Introduction
Salivary duct carcinoma (SDC) is a rare and highly
aggressive type of cancer, accounting for 1–3% of all malignant
salivary tumors (1–4). These lesions typically arise in the
parotid gland (75%), with rare cases (10%) occurring in the
submandibular gland (2). According
to the recently revised 2005 World Health Organization
classification, SDCs are classified as sarcomatoid, mucin-rich, or
invasive micropapillary variants (5). SDC presents as a rapidly growing mass
with the potential for local recurrence and cervical and/or distant
metastases, and is associated with a high mortality rate. Although
surgery, including extended radical resection and ipsilateral neck
dissection, followed by postoperative radiation is the standard
treatment for SDC (2,6,7), there
is currently no standard systemic treatment.
The overall 5-year survival rate associated with SDC
is low (42–55%) (2,7–12).
Recent studies have tested molecularly targeted therapies as novel
treatment strategies for SDC. This type of cancer resembles
intraductal and infiltrating mammary duct carcinomas with a variety
of histoarchitectural and cytological patterns. Approximately
61–100% of the cases are reported to be human epidermal growth
factor receptor 2 (HER2)-positive (13,14), and
a correlation has been identified between HER2 expression and
prognosis (13–16). Additionally, 50–70% of SDCs express
epidermal growth factor receptor (EGFR; HER1) (17–19), and
anti-EGFR-targeted therapies, such as cetuximab, are expected to be
useful as novel SDC treatments. Locati et al demonstrated
the efficacy of cetuximab in 24 of 30 cases of recurrent and/or
metastatic salivary gland carcinoma (20). However, the role of molecularly
targeted therapies in the treatment of salivary gland carcinomas
has not been well defined, and combination therapy comprising
cisplatin/5-fluorouracil (5-FU) plus cetuximab has not been tested
in SDC. We herein present the first report of clinical activity
from systemic treatment comprising cisplatin/5-FU plus cetuximab in
a patient with multiple lung metastases from SDC.
Case report
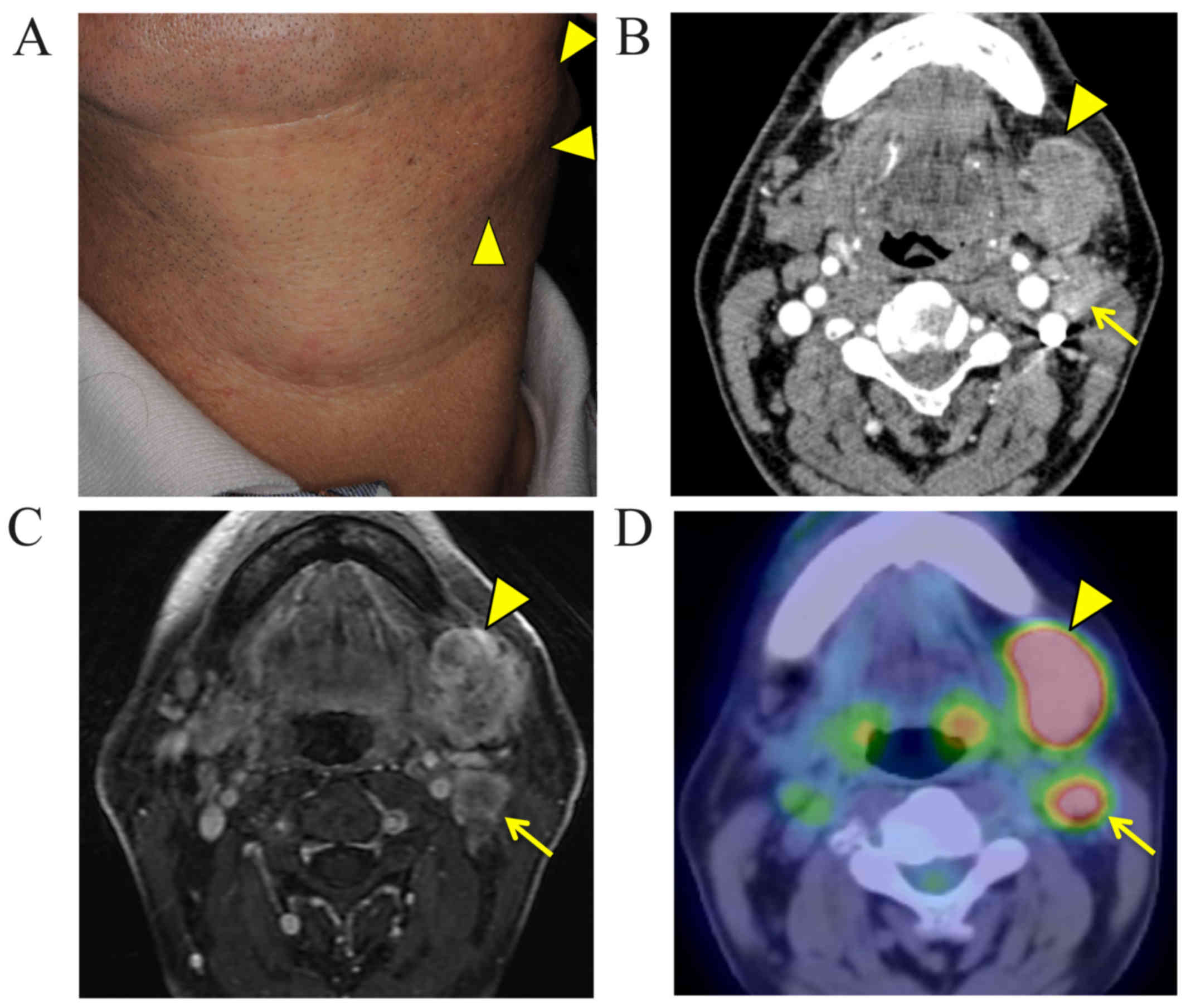
In August, 2014, a 56-year-old man was referred to
the Kumamoto University Hospital due to a gradually increasing
swelling in the submandibular region over a 2-month period
(Fig. 1A), without pain or
paresthesia. The patient's medical history included hypertension
and chronic obstructive pulmonary disease. There was no noteworthy
familial history of cancer. An extraoral examination revealed a
firm lump in the submandibular region, without adhesion to the
overlying skin; no neurological disturbance of the lingual or
facial nerves was observed. Intraorally, there were no significant
findings. Computed tomography (CT) (Fig.
