Introduction
Angiomyofibroblastoma (AMFB) is a benign mesenchymal
soft tissue tumor first described by Fletcher et al in 1992
(1). AMFB commonly develops in the
female external genitalia, but it has also been reported to occur
in the male scrotum or groin (2,3). The
average age at onset is in the late 30s, and it is a
well-circumscribed, elastic, soft tumor, usually sized <5 cm,
white to yellowish brown and sponge-like or myxoid on
cross-section. Histologically, the tumor cells are oval to
spindle-shaped and arranged in a fascicular, wavy or palisade
pattern, with areas of high and low cell density, with stromal
proliferation of small vessels. Immunohistochemically, the tumor
cells are usually positive for vimentin, desmin, estrogen receptor
and progesterone receptor, and negative for S-100 and α-smooth
muscle actin (α-SMA), although desmin-negative and α-SMA-positive
cases have been reported (1,3–5). AMFB
may be difficult to distinguish from aggressive angiomyxoma (AAM).
AMFB is usually diagnosed based on the histopathological findings
of the resected specimens. The aim of the present study was to
report an AMFB case that was diagnosed preoperatively based on the
clinical course and magnetic resonance imaging (MRI) findings and
describe our experience with the management of this patient, along
with a review of the related literature.
Case report
A 50-year-old woman (gravida 2, para 2) presented
with the chief complaint of a palpable mass in the vulva. The
patient's family history was unremarkable, but she had been
diagnosed with uterine adenomyosis at the age of 44 years and
underwent abdominal total hysterectomy. Two years earlier, the
patient had noticed the presence of a small nodule in the right
labium majus, but it was left untreated. The nodule gradually
increased in size and was eventually accompanied by spontaneous
pain, prompting the patient to visit our department. At the initial
