Introduction
Osseous and soft tissue sarcomas are rare conditions
that may easily be misdiagnosed. Apart from pathological
observations of biopsies, imaging studies such as X-rays,
whole-body bone scan, computed tomography (CT) and magnetic
resonance imaging (MRI) are often used for diagnostic purposes in
cases with osseous and soft tissue sarcomas. Positron emission
tomography (PET) is an imaging method that semiquantitatively
measures the metabolic rate of tissues by measuring the glucose
intake level of cells in vivo. As malignant tumors normally
have a higher metabolic rate compared with benign lesions and
normal tissues, PET may theoretically be used to discriminate
benign from malignant tumors and, by assessing the metabolic
activity of tumor cells following neoadjuvant therapy, it may
evaluate the treatment effect without invasive methods, such as
biopsy. PET/CT is a combination of the CT and PET techniques, which
is able to show the accurate anatomical structure and metabolic
activity of the tissues in the whole body. As a new and
sophisticated imaging diagnostic tool, PET/CT is gradually used in
an increasing number of medical centers. In the current literature,
extensive research has been performed on the application of PET/CT
in the diagnosis of a variety of tumors, such as lung, colorectal
and breast cancer, melanoma and lymphoma (1–3).
However, due to the low incidence of primary malignant osseous
sarcomas, there are only few reports with large patient samples on
the diagnostic accuracy or treatment effect evaluation of PET/CT in
osseous and soft tissue sarcomas.
Data collection methods
Literature search
Two independent reviewers performed a computerized
search of databases including PubMed (2003–2016), Medline
(2003–2016), Embase (2003–2016), Elsevier (2003–2016) and the
Cochrane Library (2008–2016) with the mesh words: ‘PET/CT’,
‘positron emission tomography/computed tomography’, ‘osseous
sarcoma’, ‘bone tumor’, ‘soft tissue sarcoma’ and ‘neoadjuvant’,
for randomized controlled trials, half-randomized controlled
studies, prospective and retrospective cohort studies on the
accuracy of PET/CT for the diagnosis of bone and soft tissue
sarcomas, and the evaluation of response to neoadjuvant therapy.
For studies whose eligibility for the inclusion criteria failed to
reach consensus between the two authors, a third author was invited
to settle the disputes.
Study quality assessment
Two authors independently assessed the quality of
the included studies by the Quality Assessment of Diagnostic
Accuracy Studies (QUADAS) tool (4).
Each study was scored as ‘+’ (positive), ‘-’ (negative) and ‘?’
(unclear). In case of disagreement, a third author made the final
decision. Studies with <7 ‘+’ were considered to be of low
methodological quality and high risk of bias. The methodological
quality of the included trials is outlined in Table I.
 | Table I.Results of quality assessment for 16
eligible studies (indicated by ref. nos.). |
Table I.
Results of quality assessment for 16
eligible studies (indicated by ref. nos.).
|
|
(Refs.) |
|---|
|
|
|
|---|
| Questions | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | (16) | (17) | (18) | (19) | (20) | (21) |
|---|
| Was the spectrum of
patients representative of the patients who received the test in
practice? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Were selection
criteria clearly described? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Is the reference
standard likely to help correctly classify the target
condition? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Is the time between
performance of reference standard and index test short enough? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Did the whole sample
or a random selection of the sample receive verification by using a
reference standard? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Did patients undergo
examination with the same reference standard regardless of the
index test result? | − | − | − | + | + | − | − | + | − | + | + | + | + | + | + | + |
| Was the reference
standard performed independently of the index test? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Was the execution
of the index test described in sufficient detail to permit
replication of the test? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Was the execution
of the reference standard described in sufficient detail to permit
replication of the test? | + | + | − | + | + | − | − | + | − | + | + | + | + | + | + | + |
| Were the index test
results interpreted without knowledge of the results of the
reference standard? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Were the reference
standard results interpreted without knowledge of the results of
the index test? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Were the same
clinical data available when test results were interpreted as would
be available in practice? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Were
uninterpretable and/or intermediate test results reported? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Were withdrawals
from the study explained? | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
Data extraction
Data in the included trials, including the authors
of each study, study design, patient sample size, patient age,
origin, time of follow-up and intervention methods, were extracted
by two independent reviewers. Patient numbers with true-positive,
false-positive, true-negative and false-negative diagnosis and
evaluations in each study were extracted and recorded in specific
tables. In case that the same patients were analyzed in more than
one study, they were extracted and analyzed as one patient
population.
Data were analyzed and processed by Meta-Disc
software (5). Two authors checked
the data input to ensure no errors were made. Considering the
possibility of publication bias between the studies, the analyses
were performed using the random-effects modes. The I2
test was used to test heterogeneity and studies were considered to
have significant heterogeneity if I2>50%. Subgroup or
sensitivity analysis was used in case of significant heterogeneity
due to the methodological quality of the included trials. The
differences in each study were defined by odds ratios (ORs) with
95% confidence intervals (95% CIs) of the categorical outcome
frequencies in the study groups and the control groups,
respectively. The OR of each individual trial was shown in a forest
plot.