1B) and magnetic resonance imaging (Fig. 1C) revealed a 3.0×3.0-cm heterogeneous
mass in the left submandibular region and several necrotic and
enlarged lymph nodes in the ipsilateral neck. Positron emission
tomography-CT revealed abnormal enhancing lesions with increased
fluorodeoxyglucose uptake in the left submandibular gland region
and cervical lymph nodes, but no distant metastases (Fig. 1D). Ultrasonography indicated enlarged
or necrotic lymph nodes in the submandibular and superior internal
jugular region. Therefore, this lesion was classified as cT4N2bM0
according to the World Health Organization International
Classification of Tumors (21).
An incisional biopsy was performed under local
anesthesia, and the histopathological examination revealed SDC.
Thereafter, the submandibular tumor was removed with 1-cm safety
margins, followed by radical neck dissection and marginal
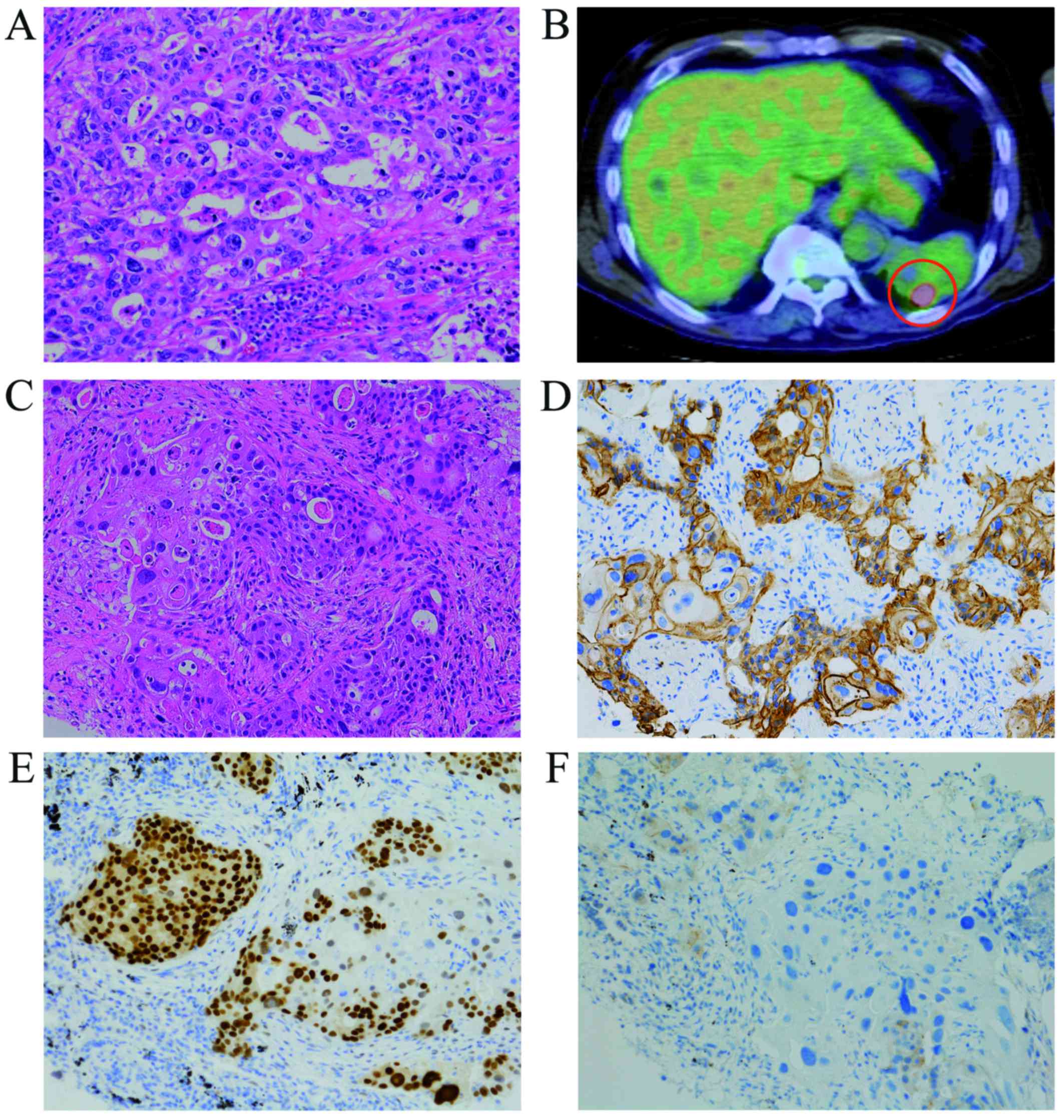
mandibulectomy. The histopathological examination revealed that all
resection margins were tumor-free. The excised lesion primarily
comprised cells with large atypical nuclei and prominent nucleoli,
and atypical cells with moderately abundant eosinophilic cytoplasm.
