 100
mg/day, second reduction to 50 mg/day).
Evaluation
Tumor response was evaluated via computed
tomography, magnetic resonance imaging and bone scintigraphy
according to RECIST every 4 weeks until treatment cessation. To
confirm a complete response (CR) or partial response (PR), a second
assessment was conducted 28 days or more after the initial
assessment. Stable disease (SD) was defined as disease control
(absence of progression) maintained for ≥6 weeks. During this
study, patients underwent physical and blood examinations and chest
X-rays at least once every 2 weeks. AEs were graded according to
the National Cancer Institute Common Terminology Criteria, version
4.0 (https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_Quick
Reference_5×7.pdf). PFS and OS were estimated using the
Kaplan-Meier method.
Results
Patient characteristics
Between April, 2009 and October, 2014, 40 patients
were enrolled in this study. A total of 38 patients were eligible
for treatment, whereas 2 patients were deemed ineligible owing to
priorly receiving 3 chemotherapy regimens, or erlotinib treatment,
respectively. The characteristics of the patients are summarized in
Table I. The median patient age was
76 years (range, 70–83 years). The majority of the patients were
men (66%) and had an ECOG PS of 1 (58%), stage IV disease (66%) and
adenocarcinoma (76%). Biopsy samples from 35 patients were screened
for gain-of-function EGFR mutations, and mutations were identified
in 13 patients (34%): An exon 19 deletion in 5 patients and an
L858R mutation in 8 patients. A total of 35 patients received
platinum-based combination chemotherapy and 3 patients received
monotherapy as first-line treatment. A total of 16 patients
received chemotherapy (including gefitinib treatment in 2 patients)
after this trial. A second biopsy was performed in 5 of the 13
patients with EGFR mutation-positive tumors (38%) and an EGFR T790
M mutation was identified in 3 of those 5 patients (60%).
 | Table I.Patient characteristics (all, <75
years and ≥75 years of age). |
Table I.
Patient characteristics (all, <75
years and ≥75 years of age).
|
| Number of
patients |
|---|
|
|
|
|---|
|
| All | <75 years | ≥75 years |
|---|
| Total enrolled | 38 | 15 | 23 |
| Age (years), median
(range) | 76 (70–83) | 72 (70–74) | 79 (75–83) |
| Gender |
|
|
|
|
Male | 25 | 9 | 16 |
|
Female | 13 | 6 | 7 |
| Smoking status |
|
|
|
|
Never-smoker | 15 | 5 | 10 |
| Current
smoker or ever-smoker | 23 | 10 | 13 |
| Smoking
index, median (range) | 750 (0–2,600) | 750 (0–1,800) | 520 (0–2,600) |
| Performance
status |
|
|
|
| 0 | 13 | 5 | 8 |
| 1 | 22 | 9 | 13 |
| 2 | 3 | 1 | 2 |
| Stage |
|
|
|
|
IIIA | 6 | 3 | 3 |
|
IIIB | 3 | 0 | 3 |
| IV | 25 | 10 | 15 |
|
Postoperative recurrence | 4 | 2 | 2 |
| Histology |
|
|
|
|
Adenocarcinoma | 29 | 13 | 16 |
|
Squamous cell carcinoma | 6 | 2 | 4 |
|
Non-small-cell
carcinoma-NOS | 3 | 0 | 3 |
| EGFR
status |
|
|
|
|
Wild-type | 22 | 10 | 12 |
| Exon 19
deletion | 5 | 2 | 3 |
|
L858R | 8 | 3 | 5 |
|
Unknown/not examined | 3 | 0 | 3 |
| Prior
chemotherapy |
|
|
|
| One
regimen | 27 | 8 | 19 |
| Two
regimens | 11 | 7 | 4 |
| First-line
treatment |
|
|
|
|
Platinum doublet | 31 | 10 | 21 |
|
Platinum doublet +
bevacizumab | 4 | 4 | 0 |
|
Monotherapy | 3 | 1 | 2 |
Response
The efficacy results of this study are summarized in
Table II. Among the 38 patients in
the study, 10 had a PR, 8 had SD and 11 had progressive disease
(PD). The ORR for all patients was 26.3% [95% confidence interval
(CI): 12.1–40.5%] and the disease control rate (DCR), defined as
CR+PR+SD/total number of patients, was 47.4% (95% CI: 31.2–63.6%).