visit, an elastic, firm, goose egg-sized subcutaneous mass
protruding from the right labium majus was detected on physical
examination (Fig. 1). On palpation,
the mass was well-circumscribed, with good mobility against the
surrounding tissues. The skin overlaying the mass was
macroscopically normal, and no subjective pain was noted. There
were no abnormalities in the complete blood count or biochemical
examinations. The tumor marker levels of carcinoembryonic antigen
(1.0 ng/ml), carbohydrate antigen (CA)19-9 (<2.0 U/ml) and CA
125 (8.8 U/ml), were also normal. MRI scans revealed a solid tumor
measuring 7 cm in diameter under the skin on the right labium
majus, which was sharply marginated, without infiltration of the
deep tissues. The tumor was hypointense on T1-weighted images and
exhibited mostly homogeneous enhancement on fat-saturated (fat-sat)
gadolinium-enhanced images, although there was a poorly enhanced
area at the center, which was attributed to either necrosis or
degeneration (Fig. 2A and B). The
patient had previously undergone fat-sat T2-weighted MRI prior to
undergoing hysterectomy at the age of 44 years, which detected a
mass measuring 2.6 cm in the same region (Fig. 2C). Based on the clinical course and
imaging findings, AMFB was diagnosed and surgery was performed. The
tumor was removed under general anesthesia. Although the tumor was
well-circumscribed, it was highly vascular, and the intraoperative
ligation of the blood vessels was time-consuming. The operative
time was 41 min and the intraoperative blood loss was 70 ml. The
postoperative course was eventless and the patient was discharged
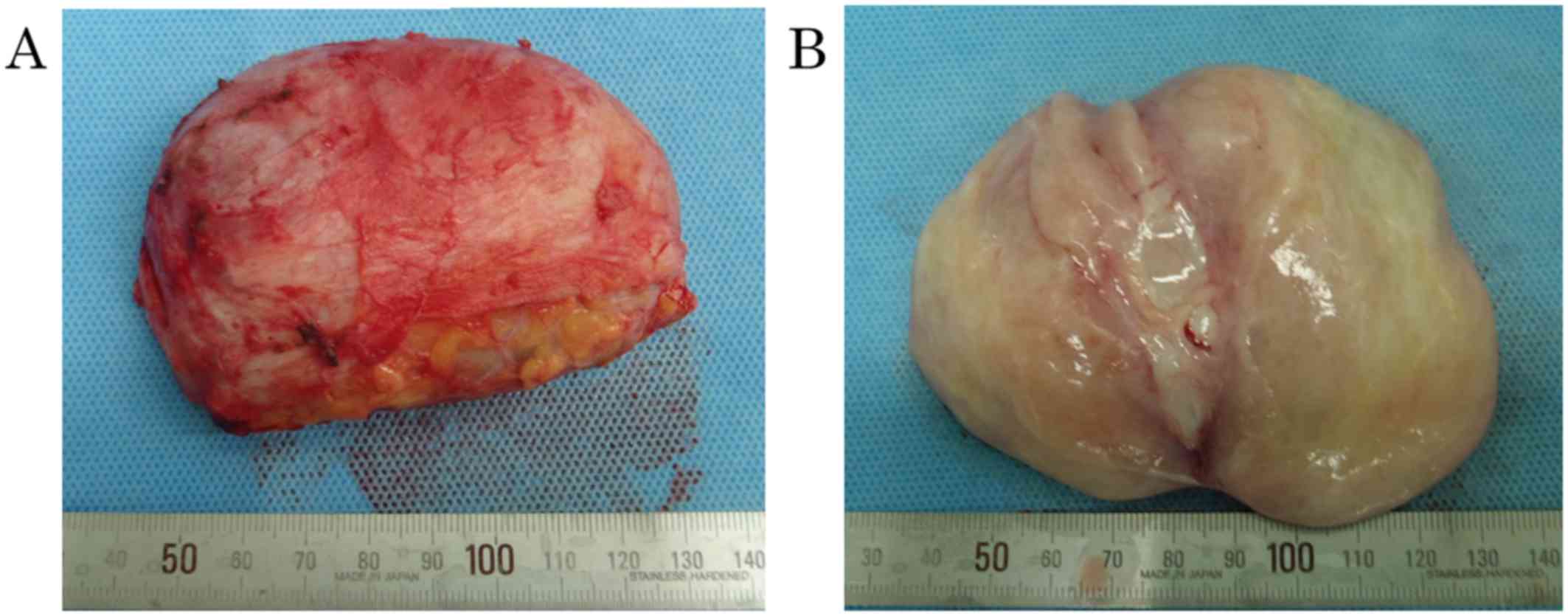
on the 7th postoperative day. Macroscopically, the resected tumor
measured 8×7×5 cm. The tumor was not encapsulated, but was
well-circumscribed, white, edematous and solid (Fig. 3A and B). Histologically, the tumor