Results
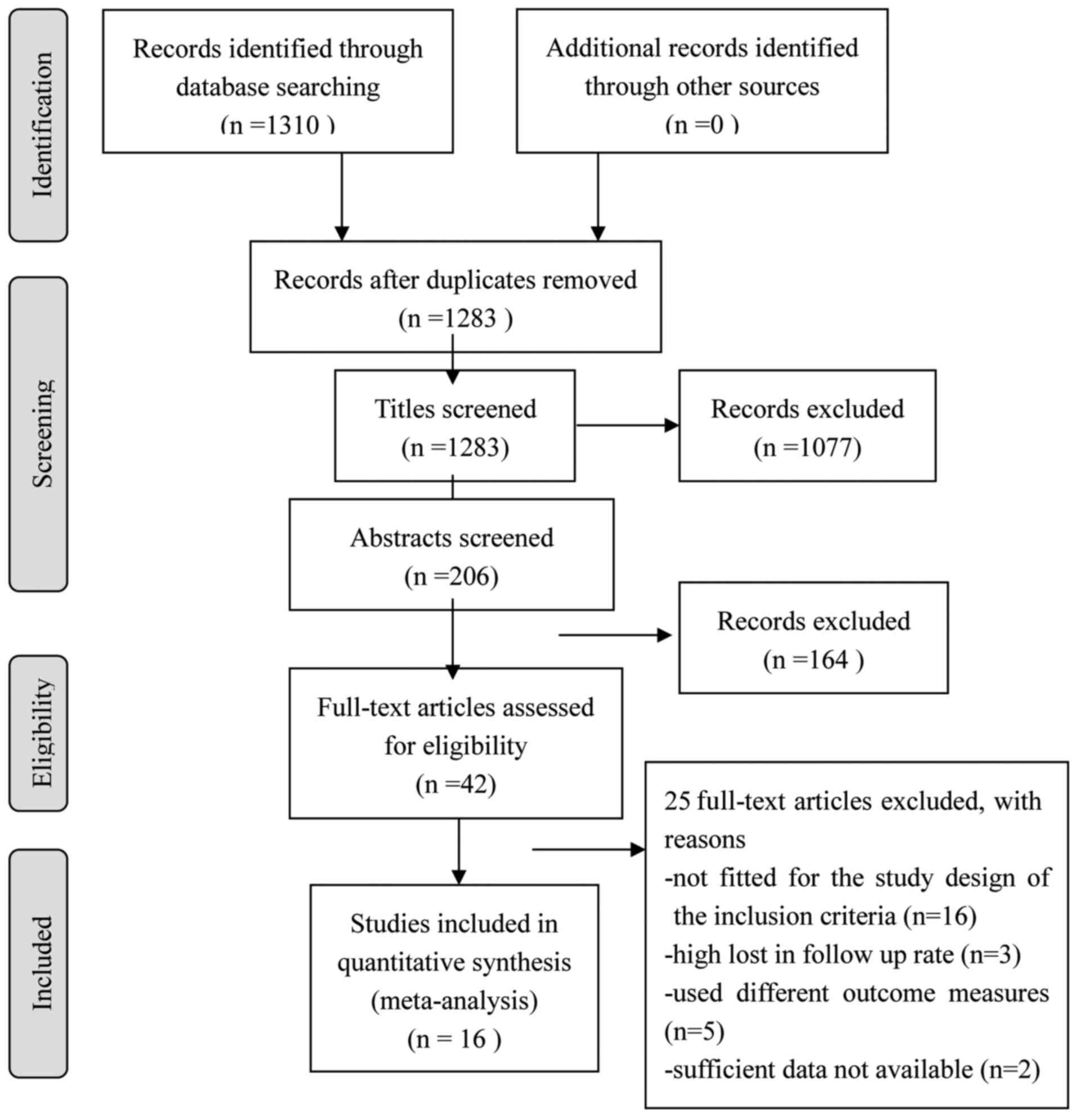
Results of the study selection
process
Of the 1,310 articles screened, 16 (6–21) were
selected for the final analysis (Fig.
1). The meta-analysis included a total of 883 patients and
2,214 lesions (Tables II and
III). The majority of the studies
were proven to be of relatively high quality according to the
QUADAS quality assessment tool (Table
I).
| Table II.Demographic characteristics of the
included studies. |
Table II.
