Introduction
Lung cancer is the leading cause of cancer-related
mortality in Japan as well as worldwide (1). Non-small-cell lung cancer NSCLC is the
third most common cause of bone metastases following breast and
prostate cancer (2). It has been
reported that 84.8% of patients exhibit multiple skeletal
metastases at the time of NSCLC diagnosis, which cause
complications including bone pain, pathological fractures, spinal
cord compression and dysmotility (3). There are differences in the prognosis
of NSCLC patients with and without bone metastases (4,5). In
addition, 54.3% of patients experience skeletal-related events
(SREs) at the time of NSCLC diagnosis (3). SREs include radiotherapy, pathological
fractures, spinal cord compression, orthopedic surgery and
hypercalcemia. SREs affect not only the prognosis but also the
activities of daily living (6).
However, to the best of our knowledge, there are currently no
reports evaluating the risk factors for SREs at NSCLC diagnosis.
The aim of the present study was to examine the risk factors for
SREs and overall survival in patients with SREs or bone metastases
at the time of NSCLC diagnosis.
Patients and methods
Patients
A total of 1,072 NSCLC patients who were treated at
Kagoshima University Hospital between 2006 and 2013 were
retrospectively identified, and 85 patients with bone metastases at
the time of NSCLC diagnosis, whose histopathological diagnosis of
NSCLC was available, were enrolled in the present study. All deaths
were due to NSCLC or cancer-related complications. The presence of
bone metastasis was diagnosed by physicians, radiologists and
orthopedic surgeons. Bone metastases were detected by X-ray,
computed tomography (CT) scans, magnetic resonance imaging (MRI) of
the skeleton, or positron emission tomography (PET)-CT. In all the
cases, diagnosis was confirmed by pathological examination. All the
patients who received molecular-targeted therapy had epidermal
growth factor receptor (EGFR) mutations. Pathological fractures,
spinal cord compression and hypercalcemia were defined as SREs, as
were radiotherapy and orthopedic surgery that were performed for
bone metastases at the time of NSCLC diagnosis. Improvements in the
primary tumor were defined as partial or complete response
according to the Response Evaluation Criteria In Solid Tumors
guidelines (7). Improvements in bone
metastases were defined as reduced tumor size on CT scan. When the
Mirel's score was >8 points, surgical treatment for long bone
metastases was undertaken (8). In
one case with a Tokuhashi score of 1, surgery for spinal metastasis
was undertaken according to the patient's request.
The local Ethics Committee of Kagoshima University
reviewed and approved the present study, and access to the database
was approved by the Research Ethics Committee at the Kagoshima
University (trial registration no. 438; name of registry:
‘Evaluation of utility of imaging analysis of metastatic bone
tumor’; URL of registry: http://www.orthop-kagoshima-u.com/; date of
registration: 02/05/2014). All the patients provided written
informed consent for their records to be used in this study.
Statistical analysis
Kaplan-Meier analysis was used to evaluate
prognosis. Multiple logistic regression analysis was used to
evaluate the risk factors for SREs. The Cox proportional hazards
model was used to examine the risk factors for survival. All
statistical analyses were performed using BellCurve for Excel
(Social Survey Research Information Co., Ltd. Tokyo, Japan).
P-values of <0.05 were considered to indicate statistically
significant differences.
Results
Squamous cell carcinoma is a risk
factor for SREs
The median patient age was 66.0 years (range,
55.0–72.0 years), and 52 of the 85 patients were male (61.2%). The
median follow-up period from NSCLC diagnosis was 7 months (range,
4.9–9.1 months). The histopathological diagnosis of NSCLC was
adenocarcinoma (n=55), squamous cell carcinoma (n=16), and other
types of NSCLC (n=14). A total of 73 patients (85.9%) were affected
by multiple bone metastases at the time of NSCLC diagnosis. The
most common site of bone metastases was the spine (n=70), followed
by the pelvis (n=46), sacrum (n=31) and extremities (n=26)
(Table I). A total of 47 patients
(55.2%) were affected by SREs at the time of NSCLC diagnosis. The
most frequent SREs were radiotherapy (87.2%) followed by spinal
cord compression (31.9%), pathological fracture (21.3%), surgery
(14.9%), and hypercalcemia (8.5%) (Table II). Univariate analysis revealed
that a higher ECOG PS score (9) and
squamous cell carcinoma were risk factors for SREs at the time of
NSCLC diagnosis. Multivariate logistic regression analysis revealed
that squamous cell carcinoma was a risk factor for SREs at the time
of NSCLC diagnosis (Table III).
The incidence rate of SREs in squamous cell carcinoma and
adenocarcinoma was 87.5% (14/16) and 47.3% (26/55), respectively.
The Fisher's exact test also revealed that the incidence rate of
SREs was significantly higher in squamous cell carcinoma compared
with that in adenocarcinoma patients at the time of NSCLC diagnosis
(Table IV).
 | Table I.Non-small-cell lung cancer patients
with bone metastases (n=85). |
Table I.
Non-small-cell lung cancer patients
with bone metastases (n=85).
| Characteristics | Values |
|---|
| Male sex, no.