consisted of sparse collagen fibers, along with small to
medium-sized blood vessels, with a scattered or clustered
distribution. The tumor cells were aggregated around blood vessels,
they were oval to spindle-shaped and had acidophilic and fibrous
cytoplasm. Outside the perivascular area, cellular components were
sparse. No mucin deposition was seen in the stroma, and there was
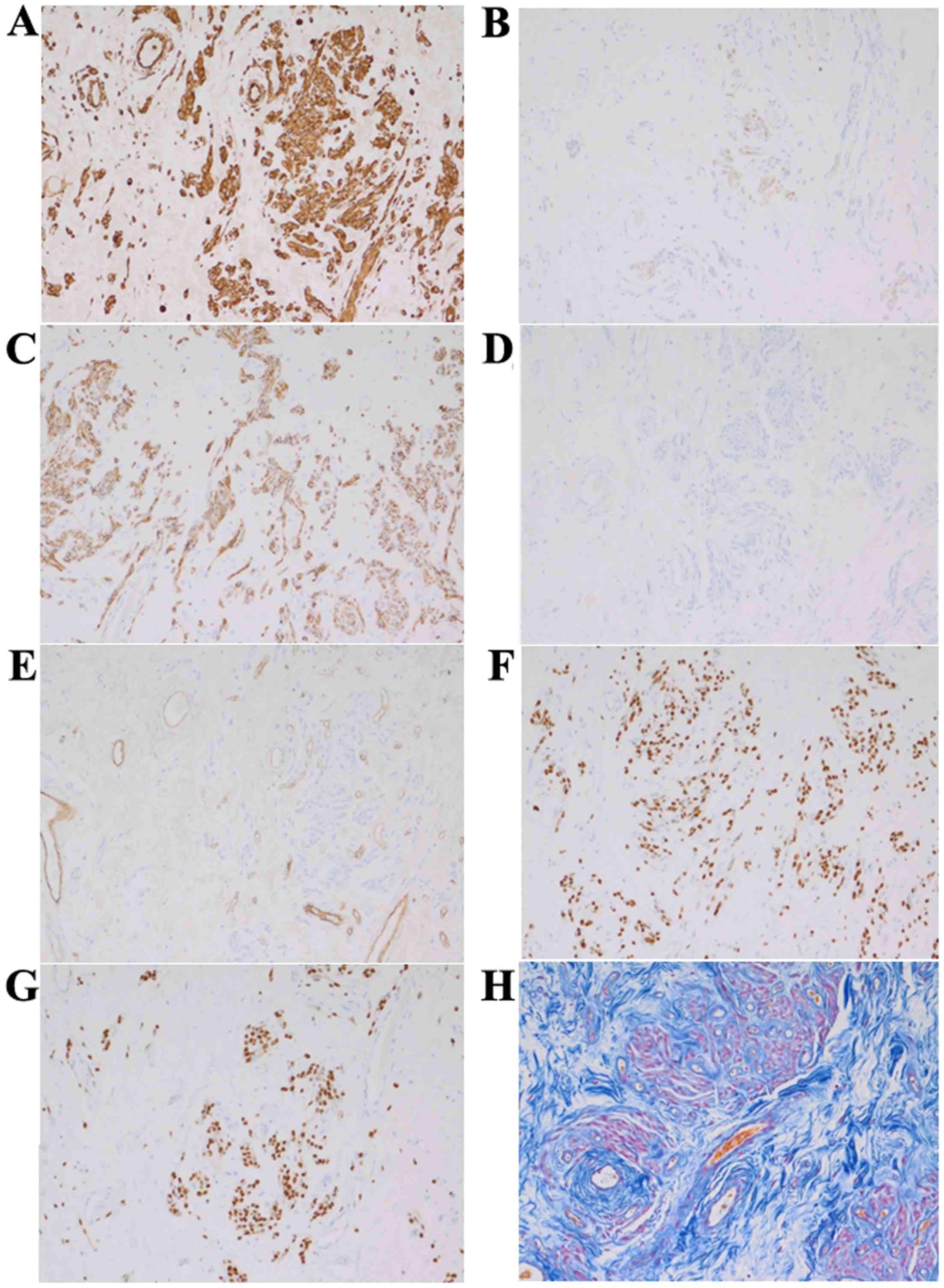
no thickening or hyalinization of the vascular walls (Fig. 4). On immunohistochemical examination,
the tumor cells were positive for vimentin, desmin, N-CAM, CD-34,
estrogen receptor and progesterone receptor, and negative for
S-100. The Azan-Mallory staining result was also positive (Fig. 5A-H). Based on these findings, the
histopathological diagnosis of AMFB was confirmed. At 10 months
postoperatively, no recurrence was observed.
Written informed consent was obtained from the
patient regarding the publication of the case details and
associated images.
Discussion
AMFB is a benign mesenchymal soft tissue tumor first
described by Fletcher et al in 1992 (1). AMFB commonly develops in the female
external genitalia, but there have also been a few reports of AMFB
involving the male scrotum or groin (2,3). As
regards the clinical characteristics of AMFB, the average age at
onset is in the late 30 s, and it is a well-circumscribed, elastic,
soft subcutaneous tumor, usually <5 cm in diameter; the cut
surface appears white to yellowish brown and sponge-like or myxoid.
Histologically, oval to spindle-shaped tumor cells are arranged in
a fascicular, wavy or palisade pattern, with areas of both high and
low cell density. Proliferation of small vessels is noted in the
stroma. Immunohistochemically, the tumor cells are usually positive
for vimentin, desmin, estrogen receptor and progesterone receptor,
and negative for S-100 and α-SMA, although some cases are
reportedly desmin-negative and α-SMA-positive (1,3–5).
