Introduction
Recent advances in the long-term survival of organ
transplant recipients have led to an increased incidence of
malignant tumors after transplantation (1). The incidence of de novo tumors has been
reported to be ranging from 2.6 to 11.5% in liver transplant
recipients (2). The most common
malignancy diseases after transplantation are solid tumors,
including lymphoproliferative disease, skin cancers and sarcomas
(3). However, chronic myeloid
leukemia (CML) is a rare complication after liver transplantation.
The first case of CML after liver transplantation was reported in
2007 (4), after that two cases of
post transplantation CML has been reported (5,6). Here we
report a 42-year-old male patient who developed CML 14 months after
liver transplantation.
Case report
A 42-year-old male patient presented with a
hepatitis B virus related acute liver failure, was admitted to our
hospital on October 1, 2014. Blood tests at the diagnosis revealed:
white blood cell (WBC) 7.4×109/l, with 17.4% lymphocytes, 71.9%
neutrophils and no immature cells. Liver function test showed: ALT
1287 U/l, AST 1063 U/l, TBIL 327.2 µmol/l, DBIL 244 µmol/l, IBIL
83.2 µmol/l. Conservative treatment was invalid. On November 21,
2014, the patient accepted a living donor liver transplantation
(LDLT). After LDLT, the patient achieved normal liver function: ALT
23 U/l, AST 15 U/l, TBIL 14.2 µmol/l, DBIL 8.86 µmol/l, IBIL 5.3
µmol/l. The immunosuppressive therapy comprised tacrolimus,
mycophenolate mofetil and prednisone. A biopsy of hepatic revealed
chronic severe hepatitis accompanied nodular cirrhosis.
In December 2015, 12 months after transplantation,
the patient's blood test revealed leukocytosis at
12.45×109/l. At 14 months posttransplantion, his white
blood cell (WBC) increased to 37.49×109/l, with 79.2%
neutrophils, 8.7% lymphocytes, 4.8% monocytes, 3.1% eosinophils,
4.2% basophils and 22.7% immature granulocyte. Liver function test
revealed normal limits: ALT 16 U/l, AST 30 U/l, TBIL 11.1 µmol/l,
DBIL 2.6 µmol/l, IBIL 8.6 µmol/l. Bone marrow (BM) aspirate showed
massive infiltration of neutrophils, eosinophils and basophils,
which confirmed the diagnosis of chronic myeloid leukemia (CML) in
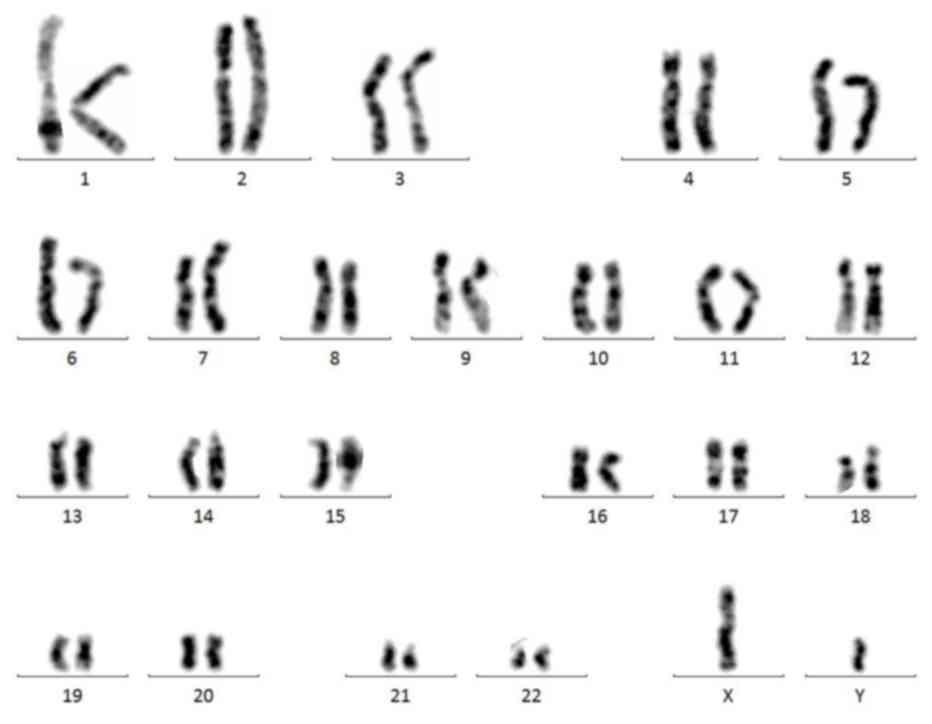
chronic phase. Genetic testing revealed BCR-ABL (P210) positive by
polymerase chain reaction (PCR). The quantitative of BCR-ABL
transcript was 31.763%. The mutation of BCR-ABL kinase region was
negative. Chromosome analysis showed 46, XY, t (9;22) (q34; q11.2)
(Fig. 1). A diagnosis of chronic
myeloid leukemia (CML) in chronic phase was made.