Among the 13 patients with EGFR mutations, 7 had a PR, 2 had SD and
2 had PD. The ORR for patients with EGFR mutations was 53.8% (95%
CI: 26.2–71.4%) and the DCR was 69.2% (95% CI: 43.6–94.8%). Among
the 22 patients with wild-type EGFR, 2 patients had a PR, 5
patients had SD and 9 patients had PD. The ORR for this group was
9.1% (95% CI: 0–21.3%) and the DCR was 31.8% (95% CI:
12.0–51.6%).
| Table II.Response assessment. |
Table II.
Response assessment.
|
| No. of
patients |
|---|
|
|
|
|---|
| Type of
response | Total | EGFR
mutant | EGFR
wild-type | Unknown or not
examined |
|---|
| Complete
response | 0 | 0 | 0 | 0 |
| Partial
response | 10 | 7 | 2 | 1 |
| Stable disease | 8 | 2 | 5 | 1 |
| Progressive
disease | 11 | 2 | 9 | 0 |
| Not evaluable | 9 | 2 | 6 | 1 |
| Total | 38 | 13 | 22 | 3 |
| Response rate
(%) | 26.3 | 53.8 | 9.1 |
|
| Disease control
rate (%) | 47.4 | 69.2 | 31.8 |
|
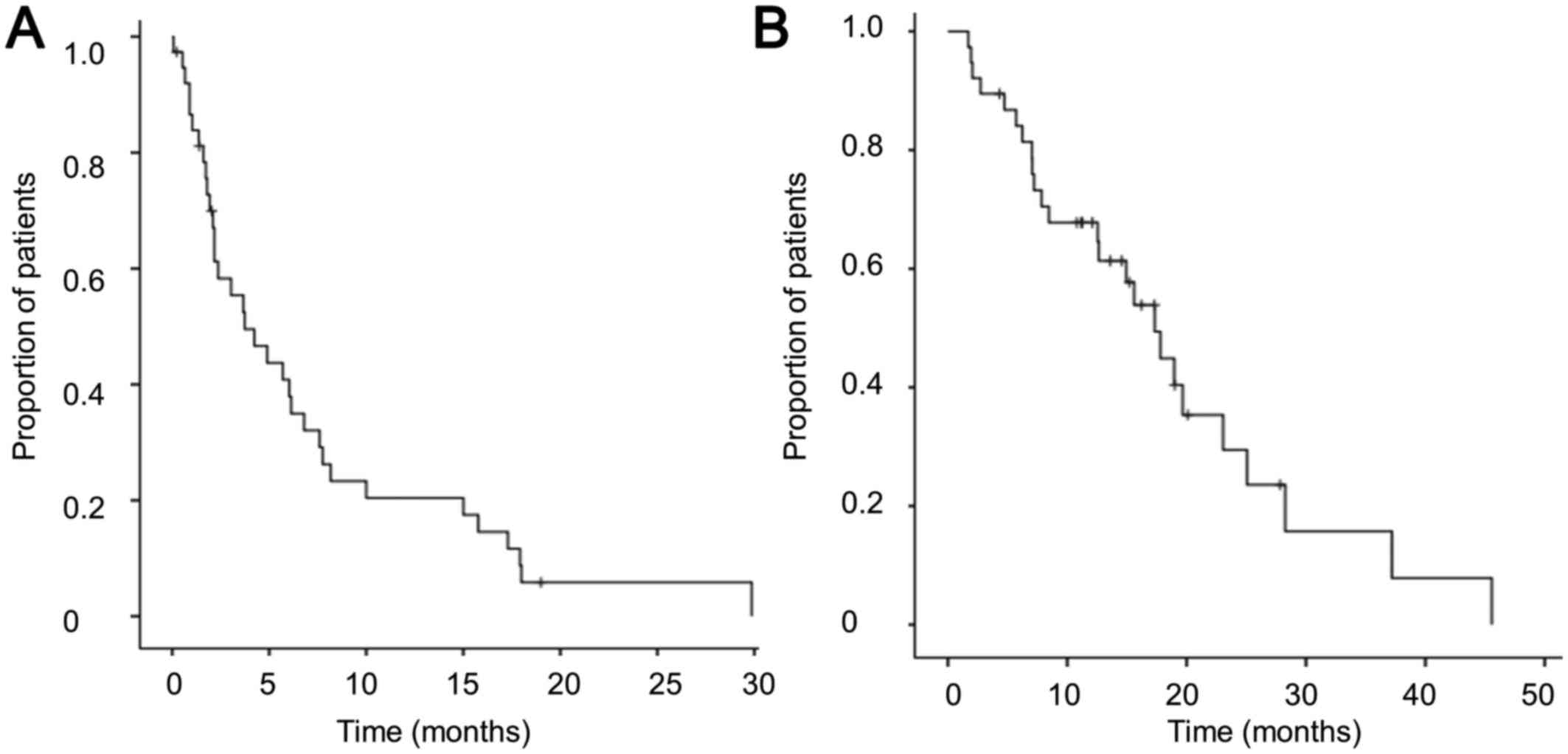
PFS and OS
All 38 patients in the study were included in the
survival analysis, and the minimum follow-up time was 7 months. At
the time of the analysis, 25 patients had succumbed to the disease,
11 patients remained alive, and 2 patients were lost to follow-up.