Demographic characteristics of the
included studies.
| Authors | Patient no. | Agea, years | Study type | Patient
enrollment | Time of study | (Refs.) |
|---|
| Tateishi et
al | 117 | 42±21 | Prospective | Consecutive | Unclear | (6) |
| Strobel et
al | 50 | 36.9 (11–72) | Prospective | Consecutive | Unclear | (7) |
| Shin et
al | 91 | 42 (6–79) | Retrospective | Unclear | 2004.5–2007.6 | (8) |
| Charest et
al | 212 | 47±19.2 | Retrospective | Consecutive | 2004.5–2008.4 | (9) |
| Pepirkova et
al | 93 | 50.1±14.9 | Retrospective | Unclear | 2004.1–2007.5 | (10) |
| Fuglø et
al | 89 | NA | Retrospective | Unclear |
2001.12–2010.12 | (11) |
| Sharma et
al | 53 | 20.1±10.5 | Retrospective | Unclear | 2006.3–2012.1 | (12) |
| Xu et
al | 103 | 59.1±18.6 | Retrospective | Unclear | 2007.3–2013.2 | (13) |
| Byun et
al | 206 | 15 (4–71) | Retrospective | Consecutive | 2006.1–2011.11 | (14) |
| Iagaru et
al | 14 | 36±14 | Retrospective | Consecutive | 1999.1–2004.12 | (15) |
| Evilevitch et
al | 42 | 17 (7–31) | Prospective | Consecutive | 2005.1–2007.1 | (16) |
| Hamada et
al | 11 | 17 (10.68) | Prospective | Consecutive | 2002.6–2006.8 | (17) |
| Benz et
al | 12 | 31.6±15.0 | Prospective | Consecutive | 2005.2–2007.11 | (18) |
| Im et
al | 20 | 15 (10–25) | Prospective | Consecutive | 2003.8–2010.7 | (19) |
| Byun et
al | 27 | 15 (10–23) | Prospective | Consecutive | 2010.5–2012.3 | (20) |
| Byun et
al | 31 | 15 (10–21) | Prospective | Consecutive | 2010.5–2013.9 | (21) |
| Table III.Characteristics of PET/CT imaging and
of reference standards. |
Table III.
Characteristics of PET/CT imaging and
of reference standards.
| Authors | FDG (MBq) | Measures | Reference
standard | Potential
verification bias | (Refs.) |
|---|
| Tateishi et
al | 300–370 | Visualization,
SUV | Histology and
radiological follow-up | Very limited | (6) |
| Strobel et
al | 350–400 | Visualization,
SUV | Histology, clinical
and imaging follow-up | Very limited | (7) |
| Shin et
al | 8.1/kg | Visualization,
SUV | Histology, clinical
and imaging follow-up | Limited | (8) |
| Charest et
al | 370–500 | Visualization,