It is important to be aware that AAM must be
considered in the differential diagnosis of AMFB. AAM was described
in 1983 by Steeper and Rosai (6).
AAM is a tumor of the external genitalia that affects young women
and is similar to AMFB in terms of both clinical presentation and
histopathological characteristics. AAM grows rapidly and
infiltrates the surrounding tissues. This tumor often recurs
locally after surgical resection, but usually does not metastasize
(6). As regards the histological
differences between AMFB and AAM, the former contains both hypo-
and hypercellular areas, whereas the latter exhibits sparse,
homogeneous growth of tumor cells with atypical nuclei. While the
stroma in AAM displays mucin deposition, proliferation of small to
medium-sized blood vessels, dilation of vascular spaces,
hyalinization and thickening of vascular walls, the stroma in AMFB
only exhibits proliferation of small blood vessels. On
immunohistochemical examination, the tumor cells of both AAM and
AMFB are positive for vimentin, estrogen receptor and progesterone
receptor and negative for S-100, but the cell kinetics for desmin
and α-SMA may differ among individual cases. Therefore,
immunochemical results alone are not sufficient to distinguish AMFB
from AAM. AAM grows rapidly and reaches a diameter of >5 cm. In
the majority of AMFB cases, the tumor is sized <5 cm (7). According to Nagai et al, the
average diameter of AMFB is 4.5 cm (7). However, there are reports describing
AMFB cases with tumors >10 cm in size (8), and it is critical to distinguish these
cases from AAM. The imaging characteristics that differentiate AMFB
from AAM are listed in Table I.
While AMFB appears well-circumscribed with strong heterogeneous
enhancement, AAM has a strong infiltrative tendency and is poorly
circumscribed, while the contrast-enhanced images are characterized
by a whorled or swirling growth pattern (9,10).
 | Table I.Differentiation between AMFB and
AAM. |
Table I.
Differentiation between AMFB and
AAM.
| Characteristics | AMFB | AAM |
|---|
| Imaging findings |
Well-circumscribed | Infiltrative
tendency |
|
| Strong heterogeneous
enhancement | Enhanced in a whorled
or swirling growth pattern |
|
| Relatively small (≤5
cm) | Large (≥5 cm) |
| Pathological
findings | Oval to
spindle-shaped cells | Stellate to
spindle-shaped cells |
|
| Both hyper- and
hypocellular areas are present | Sparse, homogeneous
cell distribution |
| Clinical outcome | Recurrence is
rare | Recurrence is
frequent |
In the present case, based on the imaging
characteristics and clinical course, the preoperative diagnosis was
AMFB and surgery was performed. The tumor was 8 cm in diameter,
which was rather large for an AMFB. Reducing intraoperative blood
loss is important, and prior studies have explored measures to
prevent excessive bleeding. Quintero et al reported that
they succeeded in reducing blood loss in a patient with a large
AMFB, 12 cm in diameter, by performing preoperative embolization
(11). In the present case, there
were several blood vessels feeding the tumor, necessitating
intraoperative ligation. Thus, the operation lasted longer than
expected and the amount of blood loss was 70 ml. AMFB has a benign
prognosis following simple surgical resection. However, in patients
with large AMFBs, the blood vessels feeding the tumor are
well-developed, and it is important to consider the possibility of
excessive blood loss when performing surgery in such patients.
There are sporadic reports on using
gonadotropin-releasing hormone (GnRH) analogs for the preoperative
reduction of AAM and prevention of postoperative recurrence
(12–15). However, there have been no reports of
their use for the treatment of AMFB. Thus, as there is no
scientific evidence showing that GnRH analogs reduce the recurrence
rate of AMFB, this patient is currently followed up without
administering additional treatment after surgery.
The patient in the present case had also been
diagnosed with uterine adenomyosis at the age of 44 years and
underwent hysterectomy. The preoperative MRI performed at the time
revealed a mass measuring 2.6 cm in diameter, but the patient
received no medical treatment. When surgery was performed for the
AMFB, the tumor was found to have grown to 7.5 cm in diameter over
the previous 6 years, suggesting a relatively slow growth rate.