The median PFS was 3.7 months (95% CI: 1.1–6.4; Fig. 1A) and the median OS was 17.3 months
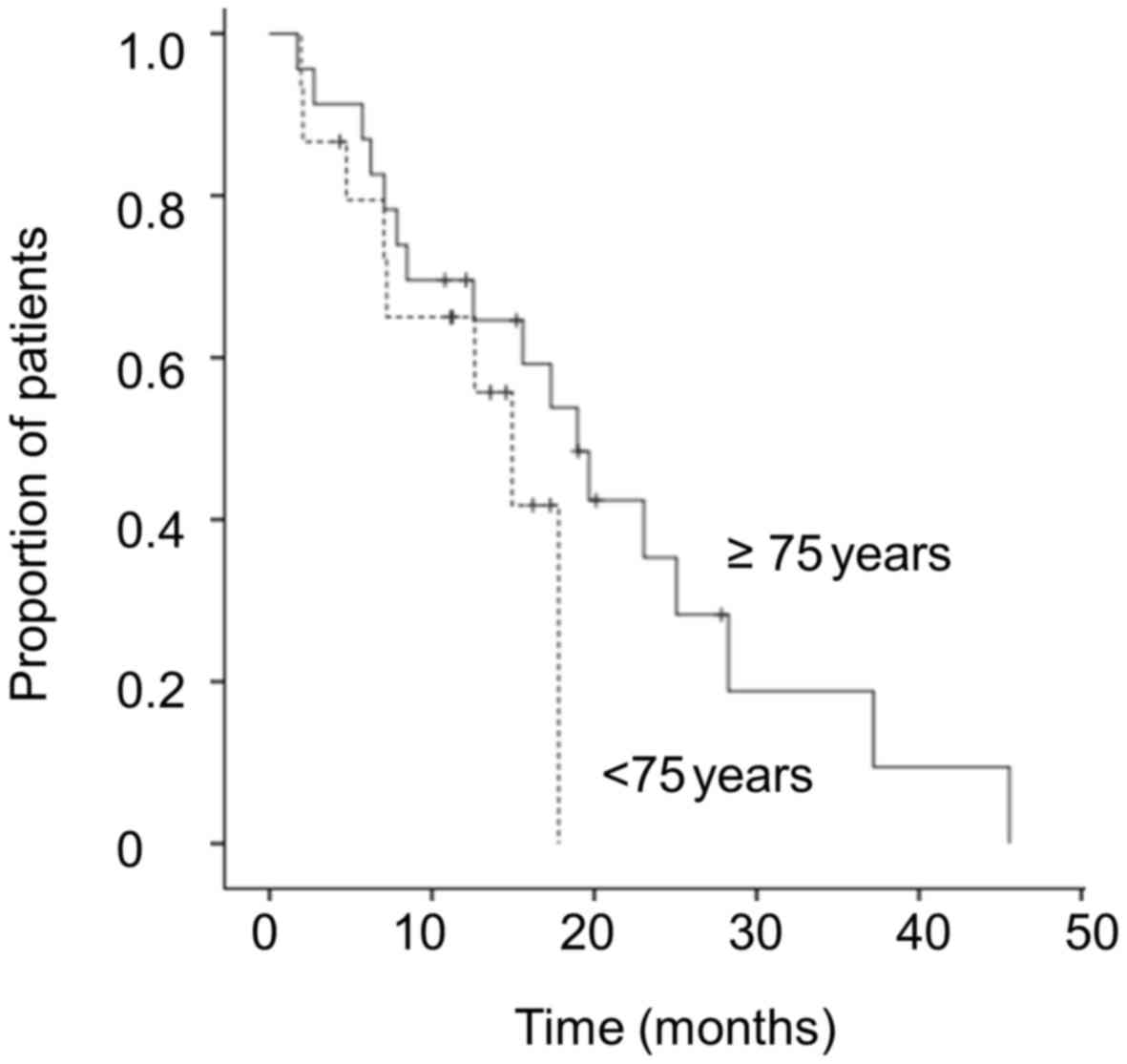
(95% CI: 13.3–21.3; Fig. 1B). The
median OS was 14.9 months (95% CI: 9.7–20.1) in patients aged
<75 years, and 19.0 months (95% CI: 13.7–24.2) in patients aged
≥75 years (log-rank test, P=0.226; Fig.