SUV | Histology | Very limited | (9) |
| Pepirkova et
al | 370–555 | Visualization,
SUV | Histology | Very limited | (10) |
| Fuglø et
al | 4.0/kg | Visualization,
SUV | Histopathology,
clinical and imaging follow-up | Limited | (11) |
| Sharma et
al | 370 | Visualization,
SUV | Histopathology,
clinical and imaging follow-up | Limited | (12) |
| Xu et
al | 3.5/kg | Visualization,
SUV | Histopathological
examination | Very limited | (13) |
| Byun et
al | 7.4/kg | Visualization,
SUV | Histology, clinical
and imaging follow-up | Very limited | (14) |
| Iagaru et
al | 550 | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (15) |
| Evilevitch et
al | 333–407 | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (16) |
| Hamada et
al | 370 | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (17) |
| Benz et
al | 7.8/kg | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (18) |
| Im et
al | 166–666 | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (19) |
| Byun et
al | 370 | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (20) |
| Byun et
al | 370 | Visualization,
SUV | Histopathological
examination of surgical specimen | Very limited | (21) |
Results of the meta-analysis
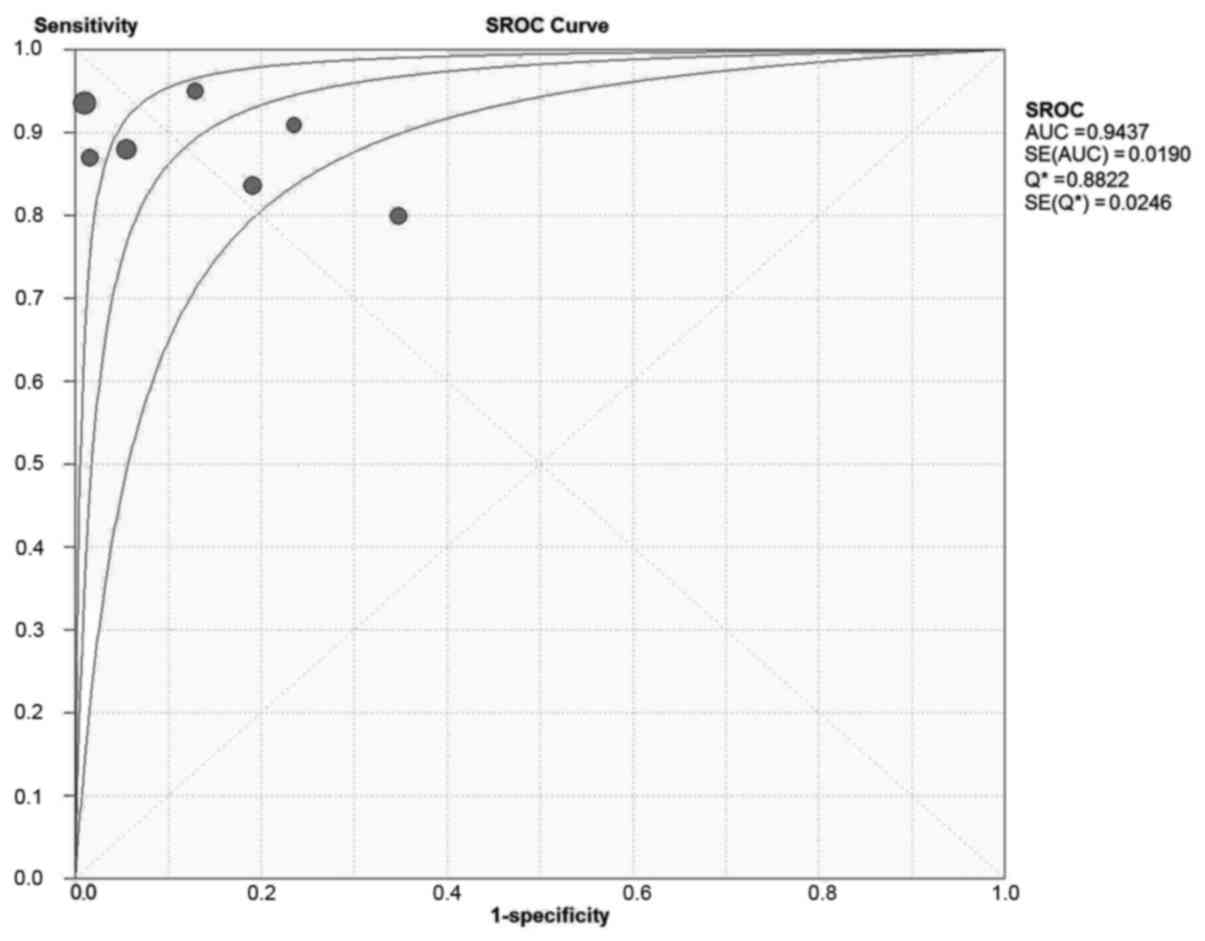
Diagnostic accuracy
A total of 9 studies, including 738 patients with
2,069 lesions, investigated the diagnostic accuracy of PET/CT in
osseous and soft tissue sarcomas (Table
IV). On patient-based analysis, the overall sensitivity and
specificity were 0.90 (0.86–0.92) and 0.89 (0.85–0.92). The area
under the summary receiver operating characteristic (SROC) curve
was 0.97, Q=0.91 (Fig. 2). On
lesion-based analysis, the overall sensitivity and specificity were
0.96 (0.94–0.97) and 0.95 (0.93–0.96). The area under the SROC
curve was 0.97, Q=0.88 (. 3). The meta-analysis indicated that
PET/CT is able to diagnose osseous and soft tissue sarcomas with
high sensitivity and specificity.
| Table IV.Diagnostic accuracy of PET/CT on
osseous and soft tissue sarcomas in the included studies. |
Table IV.
Diagnostic accuracy of PET/CT on
osseous and soft tissue sarcomas in the included studies.