Slow tumor growth is another characteristic of AMFB that
distinguishes it from AAM, and was also one of the factors that
facilitated the preoperative diagnosis. None of the past studies on
AMFB used images obtained over the 6-year period prior to surgery
for making comparisons. This report is considered valuable as it
may serve as a verification of the relatively slow growth of
AMFB.
References
|
1
|
Fletcher CD, Tsang WY, Fisher C, Lee KC
and Chan JK: Angiomyofibroblastoma of the vulva. A benign neoplasm
distinct from aggressive angiomyxoma. Am J Surg Pathol. 16:373–382.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ding G, Yu Y, Jin M, Xu J and Zhang Z:
Angiomyofibroblastoma-like tumor of the scrotum: A case report and
literature review. Oncol Lett. 7:435–438. 2014.PubMed/NCBI
|
|
3
|
Ito M, Yamaoka H, Sano K and Hotchi M:
Angiomyofibroblastoma of the male inguinal region. Arch Pathol Lab
Med. 124:1679–1681. 2000.PubMed/NCBI
|
|
4
|
Laskin WB, Fetsch JF and Tavassoli FA:
Angiomyofibroblastoma of the female genital tract: Analysis of 17
cases including a lipomatous variant. Hum Pathol. 28:1046–1055.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Aono K, Sekine M, Serikawa T, Tojo Y,
Hanaoka J and Takeuchi Y: Two cases of rare vulvar mesenchymal
tumor: Comparisons of aggressive angiomyxoma with
angiomyofibroblastoma. Acta Obst Gynaec Jpn. 50:975–978. 1998.(In
Japanese).
|
|
6
|
Steeper TA and Rosai J: Aggressive
angiomyxoma of the female pelvis and perineum. Report of nine cases
of distinctive type of gynecologic soft-tissue neoplasm. Am J Surg
Pathol. 7:463–475. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nagai K, Adachi K and Saito H: Huge
pedunculated angiomyofibroblastoma of vulva. Int J Clin Oncol.
15:201–205. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Qiu P, Wang Z, Li Y and Cui G: Giant
pelvic angiomyofibroblastoma: Case report and literature review.
Diagn Pathol. 9:1062014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sharon WW Goldkum JR: Enzinger &
Weiss's Soft Tissue Tumors 5th edition. Philadelphia: Mosby
Elsevier; pp. 10872008
|
|
10
|
Geng J, Hu S and Wang F: Large paravaginal
angiomyofibroblastoma: Magnetic resonance imaging findings. Jpn J
Radiol. 29:152–155. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Quintero C, Sasken H, Houck KL and
Hernandez E: Angiomyofibroblastoma of the retroperitoneum: A case
report. J Reprod Med. 52:741–744. 2007.PubMed/NCBI
|
|
12
|
Lee CW, Yoon JH, Park DC and Lee SJ:
Aggressive angiomyxoma of the vulva treated by using a
gonadotropin-releasing hormone agonist: A case report. Eur J
Gynaecol Oncol. 32:686–688. 2011.PubMed/NCBI
|
|
13
|
Palomba S, Oppedisano R, Annunziata G,
Zullo F and Amorosi A: Leuprolide acetate depot plus high-dose
raloxifene hydrochloride before and after surgery for recurrent
vaginal aggressive angiomyxoma: A case report. Gynecol Oncol.
123:172–173. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
McCluggage WG, Jamieson T, Dobbs SP and
Grey A: Aggressive angiomyxoma of the vulva: Dramatic response to
gonadotropin-releasing hormone agonist therapy. Gynecol Oncol.
100:623–625. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fine BA, Munoz AK, Litz CE and Gershenson
DM: Primary medical management of recurrent aggressive angiomyxoma
of the vulva with a gonadotropin-releasing hormone agonist. Gynecol
Oncol. 81:120–122. 2001. View Article : Google Scholar : PubMed/NCBI
|