(%) | 52 (61.2) |
| Age (years), median
(range) | 66.0 (55.0–72.0) |
| ECOG PS, median
(range) | 2 (1–2) |
| BMI
(kg/m2), median (range) | 20.3 (18.2–22.8) |
| Days on treatment
after diagnosis, median (range) | 15.0 (6.0–24.0) |
| Brinkmann index,
median (range) | 200 (0–840) |
| Adenocarcinoma, no.
(%) | 55 (64.7) |
| Squamous cell
carcinoma, no. (%) | 16 (18.8) |
| Spine metastasis, no.
(%) | 70 (82.4) |
| Cervical metastasis,
no. (%) | 25 (29.4) |
| Thoracic metastasis,
no. (%) | 50 (58.8) |
| Lumbar metastasis,
no. (%) | 43 (50.6) |
| Sacral metastasis,
no. (%) | 31 (36.5) |
| Pelvic metastasis,
no. (%) | 46 (54.1) |
| Bone of extremities
metastasis, no. (%) | 26 (30.6) |
| Multiple bone
metastasis, no. (%) | 73 (85.9) |
| Single bone
metastasis, no. (%) | 12 (14.1) |
| Brain metastasis, no.
(%) | 32 (37.6) |
| Adrenal gland
metastasis, no. (%) | 18 (21.2) |
| Liver metastasis, no.
(%) | 18 (21.2) |
| Lymph node
metastasis, no. (%) | 72 (84.7) |
| SREs, no. (%) | 47 (55.3) |
| Spinal complaint, no
(%) | 15 (17.6) |
| Hypercalcemia, no.
(%) | 4 (4.7) |
| Fracture, no.
(%) | 10 (11.8) |
| Operation for bone
metastasis, no. (%) | 7 (8.2) |
| Radiotherapy, no.
(%) | 41 (48.2) |
| Molecular-targeted
therapy, no. (%) | 18 (21.2) |
| Chemotherapy, no.
(%) | 43 (50.6) |
| Bisphosphonates, no.
(%) | 22 (25.9) |
| Table II.SREs at the time of NSCLC
diagnosis. |
Table II.
SREs at the time of NSCLC
diagnosis.
| SREs | No. (%) |
|---|
| Total | 47 (55.2) |
| Radiotherapy | 41 (87.2) |
| Spinal cord
compression | 15 (31.9) |
| Pathological
fracture | 10 (21.3) |
| Hypercalcemia | 4 (8.5) |
| Surgery | 7
(14.9) |
| Table III.Risk factors for SREs at the time of
NSCLC diagnosis. |
Table III.
Risk factors for SREs at the time of
NSCLC diagnosis.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Factors | Median (range) | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years | 66 (55–73) | 1.00
(0.97–1.04) | 0.93 | (−) |
|
| Male sex | 28 | 0.85
(0.36–2.07) | 0.74 | (−) |
|
| BMI | 20.3
(18.2–21.6) | 0.94
(0.83–1.06) | 0.29 | (−) |
|
| Smoking | 28 | 1.07
(0.45–2.55) | 0.88 | (−) |
|
| Number of bone
metastases | 4 (2–7) | 1.02
(0.92–1.13) | 0.72 | (−) |
|
| Spine
metastasis | 41 | 2.12
(0.68–6.61) | 0.20 | 3.11
(0.74–13.09) | 0.12 |
| Cervical
metastasis | 14 | 1.04
(0.41–2.66) | 0.93 | (−) |
|
| Thoracic
metastasis | 27 | 0.88
(0.34–2.10) | 0.77 | (−) |
|
| Lumbar
metastasis | 23 | 0.86
(0.37–2.03) | 0.73 | (−) |
|
| Sacral
metastasis | 17 | 0.47
(0.40–2.36) | 0.95 | (−) |
|
| Pelvic
metastasis | 28 | 1.64
(0.69–3.88) | 0.26 | (−) |
|
| Thigh
metastasis | 14 | 1.59
(0.59–4.32) | 0.36 | 1.46
(0.52–4.16) | 0.47 |
| Rib metastasis | 20 | 0.54
(0.23–1.28) | 0.16 | (−) |
|
| Humerus
metastasis | 7 | 2.04
(0.49–8.50) | 0.33 | (−) |
|
| Brain
metastasis | 14 | 0.92
(0.36–2.32) | 0.86 | (−) |
|
| Liver
metastasis | 6 | 0.65
(0.20–2.12) | 0.47 | (−) |
|
| Adrenal gland
metastasis | 16 | 1.049
(0.35–3.14) | 0.932 | (−) |
|
| Lymph node
metastasis | 40 | 0.32
(0.06–1.63) | 0.17 | (−) |
|
| PS score | 2 (1–3) | 1.67
(1.08–2.60) | 0.021 | 1.40
(0.88–2.24) | 0.16 |
| Squamous cell
carcinoma | 14 | 7.64
(1.61–36.16) | 0.01 | 9.41
(1.65–53.81) | 0.012 |
| Adenocarcinoma | 26 | 0.38
(0.15–0.99) | 0.04 | (−) |
|
| Molecular-targeted
therapy | 18 | 1.35
(0.47–3.92) | 0.58 | (−) |
|
| Table IV.Association between SREs and
pathological diagnosis of NSCLC. |
Table IV.