The tumor contained frequent ductal lesions and central
comedonecrosis associated with cribriform and epithelial
differentiation. Despite vascular invasion, no nerve invasion was
detected. The tumor cells were immunohistochemically positive for
EGFR and androgen receptor (AR), but negative for HER2. The patient
was ultimately diagnosed with SDC (Fig.
2A).
One month after radical surgery, a CT scan revealed
metastasis in the lower lobe of the left lung (Fig. 2B), and CT-guided transthoracic
fine-needle aspiration revealed a single metastasis. Lung
metastasectomy was performed via video-assisted thoracic surgery
(VATS). The lung tumor was histologically diagnosed as metastasis
from SDC (Fig. 2C), and the tumor
was immunohistochemically positive for EGFR and AR, but negative
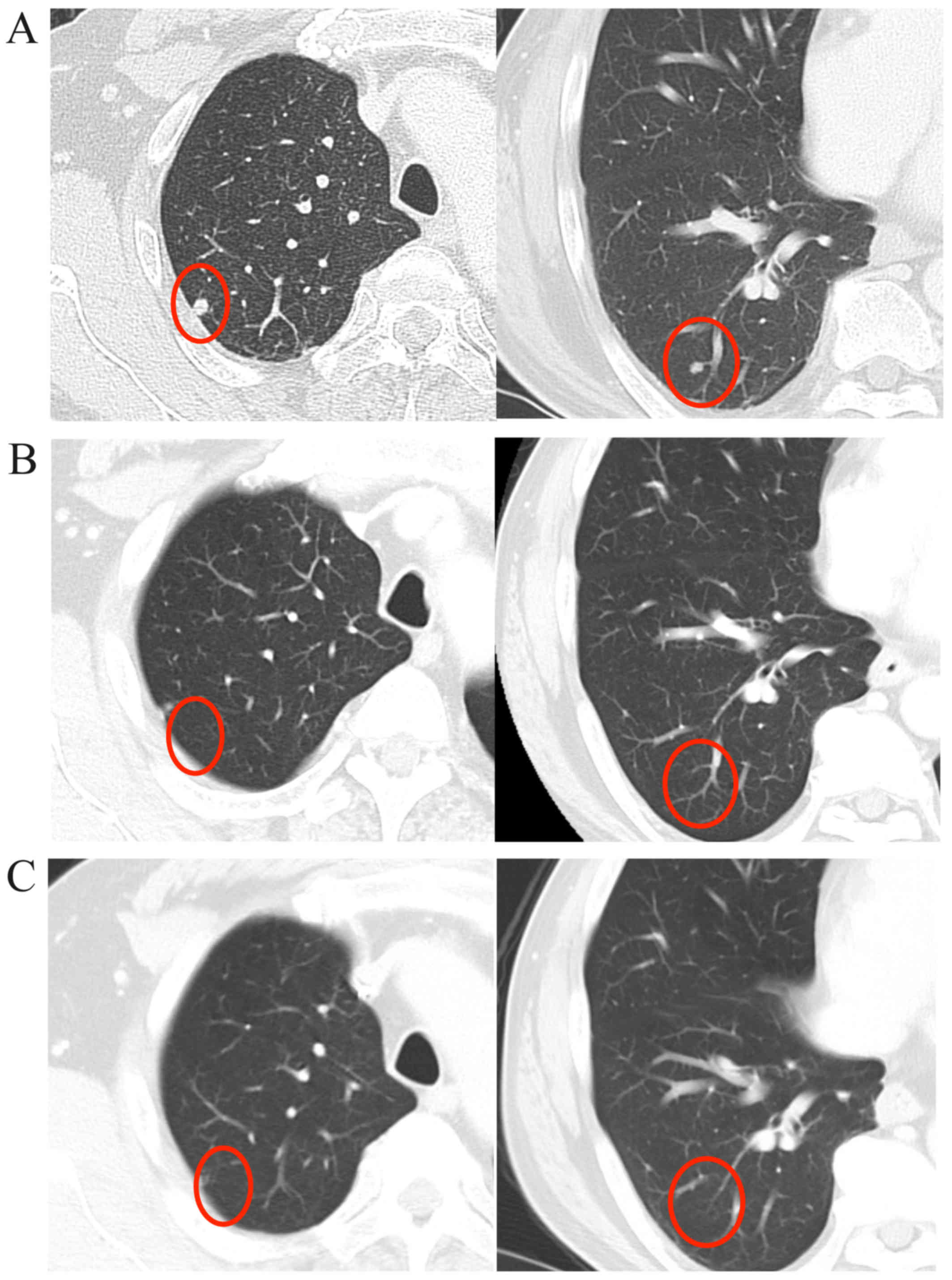
for HER2 (Fig. 2D-F). One month
later, however, another CT scan revealed multiple metastases in the
right lung (Fig. 3A), and systemic
treatment similar to the regimen used in the EXTREME trial was
initiated (22,23). The regimen comprised cetuximab every