| Authors | TP | FP | FN | TN | Sensitivity (95%
CI) | Specificity (95%
CI) | (Refs.) |
|---|
| Byun et
al | 52 | 15 | 3 | 763 | 0.95
(0.85–0.99) | 0.98
(0.97–0.99) | (20) |
| Charest et
al | 153 | 0 | 10 | 49 | 0.94
(0.89–0.97) | 1.00
(0.93–1.00) | (9) |
| Fuglø et
al | 20 | 1 | 3 | 64 | 0.87
(0.66–0.97) | 0.98
(0.92–1.00) | (11) |
| Pepirkova et
al | 424 | 0 | 3 | 71 | 0.99
(0.98–1.00) | 1.00
(0.95–1.00) | (10) |
| Sharma et
al | 38 | 4 | 2 | 27 | 0.95
(0.83–0.99) | 0.87
(0.70–0.96) | (12) |
| Shin et
al | 36 | 16 | 9 | 30 | 0.80
(0.65–0.90) | 0.65
(0.50–0.79) | (8) |
| Strobel et
al | 30 | 4 | 3 | 13 | 0.91
(0.76–0.98) | 0.76
(0.50–0.93) | (7) |
| Tateishi et
al | 44 | 4 | 6 | 69 | 0.88
(0.76–0.95) | 0.95
(0.87–0.98) | (6) |
| Xu et
al | 51 | 8 | 10 | 34 | 0.84
(0.72–0.92) | 0.81
(0.66–0.91) | (13) |
| All cases | 372 | 37 | 43 | 286 | 0.90
(0.86–0.92) | 0.89
(0.85–0.92) |
| All lesions | 848 | 52 | 49 | 1,120 | 0.95
(0.93–0.96) | 0.96
(0.94–0.97) |
|
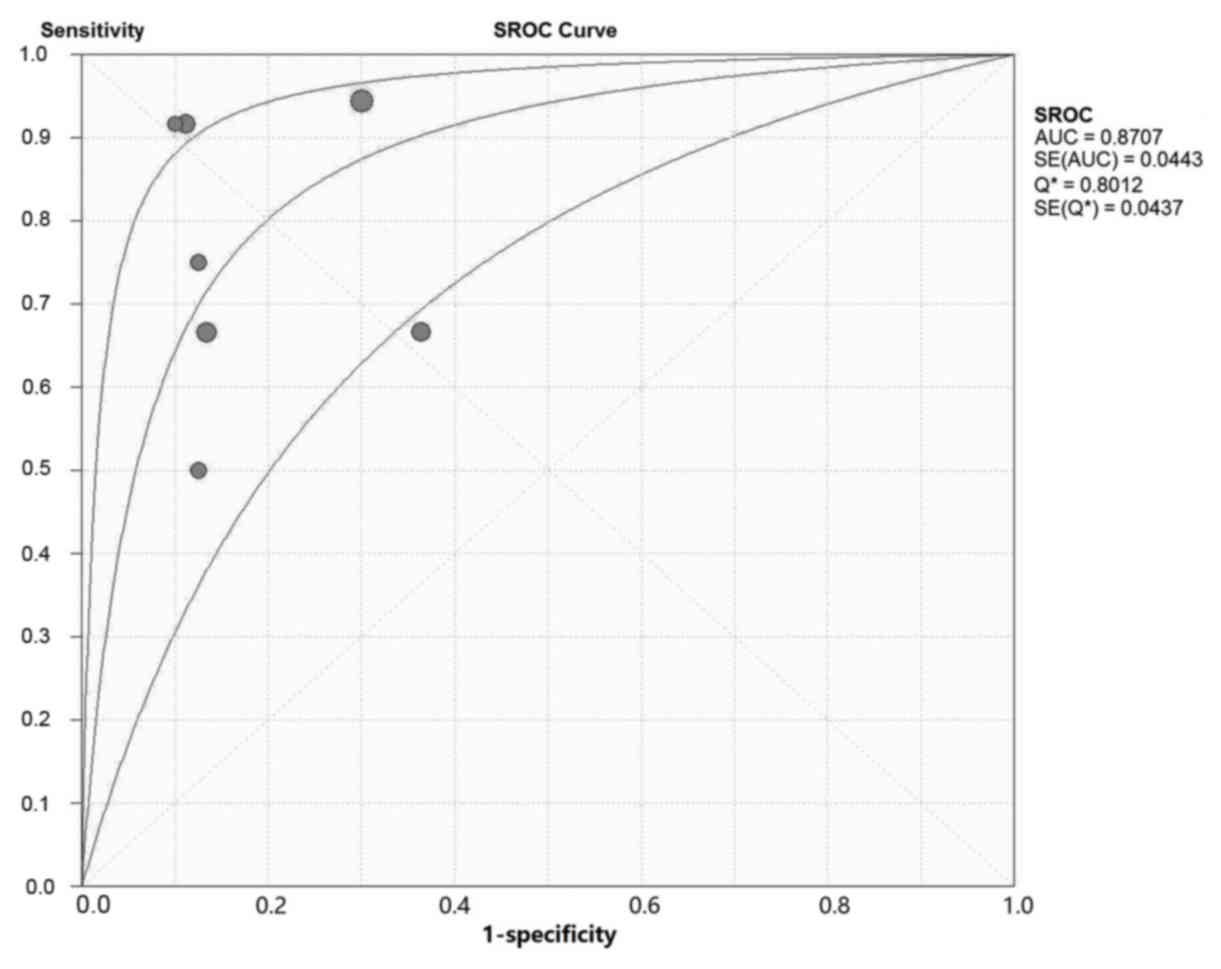
Evaluation of response to neoadjuvant
therapy
A total of 7 studies, including 145 patients,
investigated the accuracy of PET/CT in assessing the treatment
effect of neoadjuvant therapy on patients with osseous and soft
tissue sarcomas (Table V).