2).
The median PFS was 7.8 months (95% CI: 5.4–10.1) in
patients with EGFR mutations and 2.1 months (95% CI:
1.6–2.6) in patients without EGFR mutations (log-rank test,
P=0.07). The median OS was 25.1 months (95% CI: 20.1–30.0) and 14.9
months (95% CI: 2.5–27.4), respectively (log-rank test, P<0.05),
and the median post-PD OS was 13.1 months (95% CI: 8.0–18.1) and
10.8 months (95% CI: 0–21.7), respectively (log-rank test,
P=0.261).
Toxicity
Erlotinib safety was assessed in all 38 patients in
this study, and the AEs observed are summarized in Table III. The main AE was skin rash (76%
of the patients). Grade 3 AEs occurred in 11 patients (29%) and
included rash (13%), diarrhea (5%), interstitial pneumonitis (5%),
anorexia (3%) and gastrointestinal (GI) bleeding (3%). Grade 4 or 5
AEs were not observed. A total of 10 patients (26%) discontinued
erlotinib due to the following AEs: Rash (3 patients), elevated
creatinine level and interstitial pneumonitis (2 patients), and
anorexia, diarrhea and GI bleeding (1 patient). The dose of
erlotinib was reduced in 10 patients (26%) due to rash (7
patients), anorexia (2 patients), or diarrhea (1 patient).
| Table III.Adverse events. |
Table III.
Adverse events.
| Toxicities | All-grade (%) | Grade 3 (%) | Grade 4/5 (%) |
|---|
| Rash | 29 (76) | 5 (13) | – |
| Stomatitis | 10 (26) | – | – |
| Diarrhea | 9 (23) | 2 (5) | – |
| Fatigue | 2 (5) | – | – |
| Anorexia | 4 (11) | 1 (3) | – |
| Elevated
creatinine | 4 (11) | – | – |
| Elevated
bilirubin | 3 (8) | – | – |
| Elevated hepatic
transaminases | 2 (5) | – | – |
| Gastrointestinal
bleeding | 2 (5) | 1 (3) | – |
| Pneumonitis | 2 (5) | – | – |
| Interstitial
pneumonitis | 2 (5) | 2 (5) | – |
Discussion
This study investigated the efficacy and safety of
erlotinib as second- or third-line treatment for elderly Japanese
patients with NSCLC. The ORR, which was the primary endpoint of
this study, was 26.3% (95% CI: 12.1–40.5%), which exceeded the
threshold ORR (10%). This percentage (26.3%) was higher compared
with those observed in the BR.21 phase III study of erlotinib as a
second- or third-line treatment for NSCLC patients [8.9% for all
patients (n=427) and 7.6% for elderly patients (aged ≥70 years,
n=112)] (4,20). In a phase II trial of erlotinib as
second- or third-line treatment for elderly (aged ≥65 years)
Italian patients with advanced NSCLC (n=31), the ORR was 16%
(6). We hypothesized that the higher
ORR in our study reflects the inclusion of a higher proportion of
patients with EGFR mutation-positive tumors. All the
patients in our study were Japanese, and tumors with EGFR
mutations are most common among Asian patients (9,13). In
the BR.21 study, Asian patients (n=53) had a higher ORR compared
with patients of other nationalities (n=374) (18.9 vs. 7.5%,
respectively; P=0.02) (4). Other
reported ORRs for erlotinib were similar to ours: 28.3% (95% CI:
17.5–41.4%) in a Japanese phase II study of 60 previously treated
NSCLC patients of various ages (7),
and 28.3% (95% CI: 16.0–43.5) in a Japanese phase II trial of 46
NSCLC patients (21). Both those
studies were conducted on populations not selected for EGFR
mutations. Overall, the elderly patients in our trial and the
Japanese patients of all ages in previous trials had similar
ORRs.