7 days (120-min intravenous infusion of a 400-mg/m2
initial dose, followed by weekly 60-min infusions of 250
mg/m2) together with 3-week cycles of cisplatin (240-min
intravenous infusion of 80 mg/m2 on day 1) and 5-FU
chemotherapy (24-h continuous infusion of 800 mg/m2 per
day on days 1–5) (22,23). This treatment was previously found to
be well-tolerated, with mild adverse events, including grade 1 skin
rash, dermatitis acneiform and paronychia, and grade 2
hypomagnesemia. All lung metastatic lesions had regressed after two
cycles (Fig. 3B), and a complete
response (CR) was confirmed after six cycles (Fig. 3C). Although the patient continued to
receive cetuximab monotherapy, metastases had developed in both
lungs 3 months after the completion of systemic combination
therapy. The right lung metastases were removed via VATS, whereas
radiofrequency ablation treatment was planned for the left lung due
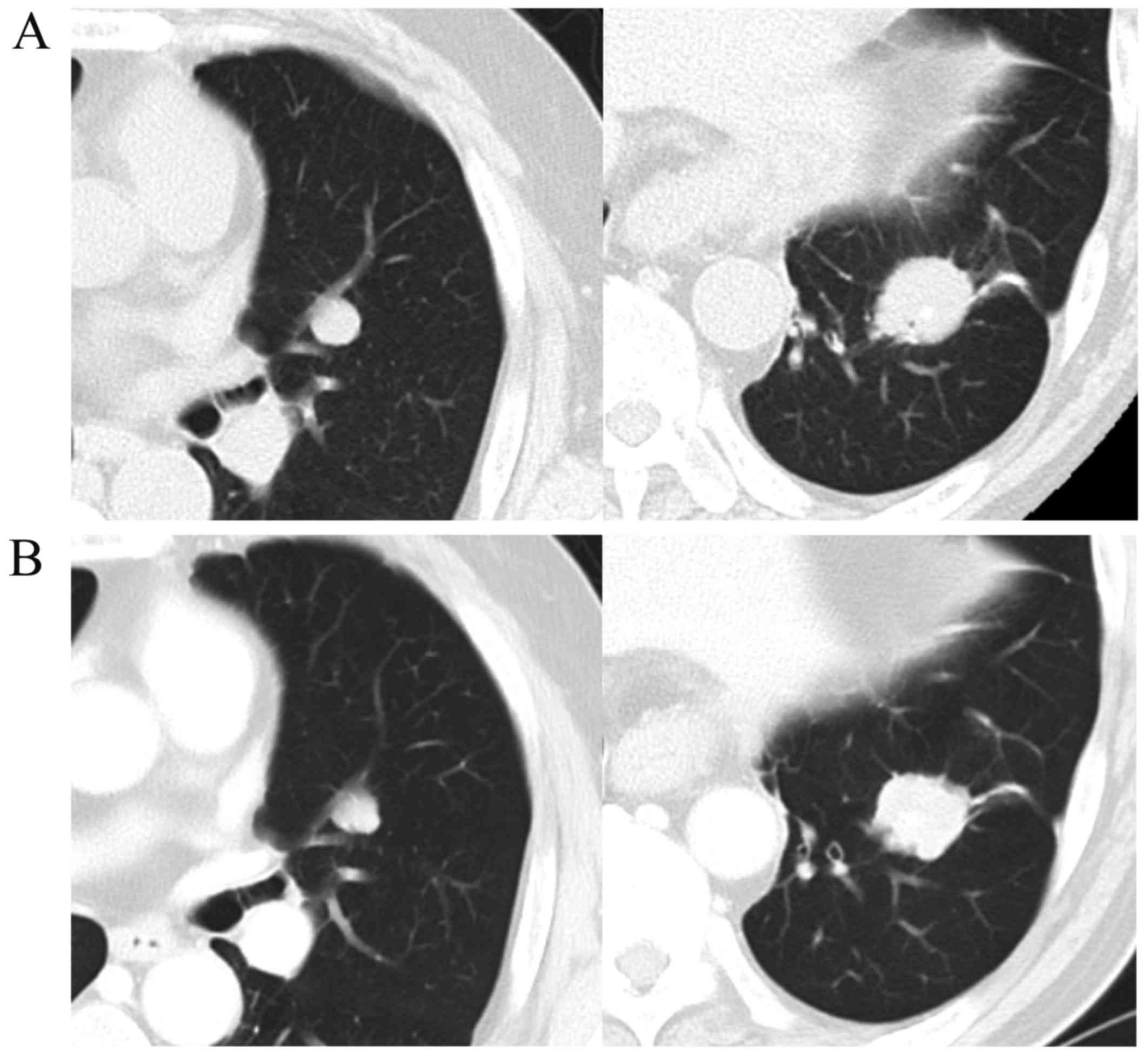
to the extensive multiple metastases. However, as new, rapidly
growing metastatic masses appeared (Fig.