The patient received imatinib 400 mg once daily.
After 1 month treatment, the WBC count decreased to
3.81×109/l. The patient achieved complete hematologic
remission (CHR) after 3 months imatinib treatment, and continuous
CHR thereafter. Liver function test was within normal limits: ALT
14 U/l, AST 20 U/l, TBIL 15.9 µmol/l, DBIL 6 µmol/l, IBIL 9.9
µmol/l. At 3 months post imatinib treatment, the quantitative of
BCR-ABL transcript had decreased to 2.7838%, consistent with early
molecular response (EMR). 12 months after imatinib treatment, the
patient's BCR-ABL transcript had been <0.1%, consistent with
major molecular response (MMR). At 30 months posttransplantion, the
patient is alive with no graft rejection. He remains CHR 13 months
after the diagnosis of CML. His current therapy includes imatinib,
tacrolimus, mycophenolate mofetil and prednisone.
Discussion
With the increasing number of long-term survivors of
transplantation, the incidence of malignancy disease post
transplantation is higher. The most common malignancy diseases
after solid organ transplantation are solid tumors, including
lymphoprolifer-ative disease, skin cancers and sarcomas (3). While the subsequent malignancy diseases
after HSCT are solid tumors, post-transplant lymphoproliferative
disease (PTLD) and hematologic malignancies (7). The annual incidence of CML ranges from
0.35 to 0.55 per 100,000 in Chinese population (8). There was no report about the incidence
of CML post LDLT, just few case reports, so CML is a rarely
complication after LDLT.
There were many hypotheses regarding the development
of malignancies in LDLT recipients. Immunosuppressive medications
were regarded as the most important risk factor for malignancies
after transplantation (9). The role
of immunosuppressants in the leukemogenesis has not been
elucidated. Mycophenolate mofetil is an inhibitor of hypoxanthine
nucleotide dehydrogenase highly expressed in the leukemia, which
can develop an anti-leukemia effect (10). Our patient received Mycophenolate
mofetil as immunosuppressive therapy. Whether Mycophenolate mofetil
can reduce the incidence of leukemia after transplantation needs to
be studied further. Moreover, viral infections have been reported
to be associated with malignancies after transplantation, such as
Epstein-Barr virus, human herpes virus-8, and Papillomaviruses
(11). The correlation between
hepatitis virus infection and CML deserved further investigation.
Some reported cases of leukemia after transplantation have
associated chromosomal abnormalities, for example trisomy 8,
monosomy 7, t(15;17), inv (16) and
t(9;22) (12,13). Our patient had chromosomal
abnormalities involving Philadelphia chromosome.
The most common presentation is leukocytosis or
thrombocytosis in the chronic phase of CML. Our patient presented
with leukocytosis for two months with no clinical symptoms. Once
the diagnosis of CML was confirmed, the patient prompty received
imatinib treatment. Effective immunosuppressive therapy greatly
reduced the incidence of graft rejection and improved survival
time, however, cancer and infections may increase. Some authors
reduced tacrolimus to the minimized dosage to maintain stable liver
function during acute leukemia chemotherapy (14). Imatinib had been used as a first-line
treatment for newly diagnosed CML. However, several cases of
hepatotoxicity, including acute liver failure have been reported in
the long term imatinib therapy (15). Imatinib-induced acute liver failure
is a rare and serious complication of imatinib therapy. Our patient
received the same dosage of immunosuppressants during imatinib
treatment, and his liver function was normal. The early diagnosis
and timely treatment of leukemia post transplantation may
significantly reduce mortality (16).
The pathogenesis, risk factors, treatment and
prognosis for CML post liver transplantation are unclear.
Therefore, further analysis through accumulation cases will be of
great importance to prevent and treat this rare complication after
liver transplantation.