Association between SREs and
pathological diagnosis of NSCLC.
| Type of NSCLC | SREs at the time of
NSCLC diagnosis | No SREs at the time
of NSCLC diagnosis |
|---|
| Squamous cell
carcinoma | 14 | 2 |
| Adenocarcinoma | 26 | 29 |
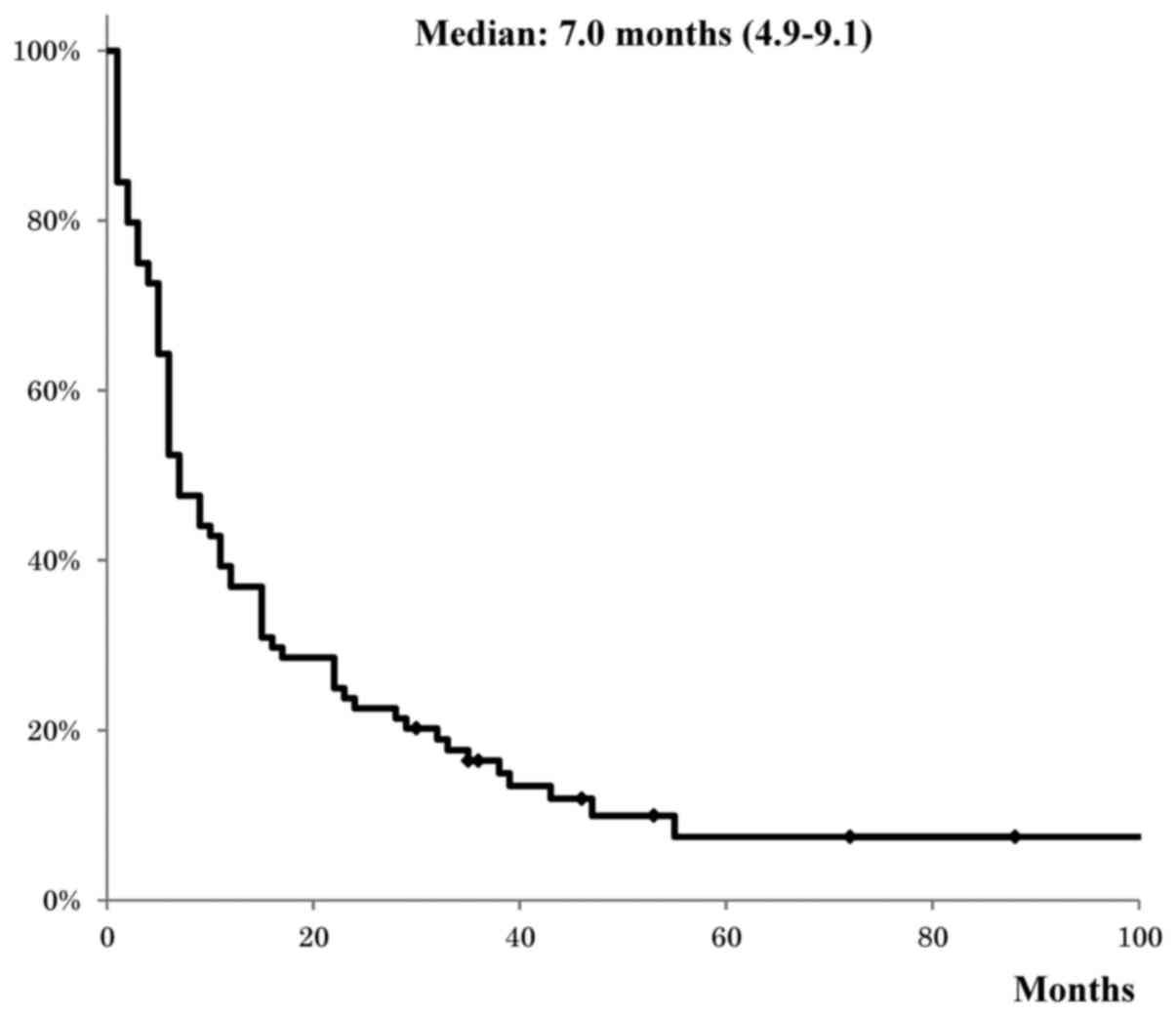
Survival rates of patients with bone
metastasis at the time of NSCLC diagnosis
The median survival after diagnosis of NSCLC and
bone metastasis was 7.0 months. The 1-, 2-, 3- and 5-year survival
rates of patients with bone metastasis at the time of NSCLC
diagnosis were 38.8, 23.5, 12.9 and 3.5%, respectively (Fig. 1).