4A), the therapeutic strategy was changed to palliative
chemotherapy and follow-up. We initiated treatment with 120-mg/day
tegafur-gimeracil-oteracil potassium (S-1) daily for 2 weeks,
followed by a 1-week rest (24),
with concurrent continued weekly cetuximab. After 5 months of
treatment, CT scans revealed stable disease (SD) regarding the left
lung metastases (Fig. 4B). The
patient has been continuing these systemic treatments for 7 months,
without any compromise to his quality of life.
The treatment protocol was approved by the Kumamoto
University Hospital. Consent to participate in this study was
obtained from the patient's family. This investigation was
conducted according to the guidelines of the Helsinki Declaration.
Written informed consent was obtained from the patient for the
publication of this case report and associated images.
Discussion
SDC was first described in 1968 by Kleinsasser et
al (25). This type of cancer is
considered to be among the most aggressive salivary gland
carcinomas due to the high frequency of local recurrence, as well
as associated cervical lymph node and distant metastases (2,7–12). The most common treatment for SDC is
surgery, particularly extended radical resection and ipsilateral
neck dissection, with postoperative radiotherapy (2,6,7). Between 2005 and 2015, SDC patients were
frequently diagnosed at an advanced stage, as in 55–82% of the
cases the disease had already spread to the cervical lymph nodes on
first diagnosis. Furthermore, local and regional recurrence and
distant metastasis following surgery and postoperative radiotherapy
were observed in 11–48, 8–26 and 24–63% of the patients,
respectively, with a 5-year survival rate of 42–55% (2,7–12).
Although curative postoperative radiotherapy (60–70
Gy) is administered after extended surgery in the majority of the
cases, only a few studies have compared surgical resection alone to
surgical resection with postoperative radiotherapy. In a previous
study involving postoperative radiotherapy, Shinoto et al
reported that the local recurrence, regional recurrence, distant
metastasis and 5-year survival rates were 28, 16, 48 and 47%,
respectively (7). Despite aggressive
treatment with postoperative radiotherapy, treatment efficacy has
been insufficient and controversial. In fact, most previous cases
involving treatment of local and regional recurrences had poor
prognoses. Meredith et al reported distant metastases in 12
of 32 (37.5%) SDC patients with local and regional recurrence. The
majority of those patients received palliative therapy or
supportive care, although some underwent salvage surgery and
additional radiation therapy, alone or combined with chemotherapy.
However, all the patients have since succumbed to the disease
(9). The most frequent cause of
death is distant metastasis, and 65% of patients with distant
metastases succumb to the disease 5 months-10 years later (5,26,27).
Although local and regional recurrence are correlated with
prognosis, targeting the metastatic potential of SDC is crucial for
disease control (28). Sites of
distant metastasis include the lungs, bones, liver, skin and brain,
although in most cases metastases develop in the lungs and bones
(9,28). Systemic chemotherapy should therefore
be considered for the treatment of distant metastasis, although
there have been no convincing reports regarding chemotherapy for
SDC. Chemotherapy comprising platinum-, anthracycline-, or
taxane-based regimens has been used, with response rates of 15–50%
(19,29), but no reliable data on the specific
chemoresponsiveness of SDC have been published to date (30). Additionally, Meredith et al
reported that SDC was not sensitive to chemotherapy (9). Therefore, treatment efficacy remains
unclear, and there is currently no consensus regarding chemotherapy
for SDC (19,31,32).
Only a limited number of studies have reported the
outcome of lung metastasectomy to remove metastases from head and
neck salivary gland carcinoma, particularly from adenoid cystic
carcinoma (ACC), whereas none have specifically addressed SDC.
Bobbio et al reported that, among 50 patients with ACC lung
metastases, the 10-year survival rates did not differ significantly
between patients who did and those who did not undergo complete
lung metastasectomy (33). Liu et
al reported that, although patients with ACC had a 5-year
survival rate of 84% following metastasectomy, there were no
disease-free survivors at 14 years (34), indicating a lack of effective
treatments for lung metastasis. ACC spreads in a manner similar to
SDC, although metastases of the former tend to develop gradually.
By contrast, SDC metastases occur earlier and develop more rapidly,
suggesting that the efficacy of lung metastasectomy for SDC may be
insufficient when compared to its efficacy for ACC. In the case
presented herein, SDC developed in the submandibular gland and the
patient had lymph node metastases at initial diagnosis, as
described previously (2,7–12).
Radical tumor resection with ipsilateral neck dissection were first
performed, followed by lung metastasectomy via VATS for left lower
lung metastasis and adjuvant chemotherapy. One month after
metastasectomy, effective treatments for new multiple right lung
metastases were sought, despite the lack of local or regional
recurrence.
Recent studies of novel treatment strategies for SDC
investigated the systemic use of molecularly targeted therapies
(14–16,35–37).
Trastuzumab, which targets HER2, effectively prevents the
recurrence of metastatic HER2-positive breast cancer. SDC
histologically resembles intraductal and infiltrating mammary duct
carcinoma, and previous studies reported the therapeutic efficacy
of adjuvant or palliative trastuzumab, carboplatin and paclitaxel
for SDC, which frequently overexpresses HER2 (14–16,35–37).