Generally, a ratio of maximum standardized uptake value (SUVmax)
after therapy/SUVmax prior to therapy of <0.5 was considered as
an indication of effective neoadjuvant therapy in the index test,
and necrosis of >90% in the intraoperative specimen was
considered as an indication of effective neoadjuvant therapy in the
reference test. The overall sensitivity and specificity were 0.79
(0.30–0.93) and 0.79 (0.69–0.89), respectively. The area under the
SROC curve was 0.87, Q=0.80 (Fig.
4). The meta-analysis indicated that PET/CT may be used to
monitor the effect of neoadjuvant therapy in patients with osseous
and soft tissue sarcomas with high sensitivity and specificity.
| Table V.Accuracy of PET/CT assessment on the
effect of neoadjuvant therapy on patients with osseous and soft
tissue sarcomas in the included studies. |
Table V.
Accuracy of PET/CT assessment on the
effect of neoadjuvant therapy on patients with osseous and soft
tissue sarcomas in the included studies.
| Authors | TP | FP | FN | TN | Sensitivity (95%
CI) | Specificity (95%
CI) | (Refs.) |
|---|
| Benz et
al | 3 | 1 | 1 | 7 | 0.75
(0.19–0.99) | 0.88
(0.47–1.00) | (18) |
| Byun et
al | 8 | 2 | 4 | 13 | 0.67
(0.35–0.90) | 0.87
(0.60–0.98) | (20) |
| Byun et
al | 11 | 1 | 1 | 8 | 0.92
(0.62–1.00) | 0.89
(0.52–1.00) | (21) |
| Evilevitch et
al | 8 | 10 | 0 | 24 | 1.00
(0.63–1.00) | 0.71
(0.53–0.85) | (16) |
| Hamada et
al | 5 | 0 | 0 | 4 | 1.00
(0.48–1.00) | 0.88
(0.40–1.00) | (17) |
| Iagaru et
al | 3 | 1 | 3 | 7 | 0.50
(0.12–0.88) | 0.88
(0.47–1.00) | (15) |
| Im et
al | 6 | 4 | 3 | 7 | 0.67
(0.30–0.93) | 0.64
(0.31–0.89) | (19) |
| Total | 44 | 19 | 12 | 70 | 0.79
(0.30–0.93) | 0.79
(0.69–0.89) |
|
Discussion
Imaging studies are important for the diagnosis of
various tumors. Currently, radiographic tests such as X-ray, CT and
MRI are widely applied for the diagnosis and treatment of
musculoskeletal system malignancies (22).
18F-fluorodeoxyglucose (FDG) PET is used
for the semiquantification of glucose consumption by cells in the
body, which makes it possible to measure the enhancement of
metabolic activity in cancer tissue. This is normally performed by
calculating the SUVmax. 18F-FDG PET has been
successfully used for the diagnosis of several types of cancer,
such as lung cancer, melanoma, lymphoma, head and neck tumors,
brain tumors, esophageal and colorectal cancer (23). The majority of the studies on the
diagnostic value of PET in different types of tumors have concluded
that it is a sensitive imaging modality for detection, staging and
re-staging in oncology (24–26).
FDG-PET has been applied for diagnostic purposes in
various malignant tumors since the early 90s (27). However, although 18F-FDG
may locate abnormally functioning anatomical structures, the
precise localization of the tumors may not be possible with PET
alone. Combining PET with a high-resolution anatomical imaging
modality, such as CT, addresses this issue, provided that the
images from the two modalities are accurately co-registered. Since
2003, a combination of PET and CT in one imaging device has gained
increasing popularity and is referred to as integrated PET/CT.
Integrated PET/CT is superior to PET or CT alone, as it can
accomplish morphological and functional imaging in one procedure,
and the images obtained with PET/CT were more accurate regarding
localization of the tumor compared with PET and CT alone, or the
fusion of PET and CT with software (28).
There are several reports on predicting the
aggressiveness of musculoskeletal tumors by measuring the glucose
consumption level using PET/CT (29). However, due to the low incidence of
primary malignant osseous sarcomas and the high cost of PRT/CT
imaging, the majority of those studies included only a small number
of patients; thus, the level of evidence obtained from those
studies was greatly compromised.
The percentage of necrotic tissue following adjuvant
therapy of tumors is one of the strongest prognostic factors of
osteosarcoma (30). In the present
study, PET/CT assessed the effect of neoadjuvant therapy with a
sensitivity and specificity of 0.79 (0.30–0.93) and 0.79
(0.69–0.89), respectively, indicating that PET/CT may be a reliable
non-invasive method for evaluating the effect of neoadjuvant
therapy on patients with osseous and soft tissue sarcomas. However,
as only 145 patients were included in the meta-analysis, a larger
sample is required to reach a more reliable conclusion.