Prognostic factors for patients with
bone metastasis at the time of NSCLC diagnosis
The Cox proportional hazards model was used to
evaluate the prognostic factors for patients with bone metastasis
at the time of NSCLC diagnosis. Univariate analysis revealed that
older age, male sex, higher ECOG PS score, and presence of adrenal
gland and liver metastasis, were risk factors for poor prognosis,
whereas molecular-targeted therapy, chemotherapy and improvement of
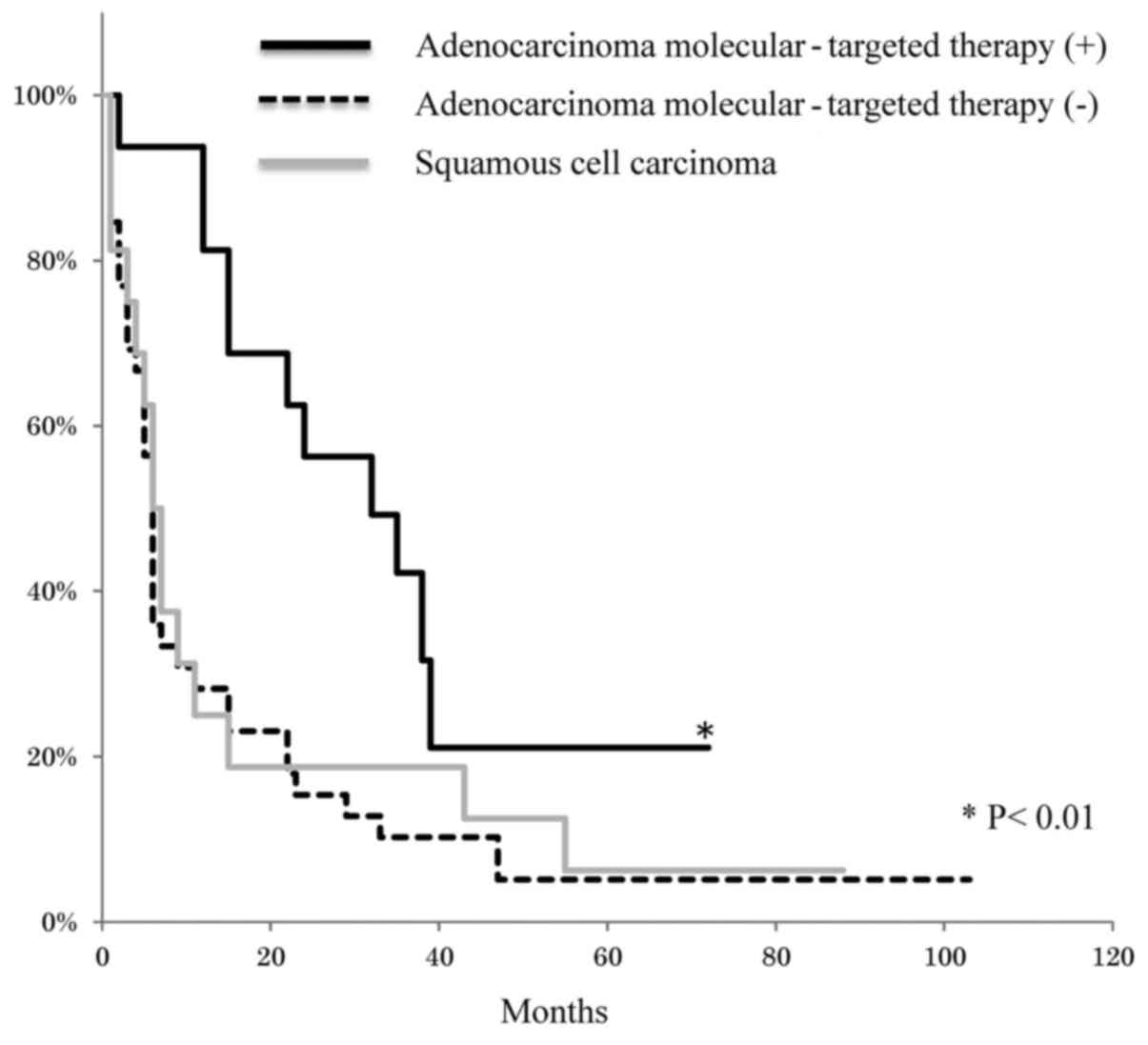
bone metastasis on CT were factors for better prognosis (Table V). Multivariate analysis revealed
that higher ECOG PS score and metastasis to the adrenal gland were
risk factors for poor prognosis, while surgery for bone metastasis
and molecular-targeted therapy were factors for better prognosis
(Table V). In addition, Kaplan-Meier
analysis revealed that adenocarcinoma with molecular-targeted
therapy had a better prognosis compared with squamous cell
carcinoma and adenocarcinoma without molecular-targeted therapy
(Fig. 2).
| Table V.Risk factors of poor prognosis for
patients with bone metastasis at the time of NSCLC diagnosis: Cox
proportional hazards model for survival. |
Table V.