Limaye et al described 8 patients with HER2-positive SDC who
were treated with concurrent radiation and chemotherapy consisting
of weekly paclitaxel, carboplatin and trastuzumab after surgical
resection, followed by adjuvant trastuzumab monotherapy (16). Of the patients who received adjuvant
therapy, 38% experienced recurrence, but all patients with
metastatic disease responded to treatment with trastuzumab. One
patient achieved a CR and currently has no evidence of disease
(16). Furthermore, trastuzumab was
found to be superior to conventional chemotherapy for the treatment
of distant metastasis, and palliative and adjuvant
trastuzumab-based therapy should be considered for all patients
with HER2-positive SDC (14–16,35–37).
Despite several reports on the usefulness of trastuzumab, these
have mostly been retrospective analyses. Prospective and larger
randomized studies with longer follow-up periods are required to
confirm the effectiveness of trastuzumab.
Cetuximab, an anti-EGFR monoclonal antibody, is also
expected to exhibit therapeutic efficacy. Recently, EGFR
inhibitors, such as cetuximab, have increasingly been used to treat
salivary gland tumors, which are often resistant to chemotherapy or
radiotherapy. Cetuximab-based regimens were used in a phase II
study including 30 patients with recurrent or metastatic salivary
gland carcinomas, and >50% of the treated patients achieved SD
(20). Thus, cetuximab is being
increasingly recognized as a more effective alternative to
conventional chemotherapy. Fan et al reported EGFR
expression in ~92% of SDC cases (17), and a marginally significant
correlation of EGFR overexpression in SDC with local recurrence was
observed (19). Furthermore, EGFR
overexpression in salivary gland tumors was found to be correlated
with poor prognosis and appeared to play an important role in
tumorigenesis (38,39). Although anti-EGFR targeted therapies
are expected to provide novel treatment options, no previous
reports have detailed their effectiveness for SDC.
In the present case, radical tumor resection was
performed, including marginal mandibulectomy and ipsilateral neck
dissection. The pathological examination revealed that all
resection margins were tumor-free, and distant metastasis was not
detected at the time. Previous reports led us to consider
postoperative adjuvant therapy to prevent local and regional
recurrence and distant metastasis (2,7–12). Therefore, a systemic molecularly
targeted therapy selected for the distant metastasis, along with
close follow-up to monitor local and regional recurrence.
Unfortunately, 1 month after surgery a left lower lung metastasis
was detected, which was treated by VATS-assisted lung
metastasectomy. The immunohistochemical analysis revealed that most
tumor cells from the primary lymph node metastases and the lung
metastasis were immunohistochemically positive for EGFR. Therefore,
the planned systemic treatment included cisplatin/5-FU chemotherapy
plus cetuximab, as reported in the EXTREME trial (22).
Shortly thereafter, new multiple metastases appeared
in the lower lobe of the right lung, and systemic treatment for
bilateral lung metastases was promptly initiated. After six cycles
of treatment, which was well-tolerated, the patient achieved a CR.
These dramatic effects on tumor regression, together with the lack
of severe adverse events, suggest that this systemic treatment may
lead to improved outcomes for patients with SDC. Although our
patient continued to receive cetuximab monotherapy in accordance
with the EXTREME trial protocol, CT scans revealed right lower,
left lower and upper lung metastases. This SDC responded to the
combination chemotherapy plus cetuximab, but it did not respond to
weekly cetuximab maintenance monotherapy. Although a cisplatin/5-FU
regimen would not be expected to exert antitumor effects on SDC,
tumor regression was achieved by combining this regimen with
cetuximab. Although the underlying mechanism of action has not been
fully elucidated, several factors may have contributed to the
three-drug combination regimen-mediated control of SDC in our
case.
Of note, late-onset cisplatin-induced peripheral
neuropathy continuing this three-drug combination regimen
difficult. After considering the combination therapy with
paclitaxel and cetuximab, cisplatin was replaced with S-1, which
may be used to provide long-term and low-impact treatment and
maintain the patient's quality of life, according to his wishes.
Therefore, S-1 and weekly cetuximab treatment was initiated, and
the multiple lung metastases have subsequently been maintained as
SD. The effects of this regimen may be similar to those of the
initial three-drug combination regimen. Although the results
indicate that cisplatin/5-FU chemotherapy plus cetuximab may be an
effective treatment for SDC, these results should be interpreted
with caution, since this is a case report of a single patient.
We herein presented the first case report of
cetuximab-containing chemotherapy for SDC. Even after treatment
with extended surgery followed by radiotherapy, ~50% of patients
with SDC experience systemic failure, resulting in a poor
prognosis. Although the main limitation of our study is that in
involves a single case, our findings demonstrated the efficacy of
cetuximab-containing chemotherapy as postoperative adjuvant therapy
for distant metastases from SDC. Prospective and larger randomized
studies with longer follow-up periods are required to confirm our
findings.
Acknowledgements
This study was supported by the Japan Society for
the Promotion of Science KAKENHI, Grant Number 90732735. The
authors would like to thank Editage (www.editage.jp) for English language editing.