Although the present study provided evidence on the
applicability of PET/CT on the diagnosis and evaluation of response
to neoadjuvant therapy for osseous and soft tissue sarcomas using
the SUVmax value, and the quality of the included studies was
relatively high, the overall sample size may be insufficient.
Considering that osseous as well as soft tissue sarcomas are
malignancies with a low incidence, multicenter prospective studies
with longer follow-up are required to investigate the full
potential of PET/CT in the diagnosis and treatment of
musculoskeletal tumors.
In conclusion, PET/CT may be a reliable method with
high accuracy for the diagnosis and evaluation of treatment
efficacy for bone and soft tissue sarcomas, although the present
findings require verification by larger-sample studies.
Acknowledgements
The present study did not directly involve any human
or animal subjects. The study was approved by the Ethics Committee
of The Sixth Affiliated Hospital of Xinjiang Medical
University.
References
|
1
|
Hoh CK, Schiepers C, Seltzer MA, Gambhir
SS, Silverman DH, Czernin J, Maddahi J and Phelps ME: PET in
oncology: Will it replace the other modalities? Semin Nucl Med.
27:94–106. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brock CS, Meikle SR and Price P: Does
fluorine-18 fluorodeoxyglucose metabolic imaging of tumors benefit
oncology? Eur J Nucl Med. 24:691–705. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bar-Shalom R, Valdivia AY and Blaufox MD:
PET imaging in oncology. Semin Nucl Med. 30:150–185. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Whiting P, Rutjes AW, Reitsma JB, Bossuyt
PM and Kleijnen J: The development of QUADAS: A tool for the
quality assessment of studies of diagnostic accuracy included in
systematic reviews. BMC Med Res Methodol. 3:252003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zamora J, Abraira V, Muriel A, Khan K and
Coomarasamy A: Meta-DiSc: A software for meta-analysis of test
accuracy data. BMC Med Res Methodol. 6:312006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tateishi U, Yamaguchi U, Seki K, Terauchi
T, Arai Y and Kim EE: Bone and Soft-Tissue Sarcoma: Preoperative
Staging with Fluorine 18Fluorodeoxyglucose PET/CT and Conventional
Imaging. Radiology. 245:839–847. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Strobel K, Exner UE, Stumpe KD, Hany TF,
Bode B, Mende K, Veit-Haibach P, von Schulthess GK and Hodler J:
The additional value of CT images interpretation in the
differential diagnosis of benign vs. malignant primary bone lesions
with 18F-FDG-PET/CT. Eur J Nucl Med Mol Imaging. 35:2000–2008.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shin D, Shon OJ, Han DS, Choi JH, Chun KA
and Cho IH: The clinical efficacy of (18)F-FDG-PET/CT in benign and
malignant musculoskeletal tumors. Ann Nucl Med. 22:603–609. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Charest M, Hickeson M, Lisbona R,
Novales-Diaz JA, Derbekyan V and Turcotte RE: FDG PET/CT imaging in
primary osseous and soft tissue sarcomas: A retrospective review of
212 cases. Eur J Nucl Med Mol Imaging. 36:1944–1951. 2008.
View Article : Google Scholar
|
|
10
|
Piperkova E, Mikhaeil M, Mousavi A, Libes
R, Viejo-Rullan F, Lin H, Rosen G and Abdel-Dayem H: Impact of PET
and CT in PET/CT studies for staging and evaluating treatment
response in bone and soft tissue sarcomas. Clin Nucl Med.
34:146–150. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fuglø HM, Jørgensen SM, Loft A, Hovgaard D
and Petersen MM: The diagnostic and prognostic value of 18F-FDG
PET/CT in the initial assessment of high-grade bone and soft tissue
sarcoma a retrospective study of 89 patients. Eur J Nucl Med Mol
Imaging. 39:1416–1424. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sharma P, Khangembam BC, Suman KC, Singh
H, Rastogi S, Khan SA, Bakhshi S, Thulkar S, Bal C, Malhotra A and
Kumar R: Diagnostic accuracy of 18F-FDG PET/CT for detecting
recurrence in patients with primary skeletal Ewing sarcoma. Eur J
Nucl Med Mol Imaging. 40:1036–1043. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xu R, Kido S, Suga K, Hirano Y, Tachibana
R, Muramatsu K, Chagawa K and Tanaka S: Texture analysis on
(18)F-FDG PET/CT images to differentiate malignant and benign bone
and soft-tissue lesions. Ann Nucl Med. 28:926–935. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Byun BH, Kong CB, Lim I, Kim BI, Choi CW,
Song WS, Cho WH, Jeon DG, Koh JS, Lee SY and Lim SM: Comparison of
(18)F-FDG PET/CT and (99 m) Tc-MDP bone metastasis in osteosarcoma.