Risk factors of poor prognosis for
patients with bone metastasis at the time of NSCLC diagnosis: Cox
proportional hazards model for survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age | 1.03
(1.01–1.06) | 0.006 | (−) |
|
| Male sex | 2.00
(1.24–3.24) | 0.005 | (−) |
|
| ECOG PS | 1.34
(1.07–1.68) | 0.01 | 1.46
(1.16–1.84) |
0.002 |
| BMI | 1.02
(0.96–1.09) | 0.51 | (−) |
|
| Smoking | 1.41
(0.89–2.25) | 0.14 | (−) |
|
| Adenocarcinoma | 0.71
(0.45–1.14) | 0.16 | (−) |
|
| Squamous cell
carcinoma | 1.13
(0.64–2.00) | 0.67 | (−) |
|
| Number of bone
metastasis | 1.04
(0.99–1.09) | 0.12 | (−) |
|
| Only bone
metastasis | 0.68
(0.31–1.49) | 0.33 | (−) |
|
| Brain
metastasis | 0.68
(0.45–1.13) | 0.13 | (−) |
|
| Adrenal gland
metastasis | 3.02
(1.66–5.48) |
<0.001 | 2.34
(1.27–4.31) |
<0.001 |
| Liver
metastasis | 2.80
(1.49–5.24) | 0.001 | (−) |
|
| Lymph node
metastasis | 1.43
(0.68–2.99) | 0.34 | (−) |
|
| SREs | 0.84
(0.53–1.33) | 0.46 | (−) |
|
| Spinal
complaint | 1.09
(0.63–1.96) | 0.76 | (−) |
|
| Hypercalcemia | 0.56
(0.17–1.79) | 0.32 | (−) |
|
| Fracture | 1.10
(0.55–2.21) | 0.79 | (−) |
|
| Radiotherapy | 0.81
(0.52–1.28) | 0.37 | (−) |
|
| Operation for bone
metastasis | 0.40
(0.16–1.02) | 0.05 | 0.35
(0.13–0.97) | 0.04 |
| Molecular-targeted
therapy | 0.38
(0.21–0.69) |
0.002 | 0.37
(0.20–0.70) |
0.002 |
|
Bisphosphonates | 0.77
(0.45–1.31) | 0.34 | (−) |
|
| Chemotherapy | 0.40
(0.25–0.64) |
<0.001 | 0.66
(0.39–1.01) | 0.11 |
| Improvement of bone
metastasis | 0.29
(0.09–0.92) | 0.036 | (−) |
|
| Improvement of
primary lesion | 0.56
(0.30–1.04) | 0.065 | (−) |
|
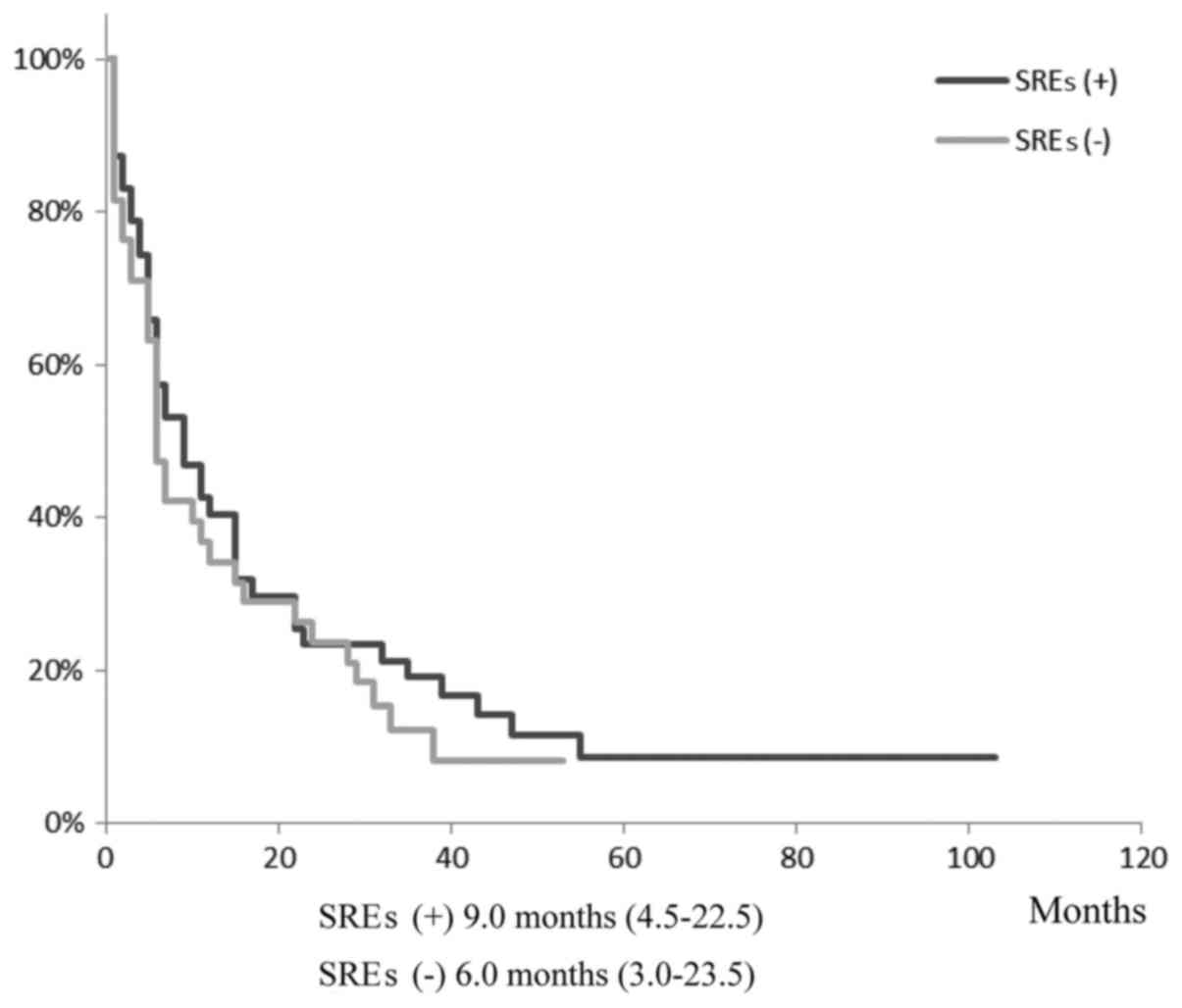
Prognostic factors for patients with
SREs at the time of NSCLC diagnosis
Kaplan-Meier analysis revealed that there was no
difference in the overall survival between the SRE and no SRE
groups (Fig. 3). Cox hazard model
analysis was performed using four factors that were found to be
significant for the prognosis of patients with bone metastasis at
the time of NSCLC diagnosis. The Cox hazard model demonstrated that
a higher ECOG PS score was a risk factor for poor prognosis, while
surgery for bone metastasis and molecular-targeted therapy were
factors for better prognosis (Table
VI).
| Table VI.Risk factors of poor prognosis with
SREs at the time of NSCLC (n=47) Cox proportional hazards model for
survival. |
Table VI.
Risk factors of poor prognosis with
SREs at the time of NSCLC (n=47) Cox proportional hazards model for
survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| ECOG PS | 1.49
(1.10–2.00) |
0.01 | 1.77
(1.30–2.42) |
<0.001 |
| Adrenal gland
metastasis | 3.11
(1.39–6.97) |
<0.01 | 2.01
(0.87–4.62) | 0.10 |
| Surgery for bone
metastasis | 0.39
(0.15–1.03) |
0.06 | 0.23
(0.08–0.69) | 0.01 |
| Molecular-targeted
therapy | 0.47
(0.22–0.99) |
0.04 | 0.32
(0.14–0.72) | 0.01 |
Discussion
The overall prognosis of NSCLC for a substantial
portion of patients remains poor, as the majority of patients have