In a retrospective analysis of several Japanese
studies, the efficacy of erlotinib in terms of survival and
tolerability was not lower among elderly compared with younger
patients. In a retrospective subgroup analysis of data collected
from a population-based observational study, the PFS was similar in
elderly (aged ≥75 years, n=74) and younger (aged <75 years,
n=233) patients (median PFS, 62 vs. 46 days; 95% CI: 44–80 vs.
35–53 days, respectively; P=0.2475) receiving erlotinib for the
treatment of NSCLC, regardless of treatment line or EGFR
mutation status (22). In that
study, OS was also similar between elderly (median, 170 days; 95%
CI: 142–239 days) and younger patients (median, 146 days; 95% CI:
114–185 days, P=0.764). There was also no difference in the
incidence of AEs between these groups, and all AEs were manageable.
In a phase IV surveillance study of Japanese patients with
previously treated NSCLC (the EGFR mutation status was not
defined), the median PFS was 65 days for patients aged <75 years
(95% CI: 62–68 days), 74 days for patients aged 75–84 years (95%
CI: 69–82 days), and 72 days for patients aged ≥85 years (95% CI:
56–93 days) (23). Moreover, the
toxicities were similar in all 3 age groups. In our study, the
median OS was 17.3 months and was longer in patients aged ≥75 years
compared with that in patients aged <75 years (19.0 vs. 14.9
months, respectively), although this difference was not
statistically significant (P=0.226). Erlotinib was considered to be
a tolerable and effective treatment for NSCLC patients,
irrespective of their age.
In our study, the OS was significantly longer in
patients with EGFR mutation-positive tumors compared with
that in patients with EGFR mutation-negative tumors. The PFS
and post-PD OS were also longer, although the difference was not
statistically significantly. To date, 2 prospective trials have
enrolled elderly NSCLC patients according to their EGFR
mutation status: One was a phase II study of elderly patients (aged
≥75 years) with EGFR mutation-positive NSCLCs who received
erlotinib as first- or second-line treatment (n=32). In that study,
the ORR was 56.3% (95% CI: 39.4–72.0%) and the median PFS was 15.5
months (95% CI: 11.2-not reached) (24). The second prospective clinical trial
examined elderly patients (aged ≥70 years) with EGFR
mutation-negative tumors in the second- and third-line settings
(25). This small phase II trial
(n=16) reported an ORR of 0% (95% CI: 0–17.1%), a median PFS time
of 1.7 months (95% CI: 1.3–2.2 months) and a median OS time of 7.2
months (95% CI: 5.6–8.7 months); however, it was terminated early
as a phase III trial (26) found
that docetaxel was superior to erlotinib in terms of PFS and ORR in
patients with EGFR mutation-negative tumors. The results of
the two prospective studies cited above (24,25)
suggested that erlotinib should be administered only to patients
with EGFR mutations, even in the second- and third-line
settings. However, in our study, 2 of the 22 patients with
EGFR mutation-negative tumors, and 1 of the 3 patients with
tumors in which the EGFR mutation status was unknown,
responded to erlotinib (ORR=12.0%; DCR=36.0%). These responses
suggest that erlotinib remains a viable second- or third-line
treatment option for elderly patients with NSCLC.
In the BR.21 study, elderly patients (aged ≥70
years) had more severe (grade 3 or 4) AEs compared with younger
patients (aged <70 years) (35 vs. 18%, respectively; P<0.001)
(20). In our study, 11 patients
(29%) had grade 3 AEs, most of which were managed via dose
reductions. Grade 4 or 5 AEs were not observed. Two patients had
grade 3 interstitial pneumonitis and were treated with
corticosteroid therapy. The frequency of AEs in our study was not
higher compared with the previously reported frequencies (28.1–35%)
(20,24). Therefore, erlotinib appears to be
well-tolerated in elderly patients with previously treated
NSCLC.