Skeletal Radiol. 42:1673–1681. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Iagaru A, Masamed R, Chawla S, Menendez
LR, Fedenko A and Conti PS: F-18 FDG PET and PET/CT Evaluation of
Response to Chemotherapy in Bone and Soft Tissue Sarcomas. Clin
Nucl Med. 33:8–13. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Evilevitch V, Weber WA, Tap WD,
Allen-Auerbach M, Chow K, Nelson SD, Eilber FR, Eckardt JJ,
Elashoff RM, Phelps ME, et al: Reduction of glucose metabolic
activity is more accurate than change in size at predicting
histopathologic response to neoadjuvant therapy in high-grade
soft-tissue sarcomas. Clin Cancer Res. 14:715–720. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hamada K, Tomita Y, Inoue A, Fujimoto T,
Hashimoto N, Myoui A, Yoshikawa H and Hatazawa J: Evaluation of
chemotherapy response in osteosarcoma with FDG-PET. Ann Nucl Med.
23:89–95. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Benz MR, Czernin J, Allen-Auerbach MS, Tap
WD, Dry SM, Elashoff D, Chow K, Evilevitch V, Eckardt JJ, Phelps
ME, et al: FDG-PET/CT imaging predicts histopathologic treatment
responses after the initial cycle of neoadjuvant chemotherapy in
high-grade soft-tissue sarcomas. Clin Cancer Res. 15:2856–2863.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Im HJ, Kim TS, Park SY, Min HS, Kim JH,
Kang HG, Park SE, Kwon MM, Yoon JH, Park HJ, et al: Prediction of
tumour necrosis fractions using metabolic and volumetric 18F-FDG
PET/CT indices, after one course and at the completion of
neoadjuvant chemotherapy, in children and young adults with
osteosarcoma. Eur J Nucl Med Mol Imaging. 39:39–49. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Byun BH, Kong CB, Lim I, Choi CW, Song WS,
Cho WH, Jeon DG, Koh JS, Lee SY and Lim SM: Combination of 18F-FDG
PET/CT and diffusion-weighted MR imaging as a predictor of
histologic response to neoadjuvant chemotherapy: Preliminary
results in osteosarcoma. J Nucl Med. 54:1053–1059. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Byun BH, Kim SH, Lim SM, Lim I, Kong CB,
Song WS, Cho WH, Jeon DG, Lee SY, Koh JS and Chung SK: Prediction
of response to neoadjuvant chemotherapy in osteosarcoma using
dual-phase (18)F-FDG PET/CT. Eur radiol. 25:2015–2024. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Nishio J, Ideta S, Iwasaki H and Naito M:
Scapular osteochondrolipoma: Imaging features with pathological
correlation. Oncol Lett. 6:817–820. 2013.PubMed/NCBI
|
|
23
|
Brenner W, Bohuslavizki KH and Eary JF:
PET Imaging of Osteosarcoma. J Nucl Med. 44:930–942.
2003.PubMed/NCBI
|
|
24
|
Fletcher JW, Djulbegovic B, Soares HP,
Siegel BA, Lowe VJ, Lyman GH, Coleman RE, Wahl R, Paschold JC,
Avril N, et al: Recommendations on the use of 18F-FDG PET in
oncology. J Nucl Med. 49:480–508. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Erdi YE: The use of PET for radiotherapy.
Curr Med Imaging Rev. 3:3–16. 2007. View Article : Google Scholar
|
|
26
|
de G eus-Oei LF, van der Heijden HF,
Corstens FH and Oyen WJ: Predictive and prognostic value of FDG-PET
in nonsmall-cell lung cancer: A systematic review. Cancer.
110:1654–1664. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hillner BE, Siegel BA, Shields AF, Liu D,
Gareen IF, Hunt E and Coleman RE: Relationship between cancer type
and impact of PET and PET/CT on intended management: Findings of
the National Oncologic PET Registry. J Nucl Med. 49:1928–1935.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Boellaard R, O'Doherty MJ, Weber WA,
Mottaghy FM, Lonsdale MN, Stroobants SG, Oyen WJ, Kotzerke J,
Hoekstra OS, Pruim J, et al: FDG PET and PET/CT: EANM procedure
guidelines for tumour PET imaging: Version 1.0. Eur J Nucl Med Mol
Imaging. 37:181–200. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Muheremu A and Niu X: Positron emission
tomography/computed tomography for bone tumors. Oncol Lett.
9:522–526. 2015.PubMed/NCBI
|
|
30
|
Glasser DB, Lane JM, Huvos AG, Marcove RC
and Rosen G: Survival, prognosis and therapeutic response in
osteogenic sarcoma: The Memorial Hospital experience. Cancer.
69:698–708. 1992. View Article : Google Scholar : PubMed/NCBI
|