Glossary
Abbreviations
Abbreviations:
|
ACC
|
adenoid cystic carcinoma
|
|
AR
|
androgen receptor
|
|
CR
|
complete response
|
|
CT
|
computed tomography
|
|
EGFR
|
epidermal growth factor receptor
|
|
FU
|
5-fluorouracil
|
|
HER2
|
human epidermal growth factor receptor
2
|
|
S-1
|
tegafur-gimeracil-oteracil
potassium
|
|
SD
|
stable disease
|
|
SDC
|
salivary duct carcinoma
|
|
VATS
|
video-assisted thoracic surgery
|
References
|
1
|
Gal R, Strauss M, Zohar Y and Kessler E:
Salivary duct carcinoma of the parotid gland. Cytologic and
histopathologic study. Acta Cytol. 29:454–456. 1985.PubMed/NCBI
|
|
2
|
Jaehne M, Roeser K, Jaekel T, Schepers JD,
Albert N and Löning T: Clinical and immunohistologic typing of
salivary duct carcinoma: A report of 50 cases. Cancer.
103:2526–2533. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Seifert G, Batsakis J, Brocheriou C,
Cardesa A, Dardick I and Ellis G: World Health Organization.
Histological typing of salivary gland tumors. 2nd. New York:
Springer; 1991, View Article : Google Scholar
|
|
4
|
Seifert G and Caselitz J: Epithelial
salivary gland tumors: Tumor markersFenoglio-Preiser CM, Wolff M
and Rilke F: Progress in surgical pathology. New York: Field &
Wood; pp. 157–187. 1989, View Article : Google Scholar
|
|
5
|
Barnes L, Eveson J, Reichart P and
Sidranksky D: World Health Organization Classification of
TumoursPathology and genetics of head and neck tumours. Lyon: IARC
Press; pp. 236–237. 2005
|
|
6
|
McHugh JB, Visscher DW and Barnes EL:
Update on selected salivary gland neoplasms. Arch Pathol Lab Med.
133:1763–1774. 2009.PubMed/NCBI
|
|
7
|
Shinoto M, Shioyama Y, Nakamura K,
Nakashima T, Kunitake N, Higaki Y, Sasaki T, Ohga S, Yoshitake T,
Ohnishi K, et al: Postoperative radiotherapy in patients with
salivary duct carcinoma: Clinical outcomes and prognostic factors.
J Radiat Res. 54:925–930. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kim JY, Lee S, Cho KJ, Kim SY, Nam SY,
Choi SH, Roh JL, Choi EK, Kim JH, Song SY, et al: Treatment results
of post-operative radiotherapy in patients with salivary duct
carcinoma of the major salivary glands. Br J Radiol. 85:e947–e952.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Johnston ML, Huang SH, Waldron JN, Atenafu
EG, Chan K, Cummings BJ, Gilbert RW, Goldstein D, Gullane PJ, Irish
JC, et al: Salivary duct carcinoma: Treatment, outcomes, and
patterns of failure. Head Neck. 8 Suppl 1:E820–E826. 2016.
View Article : Google Scholar
|
|
10
|
Salovaara E, Hakala O, Bäck L, Koivunen P,
Saarilahti K, Passador-Santos F, Leivo I and Mäkitie AA: Management
and outcome of salivary duct carcinoma in major salivary glands.
Eur Arch Otorhinolaryngol. 270:281–285. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Weon YC, Park SW, Kim HJ, Jeong HS, Ko YH,
Park IS, Kim ST, Baek CH and Son YI: Salivary duct carcinomas:
Clinical and CT and MR imaging features in 20 patients.
Neuroradiology. 54:631–640. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Roh JL, Cho KJ, Kwon GY, Choi SH, Nam SY
and Kim SY: Prognostic values of pathologic findings and hypoxia
markers in 21 patients with salivary duct carcinoma. J Surg Oncol.
97:596–600. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Falchook GS, Lippman SM, Bastida CC and
Kurzrock R: Human epidermal receptor 2-amplified salivary duct
carcinoma: Regression with dual human epidermal receptor 2
inhibition and anti-vascular endothelial growth factor combination
treatment. Head Neck. 36:E25–E27. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xie S, Yang H, Bredell M, Shen S, Yang H,
Jin L and Zhang S: Salivary duct carcinoma of the parotid gland: A
case report and review of the literature. Oncol Lett. 9:371–374.
2015.PubMed/NCBI
|
|
15
|
Lee JS, Kwon OJ, Park JJ and Seo JH:
Salivary duct carcinoma of the parotid gland: Is adjuvant
HER-2-targeted therapy required? J Oral Maxillofac Surg.
72:1023–1031. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Limaye SA, Posner MR, Krane JF, Fonfria M,
Lorch JH, Dillon DA, Shreenivas AV, Tishler RB and Haddad RI:
Trastuzumab for the treatment of salivary duct carcinoma.
Oncologist. 18:294–300. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fan CY, Melhem MF, Hosal AS, Grandis JR
and Barnes EL: Expression of androgen receptor, epidermal growth
factor receptor, and transforming growth factor alpha in salivary
duct carcinoma. Arch Otolaryngol Head Neck Surg. 127:1075–1079.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Williams MD, Roberts D, Blumenschein GR
Jr, Temam S, Kies MS, Rosenthal DI, Weber RS and El-Naggar AK:
Differential expression of hormonal and growth factor receptors in
salivary duct carcinomas: Biologic significance and potential role
in therapeutic stratification of patients. Am J Surg Path.