A limitation of our study was its small sample size,
which precluded us from drawing definitive conclusions from the
results of the main analysis and subset analysis. However, our
study recruited a larger number of patients compared with previous
prospective studies of elderly NSCLC patients in Japan (24,25). The
definition of elderly patients varies across trials. For the
present trial, age ≥70 years was used as an inclusion criterion,
which was standard at that time (20,25). In
accordance with the current standard definition for ‘elderly’ NSCLC
patients (22,23), ≥75 and <75 years of age was used
in our comparison of ‘latter-stage elderly’ and ‘early elderly’
patients, respectively. There were no significant differences in
response, survival, or toxicity between these age groups.
In conclusion, our phase II study demonstrated the
efficacy and safety of erlotinib as second- and third-line
treatment for elderly patients with NSCLC, regardless of whether
they were ‘early elderly’ or ‘latter-stage elderly’ patients.
Acknowledgements
The authors would like to thank the patients, their
families and all the members of the Keio Lung Oncology Group for
their participation and support in this study. TB discloses that
her university received research grants from Chugai
Pharmaceutical.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Molina JR, Yang P, Cassivi SD, Schild SE
and Adjei AA: Non-small cell lung cancer: Epidemiology, risk
factors, treatment, and survivorship. Mayo Clin Proc. 83:584–594.
2008. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH: Eastern
Cooperative Oncology Group: Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shepherd FA, Pereira J Rodrigues, Ciuleanu
T, Ciuleanu T, Tan EH, Hirsh V, Thongprasert S, Campos D,
Maoleekoonpiroj S, Smylie M, et al: Erlotinib in previously treated
non-small-cell lung cancer. N Engl J Med. 353:123–132. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yasuda H, Park E, Yun CH, Sng NJ,
Lucena-Araujo AR, Yeo WL, Huberman MS, Cohen DW, Nakayama S,
Ishioka K, et al: Structural, biochemical and clinical
characterization of epidermal growth factor receptor (EGFR) exon 20
insertion mutations in lung cancer. Sci Transl Med. 5:216ra1772013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rossi D, Dennetta D, Ugolini M, Catalano
V, Alessandroni P, Giordani P, Baldelli AM, Casadei V, Graziano F
and Fedeli S Luzi: Activity and safety of erlotinib as second- and
third-line treatment in elderly patients with advanced non-small
cell lung cancer: A phase II trial. Target Oncol. 5:231–235. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kubota K, Nishiwaki Y, Tamura T, Nakagawa
K, Matsui K, Watanabe K, Hida T, Kawahara M, Katakami N, Takeda K,
et al: Efficacy and safety of erlotinib monotherapy for Japanese
patients with advanced non-small cell lung cancer: A phase II
study. J Thorac Oncol. 3:1439–1445. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Matsuura S, Inui N, Ozawa Y, Nakamura Y,
Toyoshima M, Yasuda K, Yamada T, Shirai T, Suganuma H, Yokomura K,
et al: Phase II study of erlotinib as third-line monotherapy in
patients with advanced non-small-cell lung cancer without epidermal
growth factor receptor mutations. Jpn J Clin Oncol. 41:959–963.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Imielinski M, Berger AH, Hammerman PS,
Hernandez B, Pugh TJ, Hodis E, Cho J, Suh J, Capelletti M,
Sivachenko A, et al: Mapping the hallmarks of lung adenocarcinoma
with massively parallel sequencing. Cell. 150:1107–1120. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pao W and Girard N: New driver mutations
in non-small-cell lung cancer. Lancet Oncol. 12:175–180. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Soda M, Choi YL, Enomoto M, Takada S,
Yamashita Y, Ishikawa S, Fujiwara S, Watanabe H, Kurashina K,
Hatanaka H, et al: Identification of the transforming EML4-ALK
fusion gene in non-small-cell lung cancer. Nature. 448:561–566.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Serizawa M, Koh Y, Kenmotsu H, Isaka M,
Murakami H, Akamatsu H, Mori K, Abe M, Hayashi I, Taira T, et al:
Assessment of mutational profile of Japanese lung adenocarcinoma
patients by multitarget assays: A prospective, single-institute
study. Cancer. 120:1471–1481. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Naoki K, Soejima K, Okamoto H, Hamamoto J,
Hida N, Nakachi I, Yasuda H, Nakayama S, Yoda S, Satomi R, et al:
The PCR-invader method (structure-specific 5′ nuclease-based
method), a sensitive method for detecting EGFR gene mutations in
lung cancer specimens; comparison with direct sequencing. Int J
Clin Oncol. 16:335–344. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Thakkar JP, McCarthy BJ and Villano JL:
Age-specific cancer incidence rates increase through the oldest age
groups. Am J Med Sci. 348:65–70. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ershler WB and Longo DL: Aging and cancer:
Issues of basic and clinical science. J Natl Cancer Inst.