metastasis at the time of NSCLC diagnosis. Although several risk
factors affect overall survival in NSCLC (10–15), it
remains unclear which risk factors crucially affect SREs. It was
hypothesized that examination of the risk factors for patients with
SREs and bone metastasis at the time of NSCLC diagnosis would
provide a more accurate prediction of prognosis and more suitable
therapeutic strategies for these patient groups. Squamous cell
carcinoma was found to be an independent risk factor for SREs at
the time of NSCLC diagnosis. It has been reported that the
frequency of distant metastases is higher in adenocarcinoma
(3,16,17);
there are discrepancies between those findings and the findings of
the present study. It was also observed that the incidence rate of
SREs was significantly higher in squamous cell carcinoma compared
with that in adenocarcinoma patients at the time of NSCLC
diagnosis. These findings suggest that bone metastasis of squamous
cell carcinoma causes the development of SREs earlier compared with
adenocarcinoma. The development of bone metastasis is a multistage
process involving penetration of cancer cells from the surrounding
tissue, invasion into the lymphatic or vascular circulation,
transportation to the bone, proliferation in the bone tissue and
bone destruction (18,19). Our findings suggest that bone
metastasis from squamous cell carcinoma may destroy bone tissue
more quickly compared with that from adenocarcinoma. Osteoclast
cells in close proximity to bone metastases by squamous cell
carcinoma were strongly activated for bone resorption (20), which supports this hypothesis.
Although SREs are reported to reduce quality of
life, physical function, emotional happiness and overall survival
(21–23), the present results revealed no
difference in overall survival between the SRE and no SRE groups.
Multivariate analysis revealed that a higher ECOG PS score was a
risk factor for poor prognosis in patients with SREs at the time of
NSCLC diagnosis, while surgery for bone metastasis and
molecular-targeted therapy were factors for better prognosis. These
findings indicated that radical cure may be considered for patients
with SREs at the time of NSCLC diagnosis.
Multivariate analysis revealed that a higher ECOG PS
score was a risk factor for poor prognosis, while
molecular-targeted therapy was a factor for better prognosis in
patients with bone metastasis at the time of NSCLC diagnosis. These
findings are consistent with previous reports (4,24).
Kaplan-Meier analysis revealed that adenocarcinoma with
molecular-targeted therapy had a better prognosis compared with
squamous carcinoma and adenocarcinoma without molecular-targeted
therapy. All the cases treated with molecular-targeted therapy had
adenocarcinoma with EGFR mutations. Adenocarcinoma with and without
mutations may be categorized into different subgroups of NSCLC for
prognosis research.