31:1645–1652. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Williams MD, Roberts DB, Kies MS, Mao L,
Weber RS and El-Naggar AK: Genetic and expression analysis of HER-2
and EGFR genes in salivary duct carcinoma: Empirical and
therapeutic significance. Clin Cancer Res. 16:2266–2274. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Locati LD, Bossi P, Perrone F, Potepan P,
Crippa F, Mariani L, Casieri P, Orsenigo M, Losa M, Bergamini C, et
al: Cetuximab in recurrent and/or metastatic salivary gland
carcinomas: A phase II study. Oral Oncol. 45:574–578. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Seifert G, Brocheriou C, Cardesa A and
Eveson JW: WHO International histological classification of
tumours. Tentative histological classification of salivary gland
tumours. Pathol Res Pract. 186:555–581. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vermorken JB, Mesia R, Rivera F, Remenar
E, Kawecki A, Rottey S, Rottey S, Erfan J, Zabolotnyy D, Kienzer
HR, et al: Platinum-based chemotherapy plus cetuximab in head and
neck cancer. New Engl J Med. 359:1116–1127. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Guo Y, Shi M, Yang A, Feng J, Zhu X, Choi
YJ, Hu G, Pan J, Hu C, Luo R, et al: Platinum-based chemotherapy
plus cetuximab first-line for Asian patients with recurrent and/or
metastatic squamous cell carcinoma of the head and neck: Results of
an open-label, single-arm, multicenter trial. Head Neck.
37:1081–1087. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tsukahara K, Kubota A, Hasegawa Y,
Takemura H, Terada T, Taguchi T, Nagahara K, Nakatani H, Yoshino K,
Higaki Y, et al: Randomized phase III trial of adjuvant
chemotherapy with S-1 after curative treatment in patients with
squamous-cell carcinoma of the head and neck (ACTS-HNC). PLoS One.
10:e01169652015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kleinsasser O, Klein HJ and Hubner G:
Salivary duct carcinoma. A group of salivary gland tumors analogous
to mammary duct carcinoma. Arch Klin Exp Ohren Nasen
Kehlkopfheilkd. 192:100–105. 1968.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Adelstein DJ, Koyfman SA, El-Naggar AK and
Hanna EY: Biology and management of salivary gland cancers. Semin
Radiat Oncol. 22:245–253. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Barnes L, Rao U, Krause J, Contis L,
Schwartz A and Scalamogna P: Salivary duct carcinoma. Part I. A
clinicopathologic evaluation and DNA image analysis of 13 cases
with review of the literature. Oral Surg Oral Med Oral Pathol.
78:64–73. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Guzzo M, Di Palma S, Grandi C and Molinari
R: Salivary duct carcinoma: Clinical characteristics and treatment
strategies. Head Neck. 19:126–133. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Airoldi M, Fornari G, Pedani F,
Marchionatti S, Gabriele P, Succo G and Bumma C: Paclitaxel and
carboplatin for recurrent salivary gland malignancies. Anticancer
Res. 20:3781–3783. 2000.PubMed/NCBI
|
|
30
|
Surakanti SG and Agulnik M: Salivary gland
malignancies: The role for chemotherapy and molecular targeted
agents. Semin Oncol. 35:309–319. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dimery IW, Legha SS, Shirinian M and Hong
WK: Fluorouracil, doxorubicin, cyclophosphamide, and cisplatin
combination chemotherapy in advanced or recurrent salivary gland
carcinoma. J Clin Oncol. 8:1056–1062. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lagha A, Chraiet N, Ayadi M, Krimi S,
Allani B, Rifi H, Raies H and Mezlini A: Systemic therapy in the
management of metastatic or advanced salivary gland cancers. Oral
Oncol. 48:948–957. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bobbio A, Copelli C, Ampollini L, Bianchi
B, Carbognani P, Bettati S, Sesenna E and Rusca M: Lung metastasis
resection of adenoid cystic carcinoma of salivary glands. Eur J
Cardiothorac Surg. 33:790–793. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Liu D, Labow DM, Dang N, Martini N, Bains
M, Burt M, Downey R Jr, Rusch V, Shah J and Ginsberg RJ: Pulmonary
metastasectomy for head and neck cancers. Ann Surg Oncol.
6:572–578. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kaidar-Person O, Billan S and Kuten A:
Targeted therapy with trastuzumab for advanced salivary ductal
carcinoma: Case report and literature review. Med Oncol.
29:704–706. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Nabili V, Tan JW, Bhuta S, Sercarz JA and
Head CS: Salivary duct carcinoma: A clinical and histologic review
with implications for trastuzumab therapy. Head Neck. 29:907–912.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Prat A, Parera M, Reyes V, Peralta S,
Cedrés S, Andreu J, Huguet P and del Campo JM: Successful treatment
of pulmonary metastatic salivary ductal carcinoma with
trastuzumab-based therapy. Head Neck. 30:680–683. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ettl T, Stiegler C, Zeitler K, Agaimy A,
Zenk J, Reichert TE, Gosau M, Kühnel T, Brockhoff G and Schwarz S:
EGFR, HER2, survivin, and loss of pSTAT3 characterize high-grade
malignancy in salivary gland cancer with impact on prognosis. Hum
Pathol. 43:921–931. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ito FA, Ito K, Coletta RD, Graner E, de
Almeida OP and Lopes MA: Salivary gland tumors: Immunohistochemical
study of EGF EGFR, ErbB-2, FAS and Ki-67. Anal Quant Cytol Histol.
31:280–287. 2009.PubMed/NCBI
|