89:1489–1497. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gridelli C and Shepherd FA: Chemotherapy
for elderly patients with non-small cell lung cancer: A review of
the evidence. Chest. 128:947–957. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jackman DM, Yeap BY, Lindeman NI, Fidias
P, Rabin MS, Temel J, Skarin AT, Meyerson M, Holmes AJ, Borras AM,
et al: Phase II clinical trial of chemotherapy-naive patients >
or = 70 years of age treated with erlotinib for advanced
non-small-cell lung cancer. J Clin Oncol. 25:760–766. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Maruyama R, Nishiwaki Y, Tamura T,
Yamamoto N, Tsuboi M, Nakagawa K, Shinkai T, Negoro S, Imamura F,
Eguchi K, et al: Phase III study, V-15–32, of gefitinib versus
docetaxel in previously treated Japanese patients with
non-small-cell lung cancer. J Clin Oncol. 26:4244–4252. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wheatley-Price P, Ding K, Seymour L, Clark
GM and Shepherd FA: Erlotinib for advanced non-small-cell lung
cancer in the elderly: An analysis of the national cancer institute
of canada clinical trials group study BR.21. J Clin Oncol.
26:2350–2357. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Takahashi T, Yamamoto N, Nukiwa T, Mori K,
Tsuboi M, Horai T, Masuda N, Eguchi K, Mitsudomi T, Yokota S, et
al: Phase II study of erlotinib in Japanese patients with advanced
non-small cell lung cancer. Anticancer Res. 30:557–563.
2010.PubMed/NCBI
|
|
22
|
Kurishima K, Satoh H, Kaburagi T,
Nishimura Y, Shinohara Y, Inagaki M, Endo T, Saito T, Hayashihara
K, Hizawa N, et al: Erlotinib for elderly patients with
non-small-cell lung cancer: Subset analysis from a population-based
observational study by the Ibaraki Thoracic Integrative (POSITIVE)
Research Group. Mol Clin Oncol. 1:828–832. 2013.PubMed/NCBI
|
|
23
|
Yoshioka H, Komuta K, Imamura F, Kudoh S,
Seki A and Fukuoka M: Efficacy and safety of erlotinib in elderly
patients in the phase IV POLARSTAR surveillance study of Japanese
patients with non-small-cell lung cancer. Lung Cancer. 86:201–206.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Inoue Y, Inui N, Asada K, Karayama M,
Matsuda H, Yokomura K, Koshimizu N, Imokawa S, Yamada T, Shirai T,
et al: Phase II study of erlotinib in elderly patients with
non-small cell lung cancer harboring epidermal growth factor
receptor mutations. Cancer Chemother Pharmacol. 76:155–161. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Minemura H, Yokouchi H, Azuma K, Hirai K,
Sekine S, Oshima K, Kanazawa K, Tanino Y, Inokoshi Y, Ishii T, et
al: A phase II trial of erlotinib monotherapy for pretreated
elderly patients with advanced EGFR wild-type non-small cell lung
cancer. BMC Res Notes. 8:2202015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kawaguchi T, Ando M, Asami K, Okano Y,
Fukuda M, Nakagawa H, Ibata H, Kozuki T, Endo T, Tamura A, et al:
Randomized phase III trial of erlotinib versus docetaxel as second-
or third-line therapy in patients with advanced non-small-cell lung
cancer: Docetaxel and Erlotinib Lung Cancer Trial (DELTA). J Clin
Oncol. 32:1902–1908. 2014. View Article : Google Scholar : PubMed/NCBI
|