In addition, surgery for bone metastasis was found
to be a factor for better prognosis. In accordance with our
findings, several reports demonstrated that a surgical approach to
metastatic NSCLC may improve prognosis (25–27).
There is a possibility that surgery was performed only on patients
who were expected to have better prognosis. Nonetheless, our
multivariate analysis included several critical explanatory
variables for prognosis, including ECOG PS, number of bone
metastases, visceral metastasis, SREs, chemotherapy, and
molecular-targeted therapy. The inclusion of these critical
prognostic factors in the multivariate analysis excludes a
significant deviation in the indication for surgery by prediction
of overall survival.
The multivariate analysis revealed that metastasis
to the adrenal gland was a risk factor for poor prognosis. The
adrenal gland is a major site of NSCLC metastases (15%) (28). Adrenal metastases of NSCLC usually
exhibit hematogenous spread to other sites. In accordance with our
findings, it has been reported that NSCLC metastasizing to the
adrenal glands is incurable (29,30).
There were several limitations to the present study:
Data collection was retrospective. Furthermore, although the
majority of cases with bone metastasis should be referred to the
Department of Orthopaedic Surgery of Kagoshima University Hospital,
as this is the only university hospital that undertakes orthopedic
surgery and therapeutic radiology, several cases were referred to
other hospitals in the area.
Several prognostic factors for SREs and bone
metastasis patients at the time of NSCLC diagnosis were identified.
While surgical treatment and molecular-targeted therapy improve the
prognosis of patients with SREs or bone metastasis at the time of
NSCLC diagnosis, patients with higher ECOG PS score and adrenal
metastasis may benefit more from radiotherapy or best supportive
care.
Acknowledgements
The authors would like to thank Ms. Ayano Komure and
Ms. Kana Maeda for their excellent assistance. We would also like
to thank Edanz Editing Japan (Fukuoka, Japan) for providing medical
editing services.
Glossary
Abbreviations
Abbreviations:
|
NSCLC
|
non-small-cell lung cancer
|
|
SREs
|
skeletal-related events
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
PET
|
positron emission tomography
|
References
|
1
|
Zeng X, Li J, Peng L, Wang Y, Tan C, Chen
G, Wan X, Lu Q and Yi L: Economic outcomes of maintenance gefitinib
for locally advanced/metastatic non-small-cell lung cancer with
unknown EGFR mutations: A semi-Markov model analysis. PLoS One.
9:e888812014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rosen LS, Gordon D, Tchekmedyian NS,
Yanagihara R, Hirsh V, Krzakowski M, Pawlicki M, De Souza P, Zheng
M, Urbanowitz G, et al: Long-term efficacy and safety of zoledronic
acid in the treatment of skeletal metastases in patients with
nonsmall cell lung carcinoma and other solid tumors: A randomized,
Phase III, double-blind, placebo-controlled trial. Cancer.
100:2613–2621. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
He YF, Luo HQ, Wang W, Chen J, Yao YW, Cai
SB, He J, Yan Y, Wu SS, Hu XX, et al: Clinical features and
prognosis-associated factors of non-small cell lung cancer
exhibiting symptoms of bone metastasis at the time of diagnosis.
Oncol Lett. 9:2706–2712. 2015.PubMed/NCBI
|
|
4
|
Ulas A, Bilici A, Durnali A, Tokluoglu S,
Akinci S, Silay K, Oksuzoglu B and Alkis N: Risk factors for
skeletal-related events (SREs) and factors affecting SRE-free
survival for nonsmall cell lung cancer patients with bone
metastases. Tumour Biol. 37:1131–1140. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Santini D, Barni S, Intagliata S, Falcone
A, Ferraù F, Galetta D, Moscetti L, La Verde N, Ibrahim T, Petrelli
F, et al: Natural history of non-small-cell lung cancer with bone
metastases. Sci Rep. 5:186702015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shimada H, Setoguchi T, Yokouchi M, Sasaki
H, Ishidou Y, Kawamura I, Abematsu M, Nagano S and Komiya S:
Metastatic bone tumors: Analysis of factors affecting prognosis and
efficacy of CT and F-FDG PET-CT in identifying primary lesions. Mol
Clin Oncol. 2:875–881. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mirels H: Metastatic disease in long
bones. A proposed scoring system for diagnosing impending
pathologic fractures. 1989. Clin Orthop Relat Res. (415
Suppl):S4–S13. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu M, Zhao J, Song SW, Zhuo M, Wang X, Bai
H, Wang S, Yang L, An T, Zhang Y, et al: EGFR mutations are
associated with prognosis but not with the response to front-line
chemotherapy in the Chinese patients with advanced non-small cell
lung cancer. Lung Cancer. 67:343–347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Aggarwal C and Langer CJ: Older age, poor
performance status and major comorbidities: How to treat high-risk
patients with advanced nonsmall cell lung cancer. Curr Opin Oncol.