Acknowledgements
We thank the members of the Department of
Hematology, The Third Affiliated Hospital, Sun Yat-sen University
for their critical comments. The present study was supported by the
Science and Technology Planning Project of Guangzhou city (No.
201604016070) to Dr X.-W. Jiang.
References
|
1
|
Penn I: Posttransplant malignancies.
Transplant Proc. 31:1260–1262. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kauffman HM, Cherikh WS and Cheng Y:
Posttransplantation malignancies: A problem, a challenge, and an
opportunity. Liver Transpl. 8:488–490. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jiang N, Li H, Wang GS, Zhang J, Zhang JF,
Yi SH, Yang Y, Cai CJ, Lu MQ and Chen GH: Acute leukemia, a rare
but fatal complication after liver transplantation. Leuk Res.
33:1349–1351. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Concejero A, Chen CL, Wang CC, Wang SH,
Lin CC, Liu YW, Yang CH, Yong CC, Wang MC and Eng HL: Chronic
myeloid leukemia after living donor liver transplantation.
Transplantation. 83:1521–1522. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
le Coutre P, Reinke P, Neuhaus R, Trappe
R, Ringel F, Lalancette M, Hemmati PG, Dörken B and Daniel PT:
BCR-ABL positive cells and chronic myeloid leukemia in immune
suppressed organ transplant recipients. Eur J Haematol. 84:26–33.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chiefer J, Mathers E, Bras P and Milan Z:
Re-do liver transplantation in a young patient with chronic myeloid
leukemia following a recent sepsis episod. Edorium J Anesth.
2:25–27. 2016.
|
|
7
|
Gündüz M, Özen M, Şahin U, Toprak SK,
Bozdağ Civriz S, Kurt Yüksel M, Arslan Ö, Özcan M, Demirer T,
Beksaç M, et al: Subsequent malignancies after allogeneic
hematopoietic stem cell transplantation. Clin Transplant.
31:e129872017. View Article : Google Scholar
|
|
8
|
Yin XF, Wang JH, Li X, Yu MX, Ma ZX and
Jin J: Incidence of second malignancies of chronic myeloid leukemia
during treatment with tyrosine kinase inhibitors. Clin Lymphoma
Myeloma Leuk. 16:577–581. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cho YU, Chi HS, Park CJ, Seo EJ, Lee JH,
Lee JH and Lee SG: Two cases of post-liver transplant acute myeloid
leukemia in korean adults: Review of bibliographies and comparison
with post-renal transplant acute myeloid leukemia. Ann Hematol.
87:513–514. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Floryk D and Thompson TC:
Antiproliferative effects of AVN944, a novel inosine
5-monophosphate dehydrogenase inhibitor, in prostate cancer cells.
Int J Cancer. 123:2294–2302. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu M, Liu J, Liu L, Yu L, Shi B, Ye L,
Zhang Y and Chen H: A case report of acute myeloid leukemia after
liver transplantation. Acta Haematol. 129:225–228. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thalhammer-Scherrer R, Wieselthaler G,
Knoebl P, Schwarzinger I, Simonitsch I, Mitterbauer G, Berlakovich
GA, Mannhalter C, Haas OA, Mayer G, et al: Post-transplant acute
myeloid leukemia (PT-AML). Leukemia. 13:321–326. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Silliman CC, Tyson RW, Wei Q, Karrer FG,
Davies SM, Blake M and McGavran L: Acute Philadelphia
chromosome-positive leukemia in an adolescent boy after liver
transplantation. J Pediatr Hematol Oncol. 25:565–568. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang GS, Dai CW, Peng HL, Xu YX and Pei
MF: Myelodysplastic syndrome with transformation to acute monocytic
leukemia with FLT3-ITD mutation following orthotopic liver
transplantation. Leuk Res. 30:908–910. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fuster F, Medina L, Vallansot R, Granell M
and Bruguera M: Imatinib-induced toxic hepatitis: Description of
two cases and review of the literature. Gastroenterol Hepatol.
30:525–530. 2007.(In Spanish). View
Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fang Y, Pinkney KA, Lee JC, Gindin T,
Weiner MA, Alobeid B and Bhagat G: T-cell acute lymphoblastic
leukaemia after liver transplantation: Post-transplant
lymphoproliferative disorder or coincidental de novo leukaemia?
Hematol Oncol. 31:49–53. 2013. View
Article : Google Scholar : PubMed/NCBI
|