24:130–136. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Leprieur Giroux E, Lavole A, Ruppert AM,
Gounant V, Wislez M, Cadranel J and Milleron B: Factors associated
with long-term survival of patients with advanced non-small cell
lung cancer. Respirology. 17:134–142. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kalikaki A, Koutsopoulos A, Hatzidaki D,
Trypaki M, Kontopodis E, Stathopoulos E, Mavroudis D, Georgoulias V
and Voutsina A: Clinical outcome of patients with non-small cell
lung cancer receiving front-line chemotherapy according to EGFR and
K-RAS mutation status. Lung Cancer. 69:110–115. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Leung EY, Scott HR and McMillan DC:
Clinical utility of the pretreatment glasgow prognostic score in
patients with advanced inoperable non-small cell lung cancer. J
Thorac Oncol. 7:655–662. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pirker R, Pereira JR, Szczesna A, von
Pawel J, Krzakowski M, Ramlau R, Vynnychenko I, Park K, Eberhardt
WE, de Marinis F, et al: Prognostic factors in patients with
advanced non-small cell lung cancer: Data from the phase III FLEX
study. Lung Cancer. 77:376–382. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang Y, Jin B, Shao M, Dong Y, Lou Y,
Huang A and Han B: Monitoring of carcinoembryonic antigen levels is
predictive of EGFR mutations and efficacy of EGFR-TKI in patients
with lung adenocarcinoma. Tumour Biol. 35:4921–4928. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Duan JC, An TT, Wu MN, Yang L, Bai H, Wang
ZJ, Wang YY, Zhuo ML, Zhao J, Wang SH and Wang J: Correlation
between the efficacy of epidermal growth factor receptor tyrosine
kinase inhibitors and EGFR mutations in advanced squamous cell lung
cancer. Zhonghua Jie He He Hu Xi Za Zhi. 35:323–328. 2012.(In
Chinese). PubMed/NCBI
|
|
17
|
Stetler-Stevenson WG: Type IV collagenases
in tumor invasion and metastasis. Cancer Metastasis Rev. 9:289–303.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mundy GR: Mechanisms of bone metastasis.
Cancer. 80 (8 Suppl):S1546–S1556. 1997. View Article : Google Scholar
|
|
19
|
Tomita A, Kasaoka T, Inui T, Toyoshima M,
Nishiyama H, Saiki H, Iguchi H and Nakajima M: Human breast
adenocarcinoma (MDA-231) and human lung squamous cell carcinoma
(Hara) do not have the ability to cause bone resorption by
themselves during the establishment of bone metastasis. Clin Exp
Metastasis. 25:437–444. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Coleman RE: Metastatic bone disease:
Clinical features, pathophysiology and treatment strategies. Cancer
Treat Rev. 27:165–176. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Coleman RE: Bisphosphonates: Clinical
experience. Oncologist. 9 Suppl 4:S14–S27. 2004. View Article : Google Scholar
|
|
22
|
Cetin K, Christiansen CF, Jacobsen JB,
Nørgaard M and Sørensen HT: Bone metastasis, skeletal-related
events, and mortality in lung cancer patients: A Danish
population-based cohort study. Lung Cancer. 86:247–254. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bae HM, Lee SH, Kim TM, Kim DW, Yang SC,
Wu HG, Kim YW and Heo DS: Prognostic factors for non-small cell
lung cancer with bone metastasis at the time of diagnosis. Lung
Cancer. 77:572–577. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Plones T, Osei-Agyemang T, Krohn A and
Passlick B: Surgical treatment of extrapulmonary oligometastatic
non-small cell lung cancer. Indian J Surg. 77 Suppl 2:S216–S220.
2015. View Article : Google Scholar
|
|
25
|
Chen YJ, Chang GC, Chen HT, Yang TY, Kuo
BI, Hsu HC, Yang HW and Lee TS: Surgical results of metastatic
spinal cord compression secondary to non-small cell lung cancer.
Spine (Phila Pa 1976). 32:E413–E418. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lei M, Liu Y, Tang C, Yang S, Liu S and
Zhou S: Prediction of survival prognosis after surgery in patients
with symptomatic metastatic spinal cord compression from non-small
cell lung cancer. BMC Cancer. 15:8532015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Niu FY, Zhou Q, Yang JJ, Zhong WZ, Chen
ZH, Deng W, He YY, Chen HJ, Zeng Z, Ke EE, et al: Distribution and
prognosis of uncommon metastases from non-small cell lung cancer.
BMC Cancer. 16:1492016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Urschel JD, Finley RK and Takita H:
Long-term survival after bilateral adrenalectomy for metastatic
lung cancer: A case report. Chest. 112:848–850. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Karolyi P: Do adrenal metastases from lung
cancer develop by lymphogenous or hematogenous route? J Surg Oncol.
43:154–156. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chadeyras JB, Mazel C and Grunenwald D:
Vertebral en bloc resection for lung cancer: Twelve years'
experience. Ann Chir. 131:616–622. 2006.(In French). View Article : Google Scholar : PubMed/NCBI
|